
Abstract
Worry and rumination, two forms of repetitive negative thinking (RNT), are prevalent in generalized anxiety disorder (GAD) and depression. Cognitive processing biases, especially the tendency to draw negative conclusions from ambiguous information (interpretation bias), may maintain worry and rumination. Yet the relationship between interpretation bias and both forms of RNT has not been explored in clinical versus nonclinical samples. In this cross-sectional study, participants with GAD (n = 72), depression (n = 79), or neither disorder (n = 71) completed two tasks assessing interpretation bias, measures of worry and rumination, and reported negative thought intrusions during a behavioral task. Interpretation bias was associated with higher levels of worry, rumination, and negative thought intrusions. Both clinical groups generated significantly more negative interpretations than healthy comparison participants. These findings link interpretation bias to worry and rumination and establish the need for research investigating the causal role of interpretation bias in maintaining RNT.
Worry and rumination are two styles of thinking characterized by streams of negative, relatively abstract, and repetitive thoughts. Both are associated with increased anxiety and low mood (e.g., Fresco, Frankel, Mennin, Turk, & Heimberg, 2002; Segerstrom, Tsao, Alden, & Craske, 2000). The prevalence of worry and rumination across a range of psychological problems has led to their being conceptualized as part of a transdiagnostic repetitive-negative-thinking process (Ehring & Watkins, 2008). Yet despite crossing diagnostic boundaries, worry and rumination are most strongly associated and especially problematic in two particular psychological disorders. Persistent and ostensibly uncontrollable worry is a central feature of generalized anxiety disorder (GAD; American Psychiatric Association, 2013). Rumination is a common characteristic of depression (see, e.g., Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008), associated with more prolonged periods of depression and predicting new onsets of the disorder (Nolen-Hoeksema, 2000). Because worry and rumination may play a role in maintaining GAD and depression, it is vital to better understand the mechanisms involved in driving these forms of repetitive negative thinking.
Studies investigating features of worry and rumination are heterogeneous and often difficult to compare but have overall found more similarities than differences between these two forms of negative thinking, which seem to share common process features. In particular, both worry and rumination are negative in content and perceived as unpleasant and repetitive (see Kircanski, Thompson, Sorenson, Sherdell, & Gotlib, 2015; Watkins, Moulds, & Mackintosh, 2005). Differences between worry and rumination mainly seem to pertain to temporal orientation and content. For example, worry often concerns hypothetical future threats (e.g., “What if this bad thing happens?”). By contrast, rumination commonly concerns symptoms of depression and past or ongoing concerns around failure (e.g., “Why can’t I ever get this right?”). Ruminative thoughts may be less hypothetical than worry and more susceptible to daily events (Kircanski, Thompson, Sorenson, Sherdell, & Gotlib, 2018). It is thus important to be mindful of differences in core content and temporal orientation when comparing worry and rumination. However, the similarities in process features between the two prompt the question of whether both worry and rumination might share underlying cognitive mechanisms.
Interpretation bias, the tendency to consistently resolve relatively ambiguous information in a negative manner, was proposed by Hirsch and Mathews (2012) as a key cognitive process that may maintain pathological worry. Resolving ambiguity is ubiquitous in daily life. Ambiguous information involving potential future threats or negative implications of past events may be especially pertinent in relation to streams of worry and rumination. For example, if a person is worrying about an upcoming interview and wonders whether he or she will be able to articulate his or her answers, interpreting this ambiguous situation negatively will increase perceived threat. Likewise, rumination after an interview will provide opportunity for interpreting ambiguity in a negative way (e.g., an interview panelist’s smile may be interpreted as indicating mockery or derision rather than approval). These kinds of interpretations may lead to further opportunities for drawing negative conclusions when new ambiguities arise (e.g., an interviewer making notes may then be interpreted as an unfavorable rather than promising sign), perpetuating streams of worry and rumination.
Interpretation bias is evident across emotional disorders (see Hirsch, Meeten, Krahé, & Reeder, 2016), with some evidence for biases in individuals with diagnoses of GAD and depression in particular (e.g., Butler & Mathews, 1983; Everaert, Podina, & Koster, 2017; Eysenck, Mogg, May, Richards, & Mathews, 1991; Mathews, Richards, & Eysenck, 1989). In addition, studies with nonclinical or subclinical samples have also found that levels of depressive symptoms are associated with a more negative interpretation bias (e.g., Berna, Lang, Goodwin, & Holmes, 2011; Wisco & Nolen-Hoeksema, 2010). However, although interpretation bias has been hypothesized to be involved in initiating and perpetuating repetitive negative thinking, evidence for an association between a more negative interpretation bias and worry and rumination is largely missing. This lack of studies is especially evident in clinical populations with high levels of these forms of repetitive negative thinking. Yet, revealing an association between interpretation bias and both worry and rumination would indicate that interpretation bias is related to both these maladaptive thinking styles. This association, in turn, could point to a potential shared and transdiagnostic mechanism involved in these different forms of repetitive negative thinking. Furthermore, investigating interpretation bias occurring during worry and rumination may help inform approaches aimed at reducing repetitive negative thinking. This is an especially important aim given the role of worry and rumination in maintaining clinical problems (see e.g., Drost, van der Does, van Hemert, Penninx, & Spinhoven, 2014).
To our knowledge, the association between interpretation bias and levels of worry has been investigated in only one study in a nonclinical child population, which indicated that a more negative interpretation bias was related to higher trait worry (Suarez & Bell-Dolan, 2001). No cross-sectional studies to date have looked specifically at the association between interpretation bias and worry in adult clinical populations. Although several experimental studies have shown that changing interpretation bias reduces worry in people with GAD and high worriers (Hayes, Hirsch, Krebs, & Mathews, 2010; Hirsch, Hayes, & Mathews, 2009; see also Discussion section), these studies did not look at the baseline association between interpretation bias and worry. Examining whether higher levels of worry are indeed associated with a more negative interpretation bias is an important goal: At the most basic level, a lack of association between the two calls into question the rationale for aiming to ameliorate worry by changing interpretation bias.
