
Abstract
In this study, we examined processes of change in trauma-focused cognitive behavioral therapy (TF-CBT) delivered to a community sample of 81 youths. Emotional processing theory (EPT) is used as an organizational framework. EPT highlights activating and changing pathological trauma-related responses and increasing adaptive responses across cognitive, emotional, behavioral, and physiological domains. We coded sessions during the trauma-narration and -processing phase of TF-CBT to examine the extent to which pathological and adaptive trauma-related responses were activated across domains. Higher scores indicate that more domains (range = 0–4) were activated at a threshold of moderate to high intensity. Curvilinear change (inverted U, increase then decrease) in multimodal negative response scores across sessions predicted improvement in internalizing symptoms and symptoms of posttraumatic stress disorder after treatment. Linear increases in multimodal positive responses predicted improvement in externalizing symptoms. Findings suggest value in activating and changing both pathological and adaptive trauma responses across multiple domains and examining nonlinear patterns of change.
Keywords
Childhood trauma is associated with numerous consequences that can persist throughout development, including poor academic performance, substance use, violent behavior, depression, and suicide (Paolucci, Genuis, & Violato, 2001; Roth, Newman, Pelcovitz, van der Kolk, & Mandel, 1997; Tyler, 2002). Trauma-focused cognitive behavioral therapy (TF-CBT; Cohen, Mannarino, & Deblinger, 2006, 2017) is an evidence-based treatment for youths who have experienced a wide range of childhood traumas, and there is strong empirical support for its effectiveness in reducing posttraumatic stress disorder (PTSD) and other trauma-related symptoms (Gutermann et al., 2016; Lenz & Hollenbaugh, 2015). However, as is the case with many evidence-based treatments for children and adolescents (Weisz & Kazdin, 2010), little is known about processes of therapeutic change in TF-CBT. A better understanding of which in-session variables predict treatment outcomes could help clinicians to focus on those key targets to improve treatment efficacy.
Emotional Processing Theory as a Framework for Studying Processes of Change in TF-CBT
A number of trauma treatments for children and adults focus on the processing of traumatic experiences. These treatments include TF-CBT (Cohen et al., 2006, 2017, 2018), prolonged exposure (Foa, Hembree, & Rothbaum, 2007), cognitive processing therapy (Resick, Monson, & Chard, 2017; Resick & Schnicke, 1992), cognitive therapy (e.g., Perrin et al., 2017), emotion-focused therapy (e.g., Paivio, Hall, Holowaty, Jellis, & Tran, 2001; Paivio & Nieuwenhuis, 2001), written exposure therapy (Sloan & Marx, 2019), and narrative exposure therapy (Schauer, Neuner, & Elbert, 2011). Emotional processing theory (EPT; Foa, Huppert, & Cahill, 2006; Foa & Kozak, 1986) can therefore be a useful common framework to study how therapeutic change occurs in TF-CBT and other trauma treatments for youths and adults.
EPT posits that psychopathology related to anxiety and traumatic stress is represented by a pathological network of stimuli, response elements (cognitive, emotional, behavioral, physiological), and their meaning. Emotional processing occurs when the pathological network is activated and incompatible information is introduced to promote corrective learning of more adaptive associations and responses. Although EPT has been studied most often in the context of exposure-based treatments, emotional processing was originally proposed as a transdiagnostic mechanism of change across different types of treatments (Foa & Kozak, 1986) for adults and youths (Peterman, Carper, & Kendall, 2019). Fear activation and habituation were initially emphasized as indicators of emotional processing, but updates to EPT (Foa et al., 2006) highlight the importance of changing responses to fear stimuli across multiple domains of functioning, including cognitive, emotional, behavioral, and physiological domains. The updated theory (Foa et al., 2006; Foa & McNally, 1996) also incorporates findings on inhibitory learning (e.g., Bouton, 2000; for a review, see Craske et al., 2008), which suggest that new responses learned in treatment do not replace the pathological learning but rather can inhibit or buffer the old responses. This suggests that it is also important to measure new, more adaptive responses across multiple domains.
TF-CBT is based in part on EPT (Cohen et al., 2018), especially the trauma narration and processing (second) phase of treatment. Clinicians help youths develop a trauma narrative, which activates the network of cognitive, emotional, behavioral, and physiological responses to trauma memories. Clinicians then guide youths to process their traumatic experiences and also provide corrective information to help the youths learn more adaptive responses (Cohen et al., 2018). EPT is therefore relevant to the study of change in TF-CBT and can help to link findings from this study to the broader research on change in other child and adult treatments for PTSD.
Emotional Processing and Multimodal Change
According to EPT and related treatments, processing of traumatic memories is most potent if multiple types of trauma responses are targeted (Cohen et al., 2006, 2017; Foa et al., 2006, 2007; Foa & McLean, 2016). This multimodal focus includes trauma-related cognitions, emotions, behaviors, and physiological responses. However, most studies on the process of change in PTSD treatments have examined only one domain of functioning rather than multimodal activation and change.
