
Abstract
In this article, we examine how symptoms are conceptualized in theories of psychopathology. We identify five questions that need to be asked about symptoms, including what kind of constructs they are, how we should describe them, and what causal explanations they support. We then examine how three different theoretical frameworks address these questions: the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders, the symptom-network-modeling approach, and the Cambridge model of symptom formation. We show that the assumptions these frameworks make affect the kinds of theoretical models they support and the research approaches they advocate. When symptoms are viewed as empirical observations, the focus of inquiry is directed elsewhere. However, when symptoms are understood as complex constructs in their own right, that are themselves built on certain theoretical assumptions, then understanding them becomes crucial to theoretical progress. We conclude by calling for greater focus on research that unpacks the constructs underlying symptoms.
In medicine, the process of discovering new diseases typically begins with the observation of signs and symptoms. These phenomena provide indicators as to the possible etiology of the disease—or at least pointers as to how one might go about gathering relevant evidence (Hucklenbroich, 2017; Räisänen, Bekkers, Boddington, Sarangi, & Clarke, 2006; Rovetto & Mizoguchi, 2015; Wilshire & Ward, 2020). In contrast, in the field of mental illness, the presenting problems are usually self-reported symptoms, many of which are quite nonspecific. Consequently, they provide much less guidance in themselves as to how researchers might go about investigating their causes.
One approach to this problem is organize symptoms into theoretically meaningful clusters or syndromes, which then become the primary targets of investigation. For example, in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association [APA], 2013), the syndrome of major depressive disorder (MDD) is diagnosed when the person presents with a minimum number of specified symptoms that include depressed mood, anhedonia, sleep disturbances, appetite disturbances, suicidal thoughts, fatigue, poor concentration, psychomotor retardation, and low self-esteem (see also ICD-10, World Health Organization, 1992). However, in the field of mental illness, symptoms do not organize themselves into neat clusters with distinct boundaries. Although some symptoms associated with common mental health problems cluster together in meaningful ways (e.g., low mood is more likely to be accompanied by anhedonia than by worrying thoughts; see Beard et al., 2016), others are observed across a wide range of contexts (e.g., sleep disturbance, concentration problems; Cramer, Waldorp, Van Der Maas, & Borsboom, 2010; see also Brodbeck et al., 2014). So the demarcation points between syndromes are often as much theoretical as they are empirical. In addition, in commonly used classification schemes, many diagnostic entities are polythetic—individuals need meet only a subset of criteria to qualify—which allows for considerable variability among individuals with the same diagnosis. Therefore, one cannot always assume a single common underlying cause (Olbert, Gala, & Tupler, 2014; Park et al., 2017; for discussion, see Tabb, 2015).
An alternative strategy is to focus on the symptoms themselves, irrespective of the broader syndrome diagnosis. Examples of this strategy include behaviorist approaches to certain types of problematic behaviors (e.g., specific phobias) in which the symptom is treated as the problem in its own right (see e.g., Choy, Fyer, & Lipsitz, 2007). Other examples include research that focuses on the patterns of co-occurrence among different types of symptoms (Borsboom, 2017; Borsboom & Cramer, 2013; Borsboom, Cramer, & Kalis, 2019) or that focuses on describing and explaining specific symptoms (e.g., auditory hallucinations: Corlett et al., 2019; Ford et al., 2014; Seal, Aleman, & McGuire, 2004; psychomotor retardation: Destoop, De Bruijn, Hulstijn, & Sabbe, 2009; body image disturbance: Gadsby, 2017; Gadsby & Williams, 2018; anhedonia: Gorwood, 2008; Treadway & Zald, 2011).
Regardless of whether one treats symptoms as diagnostic pointers or as sources of information in their own right, it is often assumed that the symptoms themselves are largely unproblematic concepts. However, even a cursory examination of the kinds of symptoms that are featured in common diagnostic systems reveals that many are far from simple constructs. For example, the DSM-5 (APA, 2013) includes symptoms such as body image disturbance, low self-esteem, and identity disturbance, symptoms whose conceptualization would seem to rest on a number of complex theoretical assumptions and/or normative judgments. In this article, we argue that more attention needs to be paid to describing symptoms and to understanding what kinds of constructs they are, how they come to people’s attention, and what sorts of factors influence them. The answers to these questions form the very foundation of research into psychopathology.
We begin by identifying and describing the kinds of questions that need to be asked about the nature of symptoms and their relation to mental illness and the implicit assumptions that different research approaches make concerning these questions. We then use this framework to describe how symptoms are viewed in three very different conceptual approaches to psychopathology: (a) the DSM-5 (APA, 2013), (b) symptom network modeling approaches (SNWM; Borsboom, 2017), and (c) the Cambridge model of symptom formation (Marková & Berrios, 2009). We also briefly consider whether the recent Research Domain Criteria framework (RDoC; Insel et al., 2010; Morris & Cuthbert, 2012) speaks to any of these issues. On the basis of our analysis, we argue that there is a need to construct richer descriptions of symptoms.
One point to keep in mind is that conceptualizations of symptoms will vary depending on the purpose for which they are used. One view, which is implicit in syndrome-based diagnostic frameworks, is that symptoms act primarily as heuristics for arriving at a diagnosis—and only secondarily as problems that may need addressing in their own right. Consequently, their value will depend on how effective they are as diagnostic indicators—for example, how stable they are across time, how consistently and reliably they can be identified by different clinicians, and how sensitive and specific they are at detecting cases likely to have the diagnosis and at distinguishing them from individuals with other diagnoses. Symptoms that meet some or all of these requirements may be attributed a special status as pathognomonic symptoms (or in the context of psychosis, first-rank symptoms; Schneider, 1959). Within this type of framework, research targeted at describing and explaining individual symptoms is not seen as a priority because symptoms are merely pointers to the underlying problem, in which most of the important explanatory information resides. Approaches that view symptoms as targets of investigation in their own right—irrespective of the person’s broader diagnosis—are likely to place more emphasis on their conceptual characteristics. We return to this issue at various points in our discussion below.
Defining the term symptom can itself be troublesome because it is used in a wide variety of different ways. In some contexts, it is applied only to phenomena that have already been linked to a known etiological mechanism (e.g., “X is a symptom of Y”), whereas in others, it is used without respect to diagnostic value or etiological status (e.g., “The patient presented with a range of unusual symptoms”). Furthermore, some uses restrict the term to self-reported complaints or experiences, whereas others extend it to self-reported behaviors and even behaviors reported by others. We use a relatively broad working definition: We define a symptom in the context of psychopathology as an enduring or recurring subjective experience, or behavior pattern, that is considered to be indicative of a mental health problem. This definition encompasses both subjective experiences and behavior patterns—irrespective of whether they are self-reported or observed by a third person, such as a family member or clinician. It also encompasses phenomena that are not interpreted by the person as distressing but are nonetheless indicative of a wider problem affecting their functioning (e.g., delusions of grandeur). For practical reasons, we exclude from our analysis observations that are obtainable only within a laboratory context (e.g., patterns of behavior in paradigms such as reversal learning or delay-discounting, measures of accuracy or speed on specific tasks, or neurobiological measures such as skin conductance or hemodynamic responses).
