
Abstract
We examined associations between common psychiatric disorders and fecundity in a population-based cohort of 1,252 twins prospectively assessed from adolescence into adulthood. Major depressive disorder, anxiety disorders, and alcohol use disorders were associated with lower likelihood of having children and having fewer children. Survival analyses yielded similar results accounting for timing and recurrence. Although both early- and adult-onset psychiatric disorders were associated with decreased fecundity, early-onset major depressive disorder, anxiety disorders (among boys), and alcohol use disorders (among girls) were associated with greater likelihood of having a child during adolescence. Among twin pairs discordant for psychiatric disorders (i.e., one twin affected and one twin unaffected by major depressive disorder, anxiety disorders, or alcohol use disorders), twins affected by anxiety and alcohol use disorders but not major depressive disorder were less likely to have children than their unaffected co-twins. However, unaffected twins with an affected co-twin were no more likely to have children than twins from unaffected twin pairs, inconsistent with the balancing-selection hypothesis that increased fecundity in unaffected relatives accounts for persistence of psychiatric disorders.
Decades of research indicate that severe, relatively rare psychiatric disorders (autism, schizophrenia, bipolar disorder) are associated with lower likelihood of having children, fewer children, and advanced paternal age, collectively referred to as decreased fecundity (Baron, Risch, & Mendlewicz, 1982; Bundy, Stahl, & MacCabe, 2011; Durkin et al., 2008; Frans et al., 2008; Frans, Lichtenstein, Hultman, & Kuja-Halkola, 2016; Jacobson, 2016; Jönsson, 1991; Malaspina et al., 2001; Power et al., 2013; Reichenberg et al., 2006). This well-established phenomenon of decreased fecundity for severe psychiatric disorders defies the expectations of natural selection—that is, genetic variants that reduce reproductive fitness are less likely to be passed on to offspring and should eventually be eliminated from the general population. Severe psychiatric disorders are highly heritable, typically onset before or around childbearing age, and are associated with decreased fecundity, but they nonetheless persist. One possible explanation for this apparent paradox is balancing selection, or the hypothesis that the genetic variants underlying psychiatric disorders confer advantages that increase reproductive fitness, if not in affected individuals, instead in their genetically related family members. If so, we would expect to see increased fecundity in unaffected biological relatives of affected individuals. However, this does not appear to be the case for autism, schizophrenia, or bipolar disorder (Bundy et al., 2011; Frans et al., 2016; Power et al., 2013).
What about more common forms of psychiatric disorders? Major depressive disorder, anxiety disorders, and alcohol use disorders occur more frequently in the general population than autism, schizophrenia, and bipolar disorder, with lifetime prevalence rates for common psychiatric disorders ranging from approximately 15% to 40% compared with < 1% to approximately 1% for severe psychiatric disorders (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2010 Principal Investigators, 2014; Hamdi & Iacono, 2014; Kessler et al., 2005; Merikangas et al., 2007; Moffitt et al., 2010). As for more severe psychiatric disorders, these common psychiatric disorders are highly polygenic (Kranzler et al., 2019; Milaneschi et al., 2016; Smoller, Gardner-Schuster, & Covino, 2008), and they are also heritable, although less so than more severe psychiatric disorders (heritability estimates for common psychiatric disorders range from approximately 20% to 50%, compared with approximately 60% to 90% for severe psychiatric disorders; Hettema, Neale, & Kendler, 2001; Sullivan, Neale, & Kendler, 2000; Verhulst, Neale, & Kendler, 2015; Wray & Gottesman, 2012).
Compared with severe psychiatric disorders, considerably less research has yet considered whether more common psychiatric disorders are also associated with decreased fecundity. One study found that major depressive disorder during the lifetime was associated with having fewer children among affected men, but not women, relative to the Swedish general population (Power et al., 2013). Another study, from the National Comorbidity Survey in the United States, found that depressive disorders (i.e., major depression, dysthymia) in adolescence and adulthood predicted having fewer children among affected women and men; anxiety disorders (i.e., social phobia, panic, specific phobia, agoraphobia, generalized anxiety) in adolescence predicted having more children in early adulthood among affected men, but not women, but anxiety disorders in adulthood predicted having fewer children among affected women and men (Jacobson, 2016). Both of these studies found that alcohol and drug use disorders were associated with having fewer children among affected women and men. Another series of studies, conducted in Australia, found that alcohol use disorders were associated with older age at first child among women but not men (Waldron, Heath, Bucholz, Madden, & Martin, 2008). Note that among the women in this sample, alcohol use disorders were associated with early childbearing in adolescence but delayed childbearing in adulthood (Waldron et al., 2014).
Results from the small number of initial studies thus suggest that common psychiatric disorders are associated with decreased fecundity, although there may be some nuances in timing of childbearing. These studies have capitalized on large, population-based samples but have necessarily been limited to somewhat coarse indicators of both psychiatric disorders (e.g., chart review of diagnoses made during hospitalizations and outpatient visits) and fecundity (e.g., number of living biological children, age at first childbirth). However, having children is not a static event—psychiatric disorders may be associated with variations in the timing of children during the life span or different associations with fecundity during different developmental periods. An event-level analytic approach (i.e., having ever had children, total number of children) is informative but is complemented by one that considers events, event recurrence, and event duration (i.e., time to child, time to subsequent children). Survival analysis quantifies the “hazard” or the probability of a given outcome occurring over time—in this case, the “relative risk” or likelihood of having a child as it relates to psychiatric disorder, taking into consideration variation in the timing and number of children across the lifetime.
Studies comparing the fecundity of individuals affected by severe psychiatric disorders, including autism, schizophrenia, and bipolar disorder, with their unaffected siblings, who share genes but not diagnosis, have found comparably decreased fecundity (Bundy et al., 2011; Frans et al., 2008, 2016; Gratten et al., 2016; Power et al., 2013). This well-replicated finding in large samples speaks against balancing selection and suggests there are negative influences on fecundity that are shared by family members—genetic or environmental liability that deleteriously affects fecundity even in unaffected siblings. We are aware of only one study that considered more common psychiatric disorders in affected individuals and their unaffected siblings. Individuals affected by depressive or substance use disorders had fewer children than their unaffected siblings, particularly unaffected sisters, although effects overall were small (Power et al., 2013). Thus, this study provides initial suggestive evidence of balancing selection for some common forms of psychopathology (i.e., depression and substance use).
