
Abstract
This study examined whether perceived attachment security (i.e., perceptions of caregivers as responsive, available, and open to communication during times of need) and effortful coping work in concert to buffer against uncontrollable life event effects on hypothalamic–pituitary–adrenal axis (HPA) response patterns in preadolescent boys and girls (N = 121, mean age = 10.60 years). Children completed the Trier Social Stress Test (TSST) and were immediately thereafter exposed to one of two randomly assigned coping conditions: distraction and avoidance. Piecewise growth multilevel modeling of children’s salivary cortisol levels over the course of the experimental protocol suggested that uncontrollable life events in the year prior were associated with exaggerated cortisol reactivity, though this pattern was buffered against by children’s secure attachment beliefs. Furthermore, perceived attachment security, uncontrollable life event, and coping condition interactive effects on cortisol recovery emerged. As expected, distraction supported efficient cortisol recovery for those uncontrollable stress-exposed children with secure beliefs, and avoidance worked in this fashion for those with insecure beliefs. Findings point to perceived attachment security as a putative buffer of stress-exposed preadolescents’ HPA reactivity and possible contributor to regulatory fit, informing how specific coping skills work or backfire in supporting these children’s HPA recovery efficiency.
The deleterious effects of being exposed to excessive uncontrollable life events (hereafter referred to as stress; e.g., divorce, job loss, violent crime) on children’s mental-health outcomes (e.g., internalizing psychopathology) are well known (Evans & Kim, 2013). Evidence increasingly implicates stress-related damage to the hypothalamic–pituitary–adrenal axis (HPA) as a biological mechanism of risk in stress–illness linkages (Koss & Gunnar, 2018; Shonkoff, Boyce, & McEwen, 2009). Thus, the identification of protective factors that also get “under the skin” has become critically salient. Children’s coping may be one such factor as it contributes to the efficient recovery of stressor-induced salivary cortisol (sC, an HPA biomarker) activation (Wadsworth et al., 2018). However, evidence also suggests that this HPA buffering effect depends on regulatory fit, or the degree to which strategies children use match their individual-level characteristics and the coping resources available in their environments (Bendezú, Perzow, & Wadsworth, 2016; Bendezú & Wadsworth, 2017). If coping works differently at the physiologic level for different children in different contexts (Wadsworth, 2015), then research must further disentangle for whom and under what conditions specific strategies work or backfire in helping children manage stress. Progress toward this aim will help guide development of maximally beneficial person-centered interventions for stress-exposed families.
One coping resource and potential contributor to regulatory fit is perceived attachment security, or children’s views of a caregiver as responsive, available, and open to communication in times of need (Ainsworth, 1990; Bowlby, 1982). These beliefs about the dependability of care promote adaptive patterns of approach (i.e., desire to explore, engage) and avoidance (i.e., desire to seek safety) behaviors in the face of stressors (Cassidy & Shaver, 2008). For stress-exposed preadolescents, which coping skills help them manage rather than exacerbate stress may depend on whether strategies align with these beliefs; for example, is it safer to approach (“I will be cared for”) or avoid (“I am not sure I will be safe”)? This proposition has yet to be tested at the physiologic level of analysis, which may be important given the role biological wear and tear plays in stress-illness pathways. The current study examined the interactive contribution of perceived attachment security and effortful coping to children’s cortisol recovery efficiency following a laboratory stressor in a sample of preadolescents with varying levels of recent stress exposure.
Preadolescence may be an important developmental period for examining the putative physiologic benefits of children’s secure attachment beliefs. Attachment security develops during the infant and toddler years when children are largely dependent on responsive caregivers to meet their basic needs (e.g., comfort when distressed; Bowlby, 1982). As they age into preadolescence, increased independence from caregivers is accompanied by the expectation that children begin to manage stressors in numerous domains (e.g., academic, interpersonal) on their own (Spear, 2010). Uncontrollable life events, however, occur outside a child’s sphere of influence and are therefore often quite difficult for preadolescents to cope with in an independent, active manner (Gaylord-Harden, Elmore, Campbell, & Wethington, 2011; Wadsworth & Compas, 2002). Consensus that uncontrollable stressors most affect the developing HPA lends credence to this claim (Dickerson & Kemeny, 2004). Emerging evidence, however, also suggests that the brain and body are particularly malleable and amenable to protective factors during preadolescence (Steinberg, 2015), making it an opportune age for studying the benefits to HPA functioning afforded by coping and secure attachment beliefs.
Knowing that a caregiver is readily available to provide external support may buffer against stress-related dysregulation of HPA response patterns (e.g., cortisol hyperreactivity), those shown to confer risk for psychopathological development (e.g., internalizing; Lopez-Duran, Kovacs, & George, 2009). For preadolescent children, both observed attachment quality during infancy and the physical presence of a caregiver during early adolescence have been shown to longitudinally and concurrently predict less exaggerated cortisol reactivity in response to laboratory stressors (Fearon et al., 2017; Gunnar & Hostinar, 2015; Spangler & Zimmerman, 2014). However, little is known about preadolescent attachment representation to cortisol reactivity associations (e.g., Cameron et al., 2017). We address this gap by examining perceived attachment security. This developmentally sensitive assessment modality is consistent with Bowlby’s (1982) assertion about the internalized nature of attachment security at this age, when children become more autonomous and caregivers’ direct physical presence becomes less necessary (Allen & Miga, 2010; Moretti & Peled, 2004). It also capitalizes on emerging metacognitive and self-reflective capacities that make preadolescents increasingly adept reporters of internal states and aspects of parent–child relationships (Kerns, Klepac, & Cole, 1996; Seiffge-Krenke, 1995). Addressing these knowledge gaps may identify those children who benefit most at the physiologic level of analysis from beliefs that predictable support from a responsive caregiver is available when needed most (e.g., in the face of uncontrollable stress exposure).
An additional manner by which perceived attachment security may buffer against dysregulated HPA responses is by supporting preadolescents’ capacity to cope. Indeed, although children are thought to develop their capacity for effortful coping in the context of a relationship with an adult caregiver (Gunnar, 2017; Schore & Schore, 2008), it remains to be seen whether internalized aspects of this relationship (e.g., attachment security) exert influence on effective coping, or how successful different forms of coping (e.g., distraction, avoidance) are in helping children manage acute stress response physiology (e.g., HPA). Recent accounts of children’s coping as functional adaptation to context posit that coping is shaped by the affordances and demands of nurturing and inhospitable rearing contexts and works to help align child and environmental systems in service of growth and development (Blair & Raver, 2012; Del Giudice, Ellis, & Shirtcliff, 2011; Wadsworth, 2015). Thus, stress-exposed children with secure attachment beliefs may benefit most from and use approach-oriented coping skills involving exploration (e.g., social or behavioral coping resource seeking) and reengagement with the environment (e.g., distraction) because their internalized assuredness of care supports the view that it is safe to do so.
