
Abstract
Numerous cross-sectional studies have found a positive association between level of event centrality and symptoms of posttraumatic stress disorder (PTSD), but the temporal course of this relationship is unclear. We aimed to investigate the concurrent and longitudinal association between event centrality and symptoms of PTSD in a trauma-exposed sample. In total, 319 survivors of the 2011 massacre on Utøya island, Norway, were interviewed 14 to 15 and 30 to 32 months after the event. A cross-lagged panel model was used to explore the association between event centrality and PTSD symptoms over time. Level of event centrality was significantly associated with concurrent PTSD symptoms at both time points. PTSD symptoms were significantly associated with prospective levels of event centrality but not vice versa. This finding indicates that the degree to which survivors perceive a terrorist attack as central to their identity may be an effect, not a cause, of their PTSD symptoms.
In the literature on psychological adjustment after trauma, there has been a growing interest in examining the impact of construing the traumatic event as a central component of one’s identity and life story. According to Berntsen and Rubin (2006, 2007), when a traumatic event becomes a central part of a survivor’s identity and life story, the accessibility and vividness of the distressing trauma memories increases, which again enhance symptoms of posttraumatic stress disorder (PTSD). To the extent that event centrality is important in the development and maintenance of PTSD, as proposed by Berntsen and Rubin (2006, 2007), it may be an important target for prevention and treatment, but more longitudinal research is warranted.
To standardize the measurement of the relationship between trauma centrality and PTSD, Berntsen and Rubin (2006) developed the Centrality of Event Scale (CES). This scale assesses the extent to which the trauma memory has become a turning point in a survivor’s life story, a central component of his or her identity, and a reference point for the person’s everyday inferences (Berntsen & Rubin, 2006).
In line with Berntsen and Rubin’s (2006, 2007) postulation, numerous cross-sectional studies have found a positive association between levels of event centrality and PTSD symptoms among undergraduate students self-reporting a stressful or potentially traumatic life event (e.g., Bernard, Whittles, Kertz, Burke, & Kendall-Tackett, 2015; Boals & Schuettler, 2011; Lancaster, Rodriguez, & Weston, 2011; Webb & Jobson, 2011) and in trauma-exposed samples, including war veterans (Brown, Antonius, Kramer, Root, & Hirst, 2010), adult survivors of a terrorist attack (Blix, Solberg, & Heir, 2013), and treatment-seeking adult victims of diverse potentially traumatic events (da Silva et al., 2016). This positive relationship between event centrality and PTSD symptoms persists even after controlling for other known correlates, such as anxiety, dissociation, depression, cognitive processing of trauma, and coping style (e.g., Berntsen & Rubin, 2007; Boals & Schuettler, 2011; Brown et al., 2010; Robinaugh & McNally, 2011), which might suggest that centrality is a unique predictor of PTSD. However, the cross-sectional design of these studies does not allow for causal inferences, and as noted by Boals (2014), longitudinal studies are called for to further our understanding of whether event centrality actually is a predictor of posttraumatic stress reactions or just a cross-sectional correlate.
To our knowledge, only a handful of studies have examined the relationship between event centrality and psychopathology longitudinally, of which three included PTSD symptoms (i.e., Blix, Birkeland, Solberg, Hansen, & Heir, 2016; Boals & Ruggero, 2015; Boelen, 2012). In the first of these three studies, Boelen (2012) explored the prospective linkage between event centrality and postloss psychopathology among people bereaved within the past year. He found that event centrality was positively associated with PTSD, depression, and prolonged grief 1 year later after controlling for baseline symptom levels. However, note that Boelen did not explore the other possible causal direction of this association (i.e., whether baseline PTSD predicted follow-up event centrality when controlling for baseline event centrality). In the second study, Boals and Ruggero (2015) examined the direction of the relationship between event centrality and PTSD symptoms among undergraduate students self-reporting the most stressful event they had experienced and found that event centrality predicted PTSD symptoms 1 month later (controlling for PTSD Time 1) but not vice versa.
Finally, in a study on ministerial employees exposed to the Oslo bombing in 2011, Blix et al. (2016) examined the relationship between event centrality and PTSD symptoms at three different postterror time points (10 months, 2 years, and 3 years). They found a prospective association between event centrality and PTSD symptoms in that higher levels of event centrality at Time 1 were associated with higher levels of PTSD symptoms at all three waves. They also found that higher levels of event centrality at Time 1 and Time 2 were related to concurrent higher levels of PTSD symptoms in survivors beyond what could be anticipated on the basis of their individual general trajectories. According to the authors, these findings suggest that perceiving a traumatic event as central to identity may both maintain PTSD symptoms over time and slow down an otherwise declining trajectory of PTSD symptoms. Blix et al. did not explore whether participants’ level of PTSD symptoms predicted later levels of event centrality.