In the present study, we examined associations between common psychiatric disorders and fecundity in a population-based sample of twins that had been prospectively assessed from adolescence into middle adulthood. We extended previous research by considering the three most common forms of internalizing and externalizing psychopathology (Kessler et al., 2005)—major depressive disorder, anxiety disorders, and alcohol use disorders. We used “gold-standard” assessments of psychiatric disorders (prospective, longitudinal assessment at multiple time points that increase diagnostic sensitivity and are more likely to capture less severe cases; Hamdi & Iacono, 2014) as well as detailed information on whether and at what age participants had children. We considered multiple indicators of fecundity, including having ever had children, the total number of children, and the likelihood (relative risk) of having children (including duration to and recurrence of children). Drawing on findings for severe psychiatric disorders (Baron et al., 1982; Bundy et al., 2011; Durkin et al., 2008; Frans et al., 2008; Frans et al., 2016; Jacobson, 2016; Jönsson, 1991; Malaspina et al., 2001; Power et al., 2013; Reichenberg et al., 2006), as well as the few existing studies of more common psychiatric disorders (Jacobson, 2016; Power et al., 2013; Waldron et al., 2008; Waldron et al., 2014), we expected to find that major depressive disorder and anxiety and alcohol use disorders were associated with decreased fecundity (lower rates of having children, fewer children, lower likelihood of having children accounting for timing/variation) across the life span.
We leveraged our prospective assessments of psychiatric disorders to also consider whether early occurrence of psychiatric disorders (i.e., onset during childhood or adolescence) was differentially associated with fecundity over the life span compared with adult-onset psychiatric disorders and whether early-onset psychiatric disorders were associated with early childbearing (i.e., having a child during adolescence). Early-onset psychiatric disorders (particularly those that persist into adulthood) are associated with poorer outcomes (Essau, Lewinsohn, Olaya, & Seeley, 2014; Green et al., 2016; Hicks, Iacono, & McGue, 2010; Wilson, Hicks, Foster, McGue, & Iacono, 2015; Woodward & Fergusson, 2001), which suggests that deleterious effects on fecundity might be particularly pronounced. However, there is also initial evidence that boys with anxiety disorders in adolescence have more children in early adulthood (Jacobson, 2016), whereas alcohol and other substance use in adolescence is associated with early pregnancy among girls (Waldron et al., 2014), which suggests that early-onset psychiatric disorders might be associated with increased fecundity, or greater likelihood of having a child, at least earlier in life.
Finally, we examined whether twin discordance in common psychiatric disorders (i.e., one twin affected and one twin unaffected by major depressive disorder, anxiety disorders, or alcohol use disorders) was associated with differences in fecundity. As with the sibling-control studies reviewed above, the discordant twin study design used here is a type of “natural” experiment (McGue, Osler, & Christensen, 2010; Rutter, 2007) in which fecundity among twins in pairs discordant for psychiatric disorders is compared. The discordant twin design is even more powerful (i.e., accounts for more potentially confounding factors) than the sibling-control study design used in previous research. Monozygotic (MZ; “identical”) twins share 100% of their segregating genes, and dizygotic (DZ; “fraternal”) twins share 50%, as do nontwin siblings. By definition, reared-together MZ and DZ twins and siblings share 100% of their early rearing environment, and because they are the same age, twins typically have more common experiences than typical nontwin siblings. Thus, twins who were reared together share both genes and early environments and provide powerful controls for potential confounding by these familial influences. If twins affected by common psychiatric disorders have decreased fecundity relative to unaffected co-twins, as was found for affected and unaffected siblings (Power et al., 2013), and if unaffected twins with an affected co-twin have increased fecundity relative to unaffected twins without an affected co-twin, this would provide further evidence of balancing selection for common forms of psychopathology. This would also implicate the role of the nonshared environment—that is, the effects of psychopathology itself or the unique experiences that influence the development of the psychiatric disorder—in accounting for differences in fecundity above and beyond the twin pairs’ shared genetic/environmental liability. In contrast, if twins discordant for common psychiatric disorders are comparably as likely to have children, this would be inconsistent with balancing selection and would suggest shared familial liability accounts for decreased fecundity for common psychiatric disorders, as found for more severe psychiatric disorders (Bundy et al., 2011; Frans et al., 2016; Power et al., 2013).
Method
Participants and procedures
Participants were 1,252 same-sex male and female twins (626 twin pairs, 67% MZ, 54% female) participating in the Minnesota Twin Family Study (MTFS), an ongoing, population-based, longitudinal study of twins who were reared together. The study design and sample have been described extensively elsewhere (Iacono, Carlson, Malone, & McGue, 2002; Iacono, McGue, & Krueger, 2006; Wilson et al., 2019). In brief, twin pairs born in Minnesota between 1972 and 1979, identified from publicly available birth records, were eligible if they lived within a day’s drive of the University of Minnesota and had no physical or psychological characteristics that would preclude completing the assessment. Participants were first assessed at target age 17 years (M = 17.48, SD = 0.46), along with their parents, and participated in follow-up assessments at target ages of 20 (M = 20.67, SD = 0.57), 24 (M = 24.70, SD = 0.97), and 29 years (M = 29.62, SD = 0.61). Each comprehensive assessment included interview assessment of psychiatric diagnoses as well as questionnaire and laboratory components. Retention across follow-ups has been high (range = 83%–95% across assessments), with little evidence of bias because of attrition (Iacono et al., 2002; Iacono et al., 2006). Approximately 8 years after the age-29 assessment, at age 37 (M = 36.57, SD = 1.92), participants were invited to complete a brief survey regarding household composition, including children. A total of 1,107 twins (88% of the baseline sample) completed the survey. 1 The study was approved by the University of Minnesota Institutional Review Board. Written informed parental consent and participant assent (before age 18) and participant consent (after age 18) were obtained.
Measures
Family demographics
Participants’ parents reported on race-ethnicity, parental education status, and household income at the age-17 intake assessment. Consistent with demographics of Minnesota during the targeted birth years, participating families were predominantly White (97%). Participating families were also representative of Minnesota during the targeted birth years in parental education status (years of education: M = 13, SD = 2; range = 6–20) and household income (M = $40,000–$45,000, range = < $10,000 to > $80,000).