For instance, decreases in negative cognitions predict symptom reduction in TF-CBT (Pfeiffer, Sachser, de Haan, Tutus, & Goldbeck, 2017) and other trauma-focused therapies for children and adolescents (e.g., König et al., 2019; McLean, Yeh, Rosenfield, & Foa, 2015; Smith et al., 2007) and for adults (e.g., McLean et al., 2019; McLean, Su, & Foa, 2015; Scher, Suvak, & Resick, 2017; Zalta et al., 2014). Reductions in self-reported fear reactivity across sessions predict better treatment outcomes (Asnaani, McLean, & Foa, 2016; Cooper, Clifton, & Feeny, 2017), and other negative emotions such as anger, shame, guilt, and disgust also play an important role in PTSD (McLean & Foa, 2017) and its treatment (Foa, Riggs, Massie, & Yarczower, 1995; Kaczkurkin, Asnaani, Zhong, & Foa, 2016; Rizvi, Vogt, & Resick, 2009). In the behavioral domain, avoidance (e.g., avoidance of trauma cues, homework noncompliance) predicts worse posttreatment outcomes (Cooper, Kline, et al., 2017; Gloth, 2017). In addition, there is evidence that changes in a number of physiological indicators of distress predict better treatment outcomes in exposure therapy for PTSD, such as reductions in physiological fear response (e.g., heart rate) across sessions (Asnaani et al., 2016; Cooper, Clifton, & Feeny, 2017), posttreatment decreases in trauma-potentiated startle (Maples-Keller et al., 2019), and an increase then decrease in trauma-potentiated startle (Robison-Andrew et al., 2014). Cisler and colleagues (2015) also found that adolescent girls who improved more in TF-CBT showed greater differential amygdala reactivity to fear faces than to neutral faces (i.e., better threat vs. safety discrimination) before treatment than nonresponders did. Although these studies were focused on one specific domain of functioning, taken together, they illustrate the importance of a more multimodal focus on negative trauma responses across multiple domains.
In addition to pathological responses to trauma content, some researchers have examined more adaptive responses learned in treatment. Again, one domain in isolation rather than a multimodal set of responses was typically examined in these studies. For example, accommodation (a cognitive construct that captures healthy, balanced beliefs about oneself, others, and the future) has been shown to predict better outcomes in TF-CBT (Ready et al., 2015) and in cognitive processing therapy for youths (König et al., 2019) and for adults (Dondanville et al., 2016; Iverson, King, Cunningham, & Resick, 2015). There is some evidence that positive emotions reduce the reacquisition of fear, which could have implications for trauma treatments (Dour, Brown, & Craske, 2016; Zbozinek & Craske, 2017). Increases in approach behaviors toward previously avoided trauma-related situations and reminders are also associated with PTSD symptom improvement (Porter, Romero, & Barone, 2018). Mindfulness-based interventions, which are associated with positive physiological responses (e.g., lower heart rate, increased parasympathetic activity; Ditto, Eclache, & Goldman, 2006; Mazzei, 2017), have been associated with reduction in PTSD symptoms (Colgan, Christopher, Michael, & Wahbeh, 2016; Held, Owens, Monroe, & Chard, 2017). Together, these findings suggest value in measuring the development of more adaptive responses across domains of functioning in addition to the reduction of pathological responses.
PTSD is a complex system of pathology (Sripada, Rauch, & Liberzon, 2016), and studies on processes of change in PTSD treatments should accordingly capture the breadth of pathological and adaptive trauma responses that a client can experience. We used an observational coding system of therapeutic change processes, the CHANGE observational coding system (Hayes, Feldman, & Goldfried, 2007), to code therapy sessions from TF-CBT. The CHANGE uses verbal and nonverbal information and can assess trauma reactions expressed by clients across the cognitive, emotional, behavioral, and physiological domains of interest in this study. The measure also assesses both pathological and adaptive responses.
Emotional Processing and Nonlinear Change
Another implication of EPT is that research on processes of change in treatment might be advanced by examining not only linear but also nonlinear patterns of change. According to EPT, emotional processing involves the multimodal activation of the pathological network of trauma-related responses followed by the weakening of these responses across domains (Foa et al., 2006; Foa & Kozak, 1986). Thus, this pattern of change might be captured by a quadratic (concave down, inverted U) pattern of change, beyond a linear trajectory of change. Indeed, change in psychotherapy does not always follow a linear trajectory (Hayes, Laurenceau, Feldman, Strauss, & Cardaciotto, 2007). For instance, data suggest that symptom trajectories in some PTSD treatments are better represented by quadratic functions than by linear functions (Nishith, Resick, & Griffin, 2002; Schumm, Walter, & Chard, 2013). Robison-Andrew and colleagues (2014) also found that quadratic change in startle response measured before, during, and after treatment predicted better treatment response in prolonged exposure and present-centered therapy for PTSD. Quadratic change in negative trauma responses across domains may similarly predict treatment outcome in TF-CBT, although this has not yet been examined.
The Current Study
Using EPT as an organizational framework (Foa et al., 2006), we examined change in both pathological and adaptive responses to trauma-related content during the trauma narration and processing phase of TF-CBT for trauma-exposed youths (Cohen et al., 2006, 2017). This phase of treatment was selected because it focuses specifically on the activation and processing of traumatic memories and their impacts. The CHANGE coding system (Hayes, Feldman, & Goldfried, 2007) was used to assess the extent to which pathological and adaptive responses to trauma-related content were multimodal (i.e., activated at a moderate to high level across cognitive, emotional, behavioral, and physiological domains). Higher multimodal response scores indicated that more domains (range = 0–4) were activated at threshold. Trauma responses were coded for each session during this treatment phase to allow for an evaluation of linear and curvilinear trajectories as predictors of internalizing, externalizing, and PTSD symptoms after treatment.
In line with EPT (Foa et al., 2006; Foa & Kozak, 1986) and reviews of its evidence (Asnaani et al., 2016; Foa et al., 2006), we expected that in addition to a linear decrease in multimodal negative trauma-related responses, a curvilinear pattern would also predict more improvement in posttreatment measures of psychopathology (internalizing, externalizing, and PTSD symptoms). In other words, multimodal negative response scores that increased and then decreased (weakened) over the processing phase of TF-CBT were expected to predict better outcomes. Given the emphasis in EPT on strengthening new, adaptive associations (Foa et al., 2006) and the importance of multimodal positive responses in new learning (e.g., Dour et al., 2016; Porter et al., 2018), we expected greater linear increases in multimodal positive responses to predict better posttreatment outcomes. There is no theoretical reason to expect that positive responses would change in a curvilinear way, so only linear change was examined.
