
Abstract
Major depressive disorder (MDD) is associated with persistent, impaired life functioning. Motivational deficits in physical and cognitive effort expenditure have not been evaluated as contributors to functional impairment in MDD. In this study, we adapted parallel measures of choices to expend physical and cognitive effort and assessed their associations with symptoms, cognition, and life functioning in 44 participants with MDD. Higher anhedonia severity predicted lower motivation for physical effort but not for cognitive effort. Lower cognitive effort motivation was associated with poorer life functioning even after controlling for previously established predictors of symptoms and cognitive impairment. Reduced cognitive effort motivation also had an indirect effect on the relationship between impaired cognitive and life functioning. Findings suggest motivational deficits in MDD present different barriers for recovery depending on the type of effort that is avoided. Physical effort motivation is associated with anhedonia severity, whereas cognitive effort motivation is relevant to life functioning.
Major depressive disorder (MDD) is the largest contributor to impaired life functioning among all medical conditions (Üstün, Ayuso-Mateos, Chatterji, Mathers, & Murray, 2004; Vos et al., 2012). People with MDD experience more days in bed, higher financial strain, restricted engagement in recreation, strained relationships, and significant limitations in work, school, or household duties compared with their healthy peers (Judd, Paulus, Wells, & Rapaport, 1996; Lerner et al., 2004; Lerner & Henke, 2008; Petersen et al., 2004; Wang et al., 2004). Individuals with MDD perceive their functional impairment as significant; indeed, they rate recovery of life functioning as a more important treatment goal than symptom remission (Zimmerman et al., 2006). However, recovering life functioning remains elusive given that impairments are typically persistent even after correlates of functioning such as depressive symptoms and cognitive deficits are addressed (Andrews, 2001; Gupta et al., 2013; Hirschfeld et al., 2002; Miller et al., 1998; Naismith et al., 2011; Naismith, Redoblado-Hodge, Lewis, Scott, & Hickie, 2010). A closer look at patterns of performance on cognitive testing suggests that a form of motivation deficit may be contributing to the maintenance and exacerbation of functional impairments in MDD. Depressed individuals were found to have an oversensitive reaction to failure on tests that assess cognitive functioning compared with control participants because they were more likely to fail trials after making errors (Elliott et al., 1996; Elliott, Sahakian, Herrod, Robbins, & Paykel, 1997). Along the same lines of interpretation, reduced motivation to attempt cognitively effortful tasks after experiencing challenges in carrying out daily functional roles and responsibilities could be the process by which cognitive and functional impairments persist for individuals with MDD. Researchers have yet to investigate this question, that is, the degree to which cognitive deficits and reduced motivation to expend cognitive effort interact to produce impaired functioning.
Cognitive deficits are more prevalent and pervasive in individuals with MDD than once thought even though the degree of impairment may be only mild to moderate in severity (Cohen’s d = 0.22–0.61; McIntyre et al., 2013; Rock, Roiser, Riedel, & Blackwell, 2014). Impaired cognitive functioning has emerged as an important predictor of reduced life functioning in individuals with MDD above and beyond what is accounted for by depressive symptoms (Baune et al., 2010; Godard, Grondin, Baruch, & Lafleur, 2011; Gupta et al., 2013; Jaeger, Berns, Uzelac, & Davis-Conway, 2006; McCall & Dunn, 2003; Withall, Harris, & Cumming, 2017). Even when cognitive functioning is intact or remediated by interventions that target cognitive functioning (e.g., cognitive remediation), depressed individuals often have minimal or delayed improvements in everyday roles and activities (Bowie, Grossman, Gupta, Holshausen, & Best, 2016; Gupta et al., 2013; Naismith et al., 2010; Naismith et al., 2011). Only when factors such as low motivation, interest, or engagement are also addressed in treatment do we see meaningful transfer of cognitive gains to improvements in life functioning (Bowie et al., 2016; Meusel, 2012). Reduced motivation to expend cognitive effort may limit the degree to which individuals with MDD use cognitive abilities in daily life, thereby perpetuating impaired life functioning despite actual cognitive competency.
Cognitive functioning does not occur in isolation of psychosocial factors, and this may be particularly relevant in depression, in which negative reactions to failures and low motivation exacerbate cognitive performance deficits. In multitrial cognitive testing, individuals with MDD were more likely to demonstrate poorer performance following failure on a prior trial (Elliott et al., 1996; Elliott et al., 1997). Symptoms of low motivation in MDD also negatively influence cognitive functioning. Individuals with MDD performed more poorly and exhibited longer response times on tests with higher demands of cognitive resources compared with control participants (Hammar, 2003; Hammar et al., 2011; Hammar, Lund, & Hugdahl, 2003; Hasher & Zacks, 1979). Higher depression symptom severity has been associated with avoiding cognitive effort, and the more avoidance, the lower the quality of life (Bowie, Milanovic, Tran, & Cassidy, 2017). Taken together, we suggest that in the face of cognitive challenge, depressed individuals have lower motivation to approach tasks, which could further reinforce poor self-efficacy in cognitive abilities and impaired cognitive functioning.
The cognitive-effort hypothesis posits that impaired performance observed in cognitive testing may be due at least in part to avoidance of tasks that require high as opposed to low cognitive load (Ellis & Ashbrook, 1988; Hasher & Zacks, 1979). Cognitive effort avoidance appears to be a matter of inefficient cognitive resource allocation rather than reduced resource capacity (Elliott et al., 1997; Elliott, Sahakian, Michael, Paykel, & Dolan, 1998). Avoidance of cognitive effort may reduce encounters with situations that place high demands on cognitive functions but might indeed be necessary to complete daily roles and responsibilities. The functional consequences of cognitive effort avoidance have yet to be explored, and this may be due to limited measurement tools that have been validated in individuals with MDD. Preliminary evidence in line with the cognitive-effort hypothesis has relied on secondary analyses of cognitive tests that are designed to measure cognitive functioning instead of motivation to perform cognitively effortful tasks.
Prior research has indexed motivation to expend cognitive effort in healthy adults as avoidant preferences (Kool, Mcguire, & Botvinick, 2010; Westbrook et al., 2013) and decisions to expend effort for reward (Chong et al., 2017; Lopez-Gamundi & Wardle, 2018; Schmidt, Lebreton, Cléry-Melin, Daunizeau, & Pessiglione, 2012), as demonstrated through experimental tasks. In one study, researchers administered an experimental task that aimed to measure a participant’s willingness to repeatedly exert mild cognitive effort for monetary reward in a depressed sample (Hershenberg et al., 2016). In this study, decisions to complete trial-by-trial number-pair comparisons were examined. Over successive trial sets, the amount of effort (i.e., number of correct trials) required to achieve a reward increased. Depressed participants on this task were more likely to skip trials at lower success criteria than control participants. Despite preliminary evidence of impaired persistence of mild cognitive effort in depressed individuals, very little research has assessed motivation to initiate greater cognitive effort as a function of reward in this population. Furthermore, early validation data for cognitive effort measures found that performance covaried with individual differences in cognitive functioning and did not correlate with motivation symptoms in MDD such as anhedonia—the experience of low pleasure and interest in enjoyable activities (Kool et al., 2010; Lopez-Gamundi & Wardle, 2018). Thus, in order to delineate the role of cognitive effort motivation from cognitive deficits in the prediction of impaired life functioning in individuals with MDD, we developed a novel cognitive-effort task for the current study.