Psychiatric diagnoses
Psychiatric diagnoses were as-sessed lifetime (at intake) or since the previous assessment (at follow-ups) according to criteria from the third edition (revised) and fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–III-R and DSM–IV) using semistructured interviews (Reich & Welner, 1988; Robins, Baber, & Cottler, 1987; Robins et al., 1988) administered by extensively trained interviewers. Interviews, conducted with participants and their mothers (reporting on each twin in the pair) at age 17 and with participants alone at ages 20, 24, and 29, were reviewed in case conferences, and each symptom or diagnostic criterion endorsed by participants or mothers was assigned by consensus of two individuals with advanced clinical training. Diagnoses included major depressive disorder, anxiety disorders (social phobia, specific phobia, panic disorder with and without agoraphobia, generalized anxiety disorder), and alcohol use disorders (abuse and dependence). Major depressive disorder diagnoses were assigned if criteria were met at a “definite” (i.e., at least five DSM criteria met) or “probable” (i.e., at least four DSM criteria met) level using Research Diagnostic Criteria (Spitzer, Endicott, & Robins, 1978) guidelines, which allow for the fact that most participants were not symptomatic at the time of the diagnostic assessment, meaning they had to rely on their memory of previous depressive episodes when reporting past symptoms. Anxiety and alcohol use disorders were assigned if criteria were met at a “definite” level (i.e., the required number of DSM criteria met for a diagnosis). Lifetime (at the age-29 assessment) rates were 33% for major depressive disorder, 20% for anxiety disorders, and 45% for alcohol use disorders. Of participants with a lifetime diagnosis of these disorders, 65%, 84%, and 66% had an early onset of major depressive disorder, anxiety disorders, or alcohol use disorders, respectively, defined here as during childhood/adolescence, before age 20. Interrater reliability for psychiatric diagnoses, assessed on a randomly selected subsample of 600 MTFS participants, was good (κ: M = .91).
Fecundity
Indicators of fecundity were assessed using a brief survey. Participants reported on whether they had any biological children and the number of children as well as their age at the birth of each child. Seventy-two percent of participants had children, they had an average of 1.56 (1.27) children, and participants’ mean age at first child was 27.74 years (SD = 4.54). Forty-seven (6%) participants had a child during adolescence, defined here as before 20 years (range = 14–19).
Statistical analyses
We conducted a series of generalized estimating equation (GEE) models to examine associations between major depressive disorder, anxiety disorders, and alcohol use disorders (in separate models) and event-related fecundity indicators (ever had children, total number of children, had a child during adolescence) using the geeglm function from the geepack package (Version 1.3-1; Hojsgaard, Halekoh, Yan, & Ekstrom, 2019) for the R software environment (Version 3.6.3; R Core Team, 2020). GEEs are an extension of generalized linear models that can accommodate correlated data structures (i.e., interdependent twin family data) by specifying a “working” correlation matrix for the model residuals with an iterative procedure. As an index of magnitude, we computed odds ratios (ORs) with 95% confidence intervals (CIs) for binary fecundity indicators (i.e., whether the person had ever had children). Psychiatric status was coded so that ORs < 1.00 indicated lower odds and ORs > 1.00 indicated greater odds of having children for affected relative to unaffected participants, early-onset relative to adult-onset psychiatric disorders, or affected relative to unaffected twins from discordant pairs. Total number of children was left unstandardized so that regression coefficients (b) indicated change in the number of children for affected relative to unaffected participants, early-onset relative to adult-onset psychiatric disorders, or affected relative to unaffected twins from discordant pairs. As an index of magnitude, we computed Cohen’s ds for total number of children using means adjusted for covariates in unequal groups; Cohen’s ds less than |0.20| are considered trivial, those between |0.20| and |0.50| are considered modest, those between |0.50| and |0.80| are considered moderate, and those greater than |0.80| are considered large (Cohen, 1988).
Next, we conducted a series of Cox proportional hazards models to examine associations between major depressive disorder, anxiety disorders, and alcohol use disorders (in separate models) and event- and time-varying fecundity indicators using the coxph function from the survival package (i.e., likelihood of “surviving” the “risk” of having a child; Version 3.2-7; Therneau, Lumley, Atkinson, & Crowson, 2020) for the R software environment. In these models, event (ever having a child), time to event (age at birth of child), and recurrence of event (age at birth of subsequent children) were allowed to vary across participants. Data were right-censored at the final survey assessment to account for any children that may yet be born after study participation. To account for participants with recurrent events (multiple children), models included a cluster term at the level of individual participants; to account for the interdependence of the twin family data, standard errors were adjusted with a sandwich estimator using the vcovCL function from the sandwich package (Version 3.0-0; Zeileis, Lumley, Graham, & Koell, 2020) for the R software environment. As an index of the relative risk of having a child, including variation in the timing and number of children over time, we computed hazard ratios (HRs) with 95% CIs. Psychiatric status was coded so that HRs < 1.00 indicated lower risk and HRs > 1.00 indicated greater risk of having children for affected than for unaffected twins, greater risk of early-onset than adult-onset psychiatric disorders, or greater risk of affected than unaffected twins from discordant pairs.
All models included age, sex, zygosity, race-ethnicity, parental education status, and childhood household income as covariates. We examined whether effects differed among men and women by including a Psychiatric Status × Sex interaction term. With the exception for early childbearing, there were no significant sex interactions (all ps > .320), so with that exception, all models were conducted for men and women combined. We also examined whether effects held when including comorbid psychiatric disorders in models. Finally, we examined whether effects differed among MZ and DZ twins by including a Psychiatric Status × Zygosity interaction term in discordant twin analyses. Evidence of stronger effects among DZ relative to MZ twins suggests confounding effects of familial influences (see McGue et al., 2010). Statistical significance was set at p < .050 for all analyses. All analyses were conducted using the R software environment (Version 3.6.3).
Results
Descriptive data for fecundity indicators (ever had children, total number of children) are presented in Table 1 by psychiatric disorder (affected vs. unaffected), onset of psychiatric disorder (early onset vs. adult onset), and psychiatric status among twin pairs discordant for psychiatric disorders (affected vs. unaffected), and results of GEE models examining associations between major depressive disorder, anxiety disorders, and alcohol use disorders and fecundity indicators are presented in Table 2. Rates of having ever had children were consistently lower among participants affected by psychiatric disorders than among unaffected participants, and the mean total number of children among affected participants was also consistently lower than among affected participants. Among twin pairs discordant for psychiatric disorders, rates of having ever had children and the mean total number of children were also lower among affected twins relative to their unaffected co-twins. In contrast, rates of having ever had children and the total number of children did not show consistent differences among participants whose psychiatric disorder first onset in adolescence relative to adulthood. Note that these event-related fecundity indicators provide an overall aggregate picture of fecundity as a function of psychiatric disorders. There was considerable individual variation across participants in when they had their first child (range = 14.81–40.11 years), whether they had another child (55%), the number of children they had (range = 0–7 children), and the amount of time before having subsequent children (range = 0–16.28 years).
