
Abstract
In the present work, we evaluated reciprocal, within-dyads associations between parents’ and adolescents’ depressive symptoms across two independent samples (N = 327 and N = 435 dyads; approximately 85% biological mothers) assessed every 3 months for 2 years (Study 1) to 3 years (Study 2). Results of random intercept cross-lagged panel models converged to support positive contemporaneous patterns of cofluctuation in parental and adolescent depression such that within-persons deviations in parental depression were associated with same-direction within-persons deviations in adolescent depression at the same time point. In contrast, within-persons fluctuations in parental depression did not prospectively predict within-persons fluctuations in adolescent depression, or vice versa, across the follow-up period. Results held across boys and girls, as well as dyads with and without a parental history of depressive disorder. Overall, findings advance knowledge by demonstrating that after accounting for between-persons/dyads variance, parental and adolescent depression demonstrate contemporaneous cofluctuations but do not demonstrate within-dyads reciprocity over time.
Keywords
Parental depression has been related to enduring patterns of offspring psychosocial impairment, and it has implications for youths’ socioemotional functioning across development (e.g., Brennan et al., 2002; Goodman, 2007; Lewinsohn et al., 2005; Weissman et al., 2006). Offspring of depressed parents are approximately 3 times more likely than offspring of nondepressed parents to experience clinically significant levels of depression (Lieb et al., 2002). Elevations in depressive symptoms among children of depressed parents may be particularly likely to occur during the transition to adolescence, a developmental period during which youths demonstrate enhanced vulnerability to the onset of psychopathology (Costello et al., 2011; Merikangas et al., 2010; Paus et al., 2008). Indeed, adolescence may represent a key period of risk for children of depressed parents, given evidence that presence of parental depression predicts earlier onset of depression among youths (Birmaher et al., 1996; Hammen & Brennan, 2003), which may portend life-course persistent patterns of distress and impairment (Keenan-Miller et al., 2007; Weissman et al., 1999).
Interest in understanding processes contributing to depressive risk transmission among families affected by parental depression has inspired a rich body of research examining the influence of parental depression on children’s psychopathology outcomes (for recent reviews, see Goodman, 2020; Gotlib et al., 2020), generating a number of hypotheses concerning the way in which increased risk for depression may occur among children of depressed parents. Although shared genetics are presumed to play some role in the longitudinal coupling of parent–child depressive symptoms (see Goodman & Gotlib, 1999), results of studies using genetically informed designs suggest that exposure to parental depression also functions through environmental means to increase risk for depression in offspring (McAdams et al., 2015; Natsuaki et al., 2014; Singh et al., 2011; Tully et al., 2008). Note that this pattern of relations is observed at both clinical and subclinical levels of parental symptoms (Natsuaki et al., 2014), suggesting that children’s symptoms may fluctuate in tandem with symptom fluctuation in parents. Such patterns of cofluctuation in depression levels have been observed contemporaneously among parent–child dyads (Flancbaum et al., 2011), and prospective studies indicate that within-persons fluctuations in parental depression interact with individual difference factors, including youths’ cognitive risks (Abela et al., 2006), attachment cognitions (Abela et al., 2009), and genotype (Oppenheimer et al., 2013), to predict within-persons fluctuations in youths’ depression.
It is noteworthy that if depression within the family system is transmitted, at least in part, via environmental mechanisms, parents’ depression may also be influenced by dynamic fluctuations in their children’s symptom experience. Relatively little research has rigorously addressed the ways in which parents’ and children’s depressive symptoms may demonstrate reciprocal patterns of relations over time; however, it has long been recognized that parent–child relationships are bidirectional in nature, and children’s effects on their parents represent salient, if understudied, developmental phenomena (Lougheed, 2020; Pardini, 2008). Research is needed to clarify patterns of prospective, within-dyads bidirectional relations between parents’ and youths’ depressive symptoms and advance knowledge of the ways in which parents’ and children’s depressive symptoms influence one another over time. Thus, the present inquiry aimed to investigate reciprocal patterns of within-dyads associations between parents’ and children’s depressive symptoms in two independent samples of parent–adolescent dyads followed prospectively over a period of years in repeated measures designs. Implementing an advanced statistical design aimed at disambiguating between- and within-dyads sources of variance in depressive-symptom experience, in the current work, we present a rigorous investigation of the way in which idiographic changes in parents’ and adolescents’ depressive symptoms influence one another over time.
Theories of Within-Dyads Depression Transmission
In their foundational article enumerating potential mechanisms of intergenerational risk transmission among children of depressed mothers, Goodman and Gotlib (1999) identified exposure to parental negative affectivity and maladaptive cognitions and behaviors as one candidate mechanism by which youths acquire risk for the onset of clinical symptoms. Such a mode of depressive transmission within parent–adolescent dyads would be consistent with tenets of social learning (Bandura, 1977) as well as emotional contagion and interpersonal theories of depression (Coyne, 1976; Hames et al., 2013; Hatfield et al., 1993). These theories suggest that modeling processes, nonconscious interpersonal mimicry behaviors, and dysfunctional patterns of interpersonal functioning promote the diffusion of mood states and associated behaviors within close interpersonal networks. Within this conceptual framework, increases in a given parent’s symptoms of depression would be hypothesized to contribute to changes in their child’s symptoms of depression as the parent’s negative mood states and depressive behaviors trigger implicit learning and socialization processes. Less theoretical work has specifically articulated the mechanisms by which adolescents’ depressive symptoms may influence parental levels of depression symptom severity. However, it follows from these same theories of social learning, emotional contagion, and interpersonal relations that youths’ experience of depressive symptoms may effect change in their parent’s experience of depression through analogous processes of emotional convergence. Consistent with this theoretical lens, meta-analytic findings support depressive contagion in cross-sectional studies of adult dyads (e.g., roommates, romantic partners) such that interactions with depressed peers and partners elicit proximal increases in individual partners’ levels of depression (Joiner & Katz, 1999).