Regarding rumination, research in nonclinical samples has demonstrated a positive association between negative interpretation bias and levels of rumination (Everaert, Grahek, et al., 2017; Mor, Hertel, Ngo, Shachar, & Redak, 2014; Wisco, Gilbert, & Marroquín, 2014). Moreover, it seems that for nonclinical dysphoric individuals, interpretation bias is evident during current bouts of rumination: When inducing a period of rumination, dysphoric individuals and individuals with high levels of “brooding” (a facet of rumination) made more negative interpretations compared with individuals in nonrumination conditions (i.e., distraction/external focus; Hertel & El-Messidi, 2006; Hertel, Mor, Ferrari, Hunt, & Agrawal, 2014, Experiment 1).
Although there is an indication that interpretation bias is related to rumination, no cross-sectional studies have assessed the association between interpretation bias and worry in adults, and critically, none have investigated interpretation bias in relation to both worry and rumination within the same study. Examining both worry and rumination within the same study is important because any differences found in the extent to which interpretation bias is linked to worry and rumination may otherwise be related to differences in design and assessment between studies. Furthermore, worry and rumination have been conceptualized as part of a repetitive-negative-thinking process (Ehring & Watkins, 2008; Kircanski et al., 2015). Yet it is unclear whether these forms of repetitive negative thinking also share common underlying cognitive processes. To address this gap in the literature, we assessed the relationship between interpretation bias and levels of both worry and rumination. Furthermore, we examined shared and unique variance between interpretation bias, worry, and rumination. In addition to measuring self-reported levels of worry and rumination, we also included a more behavioral repetitive-negative-thinking task measuring negative thought intrusions reported over a period of 5 min before and after an induced period of worry or rumination (see e.g., Hirsch, Mathews, Lequertier, Perman, & Hayes, 2013). This task provides a dynamic state measure of negative thinking and serves as a proxy for streams of worry and rumination.
Extant studies into worry and rumination have been conducted in nonclinical samples (see above). Although these studies are informative regarding associations between interpretation bias and worry and rumination, they do not assess whether interpretation bias is more pronounced in individuals with pathological levels of worry and rumination. To address this issue, we examined interpretation bias in relation to both worry and rumination in individuals with a clinical diagnosis of GAD or depression. We compared these groups with each other and contrasted these clinical groups with a healthy comparison group.
In sum, this cross-sectional study goes beyond previous research in several ways: First, we examined the relationship between interpretation bias and both levels of worry and rumination, assessed by self-report questionnaire and using a behavioral repetitive-negative-thinking task. Second, we investigated whether negative interpretation bias would be greater in individuals with a diagnosis of GAD or depression versus a healthy comparison group. We employed two different “offline” (i.e., reflective, not based on reaction times) measures of interpretation bias: the scrambled-sentences test (SST) and the recognition test (RT). Both are widely used in anxiety and depression research to assess interpretation bias (see e.g., Everaert, Duyck, & Koster, 2014; Everaert, Tierens, Uzieblo, & Koster, 2013; Mathews & Mackintosh, 2000; Rude, Durham-Fowler, Baum, Rooney, & Maestas, 2010; Rude, Valdez, Odom, & Ebrahimi, 2003; Rude, Wenzlaff, Gibbs, Vane, & Whitney, 2002; Sanchez, Everaert, De Putter, Mueller, & Koster, 2015). We chose the RT to complement the SST because it includes foil statements and is thus more oblique and less susceptible to demand and selection bias (see Hirsch et al., 2016, supplementary materials). Taking into account that measures should be tailored to the phenomena in question (see e.g., Hirsch et al., 2016), we used subsets of items for both the SST and the RT that specifically related to worry or rumination.
We predicted that indices of interpretation bias would be correlated with worry, rumination, and the number of negative thought intrusions, that is, that a more negative interpretation bias would be associated with greater levels of repetitive negative thinking. Furthermore, we expected that individuals with GAD or depression (i.e., both clinical groups) would display a more negative interpretation bias than the healthy comparison group. Given studies demonstrating a link between interpretation bias and both anxiety and depression (e.g., Butler & Mathews, 1983), we proposed that despite possible differences in the presumed dominant form of repetitive negative thinking in each disorder (worry in GAD and rumination in the depressed group), the role of cognitive biases as basic underlying processes would be similar in the two groups. Specifically, we predicted that in terms of interpretation bias, the two clinical groups would differ from the healthy comparison group but not each other.
Method
Participants
Participants were recruited from the community via advertisements placed on websites and in newspapers as well as via university circular e-mails. Participants were between 18 and 65 years old and met diagnostic criteria for current major depressive episode (DEP group), GAD (GAD group), or did not currently meet diagnostic criteria for either disorder (healthy comparison group) on the Structured Clinical Interview (SCID) for the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013; First, Williams, Karg, & Spitzer, 2015) administered at the screening stage.
Participants were included from two sources: Participants with a diagnosis of GAD or depression (n = 151) were drawn from a larger multisession study, described in Hirsch et al. (2018). We included all participants who completed the larger study as well as those who attended at least the first session (thus, the n is greater here than that included in Hirsch et al., 2018). Hirsch et al. excluded participants without a diagnosis of GAD or depression. However, as these participants still had elevated levels of anxiety and depression symptoms (a prerequisite for diagnostic screening in that study; see Hirsch et al., 2018), we recruited a separate group of participants for the healthy comparison group. 1 To ensure consistency between samples, we otherwise applied the exclusion criteria stipulated in Hirsch et al. to all participants included and recruited for the present study. In particular, before inviting participants to the SCID screening, we excluded individuals with severe depression, defined as a total score on the Patient Health Questionnaire (PHQ-9; Kroenke & Spitzer, 2002) of greater than 23, past or current risk to self (self-harm in past 12 months, suicide attempt in past 5 years, or PHQ-9 suicidal-ideation item 9 score > 1), comorbid psychosis, bipolar disorder, borderline personality disorder, substance abuse, nonnormal/not-corrected-to-normal hearing, as well as current or recent (past 6 months) psychological treatment or changes to psychotropic medication in the past 3 months.
Furthermore, participants with diagnoses of both GAD and depression were excluded. This decision was made to examine the association between interpretation bias and worry and rumination in groups whose dominant form of repetitive negative thinking was either worry or rumination. Comorbidity among these disorders is generally high; however, the exclusion criteria pertaining to risk meant that individuals with more severe depression and potentially higher likelihood of comorbidity were excluded before the SCID screening stage. Specifically, in the sample of participants included from the larger clinical study, only 12.8% of participants screened for diagnosis of depression or GAD on the SCID were excluded on the basis of meeting criteria for both disorders (the majority were excluded for not meeting diagnostic criteria for either disorder; for more detail, see Hirsch et al., 2018).