Descriptive Statistics for Fecundity Indicators of the Sample
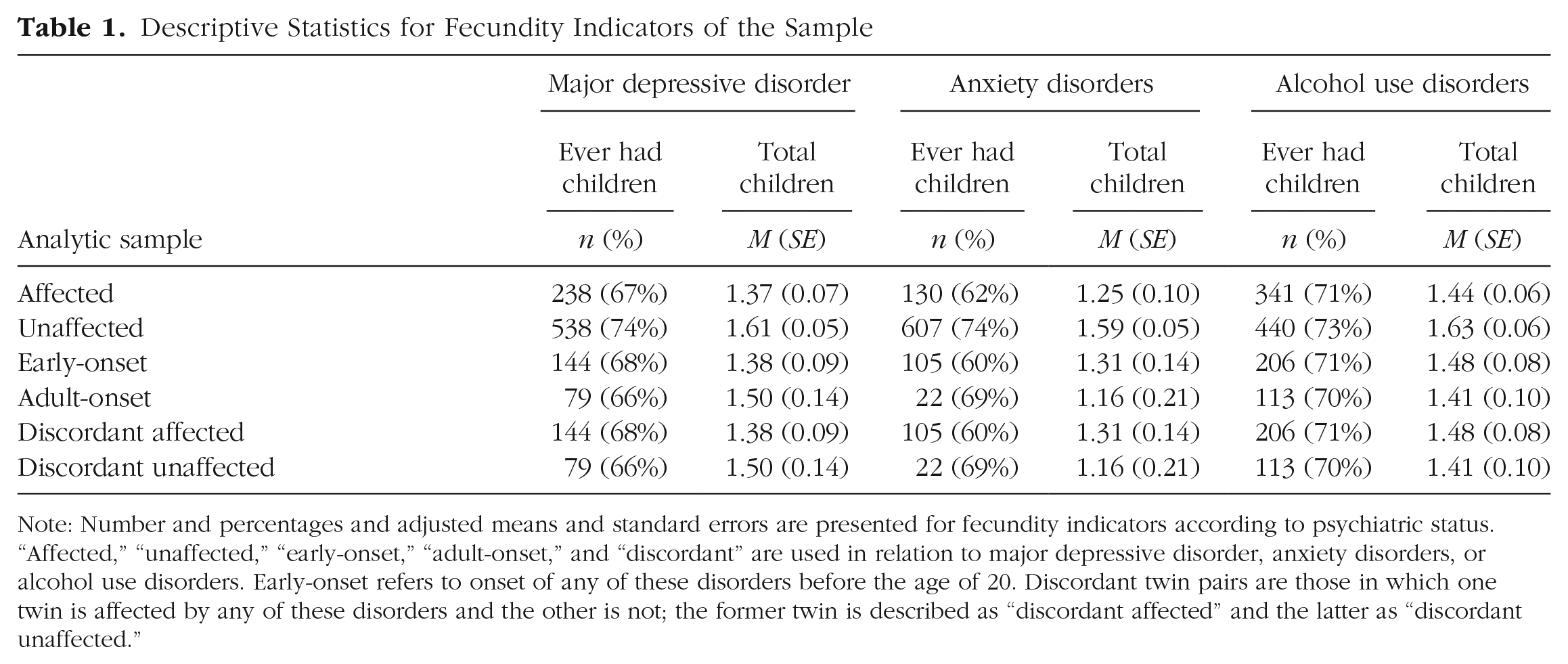
Note: Number and percentages and adjusted means and standard errors are presented for fecundity indicators according to psychiatric status. “Affected,” “unaffected,” “early-onset,” “adult-onset,” and “discordant” are used in relation to major depressive disorder, anxiety disorders, or alcohol use disorders. Early-onset refers to onset of any of these disorders before the age of 20. Discordant twin pairs are those in which one twin is affected by any of these disorders and the other is not; the former twin is described as “discordant affected” and the latter as “discordant unaffected.”
Results of Generalized Estimating Equation Models Examining Associations Between Psychiatric Disorders and Fecundity Indicators
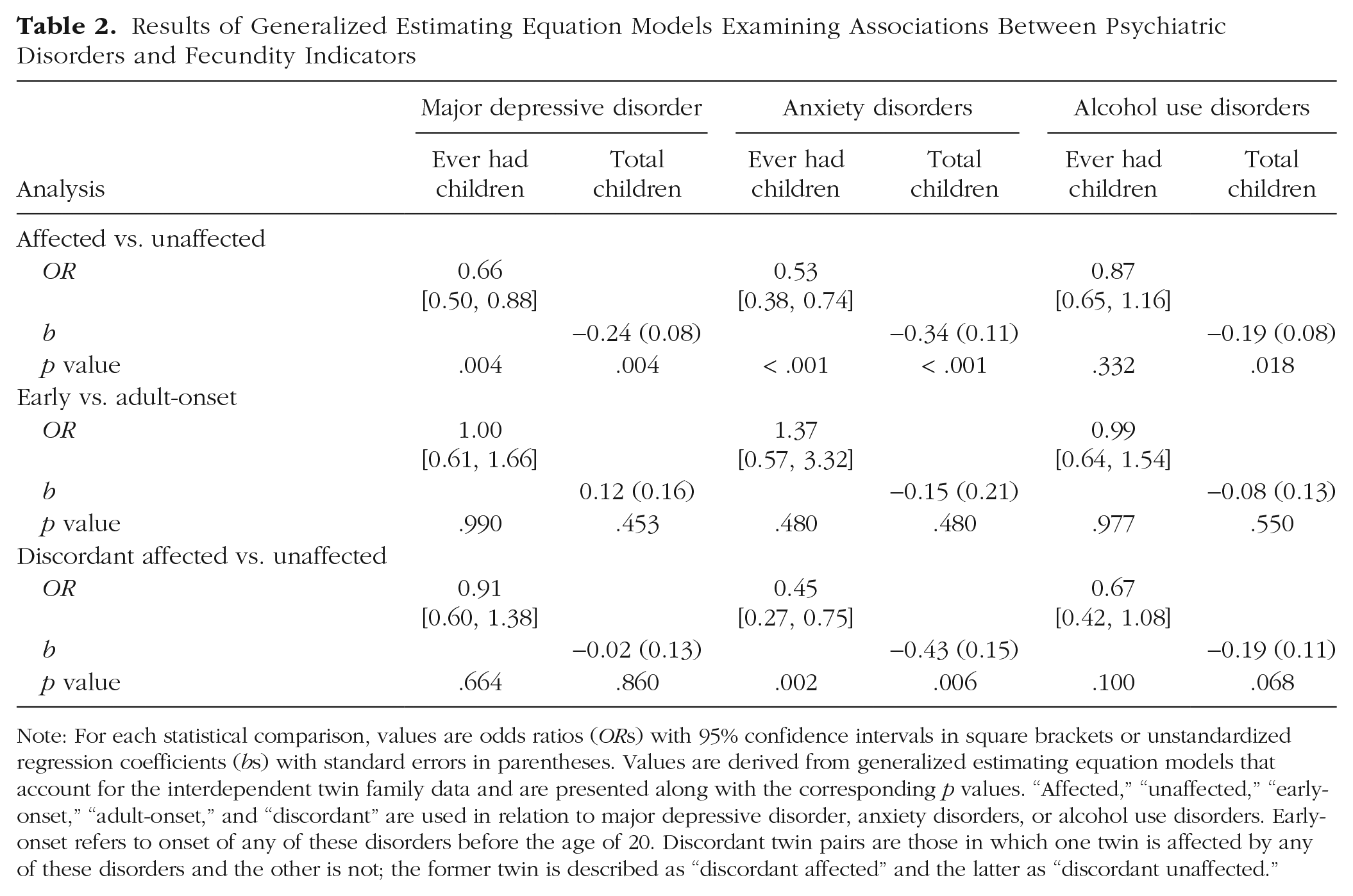
Note: For each statistical comparison, values are odds ratios (ORs) with 95% confidence intervals in square brackets or unstandardized regression coefficients (bs) with standard errors in parentheses. Values are derived from generalized estimating equation models that account for the interdependent twin family data and are presented along with the corresponding p values. “Affected,” “unaffected,” “early-onset,” “adult-onset,” and “discordant” are used in relation to major depressive disorder, anxiety disorders, or alcohol use disorders. Early-onset refers to onset of any of these disorders before the age of 20. Discordant twin pairs are those in which one twin is affected by any of these disorders and the other is not; the former twin is described as “discordant affected” and the latter as “discordant unaffected.”
Common psychiatric disorders and fecundity
We first examined rates of having ever had children among participants affected and unaffected by common psychiatric disorders. As shown in Table 1, affected participants had lower rates of having ever had children relative to unaffected participants. As shown in Table 2, rates were significantly lower among participants affected by major depressive disorder or anxiety disorders but not alcohol use disorders. Participants affected by major depressive disorder were 34% less likely to ever have children, and participants affected by anxiety disorders were 47% less likely to ever have children than participants unaffected by these disorders. Results were somewhat attenuated but held even when accounting for comorbid psychiatric disorders (major depressive disorder: OR = 0.73, 95% CI = [0.54, 0.99], p = .040; anxiety disorders: OR = 0.55, 95% CI = [0.39, 0.78], p < .001).
We also examined associations between common psychiatric disorders and the total number of children. Participants affected by major depressive disorder, anxiety disorders, and alcohol use disorders had significantly fewer children relative to unaffected participants (Tables 1 and 2). Participants affected by these disorders had an average of around one-quarter fewer children than unaffected participants; effects were at most modest (Cohen’s ds range = −0.14 to −0.24). Results held even when accounting for comorbid psychiatric disorders (major depressive disorder: b = −0.18, SE = 0.09, p = .043; anxiety disorders: b = −0.30, SE = 0.11, p = .006; alcohol use disorders: b = −0.17, SE = 0.08, p = .042).