Empirical Evidence Supporting Bidirectionality of Parent–Offspring Symptoms
A small number of studies that used prospective, repeated measures designs have found reciprocal patterns of association between parents’ and youths’ depressive symptoms across various stages of child development. Among a diverse sample of parent–toddler dyads, for example, Roubinov et al. (2019) demonstrated bidirectional associations between maternal depression and mothers’ report of children’s internalizing symptoms in 18-month-old to 4-year-old children. Evidence for transactional patterns of relations between parent–offspring symptoms also emerged in work by Gross et al. (2008); using a latent class analysis, Gross et al. found that youths’ noncompliant behavior at age 18 months predicted chronic, elevated trajectories of maternal depression across an 8.5-year follow-up period. Two studies (Ge et al., 1995; Hughes & Gullone, 2010) in which traditional cross-lagged panel modeling (CLPM) were used demonstrated bidirectional relations between parents’ and children’s psychological distress and internalizing symptoms, respectively. Specifically, Ge et al. (1995) demonstrated reciprocal relations between parent–adolescent psychological distress in a prospective study of seventh-grade students assessed annually for a period of 3 years. Hughes and Gullone (2010) demonstrated bidirectional associations between parent–adolescent internalizing symptoms in a sample of 14- to 18-year-old youths assessed twice across a 6-month period. Moreover, among a sample of mothers with a history of recurrent depression, Sellers et al. (2016) demonstrated that adolescent daughters’ depressive symptoms prospectively predicted increases in maternal symptoms of depression across a 29-month follow-up period.
Together, this body of work provides initial support for a potential transactional model of parents’ and youths’ depressive symptoms across child and adolescent development, although note that some studies have yielded mixed or inconsistent patterns of findings (Ciciolla et al., 2014; Mennen et al., 2018). In a sample of children with and without developmental delays assessed annually from ages 3 to 5, Ciciolla et al. (2014) demonstrated reciprocal associations between maternal distress and children’s internalizing symptoms only in 3- and 4-year-old developmentally at-risk youths. In another three-time-point study analyzed using a CLPM approach, Mennen et al. (2018) found no evidence for reciprocity in parent–child self-reported depression among a sample of youths ages 9 to 13 years at baseline. Moreover, unidirectional paths were moderated by children’s gender and maltreatment status such that patterns of effects differed across boys and girls and among youths with and without a history of maltreatment. In addition, using a genetically informed design, McAdams et al. (2015) demonstrated unidirectional associations from children’s to parents’ depression but not from parents’ to children’s depression, although differences in effect sizes between these divergent pathways were small in magnitude.
A key limitation of previous work is its reliance on traditional CLPM approaches (see Ge et al., 1995; Gross et al., 2008; Hughes & Gullone, 2010; McAdams et al., 2015; Mennen et al., 2018; Roubinov et al., 2019) that fail to appropriately disaggregate between-persons/dyads from within-persons/dyads sources of variance (Hamaker et al., 2015). This methodological limitation is significant because simulation studies suggest that failure to account for these unique sources of variance may contribute to misleading patterns of effects, particularly when conflicting processes exist at the between- and within-persons levels (Hamaker et al., 2015). Indeed, recent work using advanced structural equation modeling (SEM) techniques, such as random intercept cross-lagged panel models (RI-CLPMs), which address the main limitation of traditional CLPMs and appropriately partition sources of variance (between-persons from within-persons), highlights the need to reevaluate “known” patterns of associations in developmental psychopathology literatures (see Keijsers, 2016). The theoretical models positing modeling or emotion and social contagion processes presume and are conceptually based on within-dyads parent–offspring effects over time. Yet studies in which CLPMs are used cannot be assumed to accurately reflect these hypothesized within-persons/dyads change processes (see Keijsers, 2016). To rigorously and appropriately test theories of longitudinal symptom coupling, which fundamentally propose within-dyads mechanisms of action, within-dyads effects must be accurately separated from between-dyads influences so that proper inferences and conclusions can be attained.
Of the available empirical studies, to our knowledge, only Kouros and Garber (2010) employed appropriate modeling techniques to evaluate within-dyads transactional associations between parents’ and children’s depressive symptoms. In a prospective study of parent–adolescent dyads assessed annually from Grades 6 through 12, Kouros and Garber applied dynamic bivariate latent-difference-score models to demonstrate longitudinal coupling between parents’ and adolescents’ depressive symptoms such that dyad members’ level of depressive symptoms reciprocally predicted one another over time. This study had a relatively long (i.e., 1 year) interassessment time interval, and thus, research is needed using more frequent assessments to precisely evaluate reciprocal associations between parents’ and adolescents’ depressive symptoms across shorter time intervals.