Avoidance of cognitive effort might be driven by a blunted motivation system. Motivation to expend effort stems from a decision-making process that involves the hedonic capacity to evaluate reward, consideration of the probability of receiving the reward, and assessment of the cost of effort demands (Kring & Barch, 2014). Experimental paradigms examining choices to expend physical effort for reward via a cost–benefit decision-making framework have been developed and have consistently shown that patients are less motivated to expend effort for reward (for review, see Culbreth, Moran, & Barch, 2018). The effort expenditure for rewards task (EEfRT) is a particularly well-validated paradigm in depressed populations. Participants with MDD, both those who were symptomatic and those whose MDD was in remission, chose fewer high-physical-effort trials for greater monetary reward on the EEfRT than control participants (Treadway, Bossaller, Shelton, & Zald, 2012; Treadway, Buckholtz, Schwartzman, Lambert, & Zald, 2009; Yang et al., 2014). This lower motivation or at times avoidance of physical effort expenditure corresponded with the severity of anhedonia. Down-regulation of goal-directed behavior despite the real or perceived benefits of task engagement appears to be driven by blunted reward sensitivity and attenuated activation of reward neural circuitry associated with anhedonia (Pizzagalli, Iosifescu, Hallett, Ratner, & Fava, 2008; Pizzagalli, Jahn, & O’Shea, 2005; Treadway and Zaid, 2011).
This line of translational neuroscience research has advanced understanding of the link between motivation deficits and anhedonia symptoms in individuals with MDD. It is unknown whether cognitive motivation deficits measured in contexts that require cost–benefit analysis are also sensitive indicators of symptom severity and life functioning in individuals with MDD. Prior research in schizophrenia has found that lower motivation to expend cognitive effort is related to poor cognitive functioning (Horan et al., 2015), which is an established predictor of life functioning in both MDD and schizophrenia groups (Evans, Iverson, Yatham, & Lam, 2014; Green, 1996). In the present study, we adapted measures to elucidate the interaction of hedonic deficits to expend both physical and cognitive effort and evaluated their significance in predicting barriers to recovery in MDD: anhedonia severity and functional impairment.
The effort tasks in the present study required participants with MDD to make a series of choices between completing a low-effort/low-reward (“easy”) or high-effort/high-reward (“hard”) activity. For the physical-effort task, participants chose between easy and hard finger-tapping activities, whereas in the cognitive-effort task, the choice was between two difficulty levels of a working memory activity. To assess the validity of the novel cognitive-effort task, we asked comparison participants to complete both physical- and cognitive-effort tasks and outcome measures. This afforded examination of differences in hard choices by participant group and type of effort. In line with preliminary findings of the cognitive-effort hypothesis (Ellis & Ashbrook, 1988; Hasher & Zacks, 1979), we hypothesized that the MDD group would complete significantly fewer hard cognitive- and physical-effort trials relative to comparison participants. The validity of adapted effort tasks was also assessed by examining whether symptom or diagnostic factors (anhedonia and MDD status) and nonsymptom parameters (reward magnitude and probability of reward receipt) predicted the likelihood of choosing to produce physical and cognitive effort. We hypothesized that higher anhedonia would predict lower likelihood of choosing the hard trials in both effort tasks and that reward and probability would be relatively weaker predictors of hard choices in the MDD group but not in the comparison group.
In the MDD group, we tested the role of motivation to expend effort in two hypothesized models of life functioning. First, we assessed whether motivation to expend physical or cognitive effort predicted functioning after accounting for cognitive functioning and symptom severity. Given that impaired functioning in individuals with MDD persists despite resolution of depressive (Andrews, 2001; Hirschfeld et al., 2002; Miller et al., 1998) and cognitive symptoms (Bowie et al., 2016), we hypothesized that motivation to expend cognitive effort would be a unique predictor of functional impairment. Second, we tested a model that proposed cognitive functioning would be inversely related to functioning through its relationship with motivation to exert cognitive but not physical effort for reward.
Method
This study received approval from the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board.
Participants
Participants were individuals who responded to posters or online advertisement or were recruited via external referrals from community mental health clinics and the mood disorders outpatient service at a tertiary psychiatric hospital. Over 5 months, 44 depressed and 44 comparison participants were screened by phone for inclusion criteria and interviewed with the fifth version of the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998). Attempts to age- and gender-match for the full clinical sample were not successful, and eight comparison participants did not proceed with study procedures. The final sample included 44 depressed participants (31 women) and 36 comparison participants (27 women).
Participants in the MDD group met criteria for a past or current major depressive episode. Participants were included in the comparison group if they had no psychiatric illness as determined from the MINI. Potential participants were excluded from either group if they had received a medical diagnosis associated with known cognitive impairments (e.g., multiple sclerosis, traumatic brain injury, or learning disability), had been diagnosed with psychotic disorder or bipolar disorder, had an uncorrectable vision or hearing impairment, had used a controlled substance within the past 3 weeks, or had a history of substance dependence.
Measures and materials
Effort-based decision-making tasks
Following the cost–benefit decision-making framework of the EEfRT (Treadway et al., 2009), the physical- and cognitive-effort tasks required respondents to choose between completing a low-effort, low-payoff (presented to participants as “easy”) or a high-effort, high-payoff (“hard”) version of the task over multiple trials. Each trial in both tasks proceeded in the same sequence (Fig. 1). The easy trial always offered $1.00 for successful completion, and the hard trial offered one of 10 reward magnitudes ranging from $1.25 to $3.50 in 25-cent increments. Instructions indicated that not all trials successfully completed would guarantee winning the reward and that the probability of reward receipt assigned for that trial indicated the odds of winning. Probabilities of reward receipt included 12%, 50%, and 88%. Each reward magnitude for the hard trials was presented once for each probability level (yielding 30 total trials per effort task). The sequence of trials in both effort tasks was prerandomized.