Method
Participants
Participants were recruited as part of a larger effectiveness trial of TF-CBT for trauma-exposed youths (for trial outcomes, informed consent procedures, and information on participant recruitment and retention, see Webb, Hayes, Grasso, Laurenceau, & Deblinger, 2014; NCT01649141). The procedures for this trial were approved by the institutional review boards of all participating agencies. Youths were eligible for the trial if they had a score of 17 or more on the UCLA PTSD Reaction Index for DSM-IV-Abbreviated (UPID-A; Steinberg, Brymer, Decker, & Pynoos, 2004) or endorsed three of nine PTSD symptoms based on an independently verified trauma (e.g., through child welfare). Eligible youths also spoke English, qualified for publicly funded treatment, and had a nonoffending caregiver willing to participate in treatment. Youths were excluded if they had an intellectual disability, untreated psychosis, or current substance abuse; required frequent hospitalizations or a higher level of care; or had a sibling already in the study.
Of the 109 participants who met inclusion criteria for the effectiveness trial, 81 began the trauma-narration and -processing (second) phase of treatment and were included in the present sample. These youths did not differ demographically from the 28 participants who discontinued treatment before this phase of treatment. The current sample included 54 (66.7%) girls and 27 (33.3%) boys, ages 7 to 17 years old (M = 12.6 years, SD = 2.8). The sample was 51.9% White, 40.7% Black or African American, 3.7% Hispanic or Latino, and 3.7% biracial. Youths had experienced on average 3.5 types of trauma (SD = 1.7). Thirty-seven percent were in foster care when they enrolled. Youths completed an average of 5.28 sessions of the approximately six sessions in the trauma-processing phase of TF-CBT (SD = 2.17). Using hierarchical piecewise regression analyses with this same sample, Ready and colleagues (2015) reported that there were significant reductions in internalizing (γ = −.98, SE = .15, p < .001), externalizing (γ = −.76, SE = .21, p < .001), and PTSD symptoms (γ = −2.55, SE = .29, p < .001) after treatment.
Procedure
TF-CBT (Cohen et al., 2006, 2017) is an evidence-based treatment for children and adolescents who have experienced a range of childhood traumas; the treatment also involves the youths’ nonoffending caregivers. TF-CBT incorporates psychoeducation, skills building, gradual exposure to traumatic memories, and processing of trauma-related content. Youths and caregivers meet with a therapist in separate 30- to 45-min sessions for approximately 12 to 15 sessions and also in several conjoint sessions, if appropriate.
TF-CBT is divided into three phases. Phase 1, stabilization and skills building, emphasizes psychoeducation and coping skills, such as relaxation and emotion regulation skills. In Phase 2, trauma narration and processing, youths are exposed to the trauma memory and trauma-related content by developing a detailed narrative of their experiences. As youths create and discuss their narratives, therapists help them to emotionally process their experiences and challenge maladaptive beliefs about the trauma, its meaning, and its consequences. The third phase, integration and consolidation, includes in vivo mastery activities when needed, trauma-focused conjoint sessions in which youths share the narrative with caregivers if clinically appropriate, and the development of personal safety skills. In the present study, we focused on sessions from the second phase of treatment, when trauma processing is the focus of sessions.
Therapy was delivered by a team of 25 clinicians who either held a professional degree or were doctoral students in clinical psychology programs. Unlicensed clinicians were supervised by a licensed practitioner. Adherence ratings suggested that therapists delivered TF-CBT with good fidelity (for further details, see Ready et al., 2015).
Measures
Session coding
The CHANGE coding system (Hayes, Feldman, & Goldfried, 2007) was used to code each treatment session in the trauma-narration and -processing phase of TF-CBT for each participant. Sessions were coded for the extent of multimodal activation of pathological and adaptive trauma-related responses across cognitive, emotional, behavioral, and physiological domains of functioning. The CHANGE is designed to capture a range of variables thought to be central to therapeutic change. This coding system has been used to code written narratives in cognitive behavioral treatments for depression (Hayes, Beevers, Feldman, Laurenceau, & Perlman, 2005; Hayes, Feldman, & Goldfried, 2007) and adult PTSD (Alpert, Hayes, Barnes, & Sloan, 2020) as well as audiotaped sessions of prolonged exposure for adult PTSD (Jun, Keller, Zoellner, Feeny, & Hayes, 2016), cognitive therapy for personality disorders (Hayes & Yasinski, 2015), and cognitive therapy for treatment-resistant depression (Abel, Hayes, Henley, & Kuyken, 2016).
In the current study, a team of 19 graduate and undergraduate students coded audio recordings of sessions (M = 5.28 sessions per participant, SD = 2.17). Coders were trained in the CHANGE coding system and practiced coding with experienced coders until they reached sufficient agreement on target variables (intraclass correlations, or ICCs, ≥ .80). Two coders rated each session, and each coder was paired with multiple other coders. Weekly consensus meetings were held to prevent rater drift and to reach group consensus on discrepancies of 2 or more points on the 4-point scale of the CHANGE. Discrepancies were replaced with consensus ratings, and the ratings of the two coders were then averaged.