In addition, research is needed to evaluate theoretically based moderators that might be expected to modulate the strength of association between parents’ and children’s depressive symptoms. Children’s gender identity and parents’ history of depression diagnosis are two individual difference factors that may influence dyad members’ sensitivity to one another’s fluctuating levels of depression. Girls may be especially vulnerable to the depressogenic effects of fluctuations in their parents’ depression given that girls have been found to demonstrate enhanced interpersonal sensitivity relative to boys (Cyranowski et al., 2000; Hankin et al., 2007; Rudolph, 2002). Indeed, Mennen and colleagues (2018) found that reciprocal patterns of relations between parents’ and children’s symptoms varied by children’s gender. Parental history of depressive disorder may also influence strength of reciprocal associations between parents’ and adolescents’ depressive symptoms. Theory and research suggest that parents with a history of depressive disorder, as well as their offspring, demonstrate elevated reactivity to stressors in their environments relative to people without such histories (e.g., Hammen, 2005; Morris et al., 2010). This suggests that dyads characterized by parental history of depression may demonstrate stronger patterns of depressive reciprocity relative to dyads characterized by a lack of parental depression history.
Study 1
In Study 1, we aimed to investigate within-dyads, reciprocal patterns of prospective relations between parents’ and youths’ depressive symptoms in a sample of parent–adolescent dyads recruited from the general community. Participating parents completed gold-standard diagnostic interviews to ascertain parental lifetime history of depressive disorder before enrollment in the study. Participating parents and adolescents then completed self-report questionnaire measures assessing symptoms of depression every 3 months over 2 years of follow-up, yielding nine total assessment points with which to evaluate within-dyads bidirectional patterns of change. Patterns of within-dyads change were evaluated using an RI-CLPM approach. In contrast to traditional CLPMs, RI-CLPMs appropriately partition within and between variance (Hamaker et al., 2015; Mund & Nestler, 2019) and permit analysis of the ways in which fluctuations from one dyad member’s mean depression levels concurrently relate to and prospectively predict within-persons fluctuations in the other dyad member’s symptom levels over time. In addition, these RI-CLPM analyses provide information about within-persons autoregressive stability of depressive symptoms and between-persons associations between parent–offspring trait-like symptom levels. Multiple group models were conducted to examine differences in patterns of prospective associations on the basis of adolescents’ gender as well as parental history of depressive disorder.
At the between-persons/dyads level, we expected parental and adolescent random intercepts (representing trait-like levels of depression) to be positively related. Prior meta-analytic findings suggest that during adolescence, parental depression is associated with youths’ depression with a mean effect size (r) of approximately .21 (Goodman et al., 2011); thus, we expected to observe a small but significant positive effect. At the within-dyads level, we hypothesized that parents’ and children’s depressive symptoms would be positively associated both contemporaneously and over time such that within-persons fluctuations in parents’ depressive symptoms would concurrently relate to and prospectively predict same-direction within-persons fluctuations in children’s depressive symptoms and vice versa. We hypothesized that positive patterns of prospective relations would be stronger from parental depression to child depression than from child depression to parental depression, consistent with previous research (e.g., Kouros & Garber, 2010). In addition, we hypothesized that prospective within-dyads effects in both directions would be stronger in dyads characterized by a parental history of depressive disorder and that within-dyads prospective effects of parental depressive symptoms on youths’ depressive symptoms would be stronger among adolescent girls. We made no a priori hypotheses concerning the relative strength of prospective effects from adolescent symptoms to parental symptoms on the basis of adolescents’ gender.
Method
Participants and procedures
Participants included middle school age youths recruited from communities in Montreal, Quebec, Canada, and Chicago, Illinois. A total of 382 youths from 327 families were recruited using ads placed in local newspapers and community locations seeking interested families for a study of adolescent development. For the purposes of the present study, one child from each family was randomly selected for inclusion in dyadic analyses, yielding a sample size of 327 parent–adolescent dyads. Participating youths ranged in age from 11 to 15 years at baseline (M = 12.58 years, SD = 1.09; 59.9% girls). Participants predominantly identified as European American (69.9%); smaller numbers identified as African American/Black (13.0%), Asian (11.8%), or other racial or ethnic identity (5.2%). The racial and ethnic composition of the samples at each site were roughly representative of the areas in which they were recruited (see Abela & Hankin, 2011). Participating parents were primarily women (91.7%; age: M = 43.89 years, SD = 6.16). Regarding educational attainment, 54.7% of participating parents reported having completed a bachelor’s degree or higher. More details concerning sampling and demographics are reported in Abela and Hankin (2011).
All study procedures were approved by the institutional review boards at McGill University and the University of Illinois-Chicago. Upon enrollment in the study, participating dyads were invited to the laboratory to complete a baseline assessment, during which informed consent and informed assent were received from parents and adolescents, respectively. During this baseline assessment, parents were interviewed by trained clinical staff using the Structured Clinical Interview for DSM-IV (SCID; First et al., 2002) to assess parental history of depression, and parents’ and adolescents’ depressive symptoms were assessed via self-report on the Beck Depression Inventory (BDI-II; Beck et al., 1996) and Children’s Depression Inventory (CDI; Kovacs, 2003), respectively. Youths and their parents were subsequently assessed for depressive symptoms using the CDI and BDI-II every 3 months for a period of 2 years, yielding nine total assessment points per dyad. Baseline depression assessments were administered simultaneously to parents and adolescents during their initial and final in-person visits; to minimize participant burden, dyads completed follow-up assessments from the comfort of their homes, and dyad members were asked to complete measures within a 2-week period. The majority completed measures on the same day; the modal difference in the number of days between caregivers’ and children’s assessment was 1, and the mean difference in the number of days was 2.12 (SD = 2.44). The average number of follow-up assessments completed by participating dyads was 6.74 (SD = 1.61). Number of follow-up assessments completed was not related to youths’ age, gender, or level of depressive symptoms (rs < |.03|, ps > .05).
