
Abstract
Mental disorders may be best represented by dimensional constructs that span traditional diagnostic boundaries. There is evidence that empirically derived dimensional phenotypes improve nosology and etiological research, but less is known about their clinical utility. We compared dimensional and categorical representations of anxiety and depression as predictors of response to psychological treatment in a large patient sample (N = 3,760). Confirmatory factor analysis demonstrated that an internalizing factor—hypothesized to be the substrate of anxiety and depression—explained correlations among interview-based diagnoses at treatment outset. The internalizing factor had consistent, albeit sometimes modest, prospective associations with all treatment outcome measures: global clinical improvement, anxiety and depression symptoms, and need for inpatient hospitalization (standardized effect range = .13–.43). Categorical diagnoses—except major depression—did not reliably predict treatment outcome after adjusting for the higher order internalizing dimension. We conclude that reorienting clinical assessment around transdiagnostic phenotypes might enhance prognosis and other aspects of clinical decision-making.
Keywords
Categorical diagnoses are the lexicon of mental health care. The categorical model, embedded in official taxonomies such as the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM–5; American Psychiatric Association, 2013), orients clinical services, professional training, and research activity. Nevertheless, it has some significant weaknesses, such as poor discriminant validity among supposedly discrete conditions, within-diagnosis heterogeneity, and diagnostic unreliability (reviewed in Clark, Cuthbert, Lewis-Fernández, Narrow, & Reed, 2017). These limitations complicate the design and interpretation of etiological research and clinical trials (Rodriguez-Seijas, Eaton, & Krueger, 2015). As investigators move to work around the constraints of categorical nosologies, transdiagnostic approaches to psychological disorders are becoming mainstream.
The Hierarchical Taxonomy of Psychopathology (HiTOP) consortium proposed a transdiagnostic model that is intended to supplement—and eventually supplant—the DSM. The model delineates the major phenotypic dimensions of psychopathology according to patterns of symptom covariation documented over decades of structural research (Kotov et al., 2017). It is anchored by six spectra that describe broad domains of psychopathology: internalizing, disinhibited externalizing, antagonistic externalizing, detachment, thought disorder, and somatoform (see Conway et al., 2019, Fig. 1).
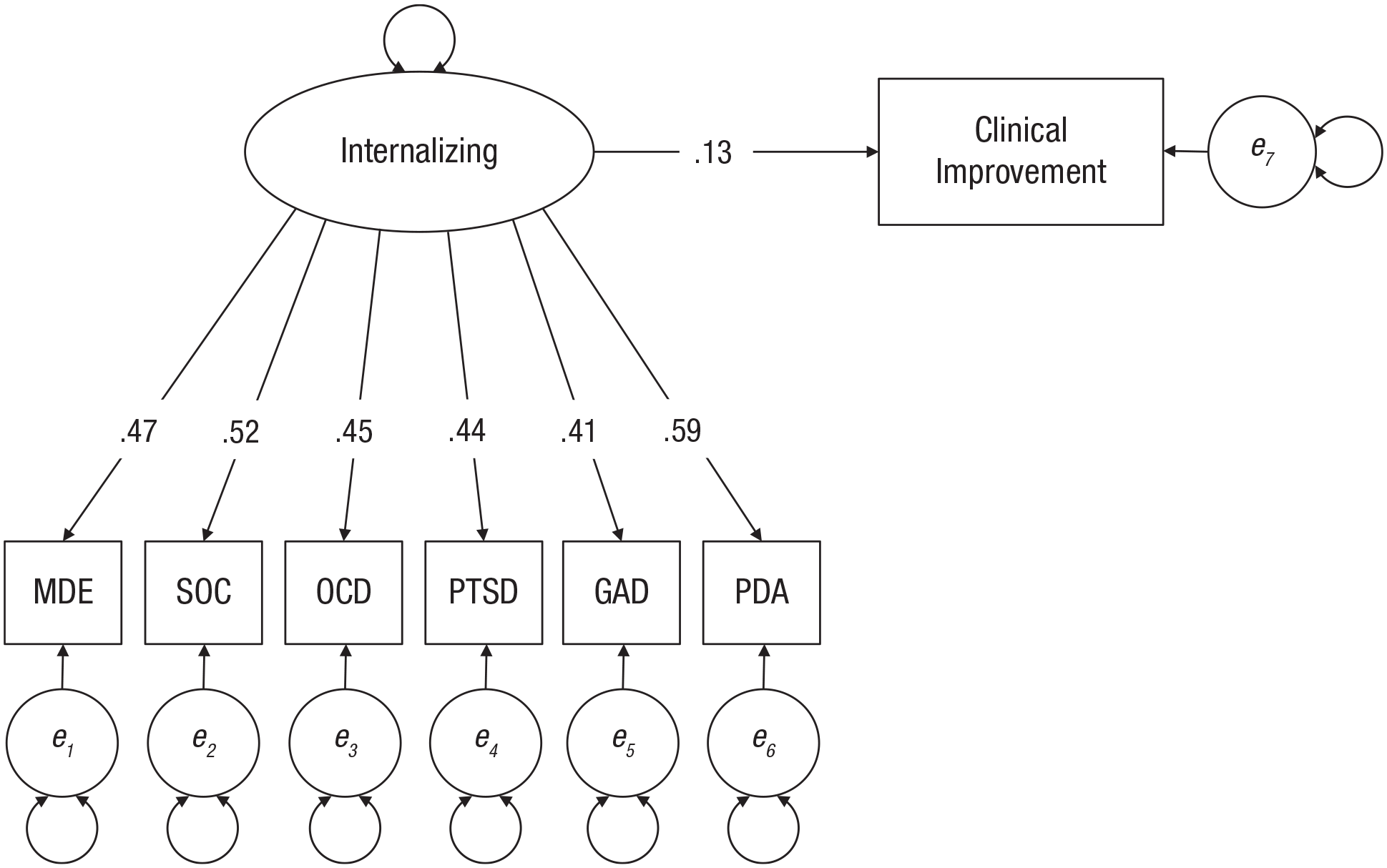
Regression of self-rated clinical improvement on the internalizing factor. All coefficients reflect fully standardized parameter estimates, and all are statistically significantly different from 0 at the .001 α level. Circles represent latent variables, whereas rectangles represent observed variables. Latent variables labeled e1 through e6 are error (residual) terms. Double-headed arrows denote variance estimates, which are omitted here for clarity of presentation. MDE = major depressive episode; SOC = social anxiety disorder; OCD = obsessive compulsive disorder; PTSD = posttraumatic stress disorder; GAD = generalized anxiety disorder; PD/A = panic disorder or agoraphobia or both.