In sum, existing findings suggest that perceiving a stressful event as central to one’s identity and life story is positively associated with concurrent and prospective PTSD symptom severity. However, as noted, an important limitation of the existing research is that most of the studies are cross-sectional. Thus, although the predominant hypothesis is that high levels of event centrality increase PTSD symptom severity, the relationship may also go in the opposite direction, as stressed by a number of researchers (e.g., Boals & Ruggero, 2015; Gehrt, Berntsen, Hoyle, & Rubin, 2018; Groleau, Calhoun, Cann, & Tedeschi, 2013). In other words, it is plausible that high levels of PTSD symptoms cause individuals to perceive the event as a central component of their identities and life stories. In addition, as noted by Boals and Ruggero (2015), because the only longitudinal study exploring the direction of the relationship between these two constructs is based on undergraduate students, to further our understanding of the role of event centrality in the development and/or maintenance of PTSD symptoms, more longitudinal studies with trauma-exposed samples are needed. Finally, to the best of our knowledge, a proposed time frame for the relationship between event centrality and PTSD symptoms has not been explicitly stated in the theoretical model or existing empirical literature. Nevertheless, in our opinion, we can hypothesize that “the extent to which a memory for a stressful event forms a reference point for personal identity and for the attribution of meaning to other experiences in a person’s life” (Berntsen & Rubin, 2006, p. 220) may have a prospective effect on trauma survivors’ level of psychopathology. And given that Boals and Ruggero (2015) did find a 1-month lag association between CES and PTSD symptoms, studies investigating whether similar results would appear for a longer time span are needed.
The Present Study: Context and Aims
The terrorist attack at Utøya island
On July 22, 2011, one man, dressed as a police officer, went to Utøya island, Norway, where a Norwegian Labor Youth summer camp with 564 participants was being hosted. Once on the island, he began shooting those he came across. The shooting lasted for approximately 90 min. The terrorist left 68 people dead on the island or in the water, and 1 individual died later at the hospital; most of these victims were youths or young adults. The survivors experienced high levels of trauma exposure during the massacre, including life threat, the intense and persistent sound of gun shots, witnessing people being injured or killed, hearing people scream in pain and fear, and the loss of someone close (Dyb et al., 2014). After the attack, the survivors were exposed to massive media attention; almost all of them were approached by reporters, and most of them participated in interviews about their terror experience (Thoresen, Jensen, & Dyb, 2014). Four to 5 months after the attack, the level of PTSD symptoms was more than six times higher among the survivors in the Utøya study than among the general population in Norway, and 47% reported clinical levels of PTSD (Dyb et al., 2014). These aspects of the traumatic event and its aftermath provide an important foundation for exploring the degree to which the survivors experience the terrorist attack as self-defining and how reports of event centrality relate to symptoms of PTSD during the first 2.5 years after the attack.
Trauma survivors’ level of PTSD and/or event centrality has been found to be related to age, sex, ethnicity, and level of traumatic exposure (Boals, Hayslip, Knowles, & Banks, 2012; May & Wisco, 2016; Olff, Langeland, Draijer, & Gersons, 2007; Perilla, Norris, & Lavizzo, 2002). Thus, these factors were included as covariates in the present study. In addition, we wanted to include factors that might have changed in the survivors’ lives between the first and the second measurement and thus possibly affect the longitudinal relationship between level of event centrality and PTSD. Hence, survivors’ exposure to new traumatic experiences in this time frame was included as a covariate. In terms of the participants’ prior trauma exposure, because the survivors at Utøya island did not differ significantly on prior trauma exposure compared with matched control subjects in the Norwegian population (i.e., Stene & Dyb, 2018), this factor was not included as a covariate.
Aims of the present work
We aimed to extend extant research by investigating the level of event centrality at two different postterror time points and examining the concurrent and longitudinal association between event centrality and PTSD symptoms among young survivors of a terrorist attack. More specifically, we wanted to explore the cross-lagged relationship between these two constructs. We had three hypotheses. First, given the nature and developmental timing of the attack, we expected the survivors to report high levels of event centrality. Second, on the basis of Berntsen and Rubin’s (2006, 2007) model and previous research, we expected to find a significant positive association between event centrality and PTSD symptoms at both time points. Finally, on the basis of Boals and Ruggero’s (2015) findings, we expected that survivors’ levels of event centrality would prospectively predict their PTSD symptoms.
Method
The present study is part of a comprehensive longitudinal face-to-face interview study designed to examine the level of posttraumatic stress reactions and potential predictors of PTSD among survivors of the terrorist attack at Utøya island in 2011 (Dyb et al., 2014).