Conversely, stress-exposed children with insecure attachment beliefs may benefit most from and consequently use withdrawal-oriented coping skills involving isolation (e.g., compulsive self-reliance) and disengagement from the environment (e.g., avoidance) because their internalized uncertainty about the provision of care supports the view that self-related coping is perhaps the safest course of action. Furthermore, if effective coping is more about the usage of strategies that improve person-context match and less about the blanket use of universally “positive” and “negative” strategies, then these different forms of coping should prove to be similarly effective at buffering dysregulated, risk-linked HPA responses (e.g., protracted recovery; Ji, Negriff, Kim, & Susman, 2016; Shull et al., 2016) if and when each is understood to optimize regulatory fit between the child and the demands of their environment.
To test this supposition, we exposed preadolescent boys and girls to the Trier Social Stress Test (TSST) and then to one of two randomly assigned coping conditions immediately thereafter: distraction (e.g., children encouraged to explore toys, art supplies, and musical instruments) and avoidance (e.g., children in plain room instructed to “Try your best not to think about your TSST performance”). Distraction generally helps children consciously reengage attention to soothing activities, whereas avoidance tends to inadvertently refocus attention to the source of stress (Compas, Connor-Smith, Saltzman, Thomson, & Wadsworth, 2001). Thus, children invited to distract should show greater cortisol recovery efficiency relative to those told to avoid following the TSST protocol. However, given that stressors activate the attachment system and may therefore color children’s perception about the safety of approach- and withdrawal-oriented coping options (Skinner & Zimmer-Gembeck, 2016), we expected coping condition effects to vary as a function of stress-exposed children’s attachment representations. Specifically, knowing a caregiver is available and open to communication in times of need may help children feel safe while exploring environments for appropriate, alternate activities (e.g., seeking coping resources; Zimmer-Gembeck et al., 2017). These secure beliefs may also free up otherwise stress-constrained executive and attention control resources needed to become fully immersed in these activities once discovered (e.g., Bergin & Bergin, 2009; Fearon & Belsky, 2004; Moss & St-Laurent, 2001). Thus, stress-exposed children with secure beliefs may make more effective use of distraction (i.e., optimal regulatory fit), as evidenced by more efficient cortisol recovery patterns.
On the other hand, perceptions of a caregiver as unresponsive, unavailable, and closed off to communication when support is needed most may alter the function of distraction and avoidance in ways that challenge traditionally held assumptions about their utility. For stress-exposed children, insecure beliefs may support a view that coping resource seeking is unsafe and may provide them with evidence of their “unworthiness” for care if attempts to cope in an approach-related manner prove unsuccessful. To this end, approach-related distraction coping for stress-exposed children with insecure beliefs may reorient their attention to additional sources of stress (e.g., lack of safety, unworthiness of care) rather than reengage it in soothing activities. In addition, worry-related (e.g., “It is not safe to explore”) and depressogenic cognitions (e.g., “I am unworthy of support”) may concomitantly restrict access to executive and attention control resources requisite for focused distraction engagement should an alternate activity present itself (Clarke, Ungerer, Chahoud, Johnson, & Stiefel, 2002; Lewis, Feiring, & Rosenthal, 2000). In turn, stress-exposed children with insecure beliefs may display a limited capacity to effectively use distraction (i.e., poor regulatory fit), as evidenced by more protracted cortisol recovery patterns. Rather, these children may seek refuge and relief in avoidance because it is consistent with their doubts about the reliability of safety and support.
Given that the capacity for introspection begins to emerge at this age, it is also possible that the ruminative processes that accompany avoidance and ironically keep children engaged with a stressor may also inadvertently help children build a “mountain of evidence” that justifies, defends, and makes them feel right about avoidance as a coping option (Nolen-Hoeksema, Wisco, & Lyubomirsky, 2008). These claims are consistent with empirical evidence of the momentary benefits afforded by avoidance on cortisol recovery as well as mood repair in individuals with elevated negative thought processes (Bendezú et al., 2016; Fox, Toole, Franklin, & Hooley, 2017). Thus, stress-exposed preadolescents with insecure beliefs may more effectively use avoidance (i.e., optimal regulatory fit), as demonstrated by more efficient cortisol recovery patterning.
The current study tested the following predictions:
Hypothesis 1: Preadolescents with high recent stress exposure and insecure attachment beliefs will display more exaggerated cortisol reactivity relative to those with high stress exposure and secure attachment beliefs.
Hypothesis 2: Preadolescents with high recent stress exposure and insecure attachment beliefs will display more protracted cortisol recovery in the distraction condition and more efficient cortisol recovery in the avoidance condition.
Hypothesis 3: Preadolescents with high recent stress exposure and secure attachment beliefs will display more efficient cortisol recovery in the distraction condition and more protracted cortisol recovery in the avoidance condition.
We operationalize recent stress exposure as the number of parent-reported child-independent (i.e., not dependent on child behavior, uncontrollable) life events in the year before the study and perceived attachment security as youth-reported views of their maternal caregiver as responsive, available, and open to communication in times of need.
Method
Participants
Preadolescent children (N = 121; mean age = 10.60 years, SD = 0.68, age range = 9.01–12.06 years; 51.6% male) as well as a parent (90.1% mothers) were recruited from suburban schools in the northeastern United States. Median annual household income was $66,000.00 (income range = $13,638.84–$245,000.00). Most children (90.1%) and their parents (92.6%) identified as White. Other children and parents in the sample identified as Asian (children = 2.5%, parents = 1.7%), American Indian/Alaska Native (children = 1.7%, parents = 0.0%), African American (children = 0.8%, parents = 0.0%), other (children = 1.7%, parents = 0.0%), or declined to respond (children = 3.3%, parents = 5.8%).
Procedures
Parents enrolled their child and completed questionnaires online. Children were then scheduled to complete the 95-min in-person experiment between the hours of 3:00 p.m. and 5:30 p.m. Parents were instructed to have their children refrain from brushing their teeth and consuming a large meal, dairy, or sugary and acidic foods within the hour before study arrival. Saliva samples were collected via passive drool into vials at seven time points (T1–T7). On arrival, children rinsed their mouths with bottled water, and then an experimenter reviewed study procedures and obtained assent. Then, an initial saliva sample was collected (T1). Next, the experimenter administered questionnaires to the child for 40 min and then collected a second saliva sample (T2). Children were then video recorded while completing the TSST, a 15-min test that asked participants to prepare (5 min) and deliver (5 min) a speech and complete a mental subtraction task (5 min) in front of an unresponsive “panel of experts” (experts were confederates unknown to participants and unaware of their coping condition). Children were randomized within gender, and investigators were not privy to the results of this process. A third saliva sample was taken immediately after the TSST (T3).