Symptoms in Psychopathology: What Questions Need to Be Asked?
To understand what symptoms can—and cannot—tell us about mental disorders, one must first examine the assumptions that are made about these constructs under different approaches. There are four broad groups of issues that an approach might speak to. First, each approach is likely to make some implicit assumptions about the metaphysics of symptoms—that is, what kinds of constructs they are (Are they seen as akin to empirical observations or as more abstract theoretical constructs?). Second, it may take an explicit or implicit position on epistemological issues—that is, about the kinds of information that should be gathered to enrich understanding of the nature and causes of symptoms. Third, it may take a position on methodological issues—about how to best go about gathering knowledge about symptoms. And finally, it might speak to operational issues—about the best way to determine whether a symptom is present or absent in a particular instance. In this article, we focus on metaphysical, epistemological, and methodological issues. We do not address the issue of how different schemes actually operationalize a symptom—that is, what criteria they recommend for determining whether a symptom is present in a specific case and whether these criteria have adequate sensitivity and specificity. These kinds of questions cannot be answered until the underlying construct has been fully fleshed out and also some form of well-validated measure has been developed to use as a “benchmark” for cross-validation.
Drawing on the above lines of inquiry, it is possible to identify five categories of questions that may be asked about how a particular approach views symptoms, which are summarized in Table 1. The first question concerns the process by which symptoms come to clinical or research attention: What kinds of contextual and individual factors are seen as important in shaping whether and how a symptom is reported? The second question concerns the degree to which symptoms should be seen as concrete, empirical entities or as abstract and dependent on theory. The third question concerns how much importance should be placed on developing good descriptive models of individual symptoms, what kinds of descriptions would be most valuable (phenomenological, behavioral, neurophysiological, or some combination of these), and what types of methodologies should be prioritized for gathering relevant data. The fourth question concerns how the causal relationships among different co-occurring symptoms should be conceptualized, and also the relationship between symptoms and mental illness more generally. The answers to these four questions will then help us to address the fifth and final question: What role should symptoms play in furthering understanding of psychiatric disorders? We expand on each question below.
Questions Concerning the Nature of Symptoms and Their Role in Understanding Mental Illness
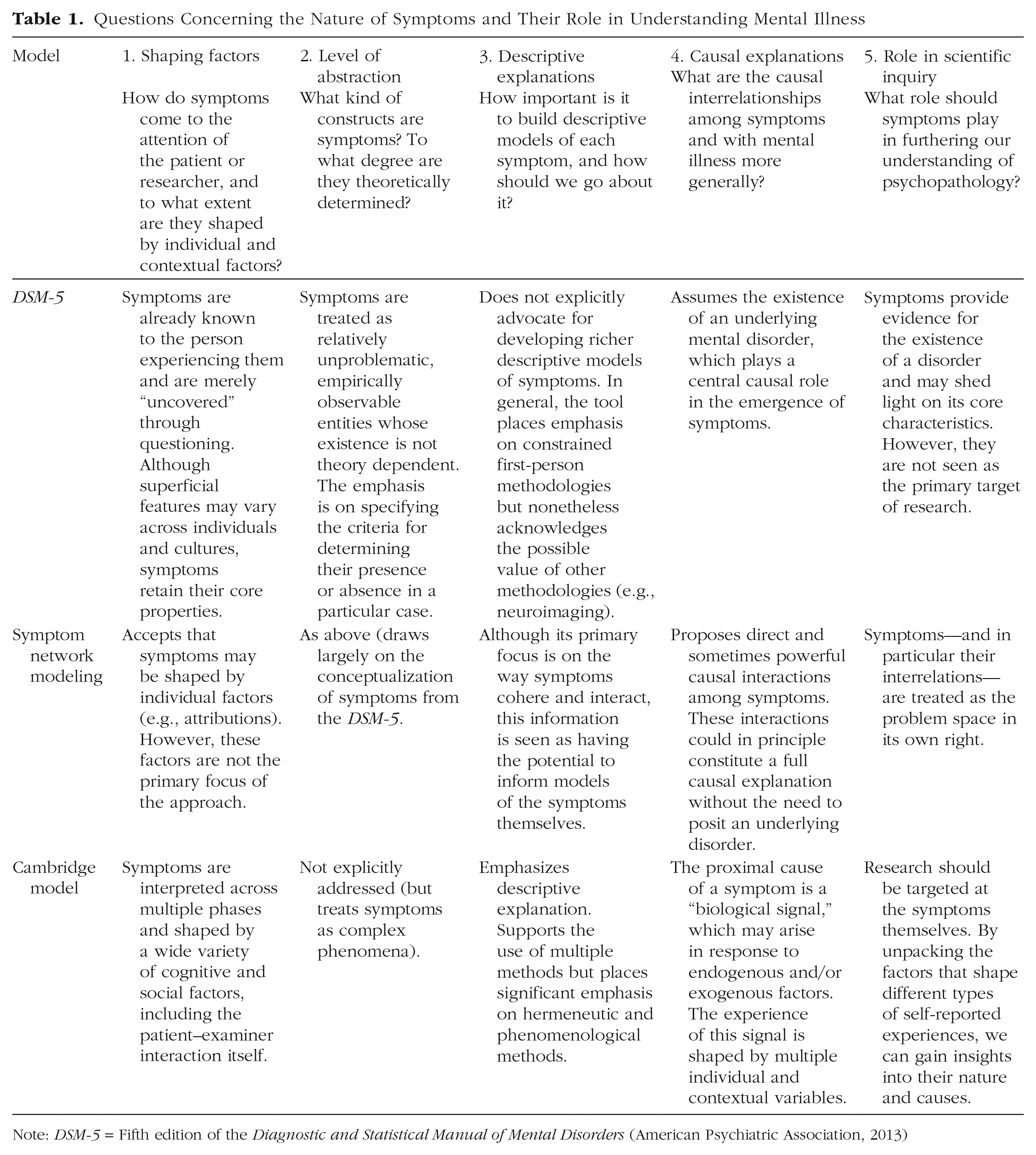
Note: DSM-5 = Fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 2013)
Shaping factors: How do symptoms come to the attention of the patient or researcher, and to what extent are they shaped by individual and contextual factors?
In the mental health domain, the experiences and behavioral patterns that constitute symptoms are usually reported by the patient during a structured clinical interview or through formal self-report tools. There are a number of variables that could potentially shape what the patient reports. In face-to-face questioning settings, this includes the nature of the questions themselves (which will be determined to a large extent by the interviewer’s theoretical framework and working clinical hypotheses) and also the nature of the doctor-patient relationship (for discussion, see Jutel, 2014; Parmley, 2006).