We focus here on the internalizing spectrum, hypothesized to be the substrate of diverse emotional problems (Watson, 2005). Internalizing, like the five other spectra, is configured hierarchically. The broad internalizing spectrum bifurcates into narrower distress and fear subfactors, which distinguish depression and generalized anxiety from panic and the phobias, respectively. Distress and fear can be broken down into syndrome dimensions (e.g., depression, panic; for a discussion of how HiTOP’s empirical syndromes differ from categorical diagnoses, see Kotov et al., 2017). Syndromes are composed of still more homogeneous maladaptive personality traits (e.g., anxiousness, affective lability) and symptom components (e.g., anhedonia, insomnia) at the base of the hierarchical structure.
This model of internalizing problems offers a new method for etiological research. Investigators can examine risk factors’ effects on constructs at varying levels of breadth in the dimensional hierarchy (reviewed in Conway et al., 2019). Recent research has demonstrated that the genetic bases of anxiety and depression map onto the phenotypic architecture of this domain (Waszczuk et al., 2020), and there is growing evidence that neurobiological correlates of emotional complaints are more robustly associated with broad, empirically derived internalizing dimensions compared with categorical syndromes (Latzman, DeYoung, & The HiTOP Neurobiological Foundations Workgroup, 2020). There is strong evidence that significant stressors, such as abuse, discrimination, and ongoing financial trouble, primarily affect risk for anxiety and depression diagnoses indirectly through their influence on higher order internalizing dimensions (Keyes et al., 2012; Rodriguez-Seijas, Stohl, et al., 2015; Snyder, Young, & Hankin, 2019).
Longitudinal studies in community populations have documented dynamic relationships between individual differences in the internalizing domain and clinical outcomes, such as prognosis, disability, and suicidality. In epidemiological data, Kessler et al. (2011) showed that differences on an internalizing factor predicted the time course of anxiety and depression much better than variation in categorical diagnoses (see also Kotov, Perlman, Gámez, & Watson, 2015). Other large-scale studies have consistently found that internalizing and its distress subfactor are strong predictors of suicidal behavior (e.g., Eaton et al., 2013; Sunderland & Slade, 2015). In this same vein, studies in patient groups suggest that transdiagnostic internalizing dimensions, compared with DSM diagnoses, explain at least twice as much variation in psychosocial impairment (Forbush et al., 2017; Waszczuk, Kotov, et al., 2017).
This same hierarchical approach, which has generated new insights into the etiology and correlates of psychopathology, has not yet been applied to understanding the predictors of treatment outcome. What components of anxiety and depression predict who will respond to psychological intervention? We have clues from prior observational studies that broader dimensions tend to be more informative than categorical diagnoses, but none of this research has been in a clinical context.