Each session was coded for trauma-related responses that occurred in that session or over the past week. To be coded, content had to relate to the trauma or its impact. Negative and positive responses, coded separately, included responses in four domains: cognitions about the self, others, or the future (e.g., “I can’t trust anyone” or “I will be able to heal”); emotions (e.g., sad or pleased); behaviors (e.g., getting in a fight or using coping skills when angry); and physiological experiences (e.g., difficulty breathing or feeling relaxed). For the cognitive variable, scores were calculated by taking the highest of three codes representing beliefs about the self, others, and the future. CHANGE variables are coded for intensity on a 4-point scale from 0 (absent or very low) to 3 (high).
Detailed descriptions of each coding category and examples of session content that would be coded as high are presented in Table 1. For each variable, a final ICC was calculated by computing the ICC for each coder pair and then averaging across coders, as recommended by Hallgren (2012). ICCs ranged from .66 to .91, which is in the good to excellent range of agreement (Cicchetti, 1994; see Table 1).
CHANGE Coding Categories With Descriptions, Examples of High Levels of Each Variable, and ICCs of Interrater Agreement
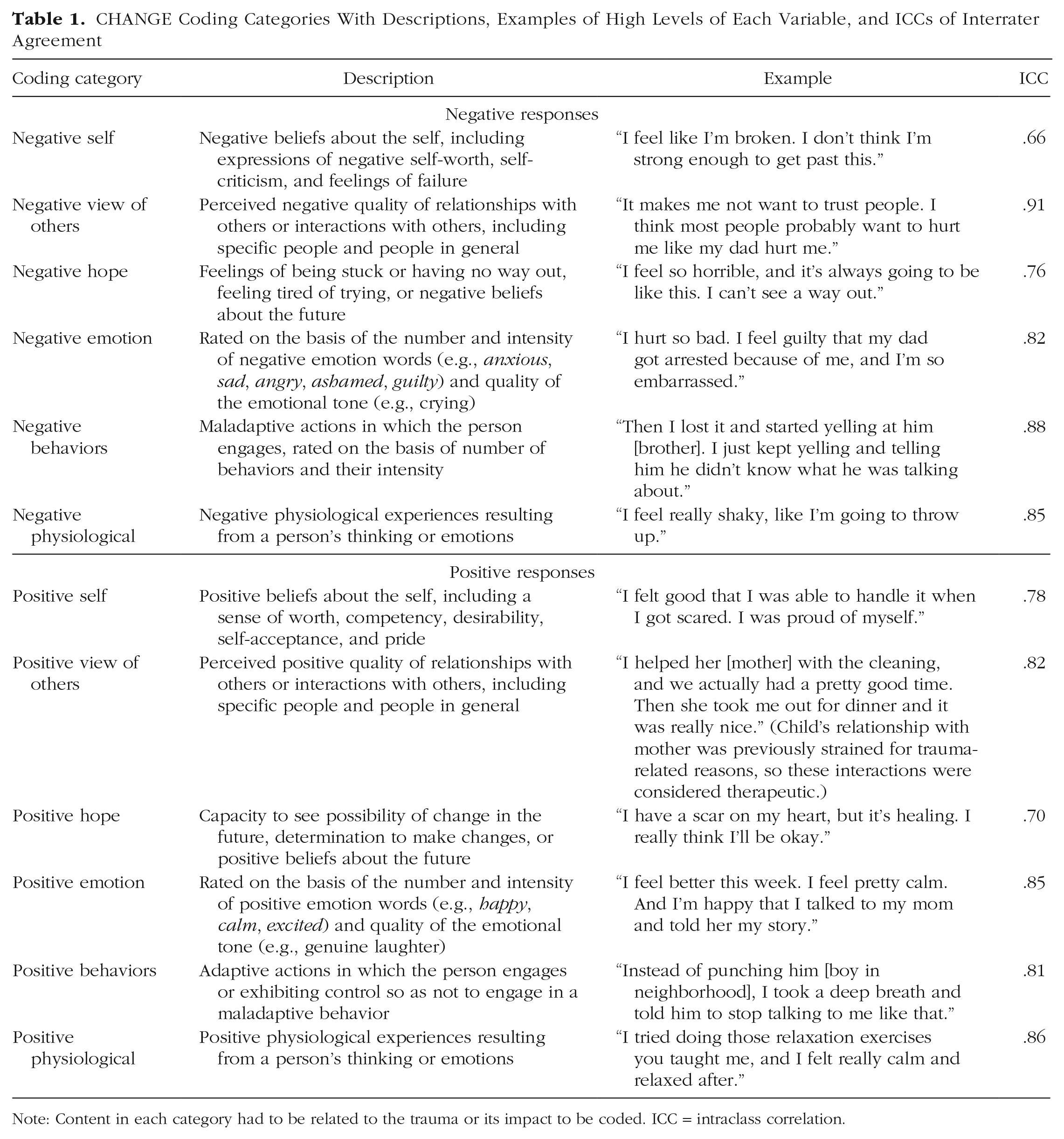
Note: Content in each category had to be related to the trauma or its impact to be coded. ICC = intraclass correlation.
Multimodal response scores
Because many trauma treatments emphasize the importance of activating and changing responses across multiple domains (e.g., Cohen et al., 2006, 2017; Foa et al., 2007), we created a composite score to quantify the extent to which negative and positive responses were activated across four domains: cognitive, emotional, behavioral, and physiological. The intensity scores (0–3) for each CHANGE variable in a given session were used to calculate the number of the four domains that were activated at a threshold of moderate to high intensity (score ≥ 2 on the 0–3 CHANGE scale). Multimodal response scores can range from zero to four domains activated at threshold; these scores take into account both the intensity and breadth of trauma-related responses.