In formal self-report instruments, the questions are prespecified, but nevertheless, a number of theoretical as well as empirical considerations could potentially shape which items are included in a scale. In addition, a person’s response to an item could be shaped by the specific framing of the questions (French & Sutton, 2010; Johnston, 1999; Schwarz, 1999; Sharpe & Gilbert, 1998; Shrout et al., 2018). A third possible factor that could shape individuals’ reports in both face-to-face and written report contexts is retrospective recall bias, which may be influenced by variables both external and internal to the interview or questionnaire (Ben-Zeev & Young, 2010; Schwarz, 2007).
Different approaches may take different views about the strength of influence of these types of factors. Some approaches may assume that the method by which symptom reports are elicited has only minimal impact on what is reported. These approaches assume that most self-reported phenomena are already known to the patient in some sense and are merely uncovered by the examiner. A contrasting view is that they are heavily influenced by the characteristics of the examination context and methods.
Another issue on which approaches may vary concerns the extent to which symptom reports are shaped by the individual’s own beliefs, attitudes, and expectations. Some approaches may view symptom reports as relatively stable and invariant across individuals, to the extent that they can be treated as reliable and consistent indicators of the nature of the underlying problem. Other approaches may view these reports as complex and strongly overlaid by individual cognitive and other characteristics. According to the second view, these phenomena need to be carefully examined within the context of the individual before they can be fully clinically understood.
Symptoms that are based on observations by a third party—such as clinician observations, clinician ratings on formal behavioral rating schemes (e.g., Åsberg, Montgomery, Perris, Schalling, & Sedvall, 1978; Hamilton, 1967; Kay, Fiszbein, & Opler, 1987; Thompson et al., 2010), and formal or informal reports of family members, teachers, or law enforcement authorities—are not subject to the same interpretative and retrospective recall biases that may be at play in first-person methods. However, they may be associated with their own potential shaping factors, which include the clinician’s theoretical framework and working clinical hypothesis (in the case of clinician ratings), the perspectives and values of the observer (in the case of family, teacher, and law enforcement reports), and the manner in which the third-party information is elicited (e.g., the specific items included in or wording of the rating tool). In addition, clinician ratings capture a single time point, which protects against recall bias but, on the other hand, does not speak to the frequency or persistence of the problem.
Level of abstraction: What kind of constructs are symptoms?
Some concepts possess a relatively stable structure across time and across different perspectives (e.g., dogs, people), whereas others are more dependent on the theoretical, social, and/or cultural perspectives of the user (e.g., success, virtue, and justice). In some approaches in psychopathology, symptoms may be viewed as similar to the former type of construct—that is, relatively “shallow” and existing relatively independently of the clinicians’ or researchers’ particular theoretical framework. Others may view them as more complex abstractions that cannot be separated from the conceptual framework in which they are embedded. According to this latter perspective, the ways in which symptoms are conceptualized and measured would be expected to evolve along with the theories in which they are embedded.
Descriptive explanations: How important is it to build descriptive models of each symptom, and how should one go about it?
Some researchers might argue that before one can develop an etiological explanation for a particular symptom (i.e., a representation of the processes causing the phenomenon of interest), one first needs to develop a rich explanation of what constitutes the symptom (for a discussion of the distinction, see Kaiser & Krickel, 2016). Descriptive explanations of symptoms often focus on a particular level of analysis. For example, it is possible to describe persistent, clinically significant sad mood in terms of its cognitive features, which have been reported to include biases favoring negative stimuli, negatively valenced autobiographical memories, and negative self-evaluations (e.g., Clasen, Wells, Ellis, & Beevers, 2013; Vrijsen, Van Oostrom, Isaac, Becker, & Speckens, 2014). Conversely, an explicit goal of some approaches is to develop descriptions at multiple levels of analysis (e.g., the RDoC; Insel et al., 2010; Morris & Cuthbert, 2012). For example, the characteristics of sad mood can be described at a physiological level (e.g., cortisol dysfunction), a neural level (e.g., heightened amygdala responsivity to sad stimuli), a psychological level (e.g., schema bias), a phenomenological level (e.g., existential feeling), and a behavioral level (e.g., withdrawal; see, e.g., Treadway & Zald, 2011; Ward & Clack, 2019).
A related issue concerns the types of methodologies that are most valued for gathering information. If the researcher’s goal is to describe a symptom at the phenomenological level, they might place particular emphasis on unconstrained first-person methods, such as qualitative analyses of patients’ narratives. If it is to provide a psychological-level description, they may emphasize more constrained first-person methods (e.g., structured interviews, self-report instruments) and observational methods, including those based on laboratory-type settings (e.g., behavior under different reinforcement schedules or performance on specific tasks). Descriptions that target the neurobiological level are likely to value methods that measure aspects of autonomic or brain-related activity, such as skin-conductance responses, electroencephalograms/evoked potentials, and functional MRI (fMRI). And finally, approaches that explicitly endorse multiple-level descriptive explanations are likely to embrace a wide range of these methodologies.
Causal explanations: What are the causal relationships that govern symptoms and their underpinnings?
An etiological explanation identifies a set of causal processes that are hypothesized to result in a subsequent downstream effect. That is, it stipulates a specific direction of causation. Clearly, etiological explanations are an important goal of psychopathology. If the causes of various distressing experiences and behaviors can be identified, clinicians may be better equipped to ameliorate them. When considering etiology, it is important to recognize that there will not necessarily be a one-to-one relationship between symptoms and their respective causes. A given symptom could in principle arise from a number of distinctly different sets of causes (equifinality). For example, social avoidance could arise as a consequence of an intense fear of negative evaluation, or a delusion that one is being persecuted, or an obsessive compulsive disorder that manifests in an extreme fear of contamination. Conversely, the same cause may manifest in a variety of different symptoms across individuals (multifinality). For example, problems in emotional self-regulation could potentially manifest in self-harming, gambling, substance abuse, or a wide variety of other behaviors.
Different approaches are also likely to make different implicit assumptions about the more general causal relations among symptoms and between symptoms and mental illness more generally. One view is that symptoms have a relatively flat causal structure in which they are primarily the result of some underlying problem and only minimally influenced by one another. An alternative view is that there are strong and sometimes bidirectional casual relations among the symptoms themselves to the extent that certain symptoms will tend to cluster by virtue of their interdependencies alone. According to this view, a number of very distinct sets of causes can ultimately lead to what appears to be a very similar constellation of symptoms (equifinality). In this type of perspective, the concept of an “underlying disorder” does little, if any, theoretical work.
What role should symptoms play in furthering understanding of mental illness?