Participants
In total, 490 individuals (≥ 13 years old at the time of the attack) survived the massacre at Utøya island. After receiving the invitation letter for the first wave of interviews in the longitudinal study (Time 1 [T1], 4–5 months after the event), 3 of the survivors contacted the project group and said that they did not want to participate. The remaining 487 survivors were invited to participate in the second wave (T2, 14–15 months). In the third wave (T3, 30–32 months), only survivors who had participated at T1 and/or T2 were invited. Altogether, 319 (65.5%) survivors participated: 227 (71.2%) at both time points (i.e., T2 and T3), 58 (18.2%) at T2 only, and 34 (10.7%) at T3 only. Their mean age at the time of the terrorist attack was 19.4 years (SD = 4.6; range, 13.3–56.8 years; 93.1% < 26), and 47.0% were female. The vast majority (87.5%) were of Norwegian origin (i.e., both parents were born in Norway). To measure socioeconomic status, participants were asked to rate how they perceived their financial well-being compared with others on a scale from 1 to 5 (much poorer, somewhat poorer, similar, somewhat better, much better); 21.0% reported that they perceived themselves as financially disadvantaged (i.e., much or somewhat poorer than others). When asked about exposure to new traumatic experiences between T2 and T3, 21.0% reported at T3 that they had experienced one new traumatic event within the past year, 11.6% reported two such experiences, and 5% had experienced three or more new incidents (M = 0.62, SD = 0.98). There were no significant differences between participants and nonparticipants with respect to age or sex. A more comprehensive description of the participants has been reported elsewhere (Dyb et al., 2014; Stene & Dyb, 2016).
Procedures
All eligible participants were posted an invitation letter with information about the purpose of the study. They were subsequently telephoned and asked if they were willing to participate. Participants took part in individual interviews with experienced health care personnel (mostly psychologists, medical doctors, and nurses). The interview was conducted face-to-face, and a self-report section was completed by the respondents while the interviewer was beside them and available for questions. Most of these interviews were conducted in survivors’ homes, although some took place in an office in their hometowns or a public place chosen by the participant. Participation was based on informed consent for adolescents ages 16 or older. Parents consented to participation for younger children in accordance with Norwegian law. All interviewers attended a 1-day training course, which included an in-depth explanation of the interview questions and the rationale behind each topic and practical exercises (the interviewers practiced using this specific manual by taking turns interviewing each other). Interviews lasted approximately an hour and a half. If interviewers identified unmet needs among the participants (e.g., for intervention or support), they were instructed to arrange for assistance. The study was approved by the Regional Committee for Medical and Health Research Ethics in Norway.
Measures
Event centrality
A short version of the Centrality of Event Scale (Berntsen & Rubin, 2006) was included in the self-report section of the interview manual and used to measure the degree to which the terror attack at Utøya island had been integrated into the survivors’ life stories and identities. The short version is a seven-item questionnaire tapping three different ways in which the memory of a traumatic event may become highly interconnected in an individual’s autobiographical memory: reference point (e.g., “This event has become a reference point for the way I understand myself and the world”), identity (e.g., “I feel that this event has become part of my identity”), and turning point (e.g., “This event permanently changed my life”). Responses are endorsed on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The CES was calculated as a mean score; high scores indicate high levels of centrality. Both the original version and the Norwegian version of the seven-item CES have been reported to be reliable (α = .88–92; Berntsen & Rubin, 2006; Blix et al., 2013). Participants completed the seven-item version of the CES at both time points, and the scale proved to have good reliability (T2 α = .86, T3 α = .89). To the best of our knowledge, there are no published recommendations for interpreting the level of CES, but in the existing literature, the reported mean varies from 2.25 (Lancaster et al., 2011) to 4.07 (da Silva et al., 2016).
Posttraumatic stress symptoms
The participants were interviewed about their posttraumatic stress reactions at both time points using the University of California at Los Angeles PTSD Reaction Index (UCLA PTSD-RI) for the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–IV; American Psychiatric Association, 1994; Pynoos, Rodriguez, Steinberg, Stuber, & Frederick, 1998; Steinberg, Brymer, Decker, & Pynoos, 2004). The PTSD-RI is a 20-item scale assessing posttraumatic stress reactions in the past month. Responses are recorded on a 5-point Likert scale ranging from 0 (never) to 4 (most of the time). However, because three items have two alternative formulations, of which the highest score was applied to calculate the total score, the total symptom scale score is made up of 17 items, corresponding with the DSM–IV criteria for PTSD (American Psychiatric Association, 1994), and the possible scores range from 0 to 68. Seven items tap avoidance, five items tap reexperiencing, and five items tap increased arousal. The Norwegian version of the UCLA PTSD-RI previously showed good psychometric properties (α = .82–87; Jensen, Dyb, & Nygaard, 2009). The UCLA PTSD-RI was designed as a self-report instrument, not a clinical assessment tool, and it can be administered as a paper-and-pencil measure. However, in this study, we chose to let the interviewers read the questions aloud and fill out the participants’ response to increase the likelihood both that the questions were understood correctly and that the frequency rating sheet was used as intended for each question. The PTSD-RI was calculated as a mean score (possible score range, 0–4), and the scale proved to have good reliability (T2, α = .90; T3, α = .92).
Traumatic exposure
A 14-item checklist was developed to assess the participants’ potential traumatic exposures during the terrorist attack; it included items such as “heard gun shots” and “saw dead bodies” (“yes” or “no” answers; for more information, see Dyb et al., 2014). Traumatic exposure was thus operationalized as the count of the number of “yes” answers.