In the present study, we investigated the prospective effect of a higher order internalizing dimension on treatment outcome in a large, acutely distressed patient sample. We expected that, consistent with the HiTOP model, we could use factor analysis to specify an internalizing factor that would account for the pattern of covariation among patients’ anxiety and depression diagnoses. Such a model parses the internalizing factor, which represents psychopathology shared across all the emotional disorders measured in our sample, from the diagnosis-specific components of each disorder.
It is possible that the transdiagnostic component, diagnosis-specific components, or both could predict improvement in emotional disorder symptoms over the course of treatment. We hypothesized that differences on the empirically derived internalizing dimension would be inversely associated with symptom and functional improvement during an acute psychological intervention. That is, we expected patients high in internalizing to report less clinical improvement, require more intensive care, and endorse more residual anxiety and depressive symptoms at the end of treatment. We predicted that categorical anxiety and depression diagnoses would be minimally related to treatment outcome after accounting for variation on the higher order internalizing dimension.
Method
Participants
Participants were patients admitted to a partial hospital program in New England. Most patients at this clinic present with mood, anxiety, or personality disorders (for more clinical and demographic information about the patient population on a similar sample, see Beard, Millner, et al., 2016). The program provides intensive, short-term treatment (1–3 weeks) aimed at stabilizing acute symptoms. Patients attended the program every weekday (from 9 a.m. to 3 p.m.) and participated in both group and individual psychotherapy. The average length of stay in the program was 11.35 days (SD = 4.47; including weekends and holidays). Each patient was assigned a three-person treatment team that consisted of a clinical team manager (a licensed social worker or psychologist), a psychiatrist (for medication management), and a program therapist (for individual therapy).
All patients attended up to five 50-min group sessions per day. Most of these sessions were based on empirically supported interventions (for details on the treatment approach, see Forgeard, Beard, Kirakosian, & Björgvinsson, 2018). For example, several groups were based on dialectical behavior therapy and covered distress tolerance, emotion regulation, and interpersonal effectiveness. Other therapy modules were based directly on cognitive-behavioral interventions, such as behavioral activation and cognitive restructuring. Still others emphasized mindfulness-based therapies and acceptance and commitment therapy (e.g., clarifying values, practicing mindful acceptance). Finally, several focused on general psychoeducation (e.g., sleep hygiene), life skills and treatment adherence (e.g., vocational counseling, medication management), and recreation and relaxation (e.g., art, yoga). The case manager and patient decided together which group therapy sessions the patient attended each day. Because patients could be admitted to the program on any weekday, the exact sequence of group therapies varied across patients.
Aside from group-based interventions, all patients met with their designated program therapist two to three times per week for individual psychotherapy. The one-on-one therapy was intended to help the patient consolidate the skills introduced in group psychotherapy sessions and to generalize gains to personally relevant life domains. The program therapists were typically advanced clinical psychology PhD students or postdoctoral fellows.
Although all patients participated in psychotherapy, a medication regimen was not required. Nevertheless, medication use, which was managed by a psychiatrist on the treatment team, was nearly universal. According to data from a subset of 1,306 patients admitted to the program between 2015 and 2017, 97% were taking at least one medication with potential psychotropic effects, and 94% were taking a medication classified as an antidepressant, anxiolytic, antipsychotic, mood stabilizer, or stimulant. The average number of medications per patient at admission was 2.7.
The sample for the present analysis was 3,760 patients who were administered a diagnostic interview upon treatment entry. No patients were excluded on the basis of diagnosis. The average age was 34 years (SD = 13.9, range = 18–74 years), and 45% were men. Most patients (96%) were of non-Hispanic ethnic origin; 87% identified as White, 5% identified as Asian, 2% identified as Black/African American, 4% identified as multiracial, and 2% identified as other races.
Measures
Psychological diagnoses
At treatment entry, patients completed the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1998) to diagnose anxiety and mood disorders according to the fourth edition of the DSM (DSM–IV; American Psychiatrist Association, 1994). 1 There is evidence from studies of outpatients with diverse primary diagnoses that mental health professionals can be trained to administer the MINI to achieve adequate interrater and retest reliability (e.g., Lecrubier et al., 1997; Sheehan et al., 1998). In our study, graduate-level clinical trainees—mostly advanced clinical psychology doctoral students—conducted the interviews, and they were trained by experienced clinical psychologists through review of administration manuals, mock interviews, ratings of audio-recorded interviews, and monthly supervision.
The MINI diagnoses analyzed were major depressive episode (MDE), generalized anxiety disorder (GAD), posttraumatic stress disorder (PTSD), social anxiety disorder (SOC), panic disorder (PAN), agoraphobia (AGO), and obsessive compulsive disorder (OCD). Descriptive statistics showed that PAN and AGO were rarely diagnosed without one another (tetrachoric correlation = .88), and we therefore collapsed these conditions into a single variable (labeled PD/A).