Depending on their perspectives on the four questions identified above, researchers may take different views as to what role symptoms should play in furthering the understanding of mental illness. One position is that symptoms should be treated primarily as diagnostic indicators. That is, although they may have clinical value beyond diagnosis (e.g., to provide context for making treatment decisions), research activities should be targeted toward addressing the features and causes of syndromes. By this view, symptoms form part of the evidence base that can be used to generate hypotheses about the nature and possible causes of syndromes, but the ultimate goal is to explain those syndromes.
A contrasting perspective is that the symptoms themselves should be the primary targets of description and explanation irrespective of diagnostic classification. By this view, research should focus on further describing the characteristics and causes of individual symptoms. This could include research focused on phenomenological, behavioral, physiological, or neurobiological aspects of individual symptoms and/or their possible causes. It could also include examination of the broader context in which a symptom occurs, which may help adjudicate whether a given symptom represents a coherent construct or whether it dissociates into multiple, qualitatively and etiologically distinct phenomena. For example, the symptom of anhedonia, when reported in the context of generally low mood, may turn out to be qualitatively different from anhedonia reported in the context of a substance use problem, and each is associated with quite different causal pathways (see Leventhal et al., 2010). Finally, this endeavor could also include systematically examining the patterns of co-occurrence of symptoms for the purposes of uncovering their causal interrelations.
Perspectives on Symptoms
Drawing on the above questions, we now examine the core assumptions of three conceptual frameworks in relation to symptoms: the DSM-5 (APA, 2013), the SNWM (Borsboom, 2017), and a specific model of symptom formation developed by the Cambridge School: the Cambridge model (Berrios, 2013). Clearly these tools are markedly different: The DSM-5 is a classification manual, SNWM is a novel approach to modeling the interrelationships among symptoms, and the Cambridge model is an explicit model of the factors that shape the symptom experience. Although inclusion of the Cambridge model is more straightforward, we have chosen the DSM-5 and the SNWM approach in this article because they are both highly influential frameworks that make implicit assumptions about the questions we have identified above. We describe each conceptual framework and then apply the five questions described above (for more comprehensive descriptions of the DSM-5 and SNWM approaches, see Borsboom, 2017; Zachar & Kendler, 2017). Finally, we briefly discuss the recently proposed RDoC project (Insel et al., 2010). The RdoC is a framework for guiding future research efforts within the field of psychopathology, rather than a theoretical approach in its own right, but it is worth considering whether it makes any implicit or explicit assumptions about the nature of symptoms and their role in research.
The DSM-5
The DSM-5 is a tool for classifying different types of mental disorders. It outlines the diagnostic criteria for each specific disorder, which primarily consist of self-reported experiences and self-reported behavior patterns, which are collectively referred to as symptoms. Behaviors observed by a third person, or signs, can also act as diagnostic criteria. The DSM-5 does not explicitly align itself with any particular theory of psychopathology and aims to be as theory-neutral as possible in its descriptions.
A key feature of the DSM-5 is its use of a polythetic classification system in which no individual is required to meet all of the criteria for a particular diagnostic category but must satisfy a certain number, sometimes including one or more “core” obligatory criteria. This innovation gives the DSM-5 great flexibility, but at the cost of reduced coherence of the primary categories. For example, it has been estimated that there are at least 227 unique symptom profiles that could qualify for the DSM-5 diagnosis of MDD (Fried & Nesse, 2015), and two individuals can receive an MDD diagnosis without sharing any overlap in symptoms at all (see e.g., Chen, Eaton, Gallo, & Nestadt, 2000 1 ). Furthermore, people exhibiting completely opposite patterns of behavior can potentially qualify for the same criterion (e.g., sleep disturbance can be demonstrated by either insomnia or hypersomnia and appetite changes by either a significant increase or decrease in appetite). Although one might expect some degree of variability in the way different individuals experience the same condition, there is evidence to suggest that not all MDD symptoms are equally associated with the same risk factors. Consequently, it is quite possible that the category captures several possibly etiologically distinct phenomena (Chen et al., 2000; Fried, Nesse, Zivin, Guille, & Sen, 2014; Fried, Nesse, Guille, & Sen, 2015; Nandi, Beard, & Galea, 2009).
Turning now to the question of how the DSM–5 conceptualizes symptoms, its implicit position is that symptoms serve primarily as indicators of the person’s diagnosis at a syndrome level. Indeed, the manual fully acknowledges that the symptoms it includes are chosen according to their diagnostic usefulness. Although “cross-cutting” symptoms (those that may be present in multiple diagnoses) are seen as valuable for constructing a richer case formulation and for identifying issues of practical concern, these considerations are secondary to diagnostic classification. The manual itself remains neutral regarding whether individual symptoms may be a worthy target of research study in their own right.
Below we consider the assumptions of the DSM-5 approach with respect to the five key questions we posed, which are summarized in Table 1.
Shaping factors
Within the DSM-5, self-reported symptoms are seen as experiences or behavior patterns that are in some sense already known to the person and are merely “uncovered” through the use of interview or written questionnaire methods. Indeed, the widespread acceptance of self-report measurement tools and structured interview schedules as a basis for diagnosis within the DSM-5 framework demonstrates how confident researchers are in this assumption (e.g., self-report scales such as the Millon Clinical Multiaxial Inventory–IV, Millon, Millon, & Grossman, 2015; and interview schedules such as the Structured Clinical Interview for DSM-5 Personality Disorders, First, Williams, Karg, & Spitzer, 2016). Furthermore, although the DSM-5 recognizes that symptoms may present differently depending on the individual and also social and cultural context, the status it assigns to them as indicators of the underlying disorder implies that symptoms are seen as sharing certain core features across individuals irrespective of how any particular person comes to understand those symptoms.
Level of abstraction
The depiction of symptoms in the DSM-5 is a conceptually “thin” one. Although there is considerable discussion about how clinical judgments should be made about whether a symptom is present (e.g., the kinds of evidence that can be brought to bear), there is no explicit acknowledgment that the symptom constructs themselves may be heavily theory laden. For example, the description of body image disturbance, a symptom that forms part of the diagnostic criteria for anorexia nervosa (AN) is described simply as a “disturbance in the way one’s body weight or shape is experienced” (APA, 2013, p. 339). This symptom would seem to be much more than an observation derived from systematic examination of patient profiles. Rather, it is a theoretical construct in its own right that is implicitly embedded within a conceptualization of AN that attributes a central role to distorted perceptions (e.g., Mölbert et al., 2017). Many symptoms included in the manual are heterogeneous categories, and as noted above, some symptoms are “double ended” in the sense that opposite extremes can both qualify for the same criterion (e.g., sleep disturbance in MDD can include insomnia and hypersomnia; APA, 2013).