For example, a child describing abuse by his uncle might express the belief “I can never trust anyone ever again” (negative cognitions intensity = 3), report feeling very anxious all the time (negative emotions = 3) and a bit shaky one time (negative physiological = 1), and refuse to engage in any discussion of his trauma narrative (negative behavior = 3). In this example, negative trauma-related responses were activated at threshold in three of the four domains (cognitive, emotional, and behavioral), so the multimodal negative response score is 3. Another adolescent discussing her father’s murder may express the beliefs “I know I’ll be able to move forward from this” and “I feel strong” (positive cognitions intensity = 3), report she is feeling pleased and proud of herself for how she was able to cope with the loss of her father (positive emotions = 2), and report that she tried to have a constructive conversation with a peer about her father’s death (positive behavior = 1). Positive physiological responses were not noted (positive physiological = 0). Positive trauma-related responses in this example were activated at threshold in two domains (cognitive and emotional), so the multimodal positive response score is 2.
Measures of treatment outcomes
Internalizing and externalizing symptoms
At pretreatment and at 6 months after randomization (approximately posttreatment), caregivers completed the Child Behavior Checklist (CBCL; Achenbach & Rescorla, 2001). The CBCL is a well-established measure of mental health problems in children that has good reliability and validity (Achenbach & Rescorla, 2001). Caregivers rate 113 items assessing a range of child emotional and behavioral problems, each rated on a 3-point Likert scale from 0 (not true) to 2 (very true or often true).
The internalizing and externalizing scales of the CBCL were the primary outcome measures used in this study, consistent with previous publications from this trial (Hayes et al., 2017; Ready et al., 2015; Yasinski et al., 2016). The internalizing scale of the CBCL measures anxiety, depression, withdrawal, and somatic complaints. The externalizing scale measures acting out, rule breaking, and aggressive behaviors. Measures of broad symptoms have been recommended over more disorder-specific measures to capture therapeutic change in treatment for youths (Becker, Chorpita, & Daleiden, 2011). Furthermore, PTSD includes many internalizing symptoms (e.g., persistent negative emotions, reduced interest, sleep disturbance), but it is also associated with higher levels of externalizing symptoms in youths (Barboza, Dominguez, & Pinder, 2017; Saigh, Yasik, Oberfield, Halamandaris, & McHugh, 2002). Data in adult populations also suggest that more transdiagnostic internalizing and externalizing symptom measures might better capture the range of trauma-related pathology than PTSD-specific measures (Wolf, Miller, Harrington, & Reardon, 2012). Thus, we examined the internalizing and externalizing scales of the CBCL as treatment outcomes. We used raw scores because T-scores can truncate the range of data and be less sensitive to gradual symptom changes during treatment (Achenbach, 1991). In the current sample, reliability across time points was excellent for both the internalizing (Cronbach’s αs = .89–.90) and externalizing scales (αs = .92–.95).
PTSD symptoms
A measure of PTSD symptoms, the self-report version of the UCLA PTSD Reaction Index for DSM-IV (UPID; Steinberg et al., 2004), was completed by youths at baseline and 6 months after randomization. The UPID can be administered as a questionnaire or structured interview to youths ages 7 to 18 years, and it assesses various trauma types and the severity of PTSD symptoms described in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–IV; American Psychiatric Association, 1994). The UPID shows good test-retest reliability, convergent validity, sensitivity, and specificity in diagnosing PTSD (Steinberg et al., 2004). In the present sample, the UPID had good reliability (Cronbach’s αs = .87–.90).
Data analytic approach
Data were analyzed in Mplus (Muthén & Muthén, 2012). Multilevel modeling was used to account for the hierarchical structure of the data (i.e., sessions nested within participants). Within-persons slopes of scores for multimodal negative and positive trauma-related responses were entered as predictors of posttreatment outcomes (internalizing, externalizing, and PTSD symptoms). Random slopes were estimated to allow for slopes to vary from person to person, and random slopes can be treated as predictors of between-persons outcomes. Two sets of models were repeated across internalizing, externalizing, and PTSD outcomes for a total of six models. Child age and gender were uncorrelated with all predictor and outcome measures, so they were not included in the final analyses.
In the first three models, within-persons slopes of multimodal negative and positive response scores were estimated to represent each individual’s linear change in these variables over time. At the within-persons level of each model, random slopes of multimodal negative and positive responses were estimated using each individual’s repeated measures by regressing each of these variables on session number, with the first session coded as 0. At the between-persons level, posttreatment internalizing (Model 1), externalizing (Model 2), or PTSD (Model 3) was regressed on the within-persons slopes of both negative and positive responses, controlling for the baseline levels of the outcome variable (e.g., the model predicting posttreatment internalizing included baseline internalizing as a covariate). We controlled for baseline symptoms to account for initial severity and capture changes in symptoms.
In the final three models, the within-persons quadratic slope of multimodal negative responses was entered as a predictor of posttreatment internalizing (Model 4), externalizing (Model 5), and PTSD symptoms (Model 6). To reduce collinearity between linear and quadratic time terms, session number was grand-mean centered in these analyses. At the within-persons level, random slopes were estimated using each individual’s repeated measures by regressing negative responses on linear (i.e., centered session number) and quadratic (centered session number squared) session terms. Change in positive responses was not included as a covariate because models including this variable failed to converge. At the between-persons level of each model, the treatment outcome (internalizing, externalizing, or PTSD) was regressed on the within-persons quadratic slope of change in multimodal negative responses, controlling for the baseline level of the outcome variable.