We conducted survival analyses that considered the likelihood of having children among participants affected and unaffected by common psychiatric disorders, taking into consideration the considerable variation in the timing and number of children. Participants affected by major depressive disorder, anxiety disorders, and alcohol use disorders had lower likelihood of having children (major depressive disorder: HR = 0.85, 95% CI = [0.76, 0.96], p = .007; anxiety disorders: HR = 0.81, 95% CI = [0.67, 0.96], p = .018; alcohol use disorders: HR = 0.88, 95% CI = [0.79, 0.97], p = .012). Participants affected by major depressive disorder were 15% less likely, participants affected by anxiety disorders were 19% less likely, and participants affected by alcohol use disorders were 12% less likely to have children at any point in time. Results held even when accounting for comorbid psychiatric disorders for anxiety and alcohol use disorders but became nonsignificant for major depressive disorder (major depressive disorder: HR = 0.89, 95% CI = [0.78, 1.00], p = .054; anxiety disorders: HR = 0.83, 95% CI = [0.69, 0.99], p = .043; alcohol use disorders: HR = 0.89, 95% CI = [0.80, 0.99], p = .029).
Taken together, these results indicate that common psychiatric disorders, including major depressive disorder, anxiety disorders, and alcohol use disorders, are deleteriously associated with various indicators of fecundity.
Timing of onset of common psychiatric disorders and fecundity
We next examined rates of having ever had children among participants with an early (childhood or adolescence, before age 20) or an adult (after age 20) onset of common psychiatric disorders. As shown in Tables 1 and 2, participants with an early-onset psychiatric disorder and those with an adult-onset psychiatric disorder had comparable rates of having ever had children. Rates were comparable among participants with an early onset of major depressive disorder, anxiety disorders, and alcohol use disorder. Participants with an early onset of these disorders were statistically as likely to ever have children as those with an adult onset of these disorders.
We also examined associations between the timing of onset of psychiatric disorders and total number of children. Participants with an early onset of major depressive disorder, anxiety disorders, or alcohol use disorder had a comparable number of children relative to those with an adult onset (Tables 1 and 2). Associations with total number of children were comparable among participants with an early onset of major depressive disorder, anxiety disorders, and alcohol use disorder. Participants with an early onset of these disorders had a statistically comparable number of children as those with an adult onset of these disorders; effects were trivial (Cohen’s ds range = −0.09 to 0.09).
We conducted survival analyses that considered the likelihood of having children among participants with an early-onset or adult-onset psychiatric disorder, taking into consideration variation in the timing and number of children. Participants with an early-onset of major depressive disorder, anxiety disorders, and alcohol use disorders had comparable likelihood of having children relative to those with an adult onset (major depressive disorder: HR = 1.09, 95% CI = [0.85, 1.39], p = .552; anxiety disorders: HR = 0.89, 95% CI = [0.68, 1.16], p = .387; alcohol use disorder: HR = 0.96, 95% CI = [0.81, 1.13], p = .602).