Finally, many of the DSM-5’s symptom definitions are underspecified and may potentially encompass a number of distinctly different phenomena with different characteristics and etiologies. For example, the symptom of impaired concentration is described in the DSM-5 variously as “diminished ability to think or concentrate” (MDD) or “difficulty concentrating or mind going blank” (in generalized anxiety disorder). Studies of patient narratives suggest that this symptom may fractionate into at least three qualitatively distinct experiences. Some individuals describe an experience of “blanking” (a feeling of disruption to the flow of consciousness); others describe a distinctly different experience of “mind wandering” (in which thoughts seem to readily drift off topic; Watts, MacLeod, & Morris, 1988; Watts & Sharrock, 1985). Yet others describe a feeling that their concentration is actively interrupted by intrusive, worrying thoughts (Hallion, Steinman, & Kusmierski, 2018).
Descriptive explanations
The DSM-5 is primarily a tool for the classification of mental disorders and does not make presumptions as to how the various self-reported and other behavioral phenomena it identifies should be researched. However, when it comes to determining the presence of symptoms for diagnostic purposes, it explicitly advocates the use of constrained first-person methodologies, such as structured interview schedules and self-report behavior rating scales. The DSM-5 manual recognizes the potential future utility of cognitive neuroscience measures such as fMRI and positron emission tomography but sees their value as primarily in improving the diagnostic classification process itself (APA, 2013).
Causal explanations
From the viewpoint of the DSM-5, symptoms arise primarily as a result of some broader underlying dysfunction. This dysfunction may be a consequence of a set of biological or environmental factors or a mixture of both (a minority of diagnostic categories, e.g., that for posttraumatic stress disorder, incorporate a hypothesized causal factor as part of the diagnosis, but for the most part, the manual is silent on the broader question of causation). It is assumed that the mechanisms or causal processes responsible for each syndrome will one day be identified and that once this occurs, diagnostic categories will be genuinely explanatory. The approach allows for the possibility of some causal interplay among the symptoms themselves. However, the core assumption of the DSM-5—that symptom profiles are meaningful indicators of the nature of the underlying disorder—implies that this interplay must necessarily be limited. Furthermore, because the DSM-5 allows for the possibility that the same symptom may be present in two hypothetically distinct disorders, it also makes the implicit assumption that, at least in some instances, very different underlying etiologies can lead to the same endpoint (equifinality).
The approach and language of the DSM-5 carry an implication that its ultimate objective is to develop explanations phrased at the biological level of description. However, the approach is not directly incompatible with the view that some mental disorders—or at least some aspects of those disorders—may be better captured at a psychological or even a social/cultural level of description (e.g., AN, substance use disorders).
Role in scientific inquiry
When it comes to the role of symptoms in furthering understanding of mental disorders, the DSM-5’s assumptions are fairly straightforward. Symptoms are seen as providing evidence that can point to a syndrome and, ultimately, an underlying cause. The symptoms that constitute a given syndrome are seen as meaningfully interrelated and capable of collectively constraining those casual explanations. Implicit in this approach is the idea that research should be directed at developing understanding of syndromes and their causes. Symptoms are a source of evidence that can be used constrain these explanations.
Comment
The characterization of symptoms in the DSM-5 is thin and list-like in quality. The manual assumes that symptoms are distinct from the underlying disorder but at the same time caused by it (either directly or indirectly). Because it is a primarily a tool for differential diagnosis, it focuses on those symptoms that have practical value in the diagnostic process—that is, those that are stable and reliably identified and are both sensitive and specific to the diagnosis in question.
The SNWM approach
SNWM is a recent approach to the investigation of mental disorders that focuses on mapping the interrelationships among individual symptoms (Borsboom, 2017; Borsboom & Cramer, 2013; Borsboom et al., 2019). It emphasizes the use of empirical data to derive statistical models of these interrelationships. Symptoms are defined as “the components in the psychopathology network [that] correspond to the problems that have been codified as symptoms in the past century and appear as such in current diagnostic manuals” (Borsboom, 2017, p. 7). A core premise of the approach is that symptoms vary with respect to their relationships with other symptoms: Those that are closely causally interrelated, form tight clusters and those with less direct causal relations are represented in the network as more widely dispersed. Furthermore, the patterns of association among different symptoms are seen as an important source of evidence in their own right. A typical empirical approach adopted within this framework is to gather data from a large number of individuals about a wide variety of symptoms through the use of self-report instruments and then to systematically examine the patterns of association among symptoms. This approach can also be used contrastively to assess the way in which these patterns of association differ among different populations (e.g., Hartung, Fried, Mehnert, Hinz, & Vehling, 2019).
A key feature of the SNWM approach is that it places less emphasis than the DSM-5 on underlying disease as the primary cause of symptoms. Rather, symptoms are viewed as emerging from a set of complex causal interactions among themselves and other relevant shaping factors. For example, chronic worry may cause sleep difficulties, which may in turn exacerbate the worry, and so on. The dynamic structure of the symptom network is simultaneously shaped by both internal factors (biological or psychological) and external factors (social or cultural). However, once a network of symptoms is established above a certain severity threshold, it becomes self-sustaining and is the disorder; external events or processes are better viewed as part of the “external field of the symptoms” (Borsboom, 2017, p. 6).
Shaping factors
Researchers working within this frame-work view people as active agents, capable of constructing meaning around their symptoms and interpreting them in a way that makes most sense to them (e.g., Borsboom et al., 2019). They also recognize that symptoms may be imperfectly operationalized. For example, two items on a self-report questionnaire could be closely associated not because the constructs they measure commonly co-occur but because they are in fact indices of the same construct (see e.g., Fried & Cramer, 2017). However, the default assumption is that each symptom identified in any particular model measures the same fundamental underlying complaint, irrespective of a person’s characteristics or social/cultural environment, and that different symptoms represent genuinely different underlying problems. Symptoms appear to strongly resemble those associated with classification manuals such as the DSM-5—discrete, independent entities that retain their basic nature across time and cultures.
Level of abstraction
Within the SNWM approach, the explanatory focus is on the relationship among symptoms; there has been comparatively little discussion of their internal structure and nature. Within the SNWM body of research, symptoms are treated as essentially observable phenomena rather than theoretical constructs in their own right.
Descriptive explanations
The primary focus of the SNWM approach is on the way symptoms cohere and interact, and this information is seen as having the potential to inform models of the symptoms themselves. The main aim of this endeavor is not to describe individual symptoms but rather to describe the way different combinations of symptoms emerge and are maintained.
Because of its emphasis on the value of subjectively reported experiences and behaviors, the SNWM approach clearly endorses constrained first-person perspectives as a means of gaining insight into the nature of mental illness. Furthermore, because it recruits symptom lists from manuals such as the DSM-5 and self-report instruments based on this type of framework, it implicitly assumes the validity of the kinds of self-report and interview methods typically used to measure them. However, the SNWM approach does not exclude the possibility that findings based on third-person methods could also be incorporated into future network models (e.g., genetic or neurobiological outcomes and measures; Borsboom & Cramer, 2013).