Children were then taken to one of two randomly assigned coping condition rooms: a distraction room (n = 62), filled with musical instruments, art supplies, and toys in which they were prompted to play with the materials, or an avoidance room (n = 59), in which they were prompted to try not to think about the TSST. After 10 min, a fourth saliva sample was taken (T4). Children were then interviewed for 10 min about the coping strategies they used during and after the TSST. A fifth saliva sample was collected (T5). Next, children engaged in 10 min of guided progressive muscle relaxation (PMR). Then, a sixth saliva sample was collected (T6). Next, the experimenter administered any remaining questionnaires and invited the child to sit quietly for 10 min and continue to visualize the guided imagery from the relaxation exercise. Then, a final seventh saliva sample was collected (T7). Experimenters debriefed children after the experiment, and families received $50 compensation.
Measures
Salivary cortisol
Seven saliva samples were collected via passive drool (Davis, Bruce, & Gunnar, 2002), stored at −20 °C in a medical-grade ultra-low-temperature freezer, and transported on dry ice to the CORE Biomarker Lab at Penn State University (Salimetrics, LLC, State College, PA). Cortisol levels were determined using a commercial expanded-range, high-sensitivity enzyme immunosorbent assay kit (Assay 1-3002 or 1-3012; Salimetrics, LLC, State College, PA) that detects levels in the range of 0.003 to 3.0 kg/dl (range, 0.08–82.77 nmol/L). Cortisol extraction was run in duplicate and batched in the same order as random assignment. Given that sC levels decrease during the 40-min pre-TSST period (Abelson et al., 2014), T2 sC levels should best index baseline sC. Due to the delay in sC presence in saliva (De Kloet, Joëls, & Holsboer, 2005), T4 sC (25 min after the start of the TSST—indexing stress 5–10 min into the TSST) should index peak reactivity. Last, T5 sC (10 min after completion of coping condition), T6 sC (after debrief and PMR), and T7 sC should reflect sC in response to children’s coping efforts.
Recent stress exposure
Parents completed a modified version of the Child and Adolescent Survey of Experiences: Parent (CASE-P; Allen & Rapee, 2009). The CASE-P is a 38-item inventory of life events (e.g., changes in household, illnesses, separation from family, moves, experiencing or witnessing traumatic events, peer interactions, and school achievement) that potentially took place in the 12 months before interview. Given our focus on uncontrollable recent stress exposure, only life events that were classified by the measurement developers as occurring independent of a child’s behavior (n = 19; “My partner or I lost our job,” “Someone broke into our house”; Allen & Rapee, 2009) were used. 1 The CASE-P has demonstrated acceptable test–retest and interrater reliability and validity (Allen, Rapee, & Sandberg, 2012).
Perceived attachment security
Children completed the Security Scale (Kerns et al., 1996), a 15-item measure assessing children’s perception of attachment security in the mother–child relationship. The measure assesses children’s perceptions of their mother as responsive and available, their tendency to rely on her for help in the face of stress, and children’s ease of communicating thoughts and feelings to her. Children are initially asked to identify their biological mother or the first mother they can remember having (e.g., biological, step, foster, aunt, grandmother). Once identified, children rated one of two statements (e.g., “Some kids find it easy to trust their mom BUT other kids are not sure if they can trust their mom”) in each item as either sort of true for them or really true for them, a response format adopted by the measurement developers to minimize social desirability response biases. Items were scored from 1 to 4; higher scores indicated greater secure attachment. Items were averaged, and resulting scores demonstrated adequate internal consistency (α = .88).
Covariates
Given their established association with sC response, the following covariates were included in all analyses: child gender (0 = boy; 1 = girl), pubertal status (Stroud, Papadonatos, Williamson, & Dahl, 2011), medication use (Granger, Hibel, Fortunato, & Kapelewski, 2009), child internalizing symptoms (Lopez-Duran et al., 2009), and family income-to-needs ratio (INR; Evans & Kim, 2013). Parent-reported pubertal status was assessed using the Pubertal Development Scale (Petersen, Crockett, Richards, & Boxer, 1988). Female status was indexed by menarche, height, body hair growth, and breast growth (α = .71). Male status was indexed by voice changes, height, body-hair growth, and facial-hair growth (α = .34). 2 Medication use (e.g., medications known to affect sC activity) was scored for each child following suggestions outlined in Granger et al. (2009). Child-reported internalizing was assessed with the Behavior Assessment System for Children, Second Edition (BASC-2; Reynolds & Kamphaus, 2004). The Self Report of Personality–Child (SRP-C, ages 8–11) and Self Report of Personality–Adolescent (SRP-A, ages 12–21) are reliable and valid measures of psychopathology and behavior; internal consistency (α) ranged from .83 to .90 and .81 to .93 for the child and adolescent forms, respectively. T-scores with combined gender norms were used to ensure the integrity of the broadband scale scores. INR is an index of annual household income relative to national poverty norms. An INR of 1.00 indicates poverty, whereas middle-income status is indicated by an INR of 3.00. Median INR for the sample was 3.01.
Data analyses
Data reduction and preprocessing
A child participant whose age was atypical for fourth and fifth grade (n = 1, age = 7.13 years) and whose parent provided online information but child did not attend the 95-min in-person experiment (n = 1) were excluded. In the final sample (N = 121), 20 sC values were ±3 SD from the sample mean (T1 and T2 samples each had four outliers; T3 and T7 had three outliers each; T4, T5, and T6 had two outliers each). These values were winsorized to equal values 3 SD above or below the sample mean (Allwood, Handwerger, Kivlighan, Granger, & Stroud, 2011; Hostinar, Johnson, & Gunnar, 2015). 3 sC values remained positively skewed, and a fourth root transformation was applied to normalize sC data (Miller & Plessow, 2013). The ladder of transformations and Tukey’s rule of the bulge were used to identify suitable transformations for skewed predictors and covariates of interest (Mosteller & Tukey, 1977; Singer, Willett, & Willet, 2003). Log10, exponential, and ln transformations were sufficient to normalize skewed recent stress exposure, attachment security, and INR data, respectively.
Coping condition manipulation check
Children reported what they did in their coping rooms to feel better or improve the situation, even if they thought it did not work. Raters unaware of coping condition coded the free responses (yes or no) for distraction (e.g., “I drew a tiger and colored,” “I played with the keyboard and Legos”) and avoidance (and/or associated intrusive thoughts) strategies (e.g., “Tried to get the speech out my head,” “I was trying not to think about how I did but I kind of did anyways”; Wadsworth, 2013). Interrater reliability was established by comparing two raters’ coding of 20% free responses (κ = .91). The relationship between coping condition and reported strategies was significant, χ2(1, N = 119) = 58.76, p < .001, suggesting that children complied with the distraction (92%) and avoidance (78%) prompts.