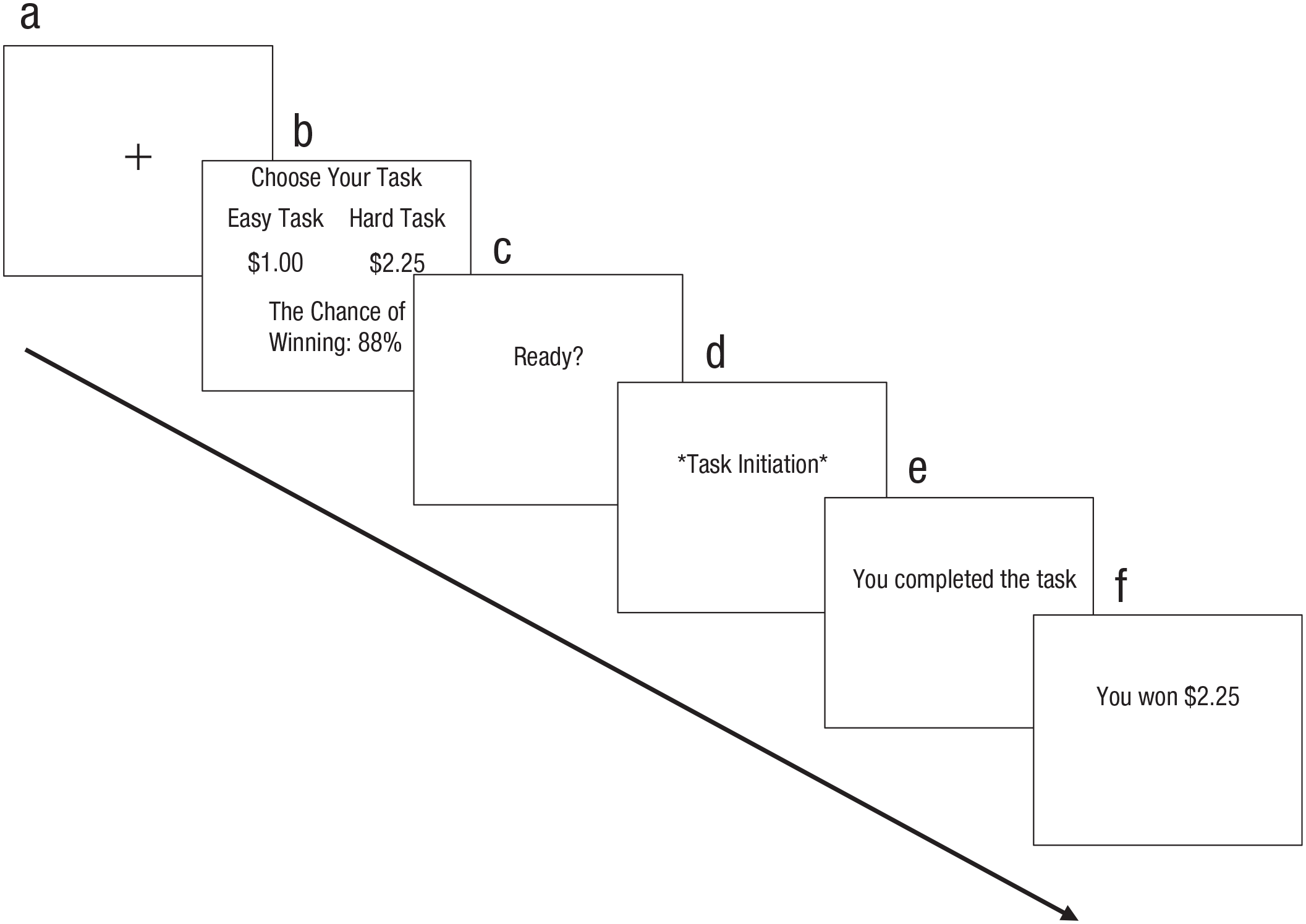
Schematic diagram of a single trial of both the physical- and cognitive-effort tasks. (a) Participants view a fixation cue for 500 ms. (b) Participants choose one of the tasks. (c) A “ready” screen is shown for 500 ms. (d) Completion of selected trial is displayed. (e) Feedback on task completion appears for 1 s. (f) Reward feedback appears for 3 s.
To encourage participants to evaluate the costs and benefits of their decisions for every trial, we manipulated certain conditions of the effort tasks, such as the original EEfRT, and made them explicit to all participants. Variable probability of reward receipt between trials was intended to encourage participants to thoughtfully evaluate whether they were willing to expend high effort for the trial. The payout participants received at the end of the experiment was one randomly selected reward value from their set of successful “win” trials. Thus, the more hard trials participants won, the greater the odds that their incentive was worth more than $1. However, participants were told they had 20 min to complete as many trials as they could and to keep in mind that the hard trial is more costly because they were longer and required more effort. Thus, more hard trials chosen meant that fewer trials were possible overall within the time limit and a greater risk of missing out on high-value, high-probability trials that might come later. Payouts from each effort task were made after participants finished both tasks.
The physical-effort task required participants to press a key a set number of times within 30 s. If an easy trial was chosen, participants had to use the index finger on the dominant hand to complete the key presses. For hard trials, they had to tap using the pinky finger of the nondominant hand. The time remaining was displayed in the top right corner of the screen while a blank bar in the center incrementally filled with lines to reflect progress during the task. In the cognitive task, participants completed one of two difficulty levels of the letter variant N-back working memory task (procedure detailed in Harvey et al., 2005). The N-back task required participants to view a 16-item prerandomized list of consonant letters (each appeared for 500 ms). Participants had to report with a “yes” or “no” key press (1.5-s response window) if the currently displayed letter matched the letter that was shown N items earlier in the sequence. The one-back and two-back difficulty levels of the N-back were used for the easy and hard trials, respectively. N-back difficulty levels were determined on the basis of self-report and task performance data on the one-back, two-back, and three-back that was borrowed from a study with a separate sample of participants with MDD who were looking to receive cognitive remediation treatment (study in progress). In that study, two-back trials were rated at baseline visit by participants with MDD as being more challenging than one-back despite performance declines that were consistent with a comparison group. We therefore selected the one-back and two-back difficulty levels for the easy and hard levels, respectively, as a manipulation of perceived cognitive effort in the current study.
The design of the effort tasks used in our study departed from the original EEfRT paradigm in the determination of criteria for successful completion of a trial (success criteria). The number of key presses in the physical-effort task and the accuracy rate in the cognitive-effort task required to complete a trial were determined on the basis of each participant’s best performance on calibration trials conducted before testing. This modification aimed to control for individual differences in ability level influencing choices of easy or hard trials. For the physical-effort task, calibration involved three 30-s practice runs of both the easy and the hard trials, presented in that order for a total of six practice trials. Participants were not informed of the purpose of the practice trials for calibration. They were instructed to press the key with the designated finger as fast as they could. Success criteria for the easy and hard trials were calculated as 50% and 80% of the highest number of key presses achieved on the hard calibration trials, respectively. This followed previously validated calibration practices that aimed to ensure a clear discrepancy in difficulty levels and to ensure the success criteria were reasonably within limits of ability (Fervaha et al., 2015). In the cognitive-effort task, the accuracy that participants were required to reach for successful completion of the task was individually calibrated for ability level using the same approach as for the physical-effort task (administration of three practice trials of both the easy and hard trials). Success criteria for the easy and hard trials were calculated as 50% and 80% of the highest accuracy achieved on the two-back, respectively.
Motivation to expend effort
Our dependent variable from each effort task was the proportion of hard choices made for trials with large relative to small reward and probability values (effort-task expected value), computed as difference scores according to formulas described in previous research that compared performance across multiple effort tasks (Horan et al., 2015). Higher scores for physical and cognitive effort-task expected value represented greater motivation to expend the respective type of effort for large over small incentives.