Causal explanations
From the viewpoint of the SNWM approach, symptoms are not necessarily consequences of underlying disorders. They are emergent properties of a complex causal network, which itself constitutes the mental illness (see Schmittmann et al., 2013). Symptoms interact to cause other symptoms, and once a network has been established above a certain severity threshold, they may sustain each other indefinitely. For example, severely disrupted sleep—whatever its cause or causes—may in turn lead to fatigue, poor concentration, memory problems, loss of enjoyment, impaired work performance, and, ultimately, reduced self-esteem (Baglioni et al., 2011; Borsboom, 2017; Fried & Cramer, 2017). Within the SNWM framework, two major types of symptoms can be distinguished that may differ with respect to their causal roles. Central symptoms are those that have numerous, close associations to a large number of other symptoms and, therefore, may play a central role in the development of the wider set of problems (Fried et al., 2017). Bridge symptoms are those that appear to be associated with more than one symptom cluster, possibly representing common endpoints of distinctly different causal chains (equifinality; e.g., sleep problems, fatigue, concentration problems; Borsboom & Cramer, 2013; Cramer et al., 2010; Fried et al., 2017). These bridge symptoms may help us to understand the factors that underpin psychiatric comorbidity. Although the ultimate aim of the SNWM approach is to uncover causal relationships, it is acknowledged that patterns of associations do not provide direct evidence regarding causal relationships, which may in fact be highly complex and bidirectional.
Role in scientific inquiry
According to the SNWM approach, symptoms do not provide evidence for an underlying mental disorder; essentially, they are the mental disorder. That is, symptoms are more than just pointers to a diagnosis; they are a valuable source of information in their own right. The approach sees particular value in examining patterns of co-occurrence among symptoms and views this information as important in advancing descriptive and explanatory models of mental health problems. The approach is not a model of causation as such but rather a framework for investigating questions about causation.
Comment
What is distinctive about the SNWM approach is the emphasis it places on the role of symptoms in constituting and causing mental disorders. Symptoms and their interrelationships are the core theoretical constructs. However, it does not address the question of what constitutes a symptom. Rather, the approach largely depends on the conceptualization of symptoms offered by the DSM-5. If these symptoms are not themselves coherent constructs, then some of the observed associations may be artifactual. For instance, if a single symptom construct dissociates into more than one qualitatively and etiologically distinct phenomenon, it may appear in a symptom network model as a “bridge” symptom. However, in this instance, it would be incorrect to conclude that it is a genuine common endpoint of multiple causal processes.
Another challenge with this approach is that the findings observed with any one sample will depend crucially on how participants are selected. Any clinical sample, no matter how inclusive, will have undergone at least some selection before the study, which itself is likely to influence the incidence of a particular symptom and also possibly the likelihood with which it is accompanied by other symptoms.
The Cambridge model
The Cambridge model (Aragona & Marková, 2015; Berrios, 2013; Marková & Berrios, 2009, 2012) is perhaps the most elaborated model of the internal structure and formation of subjectively experienced symptoms. The model proposes that these kinds of symptoms are created in the following way. In the first phase, a biological signal engenders a raw, immediate subjective experience, which is formless, “pre-linguistic and pre-conceptual” (Berrios, 2013, p. 44). This signal may be a relatively direct response to a specific stimulus (e.g., a loud noise or a pain in the muscle), or it could reflect a complex interaction between a stimulus and the person’s internal emotional and/or cognitive state (e.g., autonomic changes in a person with social anxiety when entering a crowded room).
In the second phase, people create a semantic envelope around the experience: They interpret its meaning in terms of their personal, social, and cultural schemas. If the experience is familiar, its interpretation will be straightforward and reflect previously established implicit beliefs and theories. If it is unfamiliar, the person will draw from existing knowledge and work hard to give it meaning. In the third phase, another level of interpretation occurs when people discuss their experiences with friends or clinicians or consult resources such as the Internet and/or books. These interactions further shape people’s understanding of their experience.
Shaping factors
To the extent that the symptom experience is shaped by the perceiver’s own interpretations and interactions, people may have diverse and possibly even competing ways of making sense of them. Consequently, very similar signals can result in very different experiences for different individuals. For example, a signal such as accelerated heart rate may be experienced by many individuals as aversive. However, for a person who seeks high levels of stimulation, this experience could be positive. Crucially, the model stipulates that symptoms may be further shaped by the dialogue between clinician and patient (Ratcliffe, 2015). In this respect, symptoms are seen as socially constructed entities.
Level of abstraction
The Cambridge model views symptoms not merely as pointers to a wider, underlying problem but as complex phenomena in need of an explanation in their own right. These explanations will vary across individuals and will also vary depending on the approach taken by researchers and the types of information they emphasize.
Descriptive explanations
The explicit objective of the Cambridge model is to develop rich descriptions of symptoms that consider the biological, psychological, and cultural factors that shape them. For example, a description of an auditory hallucination could elaborate on its neurophysiological correlates, the emotions that accompany the experience, and the way in which it is interpreted at a higher level of meaning (e.g., as a spiritual experience). To this end, the approach supports the use of multiple methods and perspectives in gathering information about symptoms and their nature. However, given its heavy emphasis on the phenomenological experience of a symptom and how the symptom is interpreted by the experiencer, the approach attributes a special status to open-ended first-person methods, such as qualitative analysis of patient narratives.
Causal explanations
Within this approach, symptoms are seen as layered constructs: Although they are initiated by a biological signal, they are shaped by the personality of the experiencer, and by that person’s beliefs, and social interactions more generally. The approach allows for the possibility that there may be different causal processes for what appears to be the same type of symptom experience (equifinality), and conversely, similar causal processes can lead to very different symptom experiences (multifinality).
The Cambridge approach views symptoms as emerging from a complex, interactive set of causal factors, which may include biological and/or psychological variables. At the same time, some symptoms are best understood as cultural constructs with no clear relationship to an underlying disorder. For example, the experience of hearing the voices of one’s dead ancestors may be an indicator of significant dysfunction in some cultural contexts but a widely accepted practice within others.
Role in scientific inquiry
From the viewpoint of the Cambridge model, the relationship between biological signals and symptom construction can vary in terms of its directness. In some instances, the experience associated with the signal will be very similar across individuals and cultures and only minimally shaped by the person’s own interpretations, but in other instances, it may be heavily socially and culturally mediated. In these latter instances, it may be difficult to infer much about the underlying dysfunctional mechanisms.