Taken together, these results indicate that common psychiatric disorders, including major depressive disorder, anxiety disorders, and alcohol use disorders, that onset in childhood/adolescence relative to adulthood are not differentially associated with various indicators of fecundity.
Early-onset common psychiatric disorders and early childbearing
We next examined rates of early childbearing (during adolescence, before age 20) among participants with and without an early onset of common psychiatric disorders. To ensure that psychiatric disorders were not a consequence of early childbearing (e.g., becoming depressed after having a child in adolescence), we excluded any participant whose early-onset disorder first occurred after having a child (34 participants with major depressive disorder, two participants with an anxiety disorder, zero participants with an alcohol use disorder). Among participants who had a child during adolescence, 13% had an early-onset major depressive disorder and 4% had not, 10% had an early-onset anxiety disorder and 5% had not, and 12% had an early-onset alcohol use disorder and 5% had not. Rates were significantly higher among participants with an early onset of major depressive disorder but were nonsignificant for anxiety and alcohol use disorders (major depressive disorder: OR = 3.93, 95% CI = [1.86, 8.31], p < .001; anxiety disorders: OR = 1.71, 95% CI = [0.75, 3.92], p = .206; alcohol use disorders: OR = 1.97, 95% CI = [0.93, 4.17], p = .078). Results were somewhat attenuated but held even when accounting for comorbid psychiatric disorders for major depressive disorder (OR = 3.44, 95% CI = [1.58, 7.49], p = .002).
Significant sex interactions indicated that rates differed among boys and girls for anxiety disorders, p < .001, and alcohol use disorders, p = .036. Among boys who had a child during adolescence, 13% had an early-onset anxiety disorder and 6% did not; among girls, 0% had an early-onset anxiety disorder and 3% did not. Rates among boys with an early onset of anxiety disorders were significantly higher relative to boys without an early onset of anxiety disorders and were significantly lower among girls with an early onset of anxiety disorders (boys: OR = 2.62, 95% CI = [1.02, 6.76], p = .046; girls: OR = 0.00, 95% CI = [0.00, 0.00], p < .001). Results held even when accounting for comorbid psychiatric disorders for boys and girls (boys: OR = 2.51, 95% CI = [1.01, 6.20], p = .047; girls: OR = 0.00, 95% CI = [0.00, 0.00], p < .001). Among girls who had a child during adolescence, 6% had an early-onset alcohol use disorder and 1% did not, and among boys, 9% had an early-onset alcohol use disorder and 8% did not. Rates among girls with an early onset of alcohol use disorders were significantly higher relative to girls without an early onset of alcohol use disorders and did not differ among boys with and without an early onset of alcohol use disorders (boys: OR = 1.05, 95% CI = [0.35, 3.16], p = .933; girls: OR = 14.07, 95% CI = [2.31, 85.65], p < .001). Results held even when accounting for comorbid psychiatric disorders for girls (OR = 30.02, 95% CI = [6.42, 140.36], p < .001).
Taken together, these results indicate that early onset of common psychiatric disorders, including major depressive disorder, anxiety disorders, and alcohol use disorders, is associated with early childbearing. However, for anxiety disorders, the association with early childbearing is specific to boys; for girls, anxiety disorders may instead be protective against early childbearing. In contrast, for alcohol use disorders, the association with early childbearing is specific to girls.
Fecundity among twins discordant for common psychiatric disorders
We examined whether rates of having ever had children differed among discordant twin pairs in which one twin was affected and one twin was unaffected by common psychiatric disorders. As shown in Table 1, affected twins from discordant twin pairs had lower rates of having ever had children relative to their unaffected co-twins. As shown in Table 2, rates were significantly lower among twins affected by anxiety but not major depressive disorder or alcohol use disorders. Twins affected by anxiety disorders were 20% less likely to ever have children than their unaffected co-twins. Results were somewhat attenuated but held even when accounting for comorbid psychiatric disorders for anxiety disorders (OR = 0.47, 95% CI = [0.28, 0.80], p = .005). Note that unaffected twins from discordant twin pairs had comparable rates of having ever had children relative to twins from pairs in which both twins were unaffected. Rates were statistically comparable among unaffected twins from discordant twin pairs for major depressive disorder, anxiety disorders, and alcohol use disorders (major depressive disorder: OR = 0.77, 95% CI = [0.51, 1.18], p = .227; anxiety disorders: OR = 0.89, 95% CI = [0.56, 1.42], p = .614; alcohol use disorders: OR = 1.30, 95% CI = [0.83, 2.04], p = .258). Unaffected twins from discordant twin pairs were as likely to have children as twins from unaffected twin pairs.
We also examined whether the total number of children differed among discordant twin pairs in which one twin was affected and one twin was unaffected by common psychiatric disorders. Twins from discordant twin pairs affected by anxiety disorders, but not major depressive disorder or alcohol use disorders, had significantly fewer children relative to their unaffected co-twins (Tables 1 and 2). Twins affected by anxiety disorders had an average of almost half as many children than their unaffected co-twin; effects were modest for anxiety disorders (Cohen’s d = −0.30) and trivial for major depressive disorder (Cohen’s d = −0.02) and alcohol use disorders (Cohen’s d = −0.16). Results held even when accounting for comorbid psychiatric disorders for anxiety disorders (b = −0.40, SE = 0.15, p = .010). Note that unaffected twins from discordant twin pairs had a statistically comparable number of children relative to twins from unaffected twin pairs for major depressive disorder, anxiety disorders, and alcohol use disorders (major depressive disorder: b = −0.01, SE = 0.12, p = .971; anxiety disorders: b = −0.08, SE = 0.13, p = .548; alcohol use disorders: b = −0.06, SE = 0.12, p = .630). Unaffected twins from discordant twin pairs had a comparable number of children as twins from unaffected twin pairs; effects were trivial (Cohen’s ds range = 0.00–0.08).