Cognitive functioning
We administered a brief battery of standardized neuropsychological tests relevant to MDD (Rock et al., 2014). This included tests of processing speed, sustained attention, verbal learning, working memory, and executive functioning as measured by Digit Symbol Substitution Task (DSST; Keefe, 1999), Trail Making Test Part A (TMT-A; Partington & Leiter, 1949), Hopkins Verbal Learning Test–Revised (HVLT-R; Brandt & Benedict, 2001), Letter Number Sequencing Test (LNS; Gold, Carpenter, Randolph, Goldberg, & Weinberger, 1997), and Trail Making Test Part B (TMT-B; Partington & Leiter, 1949), respectively. Raw scores were converted to age- and education-corrected standard scores on the basis of normative data published in the respective test manuals and then converted to z scores. Consistent with validated practices, a neurocognitive composite score representing an equally weighted average of all z scores was computed (Nuechterlein & Green, 2006).
Life functioning
Impairment in vocational functioning (employment, household, and school), interpersonal relations, recreation, and life satisfaction were assessed using the semistructured Longitudinal Interval Follow-up Evaluation–Range of Impaired Functioning Tool (LIFE-RIFT; Leon et al., 1999). Higher LIFE-RIFT total scores indicated more severe functional impairment. Internal consistency of the scale was good (Cronbach’s α = .84).
Depressive symptom severity
The Hamilton Rating Scale for Depression (HAM-D; Hamilton, 1960) was used to assess depressive symptoms in the past week. We computed total HAM-D scores so that higher scores indicate greater severity of depressive symptoms. The internal consistency of the HAM-D for the MDD sample was good (Cronbach’s α = .85).
Anhedonia
Anhedonia was operationalized as the capacity to experience interest or pleasure in everyday activities in the past few days, as captured by the 14-item self-report questionnaire, Snaith-Hamilton Pleasure Scale (SHAPS; Snaith et al., 1995). Responses were dichotomized (disagreement = 1, agreement = 0) and summed to produce a continuous score. A total score of 2 or more is considered clinically significant anhedonia. The internal consistency of SHAPS for the full sample was good (Cronbach’s α = .89).
Procedure
A research assistant who was blind to diagnoses and hypotheses administered the cognitive assessment battery, followed by the physical- and cognitive-effort tasks, the order of which was counterbalanced across participants. Both effort tasks followed the same sequence of events: demonstration of the easy task (i.e., one-back or dominant hand), calibration trials for the easy task, demonstration of the hard task (i.e., two-back or nondominant hand), calibration trials for the hard task, game instructions, three practice trials, and finally the 30 test trials. Orientation to each paradigm took 15 to 20 min, and the test trials each lasted approximately 20 min. Then, interviews were conducted for demographic information, symptoms, and functional impairment by trained clinical psychology doctoral students. Consensus meetings were held with a clinical psychologist (C. R. Bowie) to review each rating for HAM-D and LIFE-RIFT interviews. The SHAPS self-report form was administered last. The visit lasted about 2 hr, and participants were compensated $40 plus earnings from the effort tasks.
Statistical analysis
Because the adapted physical- and cognitive-effort tasks had not been previously administered, especially in an MDD sample, we conducted case-control comparison analyses to characterize their psychometric properties (e.g., calibration performance, completion rates, decision-making latency). We used parametric tests whenever variables did not violate normality. We conducted a validity test of the adapted effort tasks by examining mean differences via a mixed-model analysis of variance (ANOVA) with participant group as the between-subjects factor and effort type as the within-subjects factor. In addition, following previous analytical methods for the EEfRT (Treadway et al., 2009; Treadway et al., 2012), factors that moderated trial choices were assessed via generalized estimating equation (GEE) models (Liang, Beaty, & Cohen, 1986; Zeger & Liang, 1986). We applied an autoregressive working correlation matrix and a binary logistic distribution to model the probability of choosing the hard task (hard = 1, easy = 0) because these produced the best fit statistic for the data. GEE models included the main effect variables of reward magnitude, probability of reward receipt, incentive value (Reward × Probability), anhedonia, group (MDD = 1, comparison = 0), and the interaction between anhedonia and group. Any significant interactions were followed up by conducting within-groups GEE models.
The models of functional impairment included the MDD sample only. To address whether motivation to expend effort predicted impaired life functioning after controlling for cognitive functioning and symptoms, we performed a hierarchical regression model. Anhedonia, depressive symptom severity, and cognitive functioning—established correlates of life functioning in MDD—were entered in the first step, and effort-task expected value was entered in the second step. We performed a parallel indirect effects analysis using the PROCESS macro (Model 4; Hayes, 2013) for IBM SPSS (Version 25) to examine whether effort-task expected value statistically had an indirect effect on the relationship between cognition and functional impairment in MDD. Bias-corrected bootstrap confidence intervals based on 1,000 bootstrap samples were computed to estimate indirect effects of hypothesized mediators.
Results
Participant characteristics
Descriptive statistics and between-groups comparisons of both demographic and clinical variables are presented in Table 1. Groups did not significantly differ by age, t(78) = −0.45, p = .65; gender, χ2(1) = 0.21, p = .65; years of education, Mann-Whitney U = 638.00, p = .13, ethnicity, χ2(1) = 3.11, p = .08; or marital status, χ2(1) = 1.78, p = .18. MDD participants were significantly more impaired in depressive symptoms, anhedonia, and life functioning but not in cognitive functioning. According to HAM-D scores, all MDD participants reported at least a few depressive symptoms (scores ranged from 3 to 36). Only four MDD participants scored less than 7 (the cut-off for normal limits) on the HAM-D during the time of testing. Thus, we ran all subsequent analyses with and without data from the participants who displayed subclinical levels of depressive symptoms to examine the effect of depression status on results.