The final sample consisted of 222 participants, of which 79 were in the DEP group, 72 were in the GAD group, and 71 were in the healthy comparison group. An independent rater, blind to group, coded a randomly selected subset (20%) of diagnostic interviews to check diagnosis (GAD, DEP, neither GAD nor DEP). Interrater agreement was excellent (Cohen’s κ = .96).
Participants were predominantly British (73.8%); a minority came from other European (13.6%) or overseas (12.6%) countries. Groups did not differ by country of origin, χ2(4) = 6.06, p = .195. Participants’ highest level of education was most commonly bachelor degree (42.5%), followed by secondary education (28.0%), master’s degree (20.4%), other (e.g., higher national diploma; 7.7%), and doctoral degree (1.4%); the groups did not differ by highest level of education, χ2(8) = 8.42, p = .394. Mean age was 31.2 years (SD = 11.3) in the DEP group, 28.0 years (SD = 9.5) in the GAD group, and 28.5 years (SD = 11.0) in the comparison group; mean age did not differ between groups, F(2, 219) = 234.77, p = .128. The gender ratio (F/M) was 59/20 in the DEP group, 62/10 in the GAD group, and 52/19 in the comparison group, and the groups did not differ with respect to gender ratio, χ2(2) = 4.19, p = .123.
Design
The study employed a quasi-experimental correlational design. Three groups (DEP, GAD, healthy comparison) completed two measures of interpretation bias; self-report questionnaires of anxiety, depression, worry, and rumination; and a behavioral repetitive-negative-thinking task in which participants reported negative thought intrusions. We examined associations between scores on the measures of interpretation bias and levels of worry and rumination as well as number of negative thought intrusions (controlling for anxiety and depression symptoms) and compared the groups on their interpretation-bias scores. As scales on both interpretation-bias measures ranged from negative interpretations to positive interpretations, the measures were scored such that low scores reflected a more negative interpretation bias.
Materials and measures
Interpretation-bias measures
The SST (adapted from Wenzlaff & Bates, 1998, 2000) involves using five of six words, presented in a random order, to produce the first grammatically correct sentence that comes to mind. This sentence, by the nature of the task, can be either positive or negative in valence. Participants were each presented with 20 scrambled sentences; half the sentences were selected to relate to depressive rumination (taken from Wenzlaff & Bates, 1998, 2000), and half were generated by the authors to relate to anxiety and worry (in a series of validation studies, the worry-related items were found to have excellent internal consistency and split-half reliability; Krahé, Meeten, et al., in prep). An example worry-related sentence was “easy job hard finding a is,” which could be unscrambled to form the sentence “finding a job is easy” (positive interpretation) or “finding a job is hard” (negative interpretation). An example item for the rumination-related sentences was “myself in disappointed am confident I,” which could be unscrambled to make the sentence “I am confident in myself” (positive interpretation) or “I am disappointed in myself” (negative interpretation). Participants were randomly assigned to complete one of two sets of mixed worry- and rumination-related items. There was no difference in interpretation bias between sets, t(219) = −0.21, p = .836, 2 and no interaction between group and set, χ2(2) = .29, p = .867, and thus we collapsed the data across sets for analyses. Participants were required to “unscramble” as many of the 20 sentences as possible within 5 min while holding in mind a string of six digits (serving as a cognitive load; see Wenzlaff & Bates, 1998, 2000), which they were asked to recall at the end of the task. An overall SST index was calculated for each participant by dividing the number of positive sentences generated by the overall number of grammatically correct sentences generated. Thus, the index ranged from 0 to 1, with lower scores indicating a more negative interpretation bias. The SST was scored in this direction to be consistent with Hirsch et al. (2018).
The RT (adapted from Mathews & Mackintosh, 2000) involves rating the similarity of statements to previously presented scenarios. It consists of two phases: In the first phase, participants read 20 ambiguous scenarios and completed a comprehension question after each one. For example, participants saw the following scenario: The car park It is late at night and you are in a multistory car park trying to find your car. You have been looking for about 10 minutes and still cannot find it. You hear a noise behind you and see a shadow of something. Question: Did you find your car right away? (Correct answer: No)
In the second phase, participants were presented with four statements per previously seen scenario and were asked to rate how similar in meaning these statements were to the original scenario on a scale from 1 (very different in meaning) to 4 (very similar in meaning). Two statements were target statements relating to the ambiguity in the scenario, one describing a positive disambiguation and one describing a negative disambiguation of the scenario. The other two statements were foils unrelated to the ambiguity (again one was positive and one was negative) and were included as filler items only. For example, the above scenario was presented with the following statements:
You see a security person approaching to help you. (Positive target)
You see someone coming toward you looking threatening. (Negative target)
You see some money on the floor and pick it up. (Positive foil)
You see that you have forgotten your ticket and will have to pay a fine. (Negative foil)
Participants were randomly assigned to complete one of three sets of items; there was no difference in interpretation bias between sets, F(2, 217) = .54, p = .583 (see Note 2), and thus we collapsed the data across sets for analyses. A RT index was computed for each participant by subtracting mean similarity ratings for negative targets from mean similarity ratings for positive targets. Thus, lower scores denoted greater similarity ratings to negative versus positive targets, namely, a more negative interpretation bias. 3
Worry and rumination measures
Worry was measured using the 16-item Penn State Worry Questionnaire (PSWQ; Meyer, Miller, Metzger, & Borkovec, 1990; example item: “I am always worrying about something”). Items were rated on a scale from 1 (not at all typical of me) to 5 (very typical of me) and summed (after reverse-scoring appropriate items) to produce an overall score, with higher scores denoting greater worry. Rumination was assessed using the 22-item ruminative-response scale (RRS; Nolen-Hoeksema & Morrow, 1991; example item: [how much do you generally] “think about how sad you feel”). Items were rated on a scale from 1 (almost never) to 4 (almost always) and summed; higher scores denoted greater rumination. Cronbach’s αs in the present study were .93 for the PSWQ and .92 for the RRS. Both the PSWQ (Meyer et al., 1990) and the RRS (Just & Alloy, 1997) have been shown to have good test–retest reliability.