Measures
Demographics
Basic demographic information, including parents’ and children’s age and gender identity and parental educational attainment, was assessed via parental self-report upon enrollment in the study. Gender identity was coded using a dichotomous variable reflecting participant identification as a boy/man (0) or girl/woman (1).
SCID
Parental history of depression before enrollment in the study was assessed at baseline using the SCID (First et al., 2002). All interviewers were trained and supervised by PhD-level, licensed clinical psychologists in administering the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) and assigning clinical diagnoses according to criteria described in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994). Details concerning interviewer training and supervision procedures are described elsewhere (see Abela & Hankin, 2011). For the purposes of the present analyses, history of caregiver depression was a dichotomous score indicating definite or probable caregiver lifetime major depressive disorder (MDD) or definite minor depressive disorder (mDD) following criteria described in the DSM-IV (American Psychiatric Association, 2000). Diagnoses were collapsed into a single variable given evidence that depression is distributed dimensionally at the latent level (Hankin et al., 2005; Slade & Andrews, 2005) and that all diagnoses included in the present study (definite MDD, probable MDD, and definite mDD) are associated with significant distress and impairment (Cuijpers, 2004; Kessler et al., 1997). In total, 83 (25.4%) parents reported a history of depressive disorder occurring before enrollment in the study.
CDI
Youths’ depressive symptoms were measured at each assessment point via self-report on the CDI (Kovacs, 2003). The CDI comprises 27 items assessing youths’ experience of a range of psychological, social, and somatic symptoms associated with depression. Each item is scored on a 3-point Likert scale from 0 to 2, and total scores range from 0 to 54. Higher scores indicate higher levels of depressive symptoms. The CDI demonstrates good psychometric properties (Klein et al., 2005). Coefficient αs ranged from .87 to .91 across administrations in the present study, indicating strong internal consistency.
BDI-II
Parental depressive symptoms were similarly measured at each assessment point via self-report on the BDI-II (Beck et al., 1996). The BDI-II comprises 21 items assessing parents’ experience of a range of psychological, social, and somatic symptoms associated with depression. Items are scored on a 4-point Likert scale, and total scores range from 0 to 63. Higher scores indicate higher levels of depression. The BDI-II demonstrates strong psychometric properties, including reliability and validity, in diverse samples of adults (Beck et al., 1996). Coefficient αs ranged from .89 to .95 across assessment points, indicating good internal consistency.
Data analytic plan
Analyses were conducted using SEM implemented in the lavaan package (Version 0.6-5; Rosseel, 2019) for the R software environment (Version 3.5.1; R Core Team, 2018) using the maximum likelihood robust (MLR) estimator because of nonnormality of manifest variables and full-information maximum likelihood (FIML) estimation to account for missing data. Goodness of fit was assessed using convergence across multiple fit indices, including root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and comparative fit index (CFI), consistent with recommendations proposed by Hu and Bentler (1999). Specifically, good fit was indicated by RMSEA no higher than 0.06, SRMR no higher than 0.08, and CFI of at least .95 (Hu & Bentler, 1999). Acceptable fit was indicated by RMSEA no higher than .08 and CFI of at least .90. We prioritized convergence across indices over reliance on any one particular measure of fit (Chen et al., 2008; Kenny, 2020; Marsh et al., 2004).
We modeled prospective, reciprocal patterns of association between parents’ and adolescents’ depressive symptoms using an RI-CLPM approach (Hamaker et al., 2015; Mund & Nestler, 2019; see Fig. 1). To appropriately partition within-persons/dyads and between-persons/dyads variance, we constrained the variances of observed variables to 0 such that all variance would be captured by the within- and between-persons/dyads latent factors. To account for between-persons/dyads variance in constructs of interest, we created latent factors (i.e., random intercepts) corresponding to trait-like aspects of parental and adolescent depression. Observed variables at all nine time points were loaded onto their respective random intercept factors, and factor loadings were constrained to 1. These latent factors were permitted to covary to account for associations in trait-like levels of depression between parents and offspring. To model within-persons/dyads change, we loaded each of the observed scores at each time point onto its own latent factor, resulting in a total of nine latent factors. These nine latent factors were used to model within-persons autoregressive stability of depression as well as cross-lagged paths representing bidirectional, within-dyads effects of parental and adolescent depression across time. Because we did not hypothesize differences in the magnitude of autoregressive or cross-lagged paths between any two given assessment points, all autoregressive paths at the within-persons/dyads level were constrained to be equal to one another, and all cross-lagged paths from parental to adolescent depression as well as cross-lagged paths from adolescent to parental depression were similarly constrained to be equal. Contemporaneous, within-time-points covariances between latent factors corresponding to parents’ and adolescent’s depressive symptoms at the same time point were modeled to account for interdependence of parental and adolescent depression at the within-dyads level and were also constrained to be equal.