Descriptive Statistics and Group Comparisons of Demographic and Clinical Variables
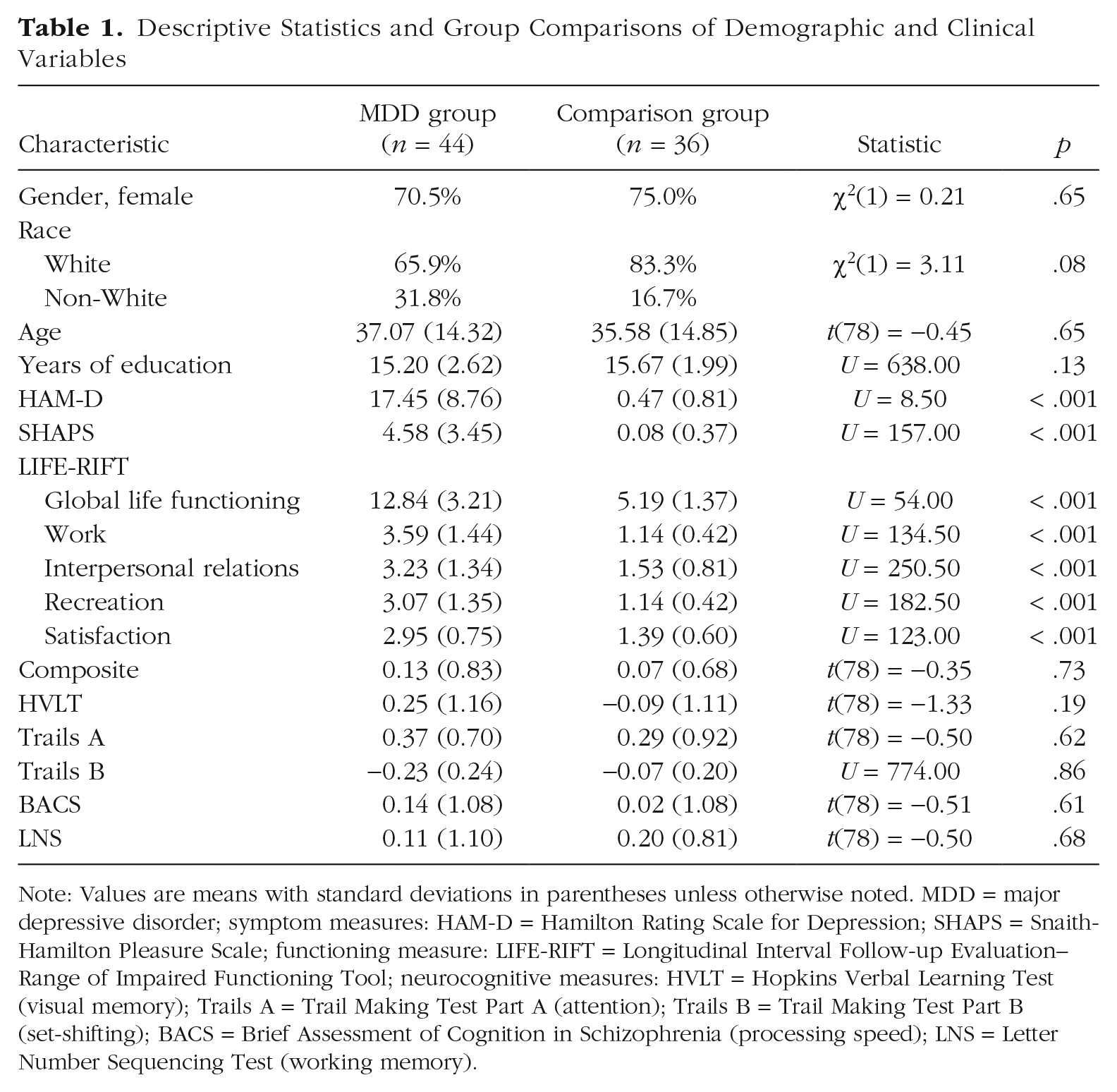
Note: Values are means with standard deviations in parentheses unless otherwise noted. MDD = major depressive disorder; symptom measures: HAM-D = Hamilton Rating Scale for Depression; SHAPS = Snaith-Hamilton Pleasure Scale; functioning measure: LIFE-RIFT = Longitudinal Interval Follow-up Evaluation–Range of Impaired Functioning Tool; neurocognitive measures: HVLT = Hopkins Verbal Learning Test (visual memory); Trails A = Trail Making Test Part A (attention); Trails B = Trail Making Test Part B (set-shifting); BACS = Brief Assessment of Cognition in Schizophrenia (processing speed); LNS = Letter Number Sequencing Test (working memory).
Psychometric properties of effort tasks
Calibration performance
The calibration performance on the hard physical task (greatest number of key presses) significantly differed by group; comparison participants (M = 137.78, SD = 27.38) made significantly more key presses than MDD participants (M = 126.28, SD = 20.60), t(78) = 2.14, p = .04.
We conducted a mixed-model analysis of covariance to assess whether calibration performance on the cognitive-effort task (highest accuracy rate) differed between groups and effort levels (one-back vs. two-back) while controlling for individual differences in processing speed (DSST) and working memory/executive functioning (TMT-B and LNS). In line with the effort manipulation of the cognitive task, there was a significant main effect of effort level, whereby the highest accuracy achieved by all participants on the one-back (M = 96.98%, SE = 0.78) was significantly greater than the highest accuracy achieved on the two-back calibration trials (M = 87.96%, SE = 1.08), F(1, 75) = 65.35, p < .001. The main effect of group was also significant, F(1, 75) = 4.18, p = .04. Across all effort levels, the highest accuracy rates achieved by MDD participants (M = 90.85%, SE = 1.05) were significantly lower than the highest accuracy rates achieved by comparison participants (M = 94.08%, SE = 1.16). The group by effort level interaction was nonsignificant, F(1, 75) = 0.09, p = .77, suggesting that the group difference in calibration performance was consistent across the one-back and two-back. Across all participants, calibration performance between the one-back and two-back was not significantly different as a function of processing speed—DSST: F(1, 75) = 2.62, p = .10—and working memory/executive functioning abilities—TMT-B: F(1, 75) = 3.42, p = .07; LNS: F(1, 75) = 0.80, p = .37.
We examined the strength of the correlational relationships between calibration performance on the cognitive-effort task and individual differences in processing speed (DSST), sustained attention (TMT-A), working memory/executive functioning (LNS and TMT-B). In the comparison group, the calibration performance on the easy task (one-back) was not significantly related to performance on the DSST (r = .07, p = .70), TMT-A (r = .17, p = .33), LNS (r = .21, p = .21), and TMT-B (r = .27, p = .11) measures. Calibration performance on the hard task (two-back) by comparison participants was significantly related to TMT-B scores (r = .38, p = .02) but was not significantly related to DSST (r = .27, p = .12), TMT-A (r = .17, p = .33), and LNS (r = .23, p = .17) scores. In the MDD group, the calibration performance on the easy cognitive-effort task was not significantly related to performance on any cognitive tests (DSST: r = .14, p = .38; TMT-A: r = −.12, p = .45; LNS: r = .21, p = .16; TMT-B: r = .02, p = .91). On the hard task, calibration performance by MDD participants was significantly associated with scores on the DSST (r = .41, p = .006) and TMT-B (r = .31, p = .04) but not with scores on the TMT-A (r = .06, p = .68) and LNS (r = .21, p = .18).
Completion rates
Both MDD and comparison participants met the success criteria for 100% of the trials they completed in the physical-effort task regardless of hard or easy choices. In terms of the cognitive-effort task, there were no significant group differences in completion rate for easy (one-back) trials (comparison: M = 99.74%, SD = 1.54; MDD: M = 99.88%, SD = 0.76), Mann-Whitney U = 748.00, p = .87, and hard (two-back) trials (comparison: M = 91.19%, SD = 18.38; MDD: M = 88.62%, SD = 18.59), Mann-Whitney U = 666.00, p = .71.