Missing data
Missing value analysis was conducted for all key demographic and study variables in the current analysis. Little’s (1988) missing completely at random (MCAR) test was nonsignificant; χ2(134, N = 121) = 149.52, p = .17. Thus, the data could be MCAR. Markov chain Monte Carlo (MCMC) multiple imputation methods (PROC MI, SAS 9.3) were used to avoid power loss related to listwise deletion. 4 Ten imputations are recommended given 10% missing data and a willingness to tolerate a 1% power falloff (Graham, Olchowski, & Gilreath, 2007). Because only 3.36% of data values were missing, the standard five imputations were performed, which included all variables used in our analyses. Pooled parameter estimates were generated using PROC MIANALYZE in SAS (Version 9.3; The SAS Institute, Cary, NC).
Bivariate associations and multilevel models
Fisher’s Z-adjusted correlations controlling for child gender, pubertal status, family INR, medication use, and internalizing symptoms were used to examine bivariate associations. Preadolescents’ sC reactivity and recovery patterning was analyzed with piecewise growth multilevel model (MLM) techniques (PROC MIXED in SAS), using reactivity (T2–T4) and recovery (T4–T7) phase sample time as a Level 1 within-subjects factor and stress variables, coping condition (0 = avoidance, 1 = distraction), and all covariates (controlled for despite statistical nonsignificance) as Level 2 between-subjects factors. It is well known that physiological baseline levels can set the ceiling for peak reactivity and thus recovery (Berntson, Uchino, & Cacioppo, 1994; Burt & Obradović, 2012). Thus, a piecewise approach was adopted that permitted the concurrent modeling of sC baseline levels as well as reactivity and recovery patterning. Specifically, a linear reactivity-quadratic recovery piecewise growth model was used (e.g., Cudeck & Klebe, 2002; Llabre, Spitzer, Saab, & Schneiderman, 2001; MacMillan et al., 2009) with Kenward-Rogers corrected degrees of freedom. With the exception of coping condition (for ease of interpretation), all covariates and predictors in our cross-level interactions (Level 2 Between-Person Predictors × Level 1 Within-Person Growth Parameters) were grand-mean centered. The general form of our models was:









At Level 1, Equation 1a models within-child variation in sC response,
Results
Descriptive and bivariate statistics are shown in Table 1. Children’s sC levels were positively associated across time points. The number of child-independent life events reported by parents was commensurate with that reported in other community samples (Allen & Rapee, 2009; Kercher, Rapee, & Schniering, 2009). sC levels did not differ for children who did and did not take medication (all p > .24). Coping condition was not significantly associated with any study variable (all p > .11). In addition, children’s perceived stress ratings pertaining to preparing the speech, t(117) = −0.034, p = .973; delivering the speech, t(117) = −0.129, p = .898; and performing mental subtraction, t(116) = −0.264, p = .792, did not differ across coping conditions. With respect to predictor-covariate associations, perceived attachment security was positively associated with family INR, r = .20, p < .05, and negatively associated with internalizing symptoms, r = −.48, p < .05, respectively. Recent stress exposure was positively associated with internalizing symptoms, r = .23, p < .05. No other significant bivariate associations emerged.
Descriptives and Correlations for Child Recent Stress Exposure, Attachment Security, Coping Condition, and Salivary Cortisol
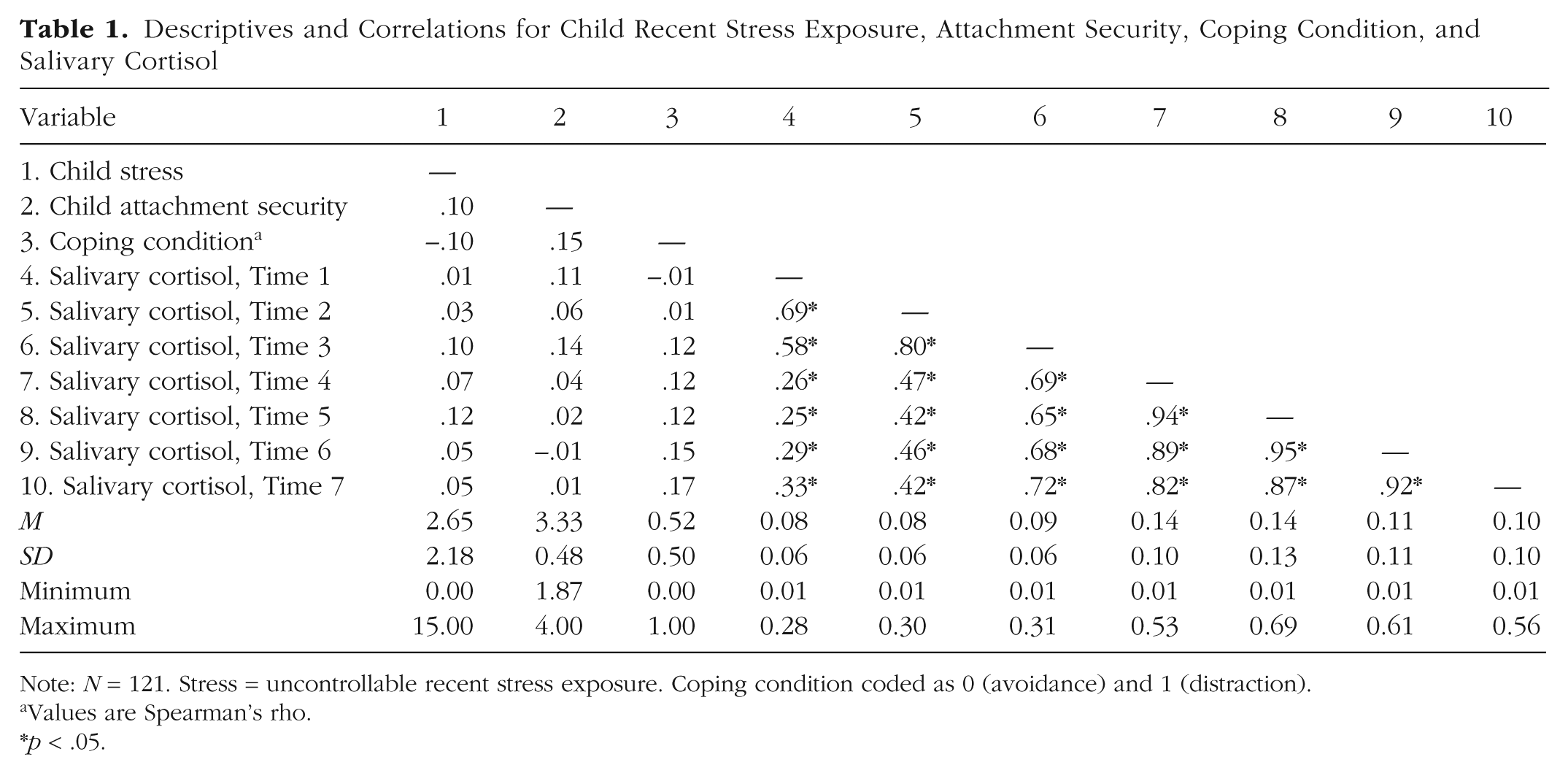
Note: N = 121. Stress = uncontrollable recent stress exposure. Coping condition coded as 0 (avoidance) and 1 (distraction).