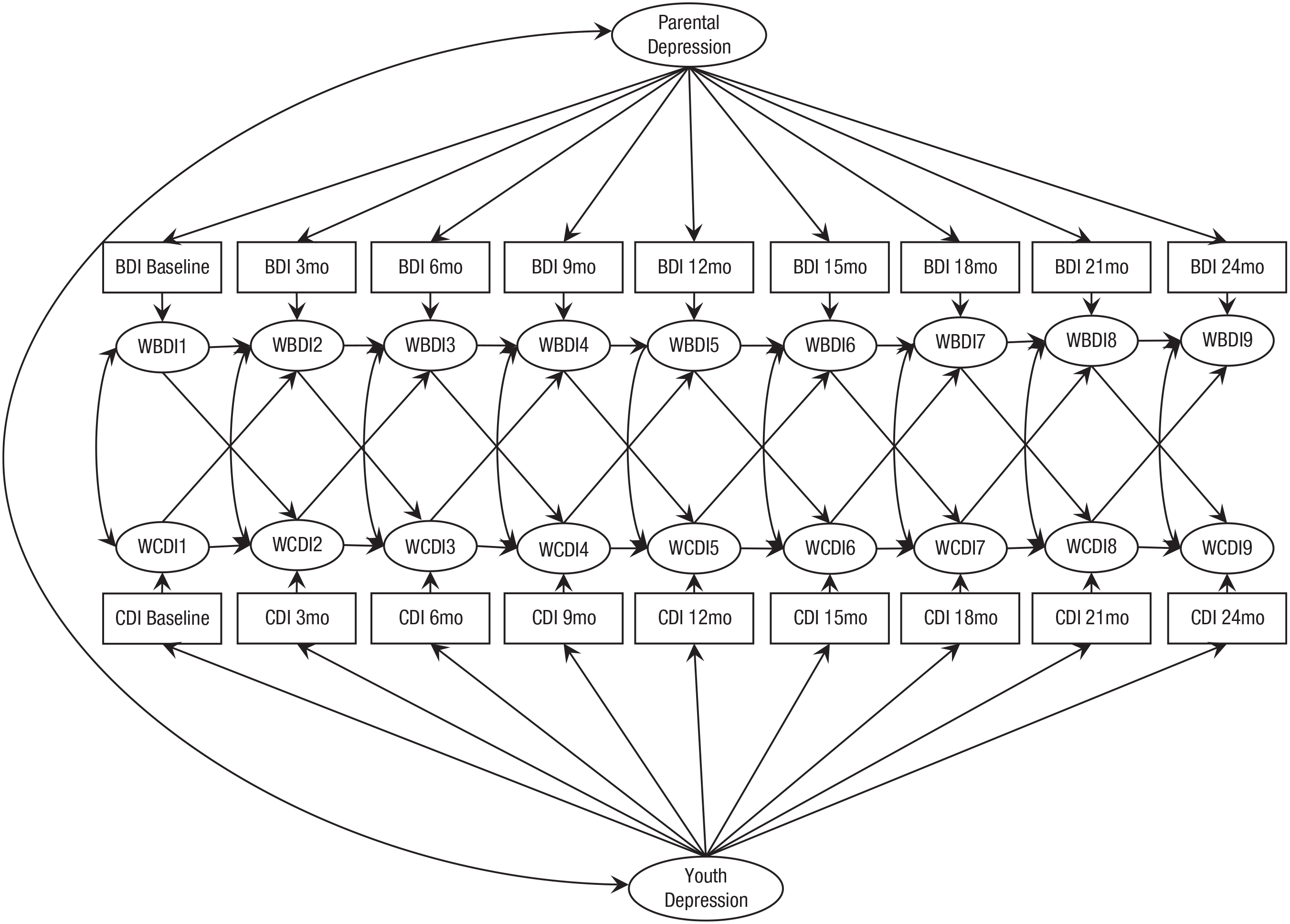
Random intercept cross-lagged panel model (RI-CLPM) examining reciprocal patterns of within-dyad associations of parents’ and adolescents’ depressive symptoms over time, as implemented in Study 1. The RI-CLPM implemented in Study 2 is conceptually identical to the model described in the above figure, with the addition of four additional time points of observed data from the Children’s Depression Inventory (CDI; Kovacs, 2003) and the Beck Depression Inventory (BDI-II; Beck et al., 1996) that were loaded onto their respective random intercept factors as well as onto individual latent factors used to model within-persons/dyads patterns of change over time. Children’s depressive symptoms were assessed using the CDI; parents’ depressive symptoms were assessed using the BDI-II.
Sensitivity analyses
To account for potential effects of seasonality on parents’ and adolescents’ depressive symptoms (e.g., Harmatz et al., 2000; Nillni et al., 2009), we conducted additional sensitivity analyses in which all within-persons latent factors were regressed on to month of assessment. In addition, site, parents’ and children’s age and gender identity, and parental level of education were included as between-persons covariates to account for potential effects of site and demographic characteristics in contributing to patterns of effects.
Multiple group analyses
To evaluate whether patterns of effects varied according to adolescents’ gender or parents’ history of depressive episode, we conducted multiple group models. One set of analyses examined whether the model fit equally well across parental diagnostic history groups (i.e., no parental history of depression vs. parental history of at least one lifetime depressive episode). Separate multiple group analyses were also conducted to examine whether the model fit equally well across adolescents’ genders. Each multiple group analysis proceeded according to the following steps. First, we specified a model in which all within-dyads, prospective cross-lagged paths were constrained to be equal across groups (e.g., parents with and without a history of depressive episode, boys and girls). Next, we specified a model in which all cross-lagged paths were allowed to vary between groups. We then compared the fully constrained model with the relatively unconstrained model using χ2 difference tests as well as multiple fit indices, including change in RMSEA and CFI. Models were determined to be invariant if the χ2 difference test was not significant and/or comparison across multiple fit indices indicated equivalent fit, including change in Akaike information criterion (AIC) and Bayesian information criterion (BIC). Lower AIC and BIC values indicate better fit. ΔRMSEA no higher than .015, ΔCFI no higher than .01, and ΔAIC/BIC no higher than 10 were applied as criteria indicating relative equivalence in model fit (Chen, 2007; Cheung & Rensvold, 2002).