Depression and anxiety symptoms
We used the nine-item PHQ-9 (Kroenke & Spitzer, 2002) and the seven-item GAD-7 (Spitzer, Kroenke, Williams, & Löwe, 2006) to measure depression and anxiety symptoms, respectively, in the past 2 weeks (example item for depression: “Feeling down, depressed, or hopeless?”; example item for anxiety: “Feeling nervous, anxious, or on edge?”). On each measure, items were rated on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day), and responses were summed to give the overall score, with higher scores denoting greater depression/anxiety symptoms. Cronbach’s αs were .83 for the PHQ-9 and .91 for the GAD-7.
Behavioral repetitive-negative-thinking task
The behavioral repetitive-negative-thinking task is a state measure of negative thought intrusions, which often initiate a period of repetitive negative thinking, and can be seen as a more behavioral proxy for streams of worry and rumination than self-report questionnaires. On the basis of the original breathing-focus task/worry task, which has been used widely in past research (Hayes et al., 2010; Hirsch et al., 2009, 2013; Ruscio & Borkovec, 2004), participants focused on their breathing for 5 min and indicated at randomly cued intervals whether they were focusing on their breathing or experiencing a thought intrusion, which they then categorized as negative or otherwise (neutral, positive). Participants then identified a salient current or past worry (GAD group) or rumination (DEP group) topic; the healthy comparison group chose either worry or rumination, depending on what they felt was dominant for them on the day. After discussing this topic briefly with the experimenter, participants were asked to silently worry/ruminate about the topic in their usual manner for 5 min while the experimenter left the room. This repetitive-negative-thinking induction was designed to activate worry/rumination and was followed by another 5-min breathing-focus period, with sampling as before. The outcome measure was the mean number of negative thought intrusions reported per time period (before or after worry/rumination induction).
Procedure
Participants took part in one experimental session lasting approximately 1 hr. Questionnaire measures were completed online within 24 hr before the session, and diagnosis/diagnostic status was confirmed by administering the GAD and depression modules of the SCID either at a screening phone call before the session or as a screener at the beginning of the session. Participants provided informed consent and completed the SST, RT, and behavioral repetitive-negative-thinking task, in this order. Clinical participants subsequently completed further tasks, which are not reported here. Ethical approval was granted by the ethics committee of the authors’ university. The study was carried out in accordance with the World Medical Association Declaration of Helsinki.
Statistical analyses
All analyses were carried out in Stata (Version 14; StataCorp, College Station, TX). We initially computed correlations between the questionnaire measures and examined group differences on these measures. To investigate our first hypothesis that interpretation bias would be associated with levels of worry and rumination, we examined correlations between interpretation bias, as measured by SST and RT, and each form of repetitive negative thinking. To see whether negative thought intrusions were predicted by interpretation bias, we specified multilevel models, given that breathing-focus period (Level 1) was nested within individuals (Level 2). For SST and RT separately, we specified a model with number of negative thought intrusions as the outcome variable, and interpretation-bias score, breathing-focus period (before vs. after worry/rumination induction), and their within-level interaction as predictors. Furthermore, to check that associations were not explained by anxiety and depression symptoms, we conducted regression analyses (with bootstrapped standard errors in the case of nonnormally distributed data) with interpretation-bias score as the outcome variable, worry and rumination scores as predictor variables, and controlled for anxiety and depression symptoms. For negative thought intrusions, we reran the above analysis and controlled for anxiety and depression symptoms. Second, to examine whether clinical groups showed a more negative interpretation bias than the healthy comparison group, regression analyses were carried out with interpretation-bias score as the outcome variables and group (three levels: DEP, GAD, healthy comparison) as categorical predictor variable. Wald tests (χ2) were conducted to test linear hypotheses about the parameters of the model. Sidak-corrected pairwise comparisons as well as one-sample t tests were used to follow up group differences.
Results
Descriptive statistics, correlations, and group differences
Mean questionnaire scores by group are presented in Table 1. Mean scores for worry and rumination in the clinical groups were high and similar to previous studies with clinical populations (e.g., Fresco, Mennin, Heimberg, & Turk, 2003; Pearson, Brewin, Rhodes, & McCarron, 2008; Rimes & Watkins, 2005). Overall, worry, rumination, anxiety, and depression were significantly moderately to strongly correlated with each other (see Table 1). Furthermore, higher levels of worry (r = .52, p < .01) and rumination (r = .55, p < .01) were significantly correlated with a greater number of negative thought intrusions on the behavioral repetitive-negative-thinking task (averaged across both time periods 4 ). Comparing questionnaire scores among groups, both clinical groups had significantly higher levels of worry, rumination, depression, and anxiety symptoms than did the healthy comparison group (see Table 1). Furthermore, the depressed group reported higher levels of trait rumination than did the GAD group, whereas the GAD group reported higher levels of trait worry than did the depressed group. The depressed group reported higher levels of depressive symptoms than did the GAD group, but the two clinical groups did not differ from each other in terms of self-reported anxiety symptoms.