We conducted survival analyses that considered the likelihood of having children among discordant twin pairs in which one twin was affected and one twin was unaffected by common psychiatric disorders, taking into consideration variation in the timing and number of children. Twins from discordant twin pairs affected by anxiety and alcohol use disorders, but not major depressive disorder, had lower likelihood of having children (major depressive disorder: HR = 0.97, 95% CI = [0.81, 1.18], p = .775; anxiety disorders: HR = 0.74, 95% CI = [0.56, 0.99], p = .047; alcohol use disorders: HR = 0.87, 95% CI = [0.75, 0.99], p = .043). Twins affected by anxiety disorders were 26% less likely and twins affected by an alcohol use disorder were 13% less likely to have children at any point in time relative to their unaffected co-twins. Results held even when accounting for comorbid psychiatric disorders for alcohol use disorders but became nonsignificant for anxiety disorders (anxiety disorders: HR = 0.76, 95% CI = [0.57, 1.01], p = .062; alcohol use disorders: HR = 0.84, 95% CI = [0.72, 0.98], p = .022). Note that unaffected twins from discordant twin pairs had a statistically comparable likelihood of having children relative to twins from unaffected twin pairs for major depressive disorder, anxiety disorders, and alcohol use disorders (major depressive disorder: HR = 1.01, 95% CI = [0.86, 1.19], p = .894; anxiety disorders: HR = 0.95, 95% CI = [0.82, 1.11], p = .530; alcohol use disorders: HR = 0.97, 95% CI = [0.83, 1.12], p = .648). Unaffected twins from discordant twin pairs were as likely to have children as twins from unaffected twin pairs.
Finally, we examined whether effects differed as a function of zygosity. There were no significant interaction effects for zygosity for major depressive disorder or anxiety disorders for any fecundity indicator (all ps > .073), which indicates that associations between these psychiatric disorders and decreased fecundity did not differ significantly among MZ and DZ twins and suggests effects were unconfounded by familial influences.
Taken together, these results indicate that among twin pairs discordant for anxiety and alcohol use disorders but not major depressive disorders, the affected twin shows negative associations with various indicators of fecundity. However, unaffected twins from discordant twin pairs did not show decreased fecundity compared with twins from unaffected twin pairs (in which both twins in the twin pair are unaffected).
Discussion
We examined associations between common psychiatric disorders—major depressive disorder, anxiety disorders, and alcohol use disorders—in a population-based sample of men and women who had been prospectively assessed from adolescence into middle adulthood. We found evidence of decreased fecundity, indexed by lower rates of having ever had children, having fewer children, and lower likelihood of having children across the life span, among individuals affected by these common psychiatric disorders. These results add to the relatively larger body of research finding evidence of decreased fecundity for more severe forms of psychopathology, including autism, schizophrenia, and bipolar disorder (Baron et al., 1982; Bundy et al., 2011; Durkin et al., 2008; Frans et al., 2008; Frans et al., 2016; Jacobson, 2016; Jönsson, 1991; Malaspina et al., 2001; Power et al., 2013; Reichenberg et al., 2006), and the very small number studies that have considered more common psychiatric disorders (Jacobson, 2016; Power et al., 2013; Waldron et al., 2008; Waldron et al., 2014). We extended the existing research on common psychiatric disorders by considering multiple indicators of fecundity, including both event-related indicators (i.e., having ever had children and the total number of children during the lifetime), and conducting survival analyses that considered time-varying indicators (i.e., time to first child, time to subsequent children). Results were largely consistent across these indicators, which indicates that common psychiatric disorders are generally and deleteriously associated with fecundity.
We found no significant differences in fecundity as a result of early-onset (in childhood or adolescence) versus later-onset (in adulthood) psychiatric disorders. Participants with early-onset disorders showed comparably decreased fecundity over the life span as those with adult-onset disorders. However, we did find some nuances in the timing of childbearing and differences in associations for boys and girls. Major depressive disorder was associated with greater likelihood of early childbearing (during adolescence); because we excluded the relatively small number of participants whose major depressive disorder first onset after having a child, this finding is consistent with effect of major depressive disorder on early childbearing. Anxiety disorders were associated with greater likelihood of early childbearing among boys, consistent with evidence that boys with anxiety disorders in adolescence have more children in early adulthood (Jacobson, 2016). However, anxiety disorders were associated with lower likelihood of early childbearing among girls, which suggests that anxiety in girls might actually be protective against early childbearing. In contrast, early-onset alcohol use disorders were associated with greater likelihood of early childbearing among girls, but not boys, as found in another series of studies in Australia (Waldron et al., 2008; Walderon et al., 2014).
We leveraged our twin sample to examine potential mechanisms by which common psychiatric disorders are associated with fecundity. We found that in comparisons among twin pairs discordant for anxiety and alcohol use disorders, the affected twin showed decreases in various indicators of fecundity. Twins affected by anxiety and alcohol use disorders were less likely to ever have children, had fewer children, and had lower likelihood of having children across the life span relative to their unaffected co-twins. Because twins reared together share genetic liability and the early family environment, this finding implicates the negative effects of anxiety or drinking on fecundity or twins’ unique experiences that gave rise to anxiety or led to problematic drinking, or both. In contrast, twins affected by major depressive disorder and their unaffected co-twins both showed negative associations with various indicators of fecundity. This suggests that shared familial liability (rather than depressive symptomatology per se) may account for decreased fecundity—even when this liability is unexpressed. This finding for major depressive disorder is consistent with research on autism, schizophrenia, and bipolar disorder, which found decreased fecundity among unaffected siblings (Bundy et al., 2011; Frans et al., 2016; Power et al., 2013).
Note that that even though affected twins from twin pairs discordant for anxiety and alcohol use disorders showed decreased fecundity relative to their unaffected co-twins, these unaffected twins from discordant twin pairs did not show increased fecundity relative to twins from unaffected twin pairs (in which both twins in the pair were unaffected). This is inconsistent with the balancing-selection hypothesis, in which unaffected relatives have increased fecundity, thereby perpetuating deleterious genetic variants in the general population. Thus, as for severe psychiatric disorders, alternative explanations must account for the seeming paradox of the persistence of common psychiatric disorders. Individuals with severe or common psychiatric disorders are less likely to have children and pass on their genes, but new incidences of psychiatric disorders may still occur because of de novo genetic mutations during spermatogenesis. Psychiatric disorders, along with most complex human phenotypes, are now known to be highly polygenic. The inevitable likelihood of mutational load across the many genetic variants that collectively confer risk for psychiatric disorders may account for their persistence (Keller & Miller, 2006).