New traumatic experiences
A 10-item checklist was developed that was based on the Life Event Interview (Costello, Erkanli, Fairbank, & Angold, 2002) to assess whether the survivors had been exposed to any new traumatic experiences between T2 and T3, such as exposure to violence, a serious accident, or the sudden (unexpected) loss of someone close. At T3, the participants were asked to tick off which, if any, of these experiences they had had within the past year. The new traumatic experiences scale was operationalized as the count of the number of “yes” answers.
Data analyses
To analyze the relationship between event centrality and PTSD symptoms, we fitted a latent variable cross-lagged panel model, implemented as a structural equation model (SEM) in the software package Mplus (Muthén & Muthén, 2017). A central feature of the cross-lagged model is that the initial levels of the dependent variables are controlled for, which allows us to predict changes in the dependent constructs over and above previous levels (Selig & Little, 2012). CES and PTSD-RI items were treated as ordinal, and model parameters were estimated using the robust weighted least squares estimator (WLSMV).
Before conducting the SEM analyses, we fitted a series of confirmatory factor models to examine the relationships between the factor indicators and the corresponding latent factors (i.e., CES and PTSD-RI) at T2 and T3, including factor loadings and correlations. The SEM analyses were then conducted in two steps. First, to assess whether the same items measured event centrality and PTSD symptoms at both time points, we assessed measurement invariance for the latent variables by conducting a configural invariance test. Subsequently, we used a metric invariance test in which all factor loadings were constrained to be equal to corresponding indicators at both time points. As recommended by Little, Preacher, Selig, and Card (2007), the residuals for the corresponding indicators were allowed to correlate over time. Finally, we examined the concurrent and lagged relationships between CES and PTSD-RI, controlling for sex, age, ethnicity, trauma exposure, and new traumatic experiences, using a cross-lagged panel model (CLPM).
The fit of each model was assessed using the overall χ2 value, the comparative fit index (CFI), Tucker-Lewis index (TLI), and the root mean square error of approximation (RMSEA). In line with Little (2013), RMSEA values in the range from less than 0.05 to 0.08 and CFI and TLI values greater than.90 were considered indicative of acceptable model fit.
Descriptive analyses were performed using IBM SPSS (Version 20.0). For all modeling analyses, we used Mplus (Version 8; Muthén & Muthén, 2017).
Attrition analyses
Of the 319 survivors who participated in the study, 227 participated at both time points, of which 201 (88.5%) provided complete data on all items across the two time points. Most missing data were due to wave nonresponse. Paired-sample t tests indicated no significant differences in sex, age, mean PTSD-RI, or mean CES among survivors who participated at both time points compared with only T2 (p > .05). Missing data on the study variables were minimal at both time points, ranging from 0% to 1.4% and 0% to 2.3% for PTSD-RI at T2 and T3, respectively, and 1.4% to 2.1% and 0% to 1.1% for CES at T2 and T3, respectively. Because of missing data on the covariates, the final sample used in the Mplus analyses consisted of 310 survivors. To handle missing data, we used the default routines for the WLSMV in Mplus, which are based on pairwise present analysis (Muthén & Muthén, 2017).
Results
Descriptive analyses
The participants had high levels of traumatic exposure during the massacre (M = 9.6, SD = 2.2). The total CES mean score and the mean of each item were well above the middle point of the scale at T2 (M = 3.65, range, 3.29–4.00) and T3 (M = 3.65, range, 3.32–3.99). Whereas the CES mean score remained stable over time, the PTSD-RI mean score decreased somewhat from T2 to T3 (Table 1). An independent-samples t test showed that the decrease in the PTSD-RI was significant, t(226) = 2.80, p < .01. Pearson correlations were performed between the PTSD-RI and CES at both time points and over time. Table 1 shows that all correlations were statistically significant.
Correlations Between Symptoms of Posttraumatic Stress Symptoms and Event Centrality Over Time
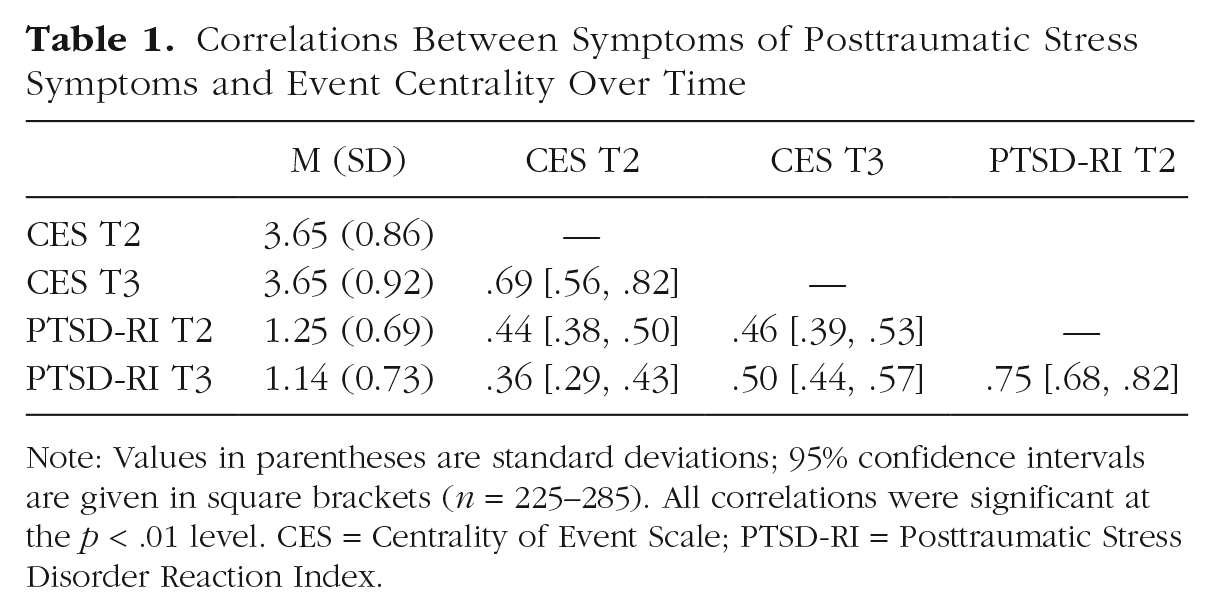
Note: Values in parentheses are standard deviations; 95% confidence intervals are given in square brackets (n = 225–285). All correlations were significant at the p < .01 level. CES = Centrality of Event Scale; PTSD-RI = Posttraumatic Stress Disorder Reaction Index.