Descriptive Statistics and Correlations for Self-Report Questionnaires and ANOVA Results for Group Differences
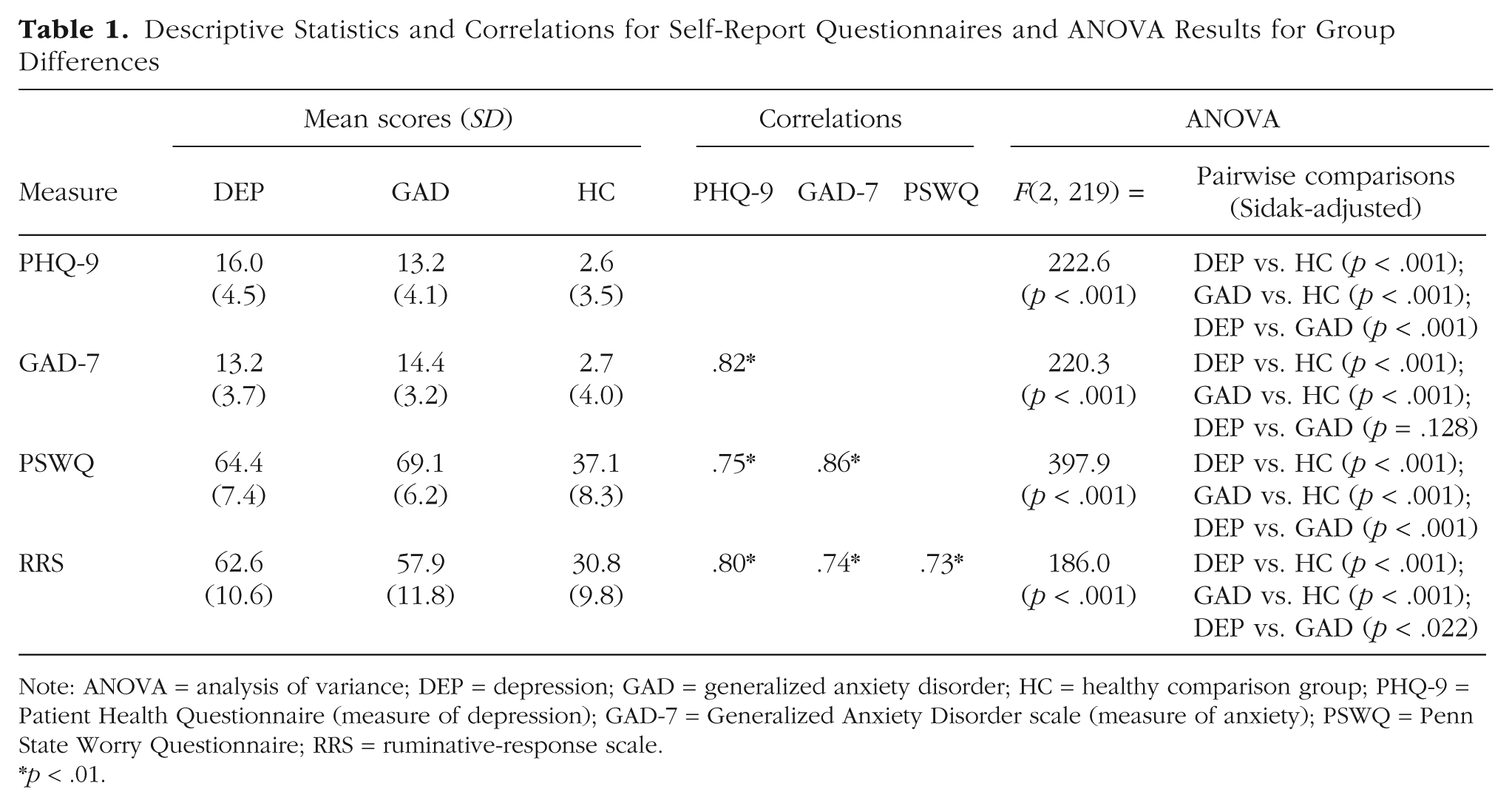
Note: ANOVA = analysis of variance; DEP = depression; GAD = generalized anxiety disorder; HC = healthy comparison group; PHQ-9 = Patient Health Questionnaire (measure of depression); GAD-7 = Generalized Anxiety Disorder scale (measure of anxiety); PSWQ = Penn State Worry Questionnaire; RRS = ruminative-response scale.
p < .01.
Are levels of worry and rumination associated with a more negative interpretation bias?
The two interpretation-bias measures were significantly moderately correlated (r = .52, p < .01). On the SST, 1 person was excluded for failing to complete any grammatically correct sentences, leaving N = 221 for this analysis. For the SST, both levels of worry (r = −.72, p < .01) and rumination (r = −.68, p < .01) were significantly strongly negatively correlated with SST index (Fig. 1a), indicating that higher levels of worry and rumination were associated with a more negative interpretation bias (i.e., more negative interpretations generated). When controlling for anxiety and depression symptoms, both worry (b = −0.005, bootstrapped SE = .00, p < .001, 95% confidence interval, or CI = [–0.008, –0.002]) and rumination (b = −0.003, bootstrapped SE = .00, p = .009, 95% CI = [–0.006, –0.001]) predicted SST index, with higher levels of worry and rumination predicting more negative interpretations. Adding the two critical variables (i.e., worry and rumination) into the model containing the covariates (anxiety and depression) explained a further 5.6% of the variance (p < .001; both worry and rumination predicted unique additional variance); the full model explained 58.0% of the variance. Furthermore, SST index predicted negative thought intrusions reported by participants (b = −4.65, SE = .55, p < .001, 95% CI = [–5.72, –3.58]), in that more negative interpretations (a lower score) predicted more negative thought intrusions. 5
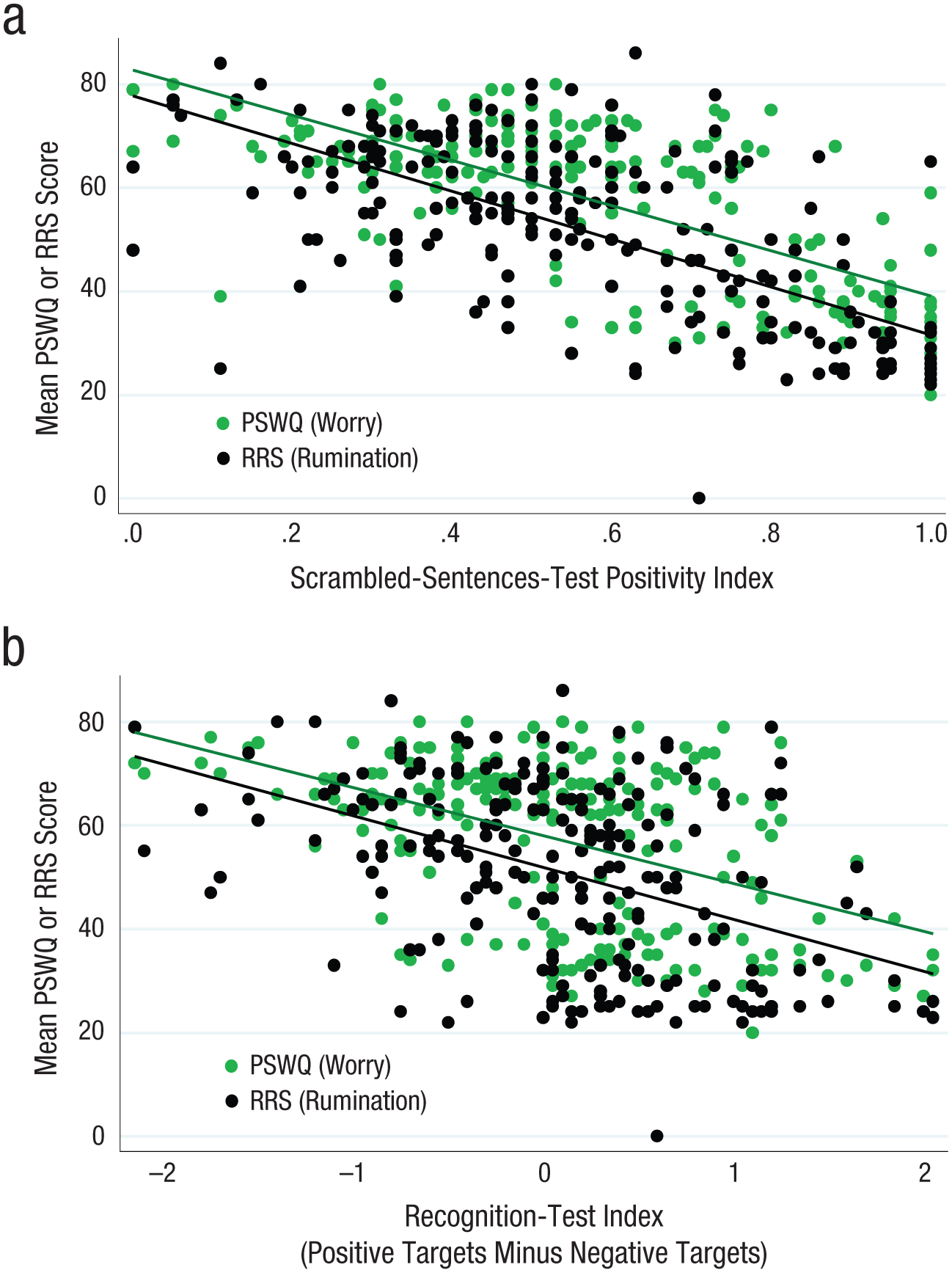
Scatterplots (with best-fitting regression lines) showing the association between (a) the scrambled-sentences-test positivity index and (b) the recognition-test index and two measures of negative thinking: scores on the Penn State Worry Questionnaire (PSWQ) and scores on the ruminative-response scale (RRS).