Results
Preliminary analyses
Means and standard deviations for all assessments of parental and adolescent depression are reported in Table 1. Gender differences in adolescents’ depressive symptoms were inconsistently observed; differences generally demonstrated higher levels of depression among girls. Parental symptom scores did not vary according to adolescents’ gender at any assessment point. Across assessment points, an average of 12.19% of youths and 12.19% of parents reported depressive symptoms scores in the clinically significant range according to cutoff values of CDI of at least 16 (Timbremont et al., 2004) and BDI of at least 14 (Beck et al., 1996), respectively. 1 At the time of study enrollment, 3.7% of youths were currently receiving psychotherapy or antidepressant treatment according to parental report; 15.9% of parents reported having received psychotherapy at some time in their life.
Study 1: Primary Variables of Interest
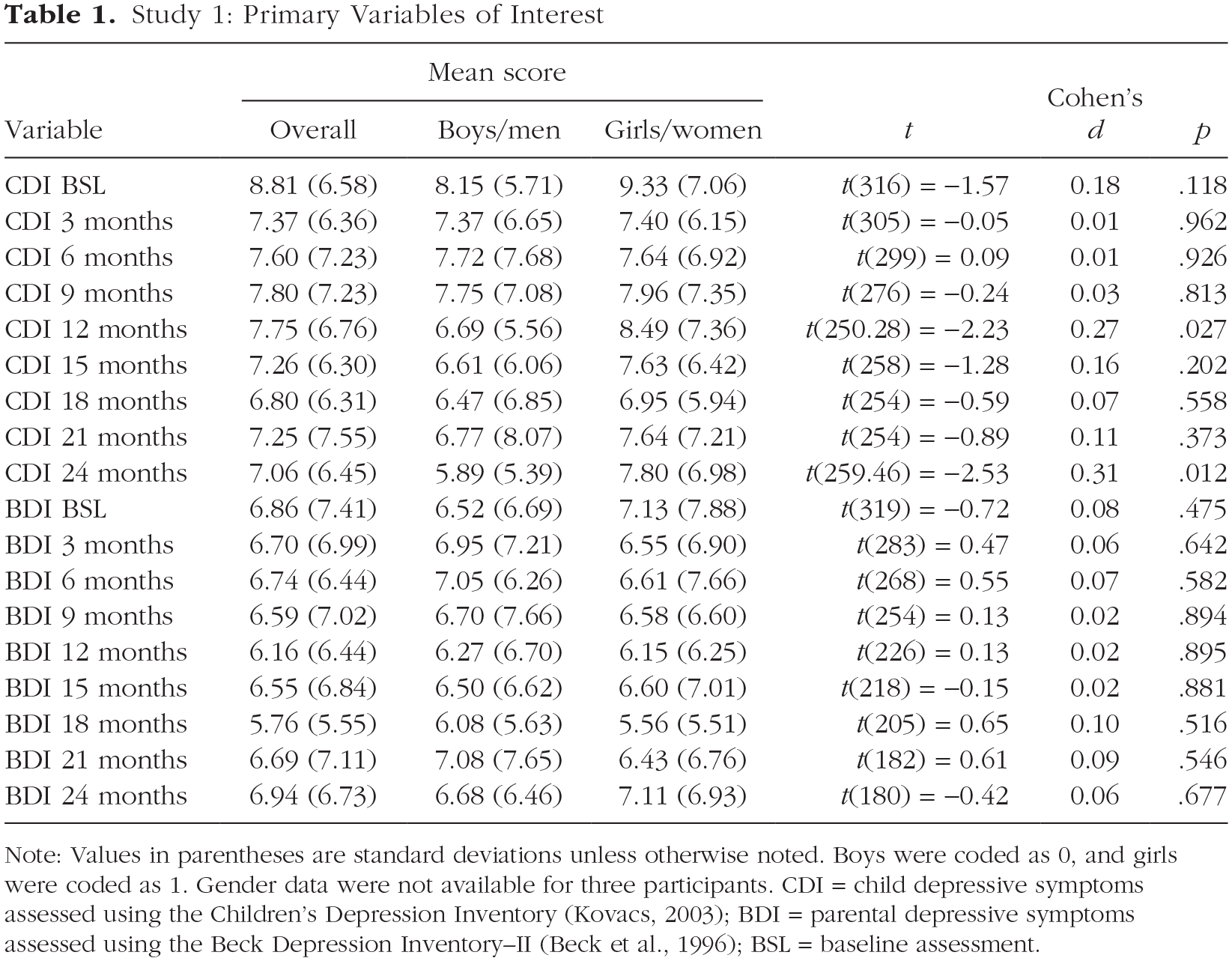
Note: Values in parentheses are standard deviations unless otherwise noted. Boys were coded as 0, and girls were coded as 1. Gender data were not available for three participants. CDI = child depressive symptoms assessed using the Children’s Depression Inventory (Kovacs, 2003); BDI = parental depressive symptoms assessed using the Beck Depression Inventory–II (Beck et al., 1996); BSL = baseline assessment.