Although we tested for sex-specific effects, with two notable exceptions for early childbearing, discussed below, we found little evidence of differences for men and women in our sample. This is in contrast to some previous findings of greater effects of severe and common psychiatric disorders among men than among women (Bundy et al., 2011; Power et al., 2013). It could be that we were simply underpowered to detect small sex differences. These divergent findings might also reflect national differences or secular change, given that participants in one study (Power et al., 2013) were born in Sweden between 1950 and 1970 and participants in this study were born in Minnesota between 1972 and 1979. Note that many previous studies relied on hospital discharge records for psychiatric disorder classification, meaning affected individuals experienced severe psychopathology. It is possible that fecundity for men is affected more adversely at more severe levels than in our population-based study of common psychiatric disorders. Lack of differential effects by sex suggests that common psychiatric disorders are comparably associated with men and women’s interest in and ability to attract mating partners or biological fertility, or both.
We did find two notable sex effects, both on early childbearing. Boys with an early-onset anxiety disorder were more likely to have a child during adolescence, whereas girls with an early-onset anxiety disorder were less likely to have a child during adolescence. This finding for boys with anxiety disorders is consistent with one other study in which anxiety disorders in adolescence predicted having more children in early adulthood among affected men but not women (Jacobson, 2016). We also found that early-onset alcohol use disorders were associated with greater likelihood of early childbearing among girls, but not boys, as found in another series of studies in Australia (Waldron et al., 2008; Waldron et al., 2014). These results highlight the importance of identification of and intervention for early-onset anxiety and alcohol use disorders.
The present study has a number of strengths, including gold-standard assessments of psychiatric diagnoses at multiple time points using highly reliable interviewing methods in a population-based sample of twins. We examined associations between common forms of psychiatric disorders and multiple indicators of fecundity, including event-related and time-varying indicators. We considered potentially important aspects of age of onset of psychiatric disorder (in childhood/adolescence vs. adulthood) and early childbearing. We examined for the first time fecundity among twins discordant for common psychiatric disorders, which allowed us to test one proposed hypothesis for the persistence of psychiatric disorders in the general population, balancing selection. The present study also has some limitations that prompt caution in interpreting the results and suggest important directions for future research. Although participants were in middle age at the most recent assessment, some may yet have a first child or additional children, and some may yet develop a psychiatric disorder. Although our sample is representative of Minnesota during the targeted birth years in demographic characteristics, because this is a predominantly White, non-Hispanic sample, it is unclear how these results will generalize to more racially and ethnically diverse samples.
Our use of prospective, gold-standard interviewing assessments of psychiatric disorders provides some advantages over the more commonly used chart review of medical records or single diagnostic assessment of lifetime history of psychiatric disorders. Reliance on hospital discharge records for psychiatric disorder classification means that only more severe cases are likely to be included. Retrospective assessment of psychiatric disorders is likely to underestimate rates substantially (Hamdi & Iacono, 2014; Moffitt et al., 2010; Olino et al., 2012). Our approach increases diagnostic sensitivity and is more likely to capture less severe cases. Because major depressive disorder, in particular, is characterized by recurrence and remission of episodes, and most participants were not symptomatic at the time of the diagnostic assessment, we followed Research Diagnostic Criteria (Spitzer et al., 1978) guidelines that relaxed the number of criteria necessary to the “probable” level (i.e., at least four DSM criteria met). It is important to note that psychopathology symptomatology is dimensionally distributed (Kotov et al., 2017). Subsyndromal symptoms are likely evident well before formal diagnosis, and it is unlikely that there is a stepwise threshold effect on fecundity once diagnostic criteria are met. Instead, deleterious associations with fecundity are likely evident even at subsyndromal levels and may differ at different levels along the syndrome dimension (see Jacobson & Roche, 2018), which highlights the importance of examining this question using dimensional indicators of psychopathology.
We used participants’ reports of whether and when they had children to operationally define indicators of fecundity (having ever had children, number of children, likelihood of having children across the life span). Most research on psychiatric disorders and fecundity has used existing data sets that have information on, for example, number of living children, but were not specifically designed to address more nuanced questions regarding fecundity. Thus, important issues remain unresolved. Although we and others have used births of children as indicators of fecundity, use of contraceptive methods confounds such measures—even individuals who are highly fertile may not have children (i.e., show decreased fecundity) because of their use of effective contraceptive methods. Relying on births of children as indicators of fecundity also fails to consider potential associations between psychiatric disorders and likelihood of miscarriage or therapeutic or elective abortion. In addition, although women necessarily know when they have given birth, it is possible that some of the male participants in our sample may have fathered children of whom they are unaware or that children they are rearing are not actually their biological children. Thus, future investigations should consider these potentially confounding factors by, for example, assessing pregnancies in addition to births and using measures of genetic relatedness. We were able to rule out the possibility that effects on fecundity really reflect a marriage effect, that is, that individuals with psychiatric disorders may be less likely to marry and therefore less likely to have children. Instead, we found little evidence that major depressive disorder, anxiety disorders, or alcohol use disorders were associated with lower likelihood of getting married, 2 which suggests that another mechanism accounts for the decreased fecundity we found for each of these disorders.
In conclusion, in the present study, we found associations between common psychiatric disorders and decreased fecundity. Major depressive disorder, anxiety disorders, and alcohol use disorders were each associated with lower rates of having ever had children, having fewer children, and lower likelihood of having children across the life span. However, early-onset anxiety disorders were associated with greater likelihood of early childbearing among boys, but not girls, and early-onset alcohol use disorders were associated with greater likelihood of early childbearing among girls. Among twin pairs discordant for psychiatric disorders, twins affected by anxiety and alcohol use disorders, but not major depressive, were less likely to have children than unaffected co-twins. Unaffected twins with an affected co-twin were not more likely to have children than twins from unaffected twin pairs (in which both twins in the pair were unaffected), inconsistent with the balancing-selection hypothesis that increased fecundity in unaffected relatives accounts for persistence of psychiatric disorders in the general population.
Footnotes
Acknowledgements
The protocol was approved by the University of Minnesota’s Institutional Review Board. The authors assert that all procedures contributing to this work were carried out in accordance with the provisions of the World Medical Association Declaration of Helsinki.
Transparency
Action Editor: Kenneth J. Sher
Editor: Scott O. Lilienfeld
Author Contributions
S. Wilson developed the study concept. M. McGue and W. G. Iacono contributed to the study design. Data collection was conducted under the supervision of M. McGue, W. G. Iacono, and I. J. Elkins. S. Wilson performed the data analysis and interpretation, with contributions from S. M. Malone and I. J. Elkins. S. Wilson drafted the manuscript, and I. J. Elkins, S. M. Malone, W. G. Iacono, and M. McGue provided critical revisions. All the authors approved the final manuscript for submission.