Results
Descriptive analyses and intercorrelations
Descriptive analyses for within-persons (session-by-session) variables of interest and their intercorrelations revealed that multimodal negative trauma-related responses (M = 1.34, SD = 1.01, range = 0–4) and multimodal positive responses (M = .88, SD = .91, range = 0–3) were not significantly correlated (r = .10, n.s.). On average across sessions in the trauma-processing phase of TF-CBT, participants had higher multimodal negative responses than positive responses, t(412) = 7.42, p < .001. Descriptive statistics for between-persons variables (internalizing, externalizing, and PTSD) at baseline and posttreatment and their intercorrelations are presented in Table 2. Internalizing and externalizing symptom severity measures were positively correlated at all time points. Baseline PTSD severity was correlated significantly with baseline internalizing only.
Descriptive Statistics and Intercorrelations Among Between-Persons Outcome Measures, Including Internalizing and Externalizing Scales of the Child Behavior Checklist and PTSD Severity (UCLA PTSD Reaction Index for DSM-IV)
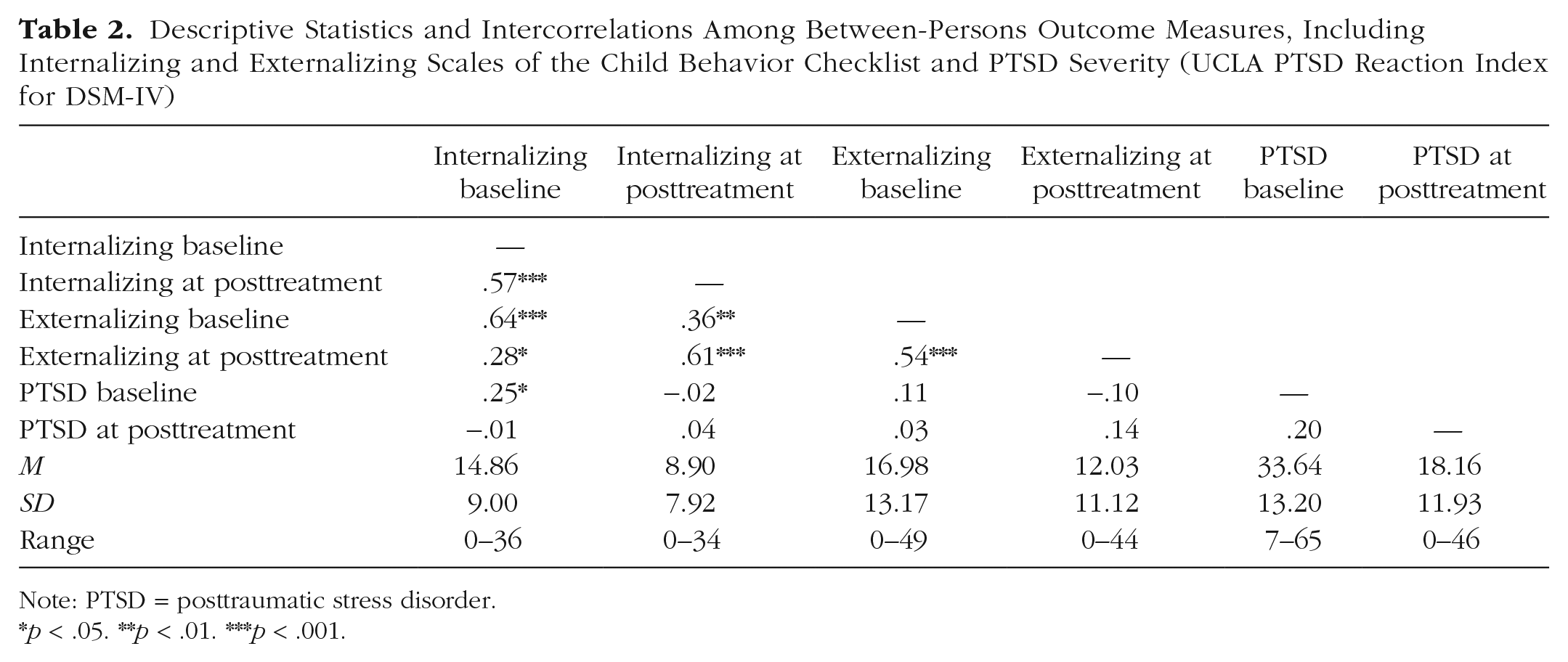
Note: PTSD = posttraumatic stress disorder.
p < .05. **p < .01. ***p < .001.
We also examined the fixed and random effects of within-persons slopes over time for the multimodal negative and positive response variables that were the predictor variables in the main analyses. None of the slopes of interest were significant on average across the sample (fixed effects = .02 for negative responses linear slope, −.02 for negative responses quadratic slope, .04 for positive responses linear slope, all n.s.). The linear slope of negative responses over time varied significantly across participants (random effect = .01, p < .05), but the other slopes of interest did not (random effects = .002 for negative responses quadratic, .01 for positive responses linear, both n.s.). Based on estimates of the averages and variances of these slopes, 95% of the sample ranged from negative to positive values for all slopes of interest (95% sample ranges = −.19 to .24 for negative responses linear, −.11 to .06 for negative responses quadratic, −.13 to .20 for positive responses linear).
Predictors of treatment outcomes
The first three models regressed internalizing, externalizing, and PTSD outcomes, respectively, on within-persons linear slopes of multimodal negative and positive responses, controlling for baseline symptoms. Results of these models (see Table 3) suggest that linear change in negative trauma-related responses over the trauma-narration and -processing phase of TF-CBT did not predict any of the three posttreatment outcomes of interest. However, as predicted, more linear improvement in positive responses predicted lower posttreatment externalizing (but not internalizing or PTSD) symptoms. The final three models regressed internalizing, externalizing, and PTSD outcomes, respectively, on the within-persons quadratic slope of multimodal negative responses. Results (Table 3) indicate that although the linear slope of negative responses did not predict posttreatment outcomes, the quadratic shape of change did predict posttreatment internalizing and PTSD outcomes, as predicted, but not externalizing symptoms. The effect was such that a more concave down curve (inverted U) predicted lower posttreatment internalizing and PTSD symptoms.