Intraclass correlations (ICCs) quantifying between-persons and within-persons sources of variance in parents’ and adolescents’ depressive symptoms indicated that 49.2% of the variance in child depression (ICC = .51) and 34.4% of the variance in parental depression (ICC = .66) could be attributed to within-persons differences. Bivariate correlations (r) between parents’ and adolescents’ depressive symptoms at any given time point ranged in magnitude from .04 to .19 and were not consistently different from zero. A full correlation matrix describing bivariate correlations between all parents’ and children’s depressive symptom scores is available on OSF (osf.io/t6dhf/). Parental history of depression significantly predicted youths’ odds of having experienced a depressive episode at baseline (odds ratio [OR] = 3.65, p = .001), as assessed by trained interviews using the K-SADS Present and Lifetime version (K-SADS-PL; Kaufman et al., 1996).
RI-CLPM
An RI-CLPM examining within-persons/dyads patterns of change in parents’ and adolescents’ depressive symptoms demonstrated adequate fit to the data across most fit indices, χ2(145) = 304.80, CFI = .93, RMSEA = 0.06, SRMR = 0.11. Random intercept factors capturing between-persons/dyads variance in parental and adolescent depression were positively correlated (β = 0.14, b = 3.56, SE = 1.68, p = .034) such that individual differences in parent trait-like depression were associated with individual differences in offspring trait-like depression. Results of within-persons/dyads analyses are reported in Table 2. Both parental and adolescent depression demonstrated autoregressive stability over time (b = 0.24, p < .001 and b = 0.29, p < .001, respectively) such that deviations from an individual’s expected depression score at time t predicted same-direction deviations in that individual’s depression at time t + 1. Within-time-points covariance estimates indicated that within-persons fluctuations in parent depression were positively related to contemporaneous within-persons fluctuations in offspring depression (b = 1.06, p = .055). In contrast, no within-dyads cross-lagged associations were observed; fluctuations in parental depression at time t did not predict fluctuations in adolescent depression at time t + 1 (b = 0.03, p = .432), nor did fluctuations in adolescent depression at time t predict fluctuations in parental depression at time t + 1 (b = 0.03, p = .449).
Study 1: Random Intercept Cross-Lagged Panel Model Results Describing Patterns of Within-Persons/Dyads Change

Note: Values in parentheses are standard errors. Paths represent the prospective association between parents’/adolescents’ depressive symptoms at any time t with parents’/adolescents’ symptoms at time t + 1 across all nine time points. CDI = child depressive symptoms assessed using the Children’s Depression Inventory (Kovacs, 2003); BDI = parental depressive symptoms assessed using the Beck Depression Inventory–II (Beck et al., 1996); b = unstandardized coefficient; CI = confidence interval.
Multiple group models
Complete model-fit statistics for all multiple group models, including fully constrained and relatively unconstrained model-fit statistics, are reported in Table S2 in the Supplemental Material available online. Regarding group differences based on parental history of depression, a fully constrained model in which cross-lagged associations were constrained to be equal across parental diagnostic groups demonstrated adequate fit that was not worse than a model in which cross-lagged associations were free to vary across groups (Δχ2 = 0.44, Δdf = 2, p = .80, ΔCFI = .001, ΔRMSEA = 0.001), indicating that prospective within-dyads associations between parental and adolescent depression did not differ on the basis of parental history of depression. Regarding group differences based on adolescents’ gender, the fully constrained and relatively unconstrained models did not significantly differ from one another in terms of model fit (Δχ2 = 0.08, Δdf = 2, p = .96, ΔCFI = .001, ΔRMSEA < 0.001). Thus, results suggest that within-dyads patterns of cross-lagged associations did not differ on the basis of adolescents’ gender. 2
Sensitivity analysis
Patterns of results held after accounting for effects of month of assessment, recruitment site, parental educational attainment, and parents’ and children’s gender identity and age at baseline (see Table S4 in the Supplemental Material).
Comparison with CLPM
In response to interested reviewers, we additionally fit a traditional CLPM to study data with constraints applied in an analogous fashion to those described regarding the RI-CLPM but without the addition of random intercept factors accounting for between-persons/dyads trait-like variance. The result of this analysis demonstrated poor fit to the data (CFI = .82, RMSEA = 0.09, SRMR = 0.17), and model fit was significantly worse than for the RI-CLPM (Δχ2 = 84.53, Δdf = 3, p < .001, ΔCFI = .11, ΔRMSEA = 0.03). Model parameters are reported in Table S5 in the Supplemental Material. Cross-lagged paths were not significantly different from zero, although poor fit statistics indicate that caution is needed in interpretation because estimates may not be reliable.
Discussion
We used an RI-CLPM approach to appropriately partition between-sources variance and within-sources of variance, and the results of Study 1 suggest that associations between parents’ and adolescents’ depressive symptoms are driven by between-dyads individual differences rather than prospective within-dyads reciprocal change processes. Consistent with a wealth of previous research (see Goodman, 2020; Gotlib et al., 2020), results support concordance in trait-like depression levels between parents and offspring such that elevated levels of trait parental depression were associated with elevated levels of offspring depression. In addition, a small, positive contemporaneous association between parents’ and children’s depression was observed at the within-dyads level. However, contrary to hypotheses, dynamic fluctuations in parental depression did not prospectively predict future fluctuations in adolescent depression or vice versa. Moreover, patterns of results held across adolescents’ gender groups and across dyads with and without a parental history of depression. Overall, findings suggest that among parents and their adolescent youths, longitudinal coupling of depression occurs via largely stable individual difference mechanisms, as well as contemporaneous processes of cofluctuation, rather than prospective reciprocal change processes manifesting at the within-dyads level per se. That is, results are suggestive of some level of depressive contagion or social learning of depression manifesting on a microlevel, contemporaneous time scale; however, these contagion or social learning processes do not appear to explain within-dyads patterns of reciprocal change over time.