On the RT, 2 participants failed to complete the task correctly, leaving N = 220 for this analysis. As on the SST, on the RT, both levels of worry (r = −.46, p < .01) and rumination (r = −.44, p < .01) were significantly moderately negatively correlated with RT index, again indicating that higher levels of worry and rumination were associated with a more negative interpretation bias (Fig. 1b). When controlling for anxiety and depression symptoms, both worry (b = −0.013, SE = .01, p = .028, 95% CI = [–0.025, –0.001]) and rumination (b = −0.016, SE = .00, p = .001, 95% CI = [–0.025, –0.006]) predicted RT index, and higher worry and rumination scores predicted lower RT index (i.e., more negative than positive interpretations). Adding worry and rumination into the model containing anxiety and depression symptoms explained a further 7.1% of the variance (p < .001; again, both worry and rumination predicted unique additional variance); the full model explained 25.5% of the variance. Furthermore, RT index predicted the number of negative thought intrusions reported by participants (b = −1.10, SE = .19, p < .001, 95% CI = [–1.48, –0.72]), in that a lower index score (more negative interpretations) predicted more negative thought intrusions. 6
Thus, confirming our hypothesis, we found moderate to strong associations between a more negative interpretation bias and higher levels of worry, rumination, and negative thought intrusions, which were not accounted for by anxiety and depression symptoms.
Do individuals with GAD or depression make more negative interpretations than individuals without these disorders?
On the SST, group significantly predicted SST index, χ2(2) = 240.30, p < .001. Marginal means are presented in Figure 2a. Follow-up Sidak-corrected pairwise comparisons showed that both the DEP group and the GAD group had significantly lower scores (i.e., made significantly more negative interpretations) than the comparison group (both ps < .001) but did not differ from each other (p = .895). Thus, the two clinical groups showed a greater negative interpretation bias compared with the healthy comparison group. On the RT, group significantly predicted RT index, F(2, 217) = 30.83, p < .001; marginal means are presented in Figure 2b. Akin to the SST, follow-up Sidak-corrected pairwise comparisons showed that both the DEP group and the GAD group had significantly lower RT scores (i.e., made more negative than positive interpretations) than the healthy comparison group (both ps < .001). The two clinical groups did not differ significantly from each other (p = .058). However, although the DEP group’s mean score did not differ significantly from 0 (i.e., the midpoint of the scale), one-sample t(76) = −0.12, p = .908, the GAD group’s mean score did differ significantly from 0 in the negative direction, one-sample t(71) = −3.51, p < .001. Overall, the two clinical groups showed a more negative interpretation bias than the healthy comparison group on both measures of interpretation bias, which was consistent with our hypothesis.