Comment
The Cambridge model provides a rich framework for understanding how symptoms—or more specifically, self-reported subjective experiences—are formed and how they come to be reported. It provides a useful framework for characterizing different kinds of symptoms and has heuristic value in generating new avenues for research. However, one challenge with this approach is that it is extremely powerful in that a myriad of factors can potentially shape the experience of symptoms. In addition, it offers little guidance to researchers as to how we might measure and identify those factors in a way that is useful for research purposes. Indeed, one is left with the rather pessimistic view that many symptoms are simply too opaque and multidetermined to be directly informative of the underlying nature and causes of mental illness.
The RDoC
The U.S. National Institute of Mental Health proposed the RDoC as a framework for conceptualizing the types of research approaches that are likely to be important for advancing understanding of mental health and illness (Insel et al., 2010; see also Kapur, Phillips, & Insel, 2012; Morris & Cuthbert, 2012). Given the impact that this proposal has had on the field, it is worth considering briefly what assumptions it makes with respect to symptoms. The RDoC framework is neither a classification system nor a theoretical framework but rather a method for identifying new research avenues in the mental health area. It is founded on the core notion that a solid understanding of mental health should be founded on a model of the normal psychological systems that are implicated in those problems. Consequently, the various research approaches identified in the RDoC are targeted toward investigating those normal systems and how their functioning varies across individuals in both clinical and nonclinical contexts.
The RDoC framework identifies six broad psychological systems that are relevant to the study of mental health: negative valence systems (those involved in the response to aversive stimuli or contexts, e.g., fear, anxiety, loss), positive valence systems (those involved in the response to positive stimuli or contexts, e.g., reward seeking, reward/habit learning), cognitive systems (those involved in complex information processing, attention, perception, and memory), systems for social processes (those that shape responses in interpersonal settings, e.g., affiliation, attachment, social communication), arousal and regulatory systems (those that modulate arousal and regulate homeostasis), and sensorimotor systems (those involved in the acquisition, control, and execution of simple and complex motor behaviors, e.g., action selection, initiation, execution, habit development, behavioral inhibition). The framework recommends that each of these broad systems be studied at various units of analysis, which includes genes, molecules, cells, circuits, physiology, behaviors, and self-reported phenomena. However, it places particular emphasis on research into the neurobiological aspects of these various systems (e.g., physiology, genomics, and neuroscience).
Turning now to the RDoC’s perspective on the nature and usefulness of symptoms, the key publications describing the approach advocate for greater research focus on “generic” symptoms (those that cut across multiple diagnostic classifications). It also recommends the use of relatively undifferentiated participant samples. The RDoC authors do not address the question of whether current symptom constructs are themselves in need of reexamination. However, it explicitly values research that is directed at developing richer conceptual understandings of a range of normal and abnormal phenomena at various levels of description. It further emphasizes the value of more objective measures to “augment” traditional symptom-based classification systems, which may include more sensitive self-report instruments, observational methods, indices of neurobiological functioning, and genetic signatures (Morris & Cuthbert, 2012).
However, the RDoC advocates a shift in emphasis away from research that aims to describe or explain the outward indicators of a mental health problem and toward that which describes how the operation of the underlying psychological systems more generally and the degree to which they vary across individuals. Within this approach, symptoms and other indicators of psychopathology are no longer the primary objects of study (the phenomena in need of explanation) but rather operate as a set of constraints on models of these broader psychological systems and how they vary across individuals.
General comments
The analysis of the DSM-5, SNWM, and the Cambridge model was not undertaken to find out which framework is the “best one” or who is the “winner.” Rather, our aim is more metatheoretical: to explore the different ways symptoms are conceptualized in the literature and to formulate strategies to improve our understanding of them.
These three frameworks offer distinctly different perspectives on how one should understand symptoms and their relationship to mental illness. The DSM-5 approach treats symptoms as relatively unproblematic. They are thin constructs that are treated as collections of empirical observations, and the focus of discussion is on how best to detect the presence. The SNWM approach explicitly challenges some of the assumptions of the DSM-5, particularly with respect to the importance of syndromes as the main targets of explanation. It advocates the importance of empirical research to identify patterns of symptom co-occurrence independently of diagnostic categories. However, like the DSM-5, it treats the symptoms themselves as relatively transparent constructs. Finally, the Cambridge model questions this simple view of symptoms and offers a framework for conceptualizing how symptoms are constructed by the person experiencing them. However, although the Cambridge model recognizes there are sources of variation relating to the way individuals construct the symptom experience, it does not address how different symptoms may be related to each other or to the underlying mental health problem more generally.
Research Implications and Future Recommendations
One theme that emerges from this discussion is that one should take care not to confuse symptom descriptions with empirical observations. Symptom labels of the kind commonly used in psychopathology may describe a highly heterogeneous collection of phenomena that could in principle be grouped together in a number of different ways. Above, we have considered examples of relatively “straightforward” symptom constructs, such as poor concentration, and even these appear to exhibit fractionation on closer inspection. When it comes to more complex constructs, whose descriptions have evolved in response to theoretical as well as practical considerations, these concerns become even more acute. Consider, for example, body image disturbance, a symptom commonly viewed as a key feature of AN (Mölbert et al., 2017). This symptom owes its origins not to empirical observations but to early theories that considered AN to be a primary disturbance in the perception of somatic and other body-related stimuli (Bruch, 1964). That is, the construct emerged from a theoretical model of the nature and causes of AN. As the theoretical understanding of AN has evolved, to place less emphasis on perception and more on internalized goal representations, so too has the description of this symptom. For example, the third edition of the DSM (APA, 1980) described this symptom simply as a “disturbance in body image,” which strongly suggests a perceptual abnormality, whereas the later DSM-5 uses the broader phrase “disturbance in the way one’s body weight or shape is experienced,” which can potentially cover general dissatisfaction as well. In sum, the symptom is not always dissociable from the overarching theory.
Some symptom constructs may even rest on complex assumptions relating to culturally embedded normative values. Consider, for example, low self-esteem, one of the diagnostic criteria for MDD within the DSM-5 (described as “feelings of worthlessness”; APA, 2013, p. 161). Implicit in this concept is a culturally embedded normative judgment about the value of viewing oneself positively. However, in nonclinical samples, there are systematic differences in reported levels of self-esteem across cultures and even generations, and as a consequence, low reported self-esteem has stronger associations with psychopathology in some cultures than others (Gentile, Twenge, & Campbell, 2010; Heine, Lehman, Markus, & Kitayama, 1999; Schmitt & Allik, 2005).
The theory-laden nature of many symptoms means that researchers should reflect on the assumptions they make when mapping observations to symptom labels and explicitly set out these assumptions. Furthermore, they also need to keep in mind that a person’s description of any experience or set of behaviors is likely to be shaped by a host of factors, many of which are external to the individual. Special attention should therefore be paid to the methods used to elicit them.