We examined the relationships between the proportion of easy (one-back) and hard (two-back) cognitive-effort task trials chosen that were successfully completed and individual differences in processing speed (DSST), sustained attention (TMT-A), working memory/executive functioning (LNS and TMT-B). In the comparison group, higher DSST scores significantly correlated with a greater proportion of successfully completed one-back trials, r = .35, p = .04. The proportion of successfully completed one-back trials by comparison participants did not significantly correlate with any other domain of cognitive functioning (TMT-A: r = .16, p = .35; TMT-B: r = .08, p = .66; LNS: r = −.04, p = .81). In addition, the proportion of successfully completed two-back trials by comparison participants did not significantly correlate with individual differences in cognitive functioning (DSST: r = .13, p = .47; TMT-A: r = .09, p = .62; TMT-B: r = .07, p = .67; LNS: r = .03, p = .86). In the MDD group, greater proportions of successfully completed one-back trials was significantly correlated with higher LNS scores (r = .31, p = .04) but did not share a significant relationship with DSST (r = .20, p = .19), TMT-A (r = .29, p = .06), and TMT-B (r = .02, p = .89) scores. The proportion of successfully completed two-back trials by MDD participants was not significantly associated with individual differences in cognitive functioning (DSST: r = .26, p = .11; TMT-A: r = −.13, p = .42; TMT-B: r = .15, p = .35; LNS: r = .05, p = .76).
Decision-making latency
The groups did not differ in mean decision-making latency (in seconds) for the physical (comparison: M = 2.90, SD = 1.35; MDD: M = 2.93, SD = 1.62), t(78) = 0.24, p = .81, or cognitive-effort tasks (comparison: M = 3.40, SD = 1.38; MDD: M = 3.31, SD = 1.53), t(78) = 0.53, p = .60.
Counterbalance effect
The counterbalance effect of incentivized hard choices as a function of the physical- and cognitive-effort tasks was examined. The main effect of counterbalanced task order was nonsignificant, F(1, 73) = .006, p = .94, as was the order by effort interaction, F(1, 73) = .13, p = .72.
Group differences in motivation to expend effort
We tested for differences in effort-task expected value as a function of group and effort type with a mixed model ANOVA. Box’s test of equal within-groups covariance was significant, Box’s M = 42.17, p < .001, and thus Pillai’s trace criterion was used to describe within-subjects effects. The main effect of effort type was significant, F(1, 73) = 10.24, p = .002, η p 2 = .12, observed power = .88, whereby participants chose more hard, high-expected value trials over easy, low-expected value ones in the physical (M = 0.91, SE = 0.03) than the cognitive-effort task (M = 0.77, SE = 0.04). The main effect of group was not significant, F(1, 73) = 3.05, p = .085, η p 2 = .04, but trended toward MDD participants (M = 0.79, SE = 0.04) choosing fewer hard, high-expected-value trials over easy, low-expected-value trials compared with control participants (M = 0.89, SE = 0.04) across both effort tasks. There was no significant interaction between group and effort, F(1, 73) = 0.09, p = .77. Results did not change after covarying for working memory and executive functioning and when the model was run with the exclusion of MDD participants who displayed subclinical depressive symptoms at the time of testing. After adjusting for the effect of calibration performance (maximum scores achieved on physical and cognitive calibration trials), the significant main effect of effort did not survive, F(1, 70) = 1.08, p = .30, η p 2 = .02, observed power = .18.
Predictors of hard-trial choices
Two main GEE models were independently tested to examine which factors predicted the odds of choosing hard trials. Each model included basic parameters of the effort tasks: reward, probability, and expected value (Reward × Probability).
Physical-effort-task choices
Model 1 tested for the interaction between anhedonia and group on preferences for hard trials during the physical-effort task. Increases in level of reward (b = 0.23, p = .001), probability (b = 1.14, p < .001), expected value (b = 0.09, p = .003), and anhedonia (b = 0.70, p = .001) were significant predictors of hard-physical-task choices. The main effect of group was not significant (b = 0.14, p = .60). However, the anhedonia by group interaction was significant (b = −0.70, p = .002), indicating the degree that anhedonia severity predicted the likelihood of hard choices in the physical-effort task depended on whether the participant had MDD or not.
We followed up the significant anhedonia by group interaction on hard-physical-task choices with separate within-groups GEE models. In the comparison group, increases in reward (b = 0.30, p = .01) and probability (b = 1.40, p < .001) were significant predictors of hard-physical-task choices. Expected value was not a significant predictor of hard choices (b = 0.10, p = .087). Anhedonia was a significant predictor of hard-physical-task choices (b = 2.05, p = .002); however, we took caution in interpreting this finding because the range of anhedonia severity in control participants was restricted (M = 0.08, SD = 0.37) and below clinical significance (clinical cutoff score of 2). The interaction terms of Reward × Anhedonia (b = −0.27, p = .23), Probability × Anhedonia (b = −0.62, p = .27), and Expected Value × Anhedonia (b = 0.15, p = .49) were not significant.
The within-subjects GEE model for the MDD group revealed the main effect of reward (b = 0.08, p = .36) and probability levels (b = 0.48, p = .12) on hard-physical-task choices were not significant. Expected value was a significant predictor of hard-physical-task choices (b = 0.11, p = .01) such that for every one-unit increase in expected value, the likelihood of MDD participants choosing the hard task was 1.12 times more likely. Anhedonia was also a significant predictor of hard-physical-task choices (b = −0.37, p = .03). For every one-unit increase in anhedonia severity, the odds that MDD participants chose the hard physical task was 1.45 times less likely. The Reward × Anhedonia (b = 0.03, p = .12) and Expected Value × Anhedonia (b = −0.009, p = .35) interaction terms were not significant. The Probability × Anhedonia interaction on hard-physical-task choices was significant (b = 0.14, p = .02).
The results did not change when Model 1 covaried for the effect of calibration performance (maximum button presses achieved on hard calibration trials). Note that this analysis revealed that the main effect of calibration performance on preferences for hard trials during the physical-effort task was nonsignificant (b = −0.005, p = .56). The results of the within-participants GEE model were mostly unchanged when run on the subsample of MDD participants who met the clinical threshold of depressive symptoms. The only difference in the model was that expected value was no longer a significant predictor of hard-trial choices in the physical-effort task for clinically depressed MDD participants (b = 0.55, p = .17).
Cognitive-effort-task choices
In Model 2, we tested for an interaction between anhedonia and group on the likelihood of hard cognitive task choices. Increases in probability (b = 0.68, p < .001) and expected values (b = 0.09, p < .001) were significant predictors. Reward (b = 0.05, p = .36), anhedonia severity (b = 0.42, p = .19), group (b = 0.27, p = .48), and the Anhedonia × Group interaction (b = −0.46, p = .16) were not significant predictors. The results did not change when Model 2 adjusted for the effects of calibration performance scores (maximum accuracy scores achieved on the one-back and two-back). In addition, the analyses revealed that calibration performance on the one-back (b = 0.35, p = .60) and two-back (b = 0.25, p = .09) did not have significant main effects on preferences for hard trials during the cognitive-effort task. The results of Model 2 also did not change when run on the MDD subsample that excluded participants with subclinical depressive symptoms.