Values are Spearman’s rho.
p < .05.
Variation in sC reactivity and recovery patterning
Before adding Level 2 predictors, likelihood ratio chi-square difference tests between random intercept, random intercept and linear reactivity slopes, random intercept and linear reactivity and recovery slopes, and random intercept and linear reactivity and linear and quadratic recovery slopes models were conducted to determine the significance of person-specific variation (i.e., random effects) in within-person sC response patterns. Results suggested that a random intercept, linear reactivity, linear recovery, and quadratic recovery slopes model best fit the data relative to a random intercepts only, χ2(9, N = 121) = 684.64, p < .001; random intercepts and linear reactivity slopes, χ2(7, N = 121) = 127.64, p < .001; and random intercept and linear reactivity and recovery slopes, χ2(4, N = 121) = 60.01, p < .001, model. The Level 1 model of within-person sC change yielded significant main effects for baseline (β = 0.51, SE = 0.01, p < .001), linear reactivity time (β = 0.03, SE = 0.01, p < .001), and quadratic recovery time (β = −0.01, SE = 0.01, p < .01). As described in the Method section, a fourth root transformation was applied to all sC data to meet modeling assumptions and, thus, Level 1 model parameter estimates and standard errors should be interpreted accordingly. To follow, these significant effects suggest that children entered the TSST with a predicted sC baseline of 0.51 µg/dl, and sC levels increased by an average of 0.03 µg/dl per 12.5 min during the reactivity phase. During the recovery phase, children’s sC levels initially declined by an average of 0.01 µg/dl cortisol, and this decline was gradually increased by an average of 0.02 µg/dl per 10 min. Significant and trend-level random variance in intercepts,
Hypothesis 1: reactivity
Covariates
Table 2 displays the reactivity phase parameter estimates of our final piecewise model. Significant Child Internalizing × Linear Reactivity Effects emerged, β = 0.01, p < .01. Children with greater, relative to fewer, symptoms displayed more dramatic positive linear increases in sC levels from T2 through T4. No other significant covariate effects emerged. 5
Parameter Estimates for Piecewise Growth Multilevel Models
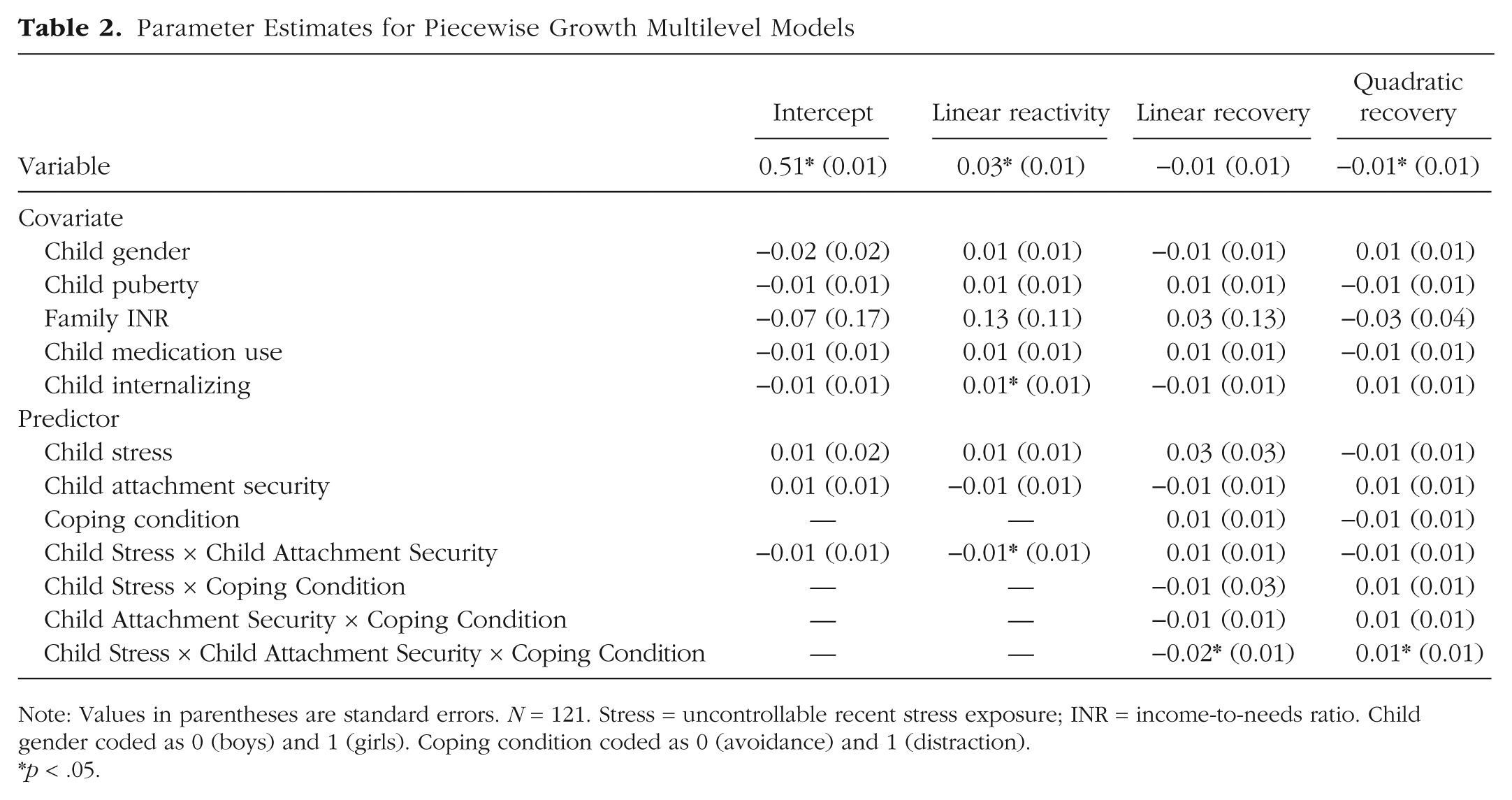
Note: Values in parentheses are standard errors. N = 121. Stress = uncontrollable recent stress exposure; INR = income-to-needs ratio. Child gender coded as 0 (boys) and 1 (girls). Coping condition coded as 0 (avoidance) and 1 (distraction).
p < .05.