Treatment response
Our primary outcome was a self-report version of the Improvement subscale of the Clinical Global Impression Scale (CGI; Guy,1976) administered at discharge. On the CGI, patients rated overall change in symptoms from treatment outset to discharge on a single 7-point scale. The response options were 1 = very much improved, 2 = much improved, 3 = minimally improved, 4 = unchanged, 5 = minimally worse, 6 = much worse, and 7 = very much worse. Lower scores therefore indicate greater perceived improvements. This measure is a common index of treatment progress in clinical research and routine practice (Busner & Targum, 2007). Moreover, patient ratings have mapped on closely to provider judgments and have shown comparable validity coefficients in prior research (e.g., Forkmann et al., 2011).
We also administered the nine-item Patient Health Questionnaire (PHQ-9; Kroenke, Spitzer, & Williams, 2001) and the seven-item Generalized Anxiety Disorder Scale (GAD-7; Spitzer, Kroenke, Williams, & Löwe, 2006) at admission and discharge to assess change in core emotional disorder symptoms. Prior research in this patient population has documented good psychometric properties for both instruments (e.g., Beard & Björgvinsson, 2014).
Finally, we monitored whether patients moved from partial hospitalization to inpatient care during the treatment period. Patients were admitted to an inpatient unit if there was significant functional deterioration or evidence that they were putting themselves or others in danger. Thus, we conceptualized inpatient admission as an index of treatment nonresponse (see Beard, Hearon, et al., 2016).
Procedure
Data were collected between 2010 and 2017 at a partial hospital program in New England. The measures described above were administered as part of routine clinical monitoring. The study was approved as an exempt protocol—because it used an existing, deidentified data set—by the hospital’s ethics review board.
Data analysis
We first tested the fit of confirmatory factor analysis (CFA) models of the comorbidity patterns among emotional disorder diagnoses. We expected that a one-factor model, in which an internalizing factor explains shared variation across anxiety and depression, would fit the data well. We also tested a two-factor model including correlated distress and fear factors that has fit well in some, but not all, samples (Krueger & Markon, 2006). The distress factor was defined by MDE, GAD, and PTSD, whereas fear was defined by SOC, PD/A, and OCD.
Using a structural equation modeling framework, we then regressed the treatment response variables onto the factor from the better fitting (one-factor) CFA model. We used a two-tailed α value of .05 for the regression of our primary outcome, CGI scores, on the internalizing factor. For all other effects, we applied a Bonferroni correction resulting in an α value of .0019 (.05 / 27 secondary tests).
In separate models for the PHQ-9 and GAD-7, we regressed symptom scores at treatment discharge on the internalizing factor and the corresponding symptom score at treatment entry. This multiple regression therefore adjusted for symptom continuity when estimating the longitudinal effect of internalizing on symptom outcomes. To examine internalizing’s effect on the probability of transitioning to more intense inpatient care, we regressed inpatient admission (0 = no, 1 = yes) on the internalizing factor.
To examine incremental effects of categorical diagnoses on treatment outcomes, we modeled the indicator residuals as latent dimensions that were orthogonal to the internalizing factor. These residual dimensions represent the parts of diagnoses that were unshared with other conditions, whereas the internalizing factor represents the shared variation across all conditions. Separately for each of the outcomes, we regressed outcome scores on the six residual dimensions to test for diagnoses’ effects independent of the internalizing dimension.
Before data analysis, we performed power simulations to decide whether we had a sufficient sample to detect the primary effect. We expected a standardized regression effect of the internalizing factor on CGI of −.20. The Monte Carlo study indicated that a sample as small as 600 was large enough to detect this effect size with power > .90 (and a two-tailed α value of .05). We used the entire available sample to maximize parameter estimates’ precision.
We report analyses performed in Mplus (Version 8; Muthén & Muthén, 2017) using the WLSMV estimator, which is the Mplus default for models involving categorical dependent variables. CGI and inpatient admission status, along with all factor indicators, were treated as categorical outcomes. CFA model fit was judged to be adequate if the root mean square of approximation (RMSEA) was 0.08 or lower and the comparative fit index (CFI) and Tucker-Lewis index (TLI) were .90 or higher (e.g., Hu & Bentler, 1999; Marsh, Hau, & Wen, 2004).
We posted all data and analysis code (along with a preregistration document) at https://osf.io/b5yw7/. For reproducibility, we supplemented our Mplus input files with code needed to perform all data cleaning and analysis in the lavaan package (Version 0.6-5; Rosseel, 2012) in the R software environment (Version 3.6.1; R Core Team, 2019). Although the overall pattern of results was equivalent, parameter estimates differed somewhat across software programs because of different estimation techniques and methods for handling missing data. In Mplus Version 8, the weighted least squares estimator involves pairwise deletion such that model-implied correlations are based on the maximum number of cases with data for that pair of variables (Muthén & Muthén, 2017). In contrast, lavaan performs listwise deletion during weighted least squares estimation (Rosseel, 2012).