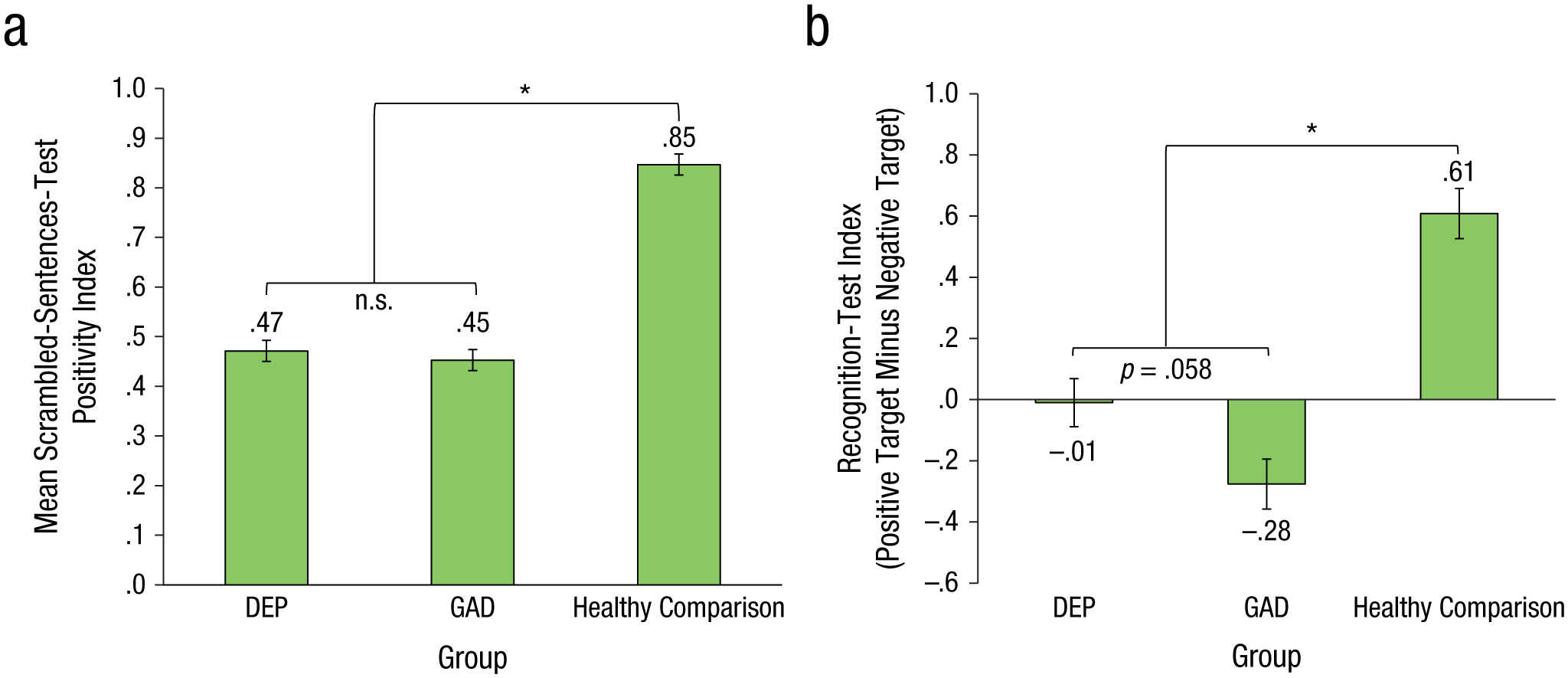
Results for (a) the scrambled-sentences-test index and (b) the recognition-test index. Error bars indicate ± 1 SEM (bootstrapped for SST). DEP = depression; GAD = generalized anxiety disorder. Asterisks indicate a significant difference between groups (p < .001).
Discussion
This cross-sectional study examined the association between interpretation bias and two types of repetitive negative thinking—worry and rumination—in a large sample of individuals with either GAD, depression, or without either disorder. In support of our hypotheses, we found that across groups, a more negative interpretation bias was moderately to strongly associated with repetitive negative thinking, that is, with higher levels of worry, rumination, and negative thought intrusions (a behavioral proxy of streams of repetitive negative thinking). As well as this linear relationship, we found that individuals with a diagnosis of GAD or depression displayed a significantly more negative interpretation bias compared with the healthy comparison group; in particular (discussed in more detail below), they appeared to lack the positive interpretation bias displayed in the healthy comparison group. Together, these findings provide compelling and novel evidence for a clear association between negative interpretation bias and both worry and rumination as assessed by self-report questionnaires and a more behavioral measure of thought intrusions. To our knowledge, this is the first study to establish the association between interpretation bias and both worry and rumination within the same study and the first to examine the link between interpretation bias and worry and rumination in clinical samples. Thus, it bridges an important gap in the current literature. It demonstrates that different forms of repetitive negative thinking may be characterized by shared cognitive processes and also examines these processes in groups with pathological levels of repetitive negative thinking (as we discuss in more detail below).
Worry and rumination share common features. Both are characterized by negative and repetitive thoughts and a perceived lack of control (see Kircanski et al., 2015). However, they also differ in aspects such as temporal orientation. Worry seems more future-oriented, whereas rumination is more present- or past-focused (Kircanski et al., 2015; Watkins et al., 2005). In the current study, we aimed to better understand whether worry and rumination may both be underpinned by the same cognitive mechanisms. To do this, we measured levels of worry and rumination using separate questionnaire measures and looked at their relationship with interpretation bias. Interpretation bias appears to operate similarly in both worry and rumination because interpretation bias was related to both worry and rumination—to the same degree—and furthermore, this was evident on two separate measures of interpretation bias (the SST and RT; see Fig. 1). Although we examined this association cross-sectionally, the current findings are in line with theoretical accounts positing that interpretation bias may play a role in the maintenance of worry (Hirsch & Mathews, 2012) and extend these to provide further evidence that rumination is also associated with interpretation bias. Furthermore, these findings indicate that worry and rumination may share interpretation bias as a common cognitive process and highlight similarities between these forms of repetitive negative thinking. However, it should be noted that although worry and rumination were strongly correlated with each other and showed the same pattern of results with regard to their relationship with interpretation bias, both worry and rumination also predicted unique variance in SST and RT scores.
The present study also demonstrated that interpretation bias was more pronounced in individuals with pathological levels of worry and rumination (i.e., those with GAD and depression) compared with individuals without these disorders. These findings were apparent when controlling for anxiety and depression symptoms, indicating that clinical status or level of impairment alone could not explain these results. Rather, clinical participants with GAD (vs. subclinical participants) report more negative thought intrusions and a reduced ability to stop such thoughts (Hirsch et al., 2013). It should be noted that we excluded participants with recent self-harm and high levels of suicidal ideation. Although future research could be more inclusive, our mean PHQ-9 score in the depression group was 16, which is well above the threshold for caseness (a score of 10; Gyani, Shafran, Layard, & Clark, 2013). We thus believe that our results still generalize to many individuals with GAD or depression.