Regression Results for Within-Persons Slopes of Multimodal Negative and Positive Responses to Trauma-Related Content Predicting Posttreatment Outcomes (Internalizing, Externalizing, and PTSD Symptoms), Controlling for Baseline Symptoms

Note: CI = confidence interval; PTSD = posttraumatic stress disorder; CBCL = Child Behavior Checklist; UPID = UCLA PTSD Reaction Index for DSM-IV. Multimodal negative responses is a composite variable representing the number of domains of pathological trauma responses (cognitive, emotional, behavioral, physiological) activated at a moderate to high level (≥ 2 on the 0–3 CHANGE scale) in response to trauma-related content during the trauma-processing phase of trauma-focused cognitive behavioral therapy (TF-CBT). Multimodal positive responses is a composite variable representing the number of domains of adaptive trauma responses activated at the same threshold.
p < .01.
Discussion
The current study extends prior research on processes of change in TF-CBT and other PTSD treatments by moving from a focus on isolated variables (e.g., negative cognitions, fear response) to an examination of multimodal pathological and adaptive trauma responses as predictors of treatment outcome. Using Foa and colleagues’ (2006) updated EPT as an organizational framework, we examined linear and nonlinear changes in the extent to which pathological and adaptive responses to trauma-related content were activated across cognitive, emotional, behavioral, and physiological domains. We examined the following predictors of outcome: (a) linear decreases in multimodal pathological responses, (b) curvilinear change (concave down, inverted U) in multimodal pathological responses, and (c) linear increases in multimodal adaptive responses. Linear change in multimodal negative responses did not predict treatment outcomes, but as hypothesized, a curvilinear pattern of negative responses did predict lower posttreatment internalizing and PTSD symptoms, although not externalizing symptoms. Also as predicted, linear increases in multimodal positive responses predicted less externalizing behavior at posttreatment, but unexpectedly did not predict improvement in internalizing or PTSD symptoms.
Most studies examining processes of change in TF-CBT and other PTSD treatments have focused on linear changes in single domains of responses to trauma content, and few predictors of TF-CBT outcome have been identified. Consistent with the most recent iteration of EPT (Foa et al., 2006), our findings suggest that linear and nonlinear changes in multimodal pathological and adaptive responses are important in TF-CBT. Although some studies have described a curvilinear pattern of symptom change across treatment (Nishith et al., 2002; Schumm et al., 2013), they did not examine this pattern as a predictor of treatment outcomes. Our study is the second to our knowledge to examine curvilinear change in trauma responses across treatment sessions as a predictor of symptom outcomes. Robison-Andrew and colleagues (2014) found that a quadratic pattern of change in startle response measured before, during, and after treatment predicted better treatment response in prolonged exposure and present-centered therapy for PTSD. Likewise, we found that curvilinear change in multimodal pathological responses (cognitive, emotional, behavioral, and physiological) predicted improvement in both internalizing symptoms and PTSD symptoms. This concave down pattern might represent the activation of multiple domains of responses in the initial trauma-processing sessions of TF-CBT followed by weakening of these responses (fewer domains activated at a moderate to high level) over subsequent sessions. This finding suggests that the trauma-processing phase of TF-CBT can involve a transient period of distress as the traumatic experiences are recalled and processed, but an increase and decrease in distress is associated with symptom improvement. Although our findings need to be replicated, they suggest the promise of multimodal measures of pathological and adaptive learning and of nonlinear analyses of change (Foa et al., 2006; Hayes, Laurenceau, et al., 2007).
A notable pattern of findings was that change in both negative and positive multimodal responses to trauma content predicted better posttreatment outcomes on one or two symptom measures but not all three. Negative and positive responses were not significantly correlated in the present sample, which suggests that positive responses represent more than the inverse of negative responses and that both can provide important information. This pattern of findings suggests that changes in pathological responses, which predicted improvement in internalizing and PTSD symptoms, may operate on different sets of symptoms than the development of more adaptive responses, which predicted improvement in externalizing symptoms. There is little research on predictors of externalizing symptoms related to trauma or on the role of developing more adaptive responses. Deblinger, Mannarino, Cohen, Runyon, and Steer (2011) found that more time teaching caregivers parenting skills in TF-CBT was associated with more improvement in child externalizing symptoms. It is possible that increases in more positive responses might have helped youths to better regulate themselves and respond to trauma-related situations with less anger, aggression, and impulsivity. Anger in particular predicts worse outcomes and higher dropout in trauma-focused treatment in adults (Foa et al., 1995; Rizvi et al., 2009), and it might also be an important target in treatments for traumatized youths.
Strengths, limitations, and future directions
One strength of the present study is the repeated, session-by-session measurement of responses to trauma-related content over the phase of TF-CBT that targets trauma exposure and processing. The longitudinal study design allowed for the estimation of within-persons slopes of change in pathological and adaptive trauma-related responses, which could then be examined as predictors of subsequent posttreatment outcomes. Because internalizing, externalizing, and PTSD symptoms were measured only at pretreatment and posttreatment rather than at each session, we cannot rule out the possibility that symptom change in the first phase of treatment influenced change in responses to trauma content in the second phase of treatment. In addition, therapists might have responded differently to clients on the basis of previous symptom change (Stiles, 2009). The current study provides preliminary evidence that changes in multimodal trauma responses predict posttreatment outcomes, but future studies should include session-by-session measurements of symptoms to better establish the temporal precedence of changes in negative and positive trauma responses (Kazdin, 2007). Future studies might also measure therapist interventions during sessions to reveal potential predictors of therapeutic change.