Results
Descriptive statistics
Table 1 presents diagnostic prevalence rates and tetrachoric correlations. MDE was the most common condition (60%), followed by anxiety disorders (19%–34%), PTSD (12%), and OCD (12%). Diagnostic correlations were small but consistent (median tetrachoric r = .23, range = .13–.34), and all were statistically significant at the .001 α level.
Descriptive Statistics for Diagnoses and Treatment Response Variables

Note: All correlations were computed using pairwise deletion. Correlations among diagnostic categories are tetrachoric correlations. Time 1 = treatment entry; Time 2 = treatment discharge; CGI = Clinical Global Impression-Improvement Subscale (Guy, 1976); PHQ-9 = Patient Health Questionnaire (Kroenke, Spitzer, & Williams, 2001); GAD-7 = Generalized Anxiety Disorder Scale (Spitzer, Kroenke, Williams, & Löwe, 2006); N = sample size.
There is some missingness for each diagnosis because interview time constraints sometimes prevented assessment of the full roster of diagnoses.
Table 1 also shows the descriptive statistics for the treatment response variables and their correlations with the observed diagnostic categories. Self-reported global improvement, as measured by the posttreatment CGI, was approximately much improved, on average (M = 2.12, SD = 0.82). Consistent with the CGI result, there was evidence of substantial improvement in GAD-7 anxiety symptoms—t(2508) = 42.21, p < .001, Cohen’s d = −0.86—and PHQ-9 depressive symptoms—t(1691) = 36.05, p < .001, Cohen’s d = −0.90—from the beginning to end of treatment. Finally, 210 cases (7% of the sample) were admitted to inpatient care during the treatment period.
The structure of internalizing
The one-factor model fit the data well, χ2(9) = 36.70, CFI = .97, TLI = .94, RMSEA = 0.029. All factor loadings were substantial (fully standardized loading range = 0.41–0.61) and statistically significant at the .001 level. Goodness-of-fit indices were also in an acceptable range for the two-factor model, χ2(8) = 31.20, CFI = .97, TLI = .94, RMSEA = 0.028. However, the very large factor correlation (r = .86) indicated to us that the distress and fear factors had limited discriminant validity in this sample, and we therefore rejected the two-factor model. For the parameter estimates for the one- and two-factor models, see Table S1 in the Supplemental Material available online.
Predicting treatment outcome
The path diagram in Figure 1 illustrates our primary analysis, Table 2 presents regression parameter estimates across structural regression models of all four outcomes, and Table S2 in the Supplemental Material reports correlations between the internalizing factor and treatment response variables.
Regressions of Treatment Outcomes on Dimensions of Anxiety and Depression
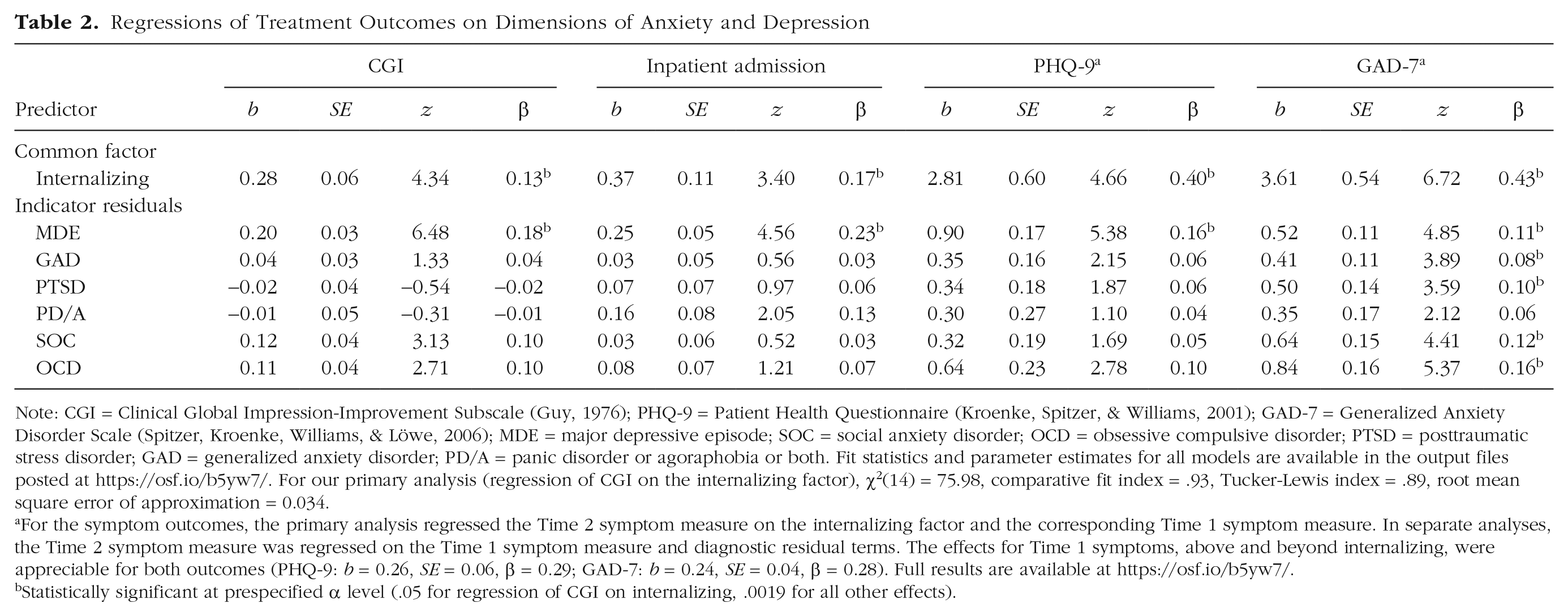
Note: CGI = Clinical Global Impression-Improvement Subscale (Guy, 1976); PHQ-9 = Patient Health Questionnaire (Kroenke, Spitzer, & Williams, 2001); GAD-7 = Generalized Anxiety Disorder Scale (Spitzer, Kroenke, Williams, & Löwe, 2006); MDE = major depressive episode; SOC = social anxiety disorder; OCD = obsessive compulsive disorder; PTSD = posttraumatic stress disorder; GAD = generalized anxiety disorder; PD/A = panic disorder or agoraphobia or both. Fit statistics and parameter estimates for all models are available in the output files posted at https://osf.io/b5yw7/. For our primary analysis (regression of CGI on the internalizing factor), χ2(14) = 75.98, comparative fit index = .93, Tucker-Lewis index = .89, root mean square error of approximation = 0.034.