Analyses
In the developmental literature, values ±2 SD from the sample average mean of a key study variable have been recommended as probing points in the evaluation of interaction effects (e.g., Roisman et al., 2012). However, in the current study, these values fell outside the range of the observed data for both perceived attachment security and recent stress exposure, making inferences about effects at these values problematic. Thus, in an attempt to examine high and low variable effects at values that fell within the range of the collected data, all significant cross-level interactions were probed at 10th and 90th percentile values (Hayes, 2013). 6 When perceived attachment security interacted with recent stress exposure and time to predict sC reactivity, we report and interpret results in the context of highest order significant interactions.
Perceived attachment security and recent stress exposure
A significant interaction between perceived attachment security, recent stress exposure, and linear time emerged, β = −0.01, p < .05 (Fig. 1), explaining 4% of the variance in sC reactivity linear growth. As expected (Hypothesis 1), children with high recent stress exposure levels who reported low perceived attachment security displayed more exaggerated sC reactivity, characterized by a more dramatic, positive linear pattern. In contrast, sC reactivity for stress-exposed children reporting high perceived attachment security was characterized by a less dramatic positive linear pattern.

Predicted salivary cortisol concentrations for high (red line, squares) and low (blue line, circles) child-uncontrollable recent stress exposure (stress) by child attachment security and coping condition during reactivity and recovery (shaded region). Predicted trajectories plotted at 10th and 90th percentile values of child-uncontrollable recent stress exposure and attachment security scores and reverse transformed for illustrative purposes.
Hypotheses 2 and 3: recovery
Covariates
Table 2 displays the recovery phase parameter estimates of our final piecewise growth model. No significant covariate effects on recovery patterning emerged. 5
Analyses
All significant cross-level interactions were probed at 10th (low) and 90th (high) percentile values. Results are interpreted in the context of higher order significant interactions.
Perceived attachment security, recent stress exposure, and coping condition
A significant interaction between perceived attachment security, recent stress exposure, coping condition, and quadratic time emerged, β = 0.01, p < .05 (Fig. 1), explaining 9% of the variance in sC recovery quadratic growth. As expected (Hypotheses 2 and 3), children with high recent stress exposure levels who reported low perceived attachment security demonstrated more quadratic, protracted sC recovery (i.e., sC levels continued to rise from T4 to T5 and decreased from T5 to T7) in the distraction condition and more linear, efficient sC recovery (i.e., constant decrease in T4–T7 sC levels) in the avoidance condition. The opposite was true for stress-exposed children reporting high perceived attachment security, with sC recovery trajectories more linear and efficient in the distraction condition and more quadratic and protracted in the avoidance condition.
Discussion
Using a novel experimental design, the current study examined the extent to which preadolescent perceived attachment security buffers against the effects of recent uncontrollable life event exposure on aspects of children’s HPA response functioning. Children’s views of caregivers as responsive and available in times of need indexed perceived attachment security, and parent-reported child-independent (not dependent on child behavior) life events in the past year comprised recent stress exposure. Children’s salivary cortisol activation patterns in response to a laboratory stressor (TSST) and one of two post-TSST coping conditions were also measured. As expected, recent stress exposure interacted with attachment security to predict cortisol reactivity. Results also demonstrate that children’s secure beliefs and coping work in concert to predict attachment-based regulatory fit patterns in cortisol recovery efficiency.
Our findings contribute to a growing literature that challenges traditionally held assumptions about “positive” (e.g., distraction) and “negative” (e.g., avoidance) coping by highlighting contexts in which each is effective in facilitating efficient cortisol recovery. In our own program of research, we have demonstrated that both distraction and avoidance similarly contribute to neuroendocrine recovery efficiency when aligned with factors intrinsic to the child, such as his or her characteristic ways of coping (Wadsworth et al., 2018), involuntary stress response propensities (Bendezú et al., 2016), and internalizing symptoms (Bendezú & Wadsworth, 2018). Shifting focus to factors more extrinsic to the child, we demonstrated similar regulatory fit dynamics for children with greater exposure to academic and interpersonal stressors (Bendezú & Wadsworth, 2017). The current study extends this work by illustrating the benefits of both distraction and avoidance when each is aligned with children’s recent history of uncontrollable life event exposure as well as their perception of available support in the caregiving environment. Thus, effective coping appears to depend less on the blanket or rigid application of universally “positive” or “negative” coping skills and more on optimizing regulatory fit between coping skills, characteristics of the child, and demands in their environments. Though effects were small and require replication, our findings tentatively bolster inference about the utility of person-centered intervention approaches to working with stress-exposed families, the potential of tailoring intervention content toward children’s coping strengths and weaknesses, and the possible value of fostering attachment security (e.g., involving parents) in this therapeutic work.
Evidence for recent stress-exposure effects on HPA reactivity
As expected, children’s secure beliefs interacted with recent stress exposure to predict cortisol reactivity patterns. Specifically, stress-exposed children’s perceptions of their caregiver as responsive and available in times of need was associated with less exaggerated cortisol reactivity. Although the HPA response is functional insofar as it mobilizes resources for managing stressors (Shirtcliff, Peres, Dismukes, Lee, & Phan, 2014), HPA hyperreactivity, especially in the absence of a buffer, is a risk factor for negative outcomes such as depression (Burke, Davis, Otte, & Mohr, 2005; Lopez-Duran et al., 2009). Consistent with this literature, results showed that children’s internalizing symptoms were associated with more exaggerated cortisol reactivity, lending support to the inference that this patterning indexed dysregulated HPA functioning. However, secure attachment views for stress-exposed preadolescents were associated with less exaggerated reactivity. Together, these findings potentially suggest that preadolescents’ HPA-related risk for internalizing may be buffered against by beliefs that predictable support from a caregiver is available should difficulties navigating their stress-laden environments arise. Future longitudinal research with sufficient time points (e.g., three) for testing mediation is needed to examine whether attachment security functions as a moderator of HPA-mediated stress-illness linkages.
Our reactivity findings also expand on recent work examining parental buffering effects on children’s HPA responses (Gunnar, 2017). Specifically, others have demonstrated that the physical presence of a caregiver while undergoing a stressful experience (e.g., TSST) reduces the magnitude of children’s cortisol reactivity (Gunnar & Hostinar, 2015). Here, we demonstrate that perceiving a caregiver as responsive and available when needed, particularly for children who arguably need this support the most (i.e., uncontrollable stress-exposed), was associated with less exaggerated cortisol reactivity. These findings may also lend additional insight to the observation that in-person parental buffering main effects on HPA functioning become nonsignificant as children age into adolescence (Doom, Hostinar, VanZomeren-Dohm, & Gunnar, 2015). First, stress-exposed youth are known to commence puberty earlier and age faster (Belsky & Shalev, 2016), aspects of child development that have been investigated as the “on/off” switch for in-person parental buffering effects (Doom et al., 2015). Second, as preadolescents shift away from reliance on caregivers for external regulation, a critical scaffold (or impediment) to this process is a shift from caregivers’ physical presence to children’s internalized representations about whether caregivers will be there to support them should difficulties navigating stressors on their own arise (Bowlby, 1988).