Preliminary analyses
The seven CES items were specified to load onto one CES factor, resulting in a poor model fit at T2, χ2(14, n = 281) = 49.914, p < .001, CFI = .979, TLI = .969, RMSEA = 0.096 (90% CI = [.068, .125]), and T3, χ2(14, n = 261) = 49.572, p < .001, CFI = .983, TLI = .974, RMSEA = 0.099 (90% CI = [0.070, 0.129]). To account for shared variance between the residuals of Items 1 and 3, Items 5 and 6, and Items 3 and 4, these items were allowed to correlate at both time points. This allowance resulted in an acceptable model fit at T2, χ2(11, n = 281) = 28.847, p = .00, CFI = .990, TLI = .980, RMSEA = 0.076 (90% CI = [0.043, 0.110]), and T3, χ2(11, n = 261) = 26.042, p < .01, CFI = .993, TLI = .986, RMSEA = 0.072 (90% CI = [0.036, 0.109]).
In line with a recent systematic literature review of the latent structure of PTSD in DSM (Armour, Muűllerová, & Elhai, 2016), in which the higher-order Dysphoric Arousal model (Elhai et al., 2011) was found to demonstrate best fit, the PTSD-RI items were specified to load onto five subfactors (reexperiencing, avoidance, dysphoric arousal, anxious arousal, and numbing). This resulted in an acceptable model fit at T2, χ2(114, n = 285) = 266.159, p < .01, CFI = .956, TLI = .948, RMSEA = 0.068 (90% CI = [0.058, 0.079]), and T3, χ2(114, n = 261) = 241.251, p < .01, CFI = .970, TLI = .964, RMSEA = 0.065 (90% CI = [0.054, 0.077]).
As for the covariates (i.e., sex, age, ethnicity, trauma exposure, and new traumatic experiences), most were nonsignificant, but new traumatic experiences were significantly associated with both CES and PTSD-RI at T2 (p < .05), and sex, ethnicity, and trauma exposure were significantly associated with PTSD-RI at T2 (p < .05). For the standardized estimates and residual variance for the covariates at T2 and T3, see Table S1 in the Supplemental Material available online.
To test for measurement invariance, we compared the relative fit of the unconstrained (configural) model with the constrained (metric) model using the DIFFTEST function in Mplus (Muthén & Muthén, 2017). The model fit did not change significantly when all factor loadings were constrained to be equal to corresponding indicators at both time points, which provides evidence for weak invariance across time (see Table 2). In other words, the same manifest variables appeared to measure the same latent factors in the same way at T2 and T3.