For the symptom outcomes, the primary analysis regressed the Time 2 symptom measure on the internalizing factor and the corresponding Time 1 symptom measure. In separate analyses, the Time 2 symptom measure was regressed on the Time 1 symptom measure and diagnostic residual terms. The effects for Time 1 symptoms, above and beyond internalizing, were appreciable for both outcomes (PHQ-9: b = 0.26, SE = 0.06, β = 0.29; GAD-7: b = 0.24, SE = 0.04, β = 0.28). Full results are available at https://osf.io/b5yw7/.
Statistically significant at prespecified α level (.05 for regression of CGI on internalizing, .0019 for all other effects).
Global improvement
Internalizing had a statistically significant effect on CGI scores at discharge (b = 0.28, SE = 0.06, p < .001, standardized effect = .13). The positive sign for this coefficient implies that higher internalizing levels predicted higher scores on the CGI (less self-rated improvement) at the end of treatment. Table 2 shows that diagnostic residual effects, except for MDE (standardized effect = .18), were not statistically significant. Higher standing on the MDE dimension was associated with poorer global improvement independent of the internalizing effect.
Inpatient admission
Internalizing was positively asso-ciated with the probability of inpatient hospitalization (b = 0.37, SE = 0.11, p < .001, standardized effect = .17). Besides MDE (standardized effect = .23), no categorical diagnosis had a significant incremental effect. To compute a more intuitive effect size, we also regressed the latent dimensions from the common factor model on the inpatient admission variable (i.e., reversed the direction of the structural regressions). This analysis, summarized in Table S3 in the Supplemental Material, yielded the difference in location on the internalizing dimension across inpatient status (yes vs. no) in standard units. The results indicated that patients who stepped up to inpatient care were one third of a standard deviation higher on the internalizing dimension and one half of a standard deviation higher on the unique dimension of MDE. Effects for all other diagnoses were considerably smaller.
Emotional problems
Higher internalizing levels predicted more anxiety and depression symptoms at treatment discharge, adjusting for baseline symptoms. These effects were robust (standardized effects = .40 and .43), compared with those observed for the CGI and inpatient admission, despite the adjustment for sizeable symptom continuity from the beginning to end of intervention (for autocorrelations, see Table S4 in the Supplemental Material). Independent of internalizing, there was a significant effect of MDE on both PHQ-9 and GAD-7 scores (standardized effects = .16 and .11, respectively). All diagnoses except panic disorder had statistically significant, incremental effects on GAD-7, but the effect sizes were all about one fourth as large as that of internalizing (standardized effect range = .08–.16). 2
Discussion
Our analysis in a large patient sample indicated that patients’ anxiety and depression diagnoses reflected a mixture of (a) a broad, transdiagnostic internalizing dimension and (b) comparatively narrow, diagnosis-specific dimensions. The internalizing spectrum was a statistically significant, prospective predictor of acute treatment outcome, whereas diagnosis-specific dimensions—except major depression—tended to make relatively small and inconsistent incremental contributions.