The clinical groups did not differ from each other in terms of their level of interpretation bias. This lack of a difference again points to interpretation bias playing a similar role in relation to both worry and rumination in individuals with clinical disorders characterized by high levels of these forms of repetitive negative thinking. Given that repetitive negative thinking is prevalent across a range of disorders (see Ehring & Watkins, 2008) and proposed to operate transdiagnostically, we do not argue that the association between interpretation bias and worry and rumination is limited to GAD and depression. Indeed, we found this association across all groups, including the healthy comparison group. Rather, we chose GAD and depression because worry and rumination are hallmark features of these disorders. To this end, we recruited participants with either GAD or depression. Both groups had high levels of worry and rumination (compared with a healthy comparison group). However, in line with the view that worry is particularly problematic in GAD and rumination in depression, our results showed that participants with GAD reported even higher levels of worry than participants with depression, and vice versa for rumination. This is the first study to demonstrate a link between interpretation bias and both worry and rumination within the same study; future studies could now extend this to include participants with comorbid GAD and depression and diagnoses other than depression or GAD in which repetitive negative thinking occurs. The present research lays the groundwork for such future studies.
Although GAD and depressed groups did not differ significantly from each other in terms of degree of negative interpretation bias, results on the RT, in which a score of 0 denotes an equal number of positive and negative interpretations made (see Fig. 2), showed that the depressed group scored close to 0, whereas the GAD group had a more negative score, which differed significantly from 0. This may indicate that the depressed group showed a lack of the positive interpretation bias seen in the healthy comparison group, whereas the GAD group displayed a more negative bias than the healthy comparison group, although the difference between the two clinical groups was not significant. A lack of the positive bias seen in healthy samples, rather than an overtly negative bias, has been found in other emotional disorders such as social anxiety disorder (Amir, Prouvost, & Kuckertz, 2012; Hirsch & Mathews, 2000). Tasks such as the RT, which have a midpoint (equal positive/negative interpretations), may be useful for further untangling whether participants display a lack of a positive bias or the presence of a negative interpretation bias in future studies.
In the present study, we used two offline measures of interpretation bias that allowed for reflection on the ambiguous material (though not completely time unlimited, in the case of the SST) rather than online measures in which participants make speeded responses to index interpretations that are generated at the time the ambiguity is first encountered (e.g., Hirsch & Mathews, 2000; see Hirsch et al., 2016, for a detailed discussion of offline vs. online measures). Although offline tasks are widely used, an advantage of combining them with online tasks is the ability to examine interpretations generated at the moment at which information is first encountered rather than just interpretations made after having had an opportunity for reflection. Thus, using both kinds of task in future research could tell us whether resolving ambiguity is a more automatic or more reflective process. For example, in the present study, we were unable to assess whether participants made both positive and negative interpretations and then rejected one in favor of the other or whether participants made only the interpretation they endorsed on our measures.
A limitation of our study was its cross-sectional nature. Although interpretation bias was strongly related to worry, rumination, and negative thought intrusions, in the present study, we cannot draw any conclusions regarding whether it plays a causal role in maintaining these forms of repetitive negative thinking. However, research using “cognitive bias modification” paradigms to train a certain interpretive style has found that changing interpretation bias may lead to corresponding changes in worry (Hayes et al., 2010; Hirsch et al., 2009) and rumination (Hertel et al., 2014, Experiment 2), supporting a causal link between interpretation bias and repetitive negative thinking and indicating that interpretation bias is not a result or concomitant of worry and rumination. Indeed, the longer term effects of changing interpretation bias on worry and rumination are now being explored (Hirsch et al., 2018, 2019; Krahé, Mathews, Whyte, & Hirsch, 2016). Nevertheless, this article provides novel and much needed cross-sectional evidence for the relationship between interpretation bias and levels of both worry and rumination and constitutes the first study in adults to demonstrate that worry is correlated with negative interpretation bias.
Further strengths of the present study were the large sample of clinically anxious and depressed participants recruited, the use of two separate interpretation-bias measures, and that we assessed the relationship between interpretation bias and both worry and rumination within the same study. Of the different forms of repetitive negative thinking, worry and rumination are perhaps most similar. In future research, it thus would be interesting to investigate whether interpretation bias is also related to other forms of repetitive negative thinking that involve more mental imagery, such as obsessions and intrusive memories.
We focused on interpretation bias as one cognitive process posited to maintain worry and rumination, but this process is thought to operate in interaction with other biases (see the combined-cognitive-biases hypothesis; Hirsch, Clark, & Mathews, 2006) as well as levels of attentional control and types of mentation style (Hirsch & Mathews, 2012). Thus, future research could assess the interplay between interpretation bias and other cognitive processes (e.g., attentional biases and memory biases). The SST may be a useful task in this regard. It can be adapted to yield also measures of attentional bias (whether participants initially attend to the negative or positive word) and memory bias (recall of constructed sentences), alongside interpretation bias (see Everaert et al., 2014). This adapted form of the task could therefore be employed to study how different cognitive processes might interact in relation to both worry and rumination.
In conclusion, the present study found that negative interpretation bias was moderately to strongly associated with worry and rumination. Furthermore, individuals with pathological levels of worry and rumination, namely, those with a diagnosis of GAD or depression, displayed a more negative interpretation bias than individuals without these disorders (i.e., lacked a positive bias seen in healthy individuals). Together, these findings provide novel support for a relationship between interpretation bias and maladaptive repetitive negative thinking.
Footnotes
Acknowledgements
We are grateful to Josh Graham, Amy Steele, Alice Pisoni, and Grâce Bomboko for their help in recruitment and data collection for this study. C. Krahé is now at the Department of Psychological Sciences, University of Liverpool. The views expressed are those of the authors and not necessarily those of MQ: Transforming Mental Health, the NHS, the National Institute for Health Research (NIHR), or the Department of Health.
Action Editor
Christopher G. Beevers served as action editor for this article.
Author Contributions
C. Krahé and C. R. Hirsch designed the study. Testing and data collection were performed by J. Whyte, L. Bridge, and S. Loizou. Data analysis was performed by C. Krahé, and C. Krahé and C. R. Hirsch drafted the manuscript. All the authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Funding
This work was supported by MQ: Transforming Mental Health PsyIMPACT Grant MQ14PP_84 (to C. R. Hirsch). C. R. Hirsch receives salary support from the National Institute for Health Research (NIHR), Mental Health Biomedical Research Centre at South London, and the Maudsley NHS Foundation Trust and King’s College London.