Although adolescents do not require the same degree of physical proximity as young children, their deep, entrenched trust in a parent’s responsive support even when not present remains essential to maintaining attachment security and promoting emotional and coping autonomy during this age (Allen & Miga, 2010; Bokhorst, Sumter, & Westenberg, 2010; Doyle, Lawford, & Markiewicz, 2009). This internalized assuredness of the provision of care in times of need has been argued to be a critical coping resource for stress-exposed children in particular (Chen & Miller, 2012). Thus, secure attachment views may prove a salient source of individual-level variation in parental buffering of stress-exposed preadolescent HPA reactivity.
That perceived attachment security buffered against exaggerated sC reactivity for stress-exposed preadolescents is also consistent with the recent conceptual distinction between toxic and tolerable stress (Evans, Kim, Ting, Tesher, & Shannis, 2007). Developmental theorists posit that the difference between physiologic stress responses that are tolerable versus toxic with respect to children’s physical and mental health is the presence of external support from a responsive adult caregiver (Shonkoff et al., 2009). Findings from the current study are constant with this theory insofar as stress-exposed children’s HPA responses to the TSST had the potential to be overexaggerated (i.e., more toxic), a pattern linked to internalizing symptoms in the current study and HPA risk for internalizing literature (Lopez-Duran et al., 2009). However, this HPA response pattern was less pronounced (i.e., more tolerable) for stress-exposed children endorsing secure attachment views. Thus, secure views may be a critical buffer against children’s diminished stress response system thresholds and the undue biological wear and tear that characterizes toxic stress.
Evidence of regulatory fit processes
As expected, children’s feelings of attachment security and their coping efforts worked in concert to predict hypothesized regulatory fit processes. Specifically, stress-exposed preadolescents with secure attachment beliefs appeared to be able to make effective use of the distraction condition as evidenced by the swift, efficient recovery of their cortisol levels. However, for stress-exposed preadolescents with insecure beliefs, the opposite was true. That is, these children appeared to have difficulty making effective use of distraction, as evidenced by their more protracted cortisol recovery trajectories. However, they also appeared to reap short-term benefits from avoidance as evidenced by their more efficient cortisol recovery relative to their peers in the distraction condition. Our findings suggest that the coping skills that benefit children exposed to difficult to manage stressors at the physiologic level depend on children’s views of their caregivers as available should they need support navigating those stressors.
Attachment theory and related dual-process motivation models (Cassidy & Shaver, 2008; Higgins, 1999) provide a useful framework for discussing regulatory fit findings. Stressful events (e.g., TSST) activate the attachment system (Mikulincer, Gillath, & Shaver, 2002), triggering mental representations of the self (i.e., internal working models; Vaughn et al., 2007) as worthy or unworthy of being cared for by an attachment figure (Bowlby, 1973; Main, Kaplan, & Cassidy, 1985). Viewing the self as worthy of care and feeling assured of its provision in times of need contributes to approach motivation (i.e., desire to explore, engage, and learn; Cassidy & Shaver, 2008) and promotion focus (i.e., concern with advancement and growth; Higgins, 1999). Given its approach-related nature (Connor-Smith et al., 2000), the distraction condition may have provided optimal regulatory fit (and efficient cortisol recovery) for stress-exposed children with secure attachment beliefs, providing opportunity to use their additional resources to explore the art supplies and engage in music. Alternatively, perceptions of oneself as unworthy of care and in doubt of its provision in times of need contributes to avoidance motivation (i.e., desire to seek safety; Cassidy & Shaver, 2008) and prevention focus (i.e., concern with protection; Higgins, 1999).
Thus, the avoidance condition may have provided optimal regulatory fit (and efficient cortisol recovery) for stress-exposed children with insecure attachment beliefs, giving them the opportunity to temporarily serve their goal to seek safety from the TSST and their reactions to it. The previous is consonant with literature on the value of regulatory fit across decision making, behavior change, and task performance domains (Higgins, 2005). Future research incorporating more direct measures of approach-avoidance motivation (e.g., Rudolph, Troop-Gordon, Modi, & Granger, 2018) are needed to test these propositions at the physiologic level of analysis.
Our attachment-based regulatory fit findings may also speak to resiliency frameworks that implicate attachment security as a protective psychobiological factor involved in youth stress-illness links (Luthar, Crossman, & Small, 2015). Specifically, the shift-and-persist model posits that secure attachment relationships are the vehicle by which children become able to shift (i.e., adapt via stress appraisals and flexible use of various coping strategies) and persist (i.e., finding meaning and maintaining optimism) in the face of uncontrollable stressors (Chen & Miller, 2012). When situated within this framework, it is possible that secure attachment beliefs for stress-exposed children may have promoted an approach to the TSST guided by a sense of mastery and optimism, perhaps supporting less excessive HPA reactivity. Secure attachment beliefs may have also helped stress-exposed children more flexibly shift between problem solving required by the TSST to resource seeking during the distraction condition, perhaps supporting more efficient cortisol recovery. Future research incorporating coping manipulations may help shed light on how shift-and-persist processes unfold for stress-exposed adolescents.
Implications, limitations, and future directions
Our findings provide further empirical support for the claim that children’s maladaptive coping can be viewed as functional adaptation to circumstances replete with unpredictable, uncontrollable stressors (Blair & Raver, 2012; Del Giudice et al., 2011; Wadsworth, 2015). Specifically, avoidance appears to help some children modulate their physiologic reactivity to stressors, a regulatory process that has the potential to temporarily buffer against undue wear and tear on those biological systems known to confer risk for psychopathology (Davidson & McEwen, 2012). We demonstrate these beneficial effects specifically for children facing unpredictable and uncontrollable stressors who also perceive that they lack dependable external support from an approachable caregiver. For these children, “maladaptive” coping appears to serve a function when examined at the physiologic level of analysis. Thus, coping interventions for stress-exposed youth may benefit from additional research that both challenges traditional notions about universally “good” and “bad” coping strategies and considers the possibility that coping skills work differently depending on person-context match (i.e., regulatory fit). Coping interventions informed by this research may approach stress-exposed children with acceptance and validation of their stressful life experiences and attempts to navigate them in the perceived absence of available and responsive caregiving. This work communicates understanding about maladaptive coping as a form of functional adaptation.