The internalizing dimension reliably predicted treatment response across outcome measures. Elevated internalizing levels at treatment outset were associated, albeit modestly in some cases, with lower self-rated global improvement, higher risk of requiring inpatient care, and sustained anxiety and depressive symptoms over the course of partial hospitalization treatment. This pattern of associations indicates that greater general severity of internalizing problems—even in an acutely distressed population in which individual differences are likely to be relatively constrained—portend poorer outcomes for psychological interventions.
The internalizing factor’s effects suggest that transdiagnostic phenotypes have clinical utility. For more than a century, the dominant tradition in clinical research has been to frame prediction around categorical diagnostic entities. From that perspective, each diagnostic category has a unique etiology, prognosis, and indicated treatment. This result, and others like it, points to an alternative conceptualization: The common elements of empirically related conditions can be the focus of case conceptualization and clinical decision-making (Ruggero et al., 2019).
Anxiety-based diagnoses did not consistently improve prediction of treatment outcomes over and above the internalizing dimension. The median standardized effect size across 20 regressions was .06. Thus, whereas the core aspects of anxiety and depression—reflected in the internalizing factor—modulated treatment success, the diagnosis-specific features of DSM–IV anxiety disorders did not. In other words, any observed connection between the baseline anxiety disorder diagnostic profile and progress through treatment was accounted for by variation on the underlying internalizing dimension. This interpretation mirrors conclusions from a growing body of research on the clinical correlates of emotional disorders. Data across several large-scale studies generally have shown small or nonexistent direct paths from categorical diagnoses to important outcomes such as suicide risk and psychosocial impairment after adjusting for the diagnoses’ shared variance (reviewed in Conway et al., 2019).
MDE behaved differently from the anxiety-based diagnoses. For our primary outcome, the effect for the diagnosis-specific component of MDE (i.e., the part that was unshared with other emotional disorders) was comparable with that for internalizing (i.e., the variation in MDE that was common to all emotional disorders). This pattern implies that higher- and lower order dimensions of depression had independent prognostic value in this data set.
In prior research, categorical representations of depression typically have not demonstrated strong effects on clinical outcomes over and above higher order internalizing dimensions. However, some independent effects for depression have been observed. For example, one longitudinal study found that depression diagnoses predicted future stressful events—a phenomenon known as stress generation—even after controlling for the internalizing factor (Conway, Hammen, & Brennan, 2012). More generally, structural research has shown that there are many meaningful subdimensions of depression and other emotional problems that likely play a role in predicting clinical outcome (e.g., Waszczuk, Kotov, et al., 2017).
Clinical implications
We believe these results call attention to ways that clinical assessment routines might benefit from incorporating a dimensional view of emotional disorders. For one thing, the validity of the internalizing dimension reinforces the idea that emotional disorders can be conceptualized and assessed along continua of severity, as opposed to discrete categories. There is ample evidence that people differ in anxiety and depression in terms of degree, not kind (Haslam, McGrath, Viechtbauer, & Kuppens, 2020). Assessing the full spectrum of individual differences on these phenotypes captures the maximum amount of clinical information, which is known to improve reliability and predictive utility, relative to the categorical model of anxiety and depressive disorders (Markon, Chmielewski, & Miller, 2011).
This approach has been successful in some areas of contemporary medical diagnosis. Characteristics such as weight and blood pressure are best conceptualized as continua, but they can be dichotomized according to empirical guidelines when binary clinical decisions, such as whether to follow up or administer medication, are required. In clinical psychology, we rely on dimensional assessment to characterize cognitive ability. Continuous scores from intelligence tests are integrated with psychosocial assessments to make categorical determinations regarding diagnosis and service delivery (American Psychiatric Association, 2013). Our study joins many others in pointing to the utility of dimensional perspectives in emotional-disorder assessment.
A large body of research shows that internalizing dimensions are structured hierarchically (Watson, 2005). Multiple levels of internalizing problems, ranging from very broad to very specific symptom dimensions, are likely to have clinical utility. In the present study, for instance, both the broad internalizing factor and more specific aspects of major depression were prospectively associated with clinical outcome. Thus, these different strata of the internalizing domain are complementary ways of approaching anxiety and depression and equally valid assessment targets. This framework gives practitioners some flexibility regarding which level of the hierarchy to focus on, depending on whether high-resolution or low-resolution information is a better fit to the clinical goal at hand (see Mullins-Sweatt et al., 2020; Ruggero et al., 2019).