Tests of Measurement Invariance of CES and PTSD-RI Over Time
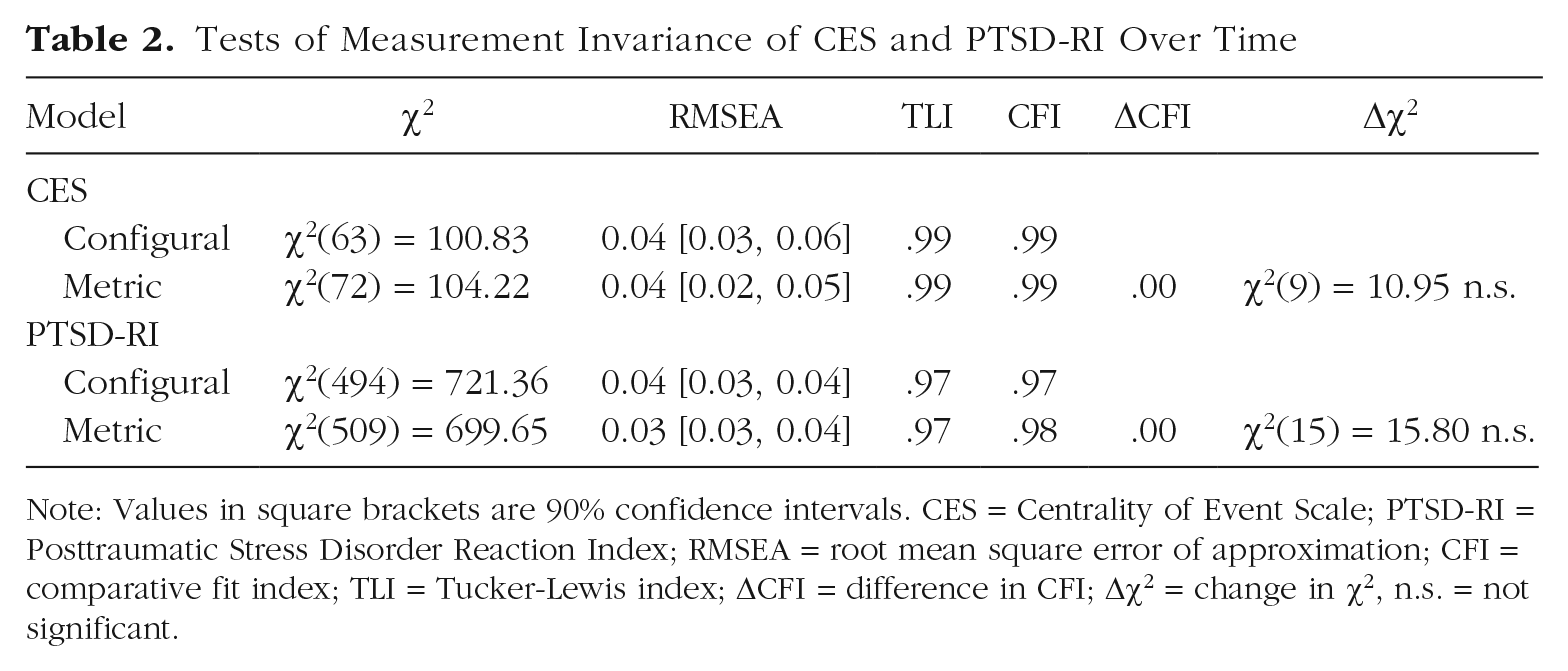
Note: Values in square brackets are 90% confidence intervals. CES = Centrality of Event Scale; PTSD-RI = Posttraumatic Stress Disorder Reaction Index; RMSEA = root mean square error of approximation; CFI = comparative fit index; TLI = Tucker-Lewis index; ΔCFI = difference in CFI; Δχ2 = change in χ2, n.s. = not significant.
Cross-lagged panel model
We tested the relationship between the two latent factors (i.e., CES and PTSD-RI) at T2 and T3 with a CLPM, controlling for sex, age, ethnicity, trauma exposure, and new traumatic experiences between T2 and T3. This test resulted in a model with good fit, χ2(1267, n = 310) = 1,540.990, p < .001, CFI = .968, TLI = .966, RMSEA = 0.026, (90% CI = [0.021, 0.031]). Standardized parameter estimates from the CLPM are reported in Figure 1. The factor loadings and residual correlations for the latent variables are presented more completely in Tables S2 and S3 in the Supplemental Material.

The relationship between event centrality (Centrality of Event Scale) and posttraumatic stress symptoms (University of California at Los Angeles PTSD Reaction Index) at T2 and T3, with standardized estimates (N = 319). Asterisks represent significant paths (*p < .01). Intr. = intrusion/reexperiencing; Numb. = numbing; Dysp. = dysphoric arousal; Anx. = anxious arousal; Avoi. = avoidance. For the sake of simplicity, correlations between residuals and the residual variances of each indicator are not included in the figure.
Figure 1 shows that the PTSD-RI T2 predicted PTSD-RI T3 (β = 0.790, SE = 0.061, p < .001), and CES T2 predicted CES T3 (β = 0.624, SE = 0.049, p < .001). In addition, CES and PTSD-RI were significantly correlated at T2 (β = 0.497, SE = 0.052, p < .001), as were the residuals at T3 (β = 0.429, SE = 0.088, p < .001). Finally, PTSD-RI at T2 predicted CES T3 (when controlled for CES T2; β = 0.267, SE = 0.064, p < .001), but CES T2 was not predictive of PTSD-RI T3 (when controlled for PTSD-RI T2; β = 0.018, SE = 0.069). Very similar estimates were found using manifest variables (see Fig. S1 in the Supplemental Material).
Discussion
The current study is the first to examine the bidirectional relationship between event centrality and PTSD symptoms over time in a trauma-exposed sample. As hypothesized, we found that survivors reported a high level of event centrality and that event centrality was significantly associated with concurrent PTSD symptoms at both time points. However, contrary to our expectation, when we explored the cross-lagged relationship between the two constructs, we found that PTSD symptoms prospectively predicted level of event centrality but not vice versa.