In terms of specific recommendations for future research, our first suggestion is that there should be greater emphasis on individual symptoms as the targets for investigation in their own right. For example, instead of selecting participants for research according to their syndrome diagnosis (DSM-5 or otherwise), we might instead select them according to the presence or absence of a key symptom (for a classic statement of this position, see Persons, 1986). The goal of research would then be to examine the causes, determinants, and characteristics of each symptom. Within this type of approach, the variation among participants with respect to their other features (e.g., co-occurring symptoms) constitutes just one of a number of sources of information that could be brought to bear in developing descriptive and explanatory models of individual symptoms. Recent studies that illustrate this type of approach include that of Stuhrmann et al. (2013), which focused on the symptom of physical anhedonia (an inability to feel pleasure in response to sensory stimulation). These researchers found that scores on a self-report measure of this construct were negatively associated with an fMRI measure of amygdala responsivity to positive stimuli, suggesting that physical anhedonia may be a consequence of emotional abnormalities occurring at very early processing levels. Other recent examples can be seen in the research on psychosis (e.g., Egeland, Holmen, Bang-Kittilsen, Bigseth, & Engh, 2018; So et al., 2018) and eating disorders (Peñas-Lledó, Vaz Leal, & Waller, 2002).
These kinds of methodological strategies can enable us to explicitly develop “mini” constitutional explanations of individual symptoms, each of which would address their features at different levels of analysis. For example, one could describe the symptom of depressed mood in terms of its phenomenology (how it feels to have this symptom), its neural or biochemical correlates (neural activity patterns that accompany the symptoms), or behavioral manifestations (accompanying behaviors, e.g., crying and restricted facial expressions). Even at the psychological level, explanations can focus on different facets of the symptom. It can be described in cognitive terms, as a set of attentional and cognitive biases that favor negative information and attribution (e.g., “everything’s getting worse,” “I am unlovable,” “I should be perfect”; Beck, 2008), or in emotional terms, as a negative affective state (Barret, Lewis, & Haviland-Jones, 2016).
This rich description approach to symptoms will not only shed light on the nature of the symptoms themselves but also will help to identify whether a given symptom description constitutes a coherent phenomenon or whether it fractionates into a number of distinctly different phenomena with different etiologies. Methods such as thematic analysis may be a particularly useful first step in this process. Consider the example of extreme fatigue, which is a common symptom of many medical and psychiatric conditions. People with significantly depressed mood commonly describe their fatigue as a feeling of heaviness, such that embarking on even simple tasks requires an enormous amount of effort (Matza et al., 2015). People reporting fatigue in the context of cancer commonly mention decreased physical performance, feelings of weakness, and an excessive need to rest after physical activity (Glaus, Crow, & Hammond, 1996), using phrases that often reference the body (e.g., “heavy limbs,” “legs like jelly/wobbly legs,” “feeling weak,” or “the body is worn out”; Bootsma, Schellekens, van Woezik, van der Lee, & Slatman, 2019). These sorts of qualitative analyses provide some useful clues as to how one might further examine the coherence of this construct at different levels of description. For example, one possible next step might be to examine the impact of mental and or physical exertion on individuals’ physical performance using techniques such as cardiopulmonary exercise testing (see e.g., Donath et al., 2010; Neil, Klika, Garland, McKenzie, & Campbell, 2013; Vigo et al., 2015). Such a method might help to tease apart fatigue associated with fatiguability after exertion from fatigue associated with a feeling of more general heaviness and lassitude. Indeed, once a subjective phenomenon can be effectively described at other levels of analysis (in this case, behavioral/physiological), this evidence can be incorporated into the symptom construct or constructs and be used as part of the criteria for identifying that symptom. It may even replace first-person accounts as the gold standard for identifying that phenomenon.
It is important to emphasize that these richer symptom descriptions can do more than just flesh out some of the finer details of what constitutes the symptom; they may also lead us to reconceptualize the symptom space altogether. If the symptom of fatigue actually fractionates into two distinctly different complaints with different etiologies, then a failure to distinguish these will confound any attempts to explain the phenomenon and may lead to spurious associations between complaints that are in fact etiologically unrelated. For example, fatigue may be found to be associated with both depressed mood and a diagnosis of cancer for entirely independent reasons, giving the false impression that the first is somehow indirectly causally related to the second.
These kinds of symptom-oriented research strategies are seen as just one of a number of research avenues in psychopathology. A complementary approach, and one advocated in the RDoC, involves directing research not at the clinical problem space but at the various psychological systems that are believed to play a crucial role in mental health problems. Within this type of approach, symptoms are not the primary targets in need of explanation but rather serve as just one of a number of potential indicators of abnormality within a particular psychological system (see especially, Elbau, Binder, & Spoormaker, 2019). Others include behavioral observations and markers of physiological or neurological activity. Of course, these kinds of approaches will yield meaningful information only if they draw on robust theoretical frameworks that adequately describe the nature of the key psychological systems and how best to assess them. It is fair to say that this kind of theory development is still in its infancy. Consequently, an optimal strategy going forward would be to use both system-oriented and symptom-oriented approaches as complementary sources of converging information about the nature of mental health problems.
Conclusions
In light of a lack of research progress in identifying the causes and nature of mental disorders, it is timely to rethink some of the field’s foundational assumptions and to consider alternative ways of proceeding. We thoroughly applaud recent research approaches that challenge the assumptions of conventional diagnostic schemes such as the DSM-5 (e.g., Borsboom, 2017; Cuthbert & Kozak, 2013; Kotov et al., 2017; Zachar & Kendler, 2017). However, here we argue that there is an equal need to challenge our assumptions regarding the nature and conceptualization of symptoms. In this article, we identified five key questions that are directly or indirectly concerned with symptoms, ranging from the way they are experienced by individuals to their relationship with mental illness more broadly. Researchers’ implicit or explicit answers to these questions shape the way they go about investigating mental health problems. For example, when symptoms are viewed as relatively low-level consequences of underlying mental illness, then our focus of inquiry is directed to the factors that are thought to cause them rather than on the symptoms themselves. However, when symptoms are conceptualized as parts of a disorder, with their own (potentially heterogeneous) internal structure, then there is likely to be greater emphasis on constructing detailed models of them at various levels of analysis. We believe that this kind of approach is capable of providing rich insights into mental health problems, which complements that provided by other approaches. In sum, the assumption that symptoms are little more than observable facts limits our progress in understanding mental disorders. There is little point in continuing to develop and refine statistical techniques or classification schemes until we have a better grasp of these key concepts.
Footnotes
Acknowledgements
We thank Snita Ahir-Knight, Hannah Hawkins-Elder, and Daniel Wegerhoff for their helpful comments on an earlier version of this article.
Transparency
Action Editor: Kenneth J. Sher
Editor: Kenneth J. Sher
Author Contributions
C. E. Wilshire and T. Ward contributed equally to this article. S. Clack provided valuable comments, added key illustrations, and extended several important lines of argument. All of the authors approved the final manuscript for submission.