Study findings may also point to the potential value of targeting attachment security into this coping intervention work. That is, attachment security appears to help stress-exposed children modulate their physiologic reactivity to stressors while also contributing to which forms of coping support physiologic recovery efficiency. Coping interventions that cultivate attachment security in the parent-child relationship for stress-exposed youth may help children appraise stressors differently (e.g., more positive, optimistic; Chen & Miller, 2012), give children access to more adaptive coping repertoires involving exploration (e.g., distraction, play), and in turn, buffer against the possible toxic effects of recent uncontrollable life event exposure. Although child-only coping interventions may provide clinic-based opportunities to practice active engagement coping, they may fail to encourage its use outside the clinic or reduce reliance on disengagement coping if the latter remains functionally adaptive in the contexts children return to (e.g., unavailable, unresponsive caregiving). Indeed, stress-exposed children with secure beliefs evinced efficient cortisol recovery in the distraction condition but also protracted recovery in the avoidance condition, perhaps suggestive that avoidance did not serve an adaptive function for these children. Attachment security may be a critical family-level component of maximally effective coping intervention work seeking to remediate HPA dysregulation, a proposal consonant with recent intervention work seeking to improve cortisol rhythms for stress-exposed children by promoting supportive parenting (e.g., Bernard, Hostinar, & Dozier, 2015).
One unexpected finding related to our reactivity analyses deserves mention. Securely attached children exposed to fewer uncontrollable life events displayed more pronounced cortisol reactivity patterning relative to their securely attached counterparts exposed to greater uncontrollable life events. The cortisol response is thought to be adaptive in the face of an acute stressor (Shirtcliff et al., 2014), and thus the reactivity patterning of securely attached children exposed to fewer uncontrollable life events may be considered an appropriate response to an uncontrollable laboratory-based challenge (i.e., TSST). However, it is also possible that securely attached children exposed to fewer uncontrollable life events may have responded with more dramatic increases in cortisol because of their relative inexperience facing and/or coping with uncontrollable stressors. In a similar vein, because the attachment system is activated by exposure to stressors (Skinner & Zimmer-Gembeck, 2016), stress-exposed children with secure attachment views may have had more frequent reminders in the past year that they would be and are worthy of responsive care when attempting to navigate and manage uncontrollable life events. In other words, it is possible that assuredness of care may have been more readily accessible for stress-exposed children with secure attachment views and provided an additional buffer as a result.
There are limitations to the current study that point to directions for future research. First, the results are limited to a sample of predominantly White, nonurban families. Although there was variability in the current sample with respect to the frequency of recent uncontrollable life events as well as household annual income, complementary research focusing on more ethnically diverse samples exposed to greater environmental risk factors (e.g., low socioeconomic status) is needed. Such research incorporating experimental psychosocial manipulations of both child-level coping and environmental coping resource provision (e.g., Chen, 2007) would be well poised to examine regulatory fit processes as they pertain to toxic versus tolerable stress (Shonkoff et al., 2009) and shift-and-persist (Chen & Miller, 2012) models. Second, although families were contacted the evening before their appointment and verbally agreed to adhere to preexperiment food and beverage intake restrictions, follow-up questions (i.e., readherence) the day of the experiment were not administered. In addition, although our food and beverage restrictions purposefully covered items containing caffeine that a group of children this age might consume (e.g., milk chocolate, candy, carbonated beverages with or without sugar, energy drinks, coffee), we did not ask participants to avoid caffeine consumption specifically. Thus, there is a small possibility that nonadherence or other caffeine consumption (e.g., unsweetened tea, caffeine pills) may have contributed to our findings. Third, although a number of important covariates were included, we did not control for or exclude participants on the basis of other variables with demonstrated associations to cortisol activation (e.g., BMI, obesity; Francis, Granger, & Susman, 2013). Fourth, our assessment of recent stress exposure was limited to the year before the study, thus limiting interpretations regarding the chronicity of uncontrollable life event exposure. Examination of both early and recent life stressors (e.g., Rao, Hammen, Ortiz, Chen, & Poland, 2008) may better inform for whom maladaptive coping (e.g., avoidance) serves as functional adaptation to chronic uncontrollable stress (Wadsworth, 2015).
Fifth, although attachment security is associated with the way children perceive stressors (Seiffge-Krenke, 2011), the current study did not assess children’s primary and secondary stress appraisals or the extent to which life events were perceived as uncontrollable, limiting inference about whether HPA reactivity effects were due to children’s perceptions of stressors (e.g., life events, TSST) as threatening or exceeding their capacity to cope. Sixth, and to this end, children’s self-reported stress ratings over the course of the experimental procedure were not examined in the current study. As physiologic reactivity and subjective reports are often discrepant (Campbell & Ehlert, 2012), particularly in clinical samples (Zonnevylle-Bender et al., 2005), future research examining their concordance and links to attachment security and uncontrollable stress exposure may further delineate those children at greatest risk for development of psychopathology. Seventh, it is possible that caregivers’ socialization of coping as well as the ways children typically cope with stressful life events may have contributed to our physiologic findings (e.g., Abaied, Wagner, & Sanders, 2014; Hastings, Kilmes-Dougan, Kendziora, Brand, & Zahn-Waxler, 2014). Secure beliefs may support views of caregivers as more available to youth in times of need, but little research has demonstrated the physiologic benefits afforded to children by what available caregivers socialize them to do once approached by their children. Future research examining attachment security, caregiver coping socialization, and subsequent child coping associations are needed to more fully understand how supportive caregiving from an attachment figure may facilitate adaptive coping and buffer against the potentially noxious effects of uncontrollable life event exposure (Shonkoff et al., 2009).
Finally, there are limitations associated with our assessment of attachment security. Given that attachment security was assessed via self-report, it is possible that certain aspects of internalizing symptoms may have biased responses to attachment items, raising questions about whether internalizing symptoms could have functioned as a proxy for attachment insecurity. In addition, our assessment of attachment security was limited to maternal caregivers. Future research examining positive attachment relationships with fathers or adults outside the primary caregiving role (e.g., teachers, role models; Howes & Ritchie, 1999) is imperative for understanding attachment-based regulatory fit processes for families overtaxed by chronic uncontrollable stress. These limitations notwithstanding, the current study provides novel empirical evidence of perceived attachment security as a coping resource and putative buffer against HPA dysregulation for stress-exposed preadolescents and points to children’s coping and secure attachment beliefs as prospective targets of coping-based intervention work.
Footnotes
Action Editor
Erin B. Tone served as action editor for this article.
Author Contributions
J. J. Bendezú and M. E. Wadsworth conceived and designed the study. J. J. Bendezú, J. Loughlin-Presnal, and M. E. Wadsworth participated in data collection. J. J. Bendezú and M. E. Wadsworth analyzed the data, and all of the authors interpreted the data. All of the authors drafted the article, revised it, and approved the final version for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.