To our knowledge, the survivors in our study reported the second highest CES mean score in a trauma-exposed sample to date—exceeded only by the treatment-seeking adults with PTSD in da Silva et al.’s (2016) study. We believe that there are at least four ways to understand the high and stable event centrality reported by our sample. First, high and stable event centrality may be related to the particularly severe and brutal nature of the attack and the profound effects it had on the survivors’ daily lives and functioning after the event, including the loss of someone close, high levels of posttraumatic symptoms, and decreased functioning, such as deteriorated performance in school (Dyb et al., 2014; Strøm, Schultz, Wentzel-Larsen, & Dyb, 2016). Second, the terrorist attack at Utøya island was a national tragedy (Thoresen et al., 2012). Having been directly involved in an event that has become a part not only their own personal life stories but of their country’s history may help explain the high and stable level of event centrality among those who survived.
Third, the attack was a public event that received extensive media attention. In our previous work, we found that almost all the survivors had been approached by reporters and that most (88%) had participated in interviews about their terror experience (Thoresen et al., 2014). Thus, the surviving youths quickly became public figures, and they were frequently referred to in the Norwegian media as “the Utøya survivors” or the “Utøya youth.” Skarstein and Schultz (2018), who studied students’ identity configuration after the terrorist attack at Utøya island, found that adolescent survivors experienced a high degree of imposed external framing of their identity not only by the media but also by their peers, teachers, and outside experts. Intrinsically, the terrorist attack was perceived as a central part of who they were not only by themselves but also by others, which, again, may contribute to the survivors’ high and stable centrality scores over time. Finally, the developmental timing of the trauma may be another important factor (i.e., the survivors were mainly youths and young adults). In a study on stressful life events and age differences in event centrality among adults, Boals and colleagues (2012) found that young adults were more likely to construe a stressful event as central to their identity compared with older adults even after controlling for how long ago the event had occurred, type of event, and sex. Together, these findings suggest that younger people may be more likely to consider stressful events as central to their identity compared with older adults, but other longitudinal studies are needed to replicate and further these findings.
The relationship between event centrality and PTSD
In line with findings in previous studies (e.g., Berntsen & Rubin, 2006; Brown et al., 2010; da Silva et al., 2016; Groleau et al., 2013), the results showed that event centrality was significantly and positively associated with concurrent PTSD symptom severity at both time points. However, when we explored the longitudinal association, we found that PTSD symptoms prospectively predicted level of event centrality but not vice versa. This result contrasts with the predominate hypothesis in the field—that high levels of event centrality increase PTSD symptom severity—and suggests that the relationship goes in the opposite direction. In other words, this finding suggests that the degree to which the survivors perceived the terrorist attack to be central to their identity may be an effect, not a cause, of their PTSD symptoms.
Given the findings in previous longitudinal studies, in which event centrality has been found to be related to prospective levels of PTSD, this result was unexpected (Blix et al., 2016; Boals & Ruggero, 2015; Boelen, 2012). However, note that of the previous studies discussed, only Boals and Ruggero (2015) examined the direction of the relationship between the constructs. Whereas they found that event centrality predicted PTSD symptoms 1 month later but not vice versa, our findings suggest the inverse. Although the present study is comparable with Boals and Ruggero’s in terms of the sample’s developmental stage (i.e., primarily young adults), there are other key differences that might account for these discrepant results, including the objective severity and public nature of the event (undergraduate students self-reporting their most stressful life event vs. directly affected survivors of a terrorist attack), the time interval between data collections (1 month vs. over a year), and the time passed since the event (lifetime vs. within the past 2.5 years). Thus, it is possible that the conflicting findings on the longitudinal association between event centrality and PTSD symptoms are related to specific characteristics of the event at hand, the time lag between data collections, and/or the time passed since the event.
According to Epskamp et al. (2018), when studying the long-term relationship between constructs, “the optimal lag interval is often unknown and can even differ between individuals and notably also for different variables” (p. 7). Thus, although it is possible that event centrality does not prospectively predict symptoms of PTSD (as our findings suggest), it is also possible that PTSD symptoms have a more long-term effect on event centrality, whereas the association between event centrality and prospective PTSD symptoms is better characterized by short-term effects not captured by the present design. In other words, the relationship between these two constructs may be more reciprocal and dynamic in nature; perceptions of event centrality and symptoms of PTSD constantly feed into and affect each other. More longitudinal studies are warranted to confirm the direction and nature of the relationship observed here.
Clinically, though, we do not think that it is difficult to explain the finding that high levels of PTSD symptoms at 14 to 15 months predicted high event centrality at 30 to 32 months. It seems only natural that survivors who were clearly profoundly affected by the trauma, with elevated PTSD symptoms more than 1 year after trauma, perceive the terrorist attack to have become a central part of their personal narrative. As noted by Sutherland and Bryant (2005), considering the impact of the traumatic experience on people with high levels of PTSD symptoms, “it would be unexpected if they did not consider their trauma among their most self-defining memories” (p. 595). Interestingly, in line with this perspective, in their qualitative article on students’ identity configuration after the terrorist attack, Skarstein and Schultz (2018) found that accounts of symptoms related to their experiences at Utøya island were framed by the students as identity discourses. This finding illuminates the intertwined relationship between identity and psychopathology.