Models of functioning in depression
We analyzed a hierarchical regression model to evaluate predictors of life functioning in the MDD group. Before conducting this analysis, the correlations between clinical measures and effort-task expected values were examined (see Table S1 in the Supplemental Material available online). The relationships of these individual difference relationships are also visualized in scatterplots in Figures S1 and S2 in the Supplemental Material. Physical-effort-task expected value did not share a significant correlation with life functioning and thus was not included in the model. As shown in Table 2, the linear combination of clinical variables (depressive symptoms, anhedonia, and cognitive functioning) in the first step significantly predicted life functioning. In the second step, cognitive-effort-task expected value accounted for a significant proportion of further variance in life functioning. Participants with MDD had poorer life functioning if they had more severe depressive symptoms and if they made fewer hard high-expected-value-trial choices in the cognitive-effort task. The results did not change after controlling for calibration performance on the easy (one-back) and hard (two-back) cognitive tasks. We also ran the regression model without the participants who displayed subclinical depressive symptoms and found that the results were unchanged with the exception of cognitive-effort-task expected value in the second step emerging as a nonsignificant predictor of functional impairment (β = −0.27, p = .08) but trending in the expected direction, ΔR2 = .07, ΔF(1, 32) = 3.21, p = .08.
Hierarchical Regression Model of Life Functioning in MDD Sample
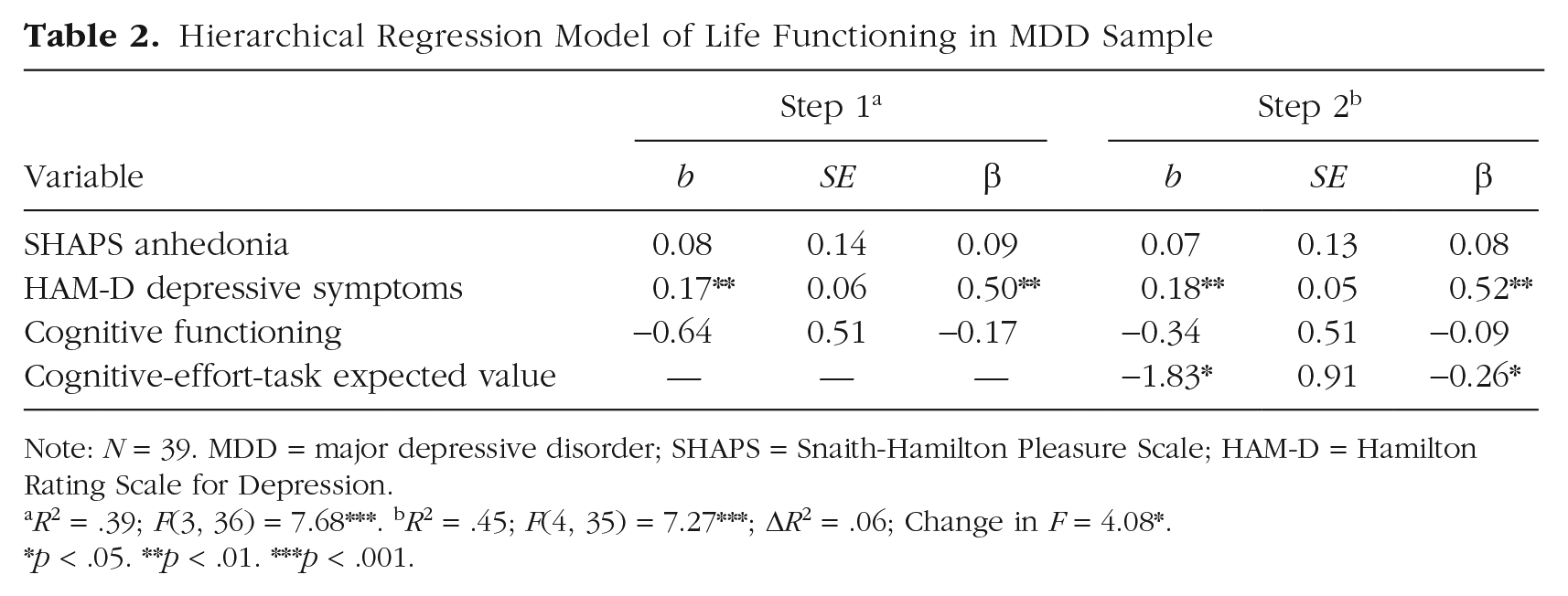
Note: N = 39. MDD = major depressive disorder; SHAPS = Snaith-Hamilton Pleasure Scale; HAM-D = Hamilton Rating Scale for Depression.
R2 = .39; F(3, 36) = 7.68***. bR2 = .45; F(4, 35) = 7.27***; ΔR2 = .06; Change in F = 4.08*.
p < .05. **p < .01. ***p < .001.
We tested a parallel indirect-effects model to examine whether the effect of cognitive functioning on life functioning in participants with MDD, b = −1.30, t(40) = −2.35, p = .02, can be explained by its relationship with two variables: physical-effort-task expected value and cognitive-effort-task expected value. The model with its regression coefficients is presented in Figure 2. Overall, a trend for significance was observed, F(3, 37) = 2.65, p = .06. The model accounted for 18% of the variance in the relationship between cognitive functioning and life functioning. The indirect effect of physical-effort-task expected value on life functioning was not significant, b = 0.05, bias-corrected and accelerated bootstrap (BCa) 95% confidence interval (CI) = [−0.045, 0.302]. There was a significant indirect effect of cognitive-effort-task expected value on functional impairment, b = −0.27, BCa 95% CI = [−1.052, −0.003]. The model was not significant when run with predictors and outcomes switched. Results held when the parallel indirect-effects model controlled for calibration performance scores on the easy and hard cognitive-effort task. When we excluded participants with subclinical depressive symptoms, we did not observe a significant parallel indirect-effects model, R2 = .16, F(3, 33) = 2.05, p = .13. The indirect effect of physical incentivized hard choices on life functioning was nonsignificant, b = 0.05, BCa 95% CI = [−0.050, 0.236]. The indirect effect of cognitive incentivized hard choices on functional impairment was also nonsignificant, although trending in the expected direction, b = −0.17, BCa 95% CI = [−0.864, 0.034].

Multiple mediation model showing the effect of cognitive functioning on life functioning in participants with major depressive disorder, as mediated by motivation to expend physical effort and motivation to expend cognitive effort. Asterisks indicate significant path coefficients (*p < .05).
Discussion
We objectively evaluated motivation to expend physical and cognitive effort in participants with MDD and the mechanisms through which they may be related to impaired life functioning. Motivation to expend physical effort for rewards was indexed by a cost–benefit decision-making experimental task adapted from the original EEfRT (Treadway et al., 2009). Following the framework of the physical-effort task, we also tested a cognitive version that adjusted for task difficulty by manipulating working memory load.