Another strength of the present study is that the CHANGE coding system (Hayes, Feldman, & Goldfried, 2007) allowed for the measurement of multiple types of responses to trauma content in one study and as rated by independent raters. The CHANGE can be useful as a single measure that captures multiple domains of pathological and adaptive trauma responses expressed during treatment sessions, in line with EPT’s emphasis on multimodal activation and change (Foa et al., 2006). This measure also reduces the possible confound of method variance. However, the CHANGE is reliant on observable verbal and nonverbal content. Future studies could include different types of measures for each of the domains assessed (cognitive, emotional, behavioral, and physiological), including self-reports, lab tasks, behavioral assessments, and psychophysiological measures.
Although the constructs that we examined involved multimodal sets of responses, we calculated composite scores rather than conducting network analyses. This was because the density of within-persons data and the number of participants were not sufficient for network analyses (Epskamp, Borsboom, & Fried, 2018). With assessments that are daily or more frequent (rather than weekly), network analyses could be used to examine the interconnectivity among the types of responses and to identify those that are most central in predicting outcome (Borsboom, 2017; Epskamp et al., 2018). The present approach still has clinical utility given that findings suggest that clinicians might attend to changes in the breadth of their clients’ responses to trauma-related content rather than focusing on one type of response or another (e.g., cognitive or emotional). Protocols for exposure therapies for PTSD, including TF-CBT, emphasize multimodal activation during exposure sessions, including sensory details, thoughts, and feelings (Cohen et al., 2006, 2017; Foa et al., 2007; Resick et al., 2017; Resick & Schnicke, 1992), but less attention is paid to change in breadth of negative responses over the course of treatment or to the development of multimodal adaptive responses.
Another notable strength of this study is the use of EPT to guide the investigation of processes of change in TF-CBT and the examination of change processes in a racially and ethnically diverse community sample of trauma-exposed youths. EPT has typically been studied in adult populations, and our findings contribute to research showing that EPT is also relevant in treatments for youths (e.g., Cohen et al., 2006, 2017; Foa, McLean, Capaldi, & Rosenfield, 2013; Franklin et al., 2011; Peterman et al., 2019) and in treatments delivered in community settings (e.g., Foa et al., 2005; Webb et al., 2014).
It should also be noted that the present sample only included youths who began the trauma-narration and -processing (second) phase of TF-CBT. Although there were no differences on demographic measures between these youths and the youths who discontinued therapy before that point, there could be other differences between these groups. In addition, we focused on the trauma-processing phase of TF-CBT, in which the focus is on the activation and processing of traumatic memories and related content. Important processes of change are also likely to occur in the other phases of TF-CBT, and these should be examined in future studies.
Another consideration is that some of the regression coefficients that were not significant predictors of outcome had large standard errors and confidence intervals. These included the linear slope of negative responses predicting posttreatment externalizing symptoms, linear slopes of negative and positive responses predicting PTSD symptoms, and the quadratic slope of negative responses predicting externalizing symptoms. Such a pattern could be related to low reliability of the predictor variables, which would increase risk of Type I error; however, the ICCs were all in the good to excellent range (.66–.91; Cicchetti, 1994), and all of the analyses in question produced nonsignificant findings. Furthermore, other models including the same predictors had much smaller standard errors and confidence intervals, which suggests that the problem was not with the predictor variables. It is possible that we were somewhat underpowered to detect significant effects given the nature of the models (i.e., using within-persons slopes as predictors) relative to the sample size. These findings will require replication in a larger sample to assure that null findings were not due to insufficient power.
Conclusion
Overall, the present findings add to the research on processes of change in TF-CBT. Consistent with the broader framework of EPT (Foa et al., 2006), we found that an increase and then decrease (a curvilinear pattern) of multimodal pathological responses over the course of the trauma-narration and -processing phase of TF-CBT predicted improvement in internalizing and PTSD symptoms. In addition, increases in multimodal adaptive responses predicted improvement in externalizing symptoms. These findings have implications for both research and clinical practice. Researchers might broaden the measurement of emotional processing and processes of change in PTSD treatments to include pathological and adaptive trauma-related responses across multiple domains, including cognitions, emotions, behaviors, and physiological responses. Our findings also illustrate the importance of examining not only linear but also nonlinear patterns of change. TF-CBT clinicians might target activation and change in trauma responses across multiple domains, facilitate an increase then a decrease in negative responses during trauma processing, and also help clients to develop new, more positive responses to traumatic experiences.
Footnotes
Acknowledgements
We thank our coding team for their help, Jean-Philippe Laurenceau and Emily Soriano for feedback on statistical analyses, and Edna Foa for her helpful comments on a previous draft of the manuscript.
Transparency
Action Editor: Stefan G. Hofmann
Editor: Scott O. Lilienfeld
Author Contributions
E. Alpert developed the rationale and method for applying EPT to this investigation of change processes in TF-CBT and conducted the data analyses and interpretation under the supervision of A. M. Hayes. E. Alpert and A. M. Hayes drafted the manuscript. A. M. Hayes designed and conducted the clinical trial on which this study was based and developed the CHANGE coding system used in the current study. C. Yasinski trained coders and supervised coder meetings. C. Webb and E. Deblinger trained and supervised study therapists throughout the clinical trial. All of the authors provided critical revisions and approved the final manuscript for submission.