Study strengths and limitations
The present study makes a significant contribution to the trauma literature in two ways. First, it provides a description of the level and development of event centrality reported by a trauma-exposed sample at two different time points. Second, it is one of very few published studies exploring the bidirectional relationship between event centrality and symptoms of PTSD over time and the first to do so among young survivors of a terrorist attack. Other study strengths include successfully tracking survivors for 2.5 years following such a circumscribed traumatic event, a relatively high response rate, and low levels of missing data.
Certain limitations should be considered when evaluating the results. First, it is important to note that our initial data collection on event centrality was conducted 14 to 15 months postattack. Thus, we do not know how the survivors would have scored on centrality at an earlier time point after the attack or how this would have related to subsequent levels of PTSD. Earlier and more frequent measurements of event centrality could provide important knowledge about how soon event centrality is “established” after a traumatic event, its temporal stability, and how perceptions of centrality relate to psychopathology.
Second, although the data are longitudinal, because they are observational and not experimental, they cannot provide conclusive support for a causal relationship. However, because we can distinguish the effect of PTSD on CES from that of CES on PTSD, the CLPM provides stronger evidence on the cause-effect relation between these constructs than a cross-sectional regression model, in which experimentation is not feasible (Little, Card, Preacher, & McConnell, 2009).
Third, despite the aforementioned strength of the cross-lagged model, it is worth noting that it does not take into account the mean level change in the construct over time, and because we had only two waves of data, a clear separation of within- and between-person level was not possible in our cross-lagged analysis. In other words, even with high autoregressive path coefficients between T2 and T3, we do not know whether the participants showed relatively similar or very different changes in the constructs of interest over time. Other statistical models, such as the random-intercept-CLPM (Hamaker, Kuiper, & Grasman, 2015), separate within-person process from between-person effects, thereby overcoming this limitation, but at least three data collections are necessary to identify these models. Thus, to get a better understanding of the longitudinal relationship between event centrality and PTSD symptoms, future longitudinal studies with frequent data collections are warranted.
Finally, the nature of the traumatic event (i.e., geographically constricted to a small island, less variability in the trauma exposure than in other disasters, intense and prolonged media attention, the survivors’ young age, and the fact that the survivors were a group before the attack as well; 82% were members of the Norwegian Labor Party’s youth organization) may impede the generalizability of the findings.
Implications and future directions
The study findings contribute to the literature by suggesting that although levels of event centrality and PTSD symptoms are strongly and positively associated in a trauma-exposed sample, contrary to the predominating hypothesis in the field, centrality does not seem to prospectively predict PTSD symptoms. Thus, although it has recently been advocated that treatments focusing on narrative centrality “hold great promise for reducing trauma-related symptoms” (Boals & Murrell, 2016, p. 481) and it can be useful for clinicians to attend to centrality in their work with trauma-exposed clients (Groleau et al., 2013), our findings suggests that targeting and reducing trauma survivors’ perception of the traumatic event as a central component of their identity and life story will not necessarily reduce their prospective levels of PTSD symptoms. Because our lag interval between data collections was over a year, we could not explore potential short-term effects of event centrality on psychopathology. However, in a recent experimental study on the effect of manipulating centrality, Boals and Murrell (2016) found a reduction in event centrality and PTSD symptoms from pre- to posttreatment, but this reduction did not hold 6 weeks later. The authors argued that this may be related to attrition and subsequent reduction in statistical power but noted that future studies are needed to examine how long a manipulation of event centrality lasts. We agree that more treatment studies with short time lags and interventions specifically targeting event centrality could help to fill this knowledge gap.
Supplemental Material
Glad_Supplemental_Material – Supplemental material for Cross-Lagged Association Between Symptoms of Posttraumatic Stress Disorder and Perceived Centrality of a Terrorist Attack
Supplemental material, Glad_Supplemental_Material for Cross-Lagged Association Between Symptoms of Posttraumatic Stress Disorder and Perceived Centrality of a Terrorist Attack by Kristin Alve Glad, Nikolai Olavi Czajkowski, Grete Dyb and Gertrud S. Hafstad in Clinical Psychological Science
Footnotes
Acknowledgements
This effort was made possible through the support of the Norwegian Extra Foundation for Health and Rehabilitation and the Norwegian Council for Medical Health, for which we express our gratitude. We sincerely thank everyone who participated in this study. Finally, we thank Marianne Skogbrott Birkeland and Ines Blix, who provided important input on the interpretation of our findings.
Action Editor
Kenneth J. Sher served as action editor for this article.
Author Contributions
K. A. Glad contributed to the design of the study, acquisition of the data, and statistical analyses and wrote the manuscript. N. O. Czajkowski contributed to the statistical analyses, interpretation of the data, and revising the manuscript. G. S. Hafstad contributed to the design of the study, acquisition of the data, and revising the manuscript. G. Dyb was the study’s principal investigator and contributed to the design of the study, acquisition of the data, and revising the manuscript. All of the authors approved the final manuscript for submission.
Declaration of Conflicting Interests
The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.