The validity of our adapted physical-effort task was supported. Choices to expend physical effort differed as a function of anhedonia severity in the MDD group. Participants with MDD with higher levels of anhedonia were less likely to choose the hard physical trial. The MDD group also demonstrated blunted sensitivity to information about reward magnitude and probability of a win when making their choices to expend physical effort. These findings are in line with the growing literature base on anhedonia in depression and its correspondence with lower motivation to expend physical effort (Treadway et al., 2009; Yang et al., 2014) and, more specifically, attenuated processes of reward valuation and anticipation (Pizzagalli et al., 2005; Pizzagalli et al., 2008). Anhedonia severity did not share a significant relationship with the likelihood of choices to complete hard cognitive trials on a parallel effort paradigm. Future research will need to clarify if motivation to mobilize physical effort as opposed to cognitive effort plays a larger role in the hedonic response to everyday activities.
The novel cognitive-effort task we developed appeared to be a sensitive measure of motivation to engage in cognitively challenging activities. Our data suggest that the design of the cognitive-effort trials in this study (i.e., abbreviated version of the one-back and two-back) likely challenged participants’ cognition but to an extent that is within the limits of their abilities. Calibration and completion rates of the cognitive-effort task shared minimal to small correlations with working memory ability, which suggested that the adapted cognitive-effort task was a sufficient manipulation of working-memory effort, but the relationship did not have a large enough effect size to suggest that responses on the cognitive-effort task were heavily associated with working-memory performance. In terms of our primary index of motivation on the cognitive-effort task, we observed that MDD and comparison groups did not significantly differ by their frequency of choices to complete the hard high-expected-value trials relative to easy low-expected-value trials. This remained the case even after we controlled for calibration performance, working memory, and executive functioning ability. Furthermore, choices to expend greater cognitive effort across both groups increased as a function of the probability and expected value of reward that was offered. Thus, the adapted cognitive-effort task did not emerge as a tool that discriminated MDD and comparison groups but rather emerged as a general measure of an individual’s motivation to expend cognitive effort. The lack of group difference in cognitive-effort motivation was surprising given that the cognitive-effort hypothesis in depression posits that challenges to appropriately allocate cognitive resources affect this population (Ellis & Ashbrook, 1988; Hasher & Zacks, 1979). A separate line of research focused on the general population found that motivation to exert cognitive effort, although highly variable, tends to favor minimization of effort exertion to conserve a limited set of resources (Kool et al., 2010; Westbrook et al., 2013). Our study offers a comparison of the motivation deficits to expend cognitive effort in both MDD and comparison groups and reveals that the deficits may be more similar between these groups than previously posited.
We investigated the implications of motivation deficits to expend cognitive effort on life functioning in MDD. Lower motivation to expend cognitive effort emerged as a unique predictor of functional impairment in individuals with MDD even after statistically adjusting for established predictors of functioning: depressive symptoms, anhedonia, and cognitive functioning. Furthermore, motivation to expend cognitive effort but not physical effort had a significant indirect effect on the negative relationship between cognitive functioning and functional impairment in daily life. These findings align with previous research by Gupta et al. (2013), in which patients with MDD failed to apply cognitive abilities during real-world functional tasks even when their cognitive functioning was within normal limits. We imagine that low motivation to apply one’s cognitive abilities can reinforce avoidance of cognitively challenging day-to-day tasks (e.g., scheduling activities, staying focused during a social interaction) and can maintain functional impairment in this population. Future research should investigate the contributors to low motivation to expend cognitive effort as a barrier to daily life functioning because it is possible that psychological factors such as aversion to cognitive failure, self-efficacy, and fatigue can inflate motivation deficits.
Taken together, we did not find a significant relationship between motivation to expend physical effort and functional impairment in the MDD group. Instead, physical effort expenditure for rewards was associated with self-reported anhedonia severity. Thus, although motivation to expend cognitive effort was found to be a unique predictor of functional impairment, motivation to expend physical effort may be a more sensitive marker for anhedonia in individuals with MDD rather than a proximal predictor of everyday functioning.
Limitations
There are limitations that are relevant to the interpretation of results. The study findings and interpretations are contingent on the assumption that hard-trial choices are a demonstration of motivated behavior. It is possible that participants chose fewer hard cognitive trials because of fear of failure or because the cognitive-effort demand exceeded their perceived ability level. We argue the latter is unlikely because the highest effort that participants were asked to expend was a portion of the maximum performance demonstrated during calibration trials, and all participants successfully completed practice trials, which suggests that the task demands were within reach of their capacity. The study also did not include measures of internalizing constructs that may relate to motivation to expend effort in depression (e.g., self-efficacy). Finally, data collected in the study are cross-sectional in nature and based on a relatively small sample (although met requirements recommended by a priori power analyses) so caution must be used when making inferences about the generalizability of results. Future research should test the reliability of findings using larger samples and longitudinal designs.
Conclusion
The current findings demonstrate experimental tasks that use a cost–benefit decision-making framework to measure choices to expend cognitive and physical effort for reward and probability are sensitive to the motivational deficits that characterize individuals with MDD. These effort constructs appear to be relatively independent of each other, at least as measured by the paradigms herein. Motivation to expend physical effort is implicated in anhedonia severity, whereas motivation to expend cognitive effort is relevant to life functioning. That is, lower motivation to complete challenging cognitive tasks, as demonstrated by individuals with MDD, appears to exacerbate the process whereby impaired cognitive functioning is associated with impaired life functioning. We see a paradox in individuals with MDD whereby one’s cognitive functioning is valued, but putting cognitive abilities into practice when real-world settings demand them is not always prioritized. Given that daily life is filled with choices to tackle effortful yet adaptive tasks, avoidance of cognitive effort may further reinforce cognitive impairment and functional disability in individuals with depression. Our novel findings highlight the importance of addressing motivation to expend cognitive effort (e.g., reward and probability discounting impairments) in treatments for MDD in order to maximize positive functional outcomes and narrow the gap between abilities and real-world functioning.
Supplemental Material
Tran_Supplemental_Material – Supplemental material for Physical- and Cognitive-Effort-Based Decision-Making in Depression: Relationships to Symptoms and Functioning
Supplemental material, Tran_Supplemental_Material for Physical- and Cognitive-Effort-Based Decision-Making in Depression: Relationships to Symptoms and Functioning by Tanya Tran, Amanda E. F. Hagen, Tom Hollenstein and Christopher R. Bowie in Clinical Psychological Science
Footnotes
Acknowledgements
The data presented in this manuscript were disseminated as a Master’s thesis that was published in an online repository maintained by Queen’s University and as an oral presentation at the 2018 Society for Affective Science meeting.
Transparency
Action Editor: Christopher G. Beevers
Editor: Scott O. Lilienfeld
Author Contributions
T. Tran and C. R. Bowie developed the study concept and design. Testing and data collection were performed by T. Tran and A. E. F. Hagen under the supervision of C. R. Bowie. Data analysis and interpretation were performed by T. Tran with guidance from T. Hollenstein and C. R. Bowie. The manuscript was drafted by T. Tran, and A. E. F. Hagen, T. Hollenstein, and C. R. Bowie provided critical revisions. All of the authors approved the final version of the manuscript for submission.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.