There are in fact ready-to-use measures of internalizing problems that were created with the dimensional and hierarchical structure of this domain in mind (see Kotov et al., 2017). The Inventory of Depression and Anxiety Symptoms (IDAS; Watson et al., 2007) is a popular option. It was factor analytically derived to tap into a broad dysphoria dimension, analogous to internalizing factor in the present study, that cuts across all expressions of anxiety and depression, along with narrower facets of the internalizing domain that reflect fine-grain symptom dimensions such as obsessions, traumatic intrusions, and panic. Expanded self-report and interview versions of this instrument make it potentially relevant for diverse clinical applications (Kotov et al., 2015; Watson et al., 2012). The IDAS is associated with a large normative database that fosters scale-score interpretation and clinical decision-making. For instance, empirical cutoffs have been suggested to mark ranges of scores consistent with clinically significant anxiety and depressive problems (Stasik-O’Brien et al., 2019).
Limitations
A number of study limitations are important to point out. First, this was not a treatment trial. Patients encountered various combinations of group psychotherapy interventions and medications during partial hospitalization. We did not systematically control the style of patients’ treatment. Thus, this study represents a naturalistic, as opposed to experimental, examination of patients’ changes in response to intervention. We judge the variation in interventions across patients in the same hospital program to be minor, but it may have had some impact on clinical outcome.
Second, the roster of outcomes examined here reflected mostly “transdiagnostic” individual differences—those that were not tied conceptually to any one narrow diagnostic construct. (One could make a case, however, that PHQ-9 and GAD-7 scores are intended to reflect MDE and GAD severity, in particular.) This selection may have made it more difficult to detect specific diagnostic effects after adjusting for the internalizing dimension.
The internalizing factor was, by definition, transdiagnostic and therefore possibly best suited to predict broad outcomes such as global improvement and inpatient hospitalization, which almost certainly reflect pathology common to multiple conditions. If instead the dependent variables had been oriented around panic attacks, social engagement, avoidance of feared objects, and so on, then any predictive value of specific diagnoses might have been more apparent. This nuance is akin to the bandwidth-fidelity dilemma in personality psychology (Cronbach & Gleser, 1957).
Our conclusions should therefore be interpreted with this caveat in mind. Our choice of outcomes reflects a constraint on the study’s generalizability to the extent that examination of narrower outcomes—particularly those linked to the specific symptom sets embodied by DSM–IV diagnoses—might lead to a more prominent predictive role for various categorical diagnoses above and beyond a higher order internalizing dimension. We believe this possibility merits focused investigation in future clinical research.
Third, and along these same lines, we caution that the diagnostic composition of this sample could limit the degree to which our observed effects generalize to other populations. Many of the diagnoses were much more prevalent in this group than in the community or even ordinary outpatient practice. MDE, in particular, was very common, and it is possible that its prevalence was related to the predictive effects observed for the residual component of MDE. 3 More simulation and meta-analytic work is needed to parse the influence of diagnostic prevalence, diagnostic correlations, and sampling in general (e.g., inpatient vs. outpatient populations) on the structure and utility of dimensional models of psychopathology. We believe that the effects of the internalizing spectrum and its constituent parts on various clinical outcomes could certainly depend partly on the population under study.
Conclusion
Quantitative, as opposed to categorical, features of anxiety and depression might have superior clinical utility. In this partial hospitalization sample, a broad internalizing dimension was prospectively associated with various clinical outcomes, such as symptom improvement and need for more intensive care. Narrower facets of emotional problems also appeared to have predictive utility, reinforcing the value of a hierarchical perspective on the internalizing domain.
Supplemental Material
sj-pdf-1-cpx-10.1177_2167702620959291 – Supplemental material for A Higher Order Internalizing Dimension Predicts Response to Partial Hospitalization Treatment
Supplemental material, sj-pdf-1-cpx-10.1177_2167702620959291 for A Higher Order Internalizing Dimension Predicts Response to Partial Hospitalization Treatment by Christopher C. Conway, Ivar Snorrason, Courtney Beard, Marie Forgeard, Kristy Cuthbert and Thröstur Björgvinsson in Clinical Psychological Science
Footnotes
Transparency
Action Editor: Kenneth J. Sher
Editor: Kenneth J. Sher
Author Contributions
C. C. Conway developed the study concept. C. Beard, M. Forgeard, and T. Björgvinsson contributed to the study design. C. C. Conway and I. Snorrason performed the data analysis and interpretation. C. C .Conway and I. Snorrason drafted the manuscript, and all of the authors provided critical revisions. All of the authors approved the final manuscript for submission.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.