After accounting for divergent sources of variance in parents’ and adolescents’ depressive symptoms, expected between- and within-persons associations were noted to emerge, although hypothesized longitudinal within-dyads patterns of relations were not observed. Specifically, results supporting within-persons stability and between-persons covariance between parents’ and adolescents’ depressive symptoms align with what is known about depression—that depression is highly stable, even at subthreshold levels, in both adolescents and adults (e.g., Merikangas et al., 2003; Tram & Cole, 2006) and tends to cluster in parent–child dyads (Goodman, 2020; Hammen, 1991). That within-dyads cross-lagged associations were not observed, although inconsistent with some previous research (e.g., Ge et al., 1995; Hughes & Gullone, 2010; but see Ciciolla et al., 2014; Mennen et al., 2018), may be reflective of the analytic strategy we used to accurately separate between-dyads from within-dyads effects in the present work relative to existing studies. Indeed, most previous studies supporting reciprocal relations between parental and adolescent symptoms relied on traditional CLPMs, with potentially misleading results (Hamaker et al., 2015). As demonstrated by a number of recent studies, the application of statistically advanced models, such as RI-CLPMs, may clarify patterns of prospective, within-persons/dyads patterns of relations, particularly in literatures littered with mixed findings and competing theoretical models (e.g., Barzeva et al., 2020; Keijsers, 2016; Long et al., 2019; Masselink et al., 2018).
Given that some of the main study findings were unexpected a priori, particularly the nonsignificance of longitudinal within-dyads cross-lagged associations, conclusions of Study 1 must be considered tentative. We sought to replicate these patterns to confidently interpret results and make more definitive conclusions. Accordingly, similar data (sample, method, design, analyses) from Study 2 were analyzed to replicate and extend results from Study 1 in an independent sample of parent–adolescent dyads.
Study 2
In Study 2, we aimed to evaluate within-dyads patterns of reciprocal associations between parents’ and children’s depressive symptoms using an RI-CLPM approach in an independent, moderately sized sample of adolescents and their parents assessed via self-report measures of depression every 3 months for a period of 3 years (13 total assessment points). Youths included in Study 2 included both middle school and high school age youths, extending the scope of the present inquiry to include older adolescents. Given findings observed in Study 1, we hypothesized that random intercepts representing trait-like variance in parental and adolescent depression would be positively correlated and that within-persons’ parents’ and adolescents’ depressive symptoms would demonstrate autoregressive stability over time. Moreover, we expected to observe positive contemporaneous associations between parents’ and children’s deviations in depression at the within-persons/dyads level. In contrast, we hypothesized that no prospective within-dyads cross-lagged associations would be found; we did not expect within-persons fluctuations in parents’ level of depression to predict within-persons fluctuations in their adolescents’ level of depression, or vice versa, over time. Consistent with our previous analyses, we examined whether patterns of cross-lagged effects differed across adolescents’ genders or according to parental history of depression. Informed by our previous findings, we expected patterns of results to be replicated across genders and parental diagnostic groups. That is, we expected no differences in patterns of cross-lagged associations across these groups.
Method
Participants and procedures
Participants in Study 2 included 435 parent–adolescent dyads recruited from the greater Denver, Colorado, and central New Jersey areas in association with the Genes, Environment, and Mood study (Hankin et al., 2015). Participants included in the present analyses represent a subset of sixth- and ninth-grade youths recruited as part of this larger study to more directly replicate analyses conducted in Study 1. In instances in which parents participated with more than one child, one sibling was randomly chosen to be included in the present analyses, as in the previous study. Participating youths ranged in age from 10 to 16 at baseline (M = 13.41 years, SD = 1.55; 57% girls). Racial demographics were approximately representative of the broader U.S. population at the time of sampling, although individuals identifying as Latinx were relatively underrepresented (66.7% European American, 12.2% African American/Black, 9.7% Asian/Pacific Islander, 0.5% American Indian/Alaskan Native, 11% multiracial or identifying with another racial group; 11% of participants reported a Latinx ethnic identity). Participating parents were primarily women (92.5%; age: M = 45.08 years, SD = 6.56; 85.1% biological mothers). Regarding educational attainment, 58.6% of participating parents reported having completed a bachelor’s degree or higher. Median family income was approximately $90,000 according to parental report.
All procedures were approved by the institutional review boards at the University of Denver and Rutgers University. Upon enrolling in the study, participants completed a baseline laboratory visit, during which parents provided informed consent and youths provided informed assent to participation in the study. Parents’ and adolescents’ depressive symptoms were subsequently assessed every 3 months for a period of 3 years via self-report on the BDI-II (Beck et al., 1996) and CDI (Kovacs, 2003), respectively, yielding a total of 13 possible assessments. Similar to Study 1, parental and adolescent baseline and 18- and 36-month depression assessments were completed at the same time as one another; follow-up assessments were completed from home and requested to be returned within a specified 2-week period. The majority completed measures on the same day; the modal difference in the number of days between caregivers’ and children’s assessment was 1, and the mean difference in the number of days was 3.35 (SD = 5.2). The mean number of assessments completed was 10.61 (SD = 3.51). Number of assessments completed was negatively correlated with age (r = −.11, p = .03) and adolescents’ depressive symptoms at baseline (r = −.19, p < .001). Number of assessments completed was not related to adolescents’ gender (r = .06, p = .23). Parents completed a diagnostic interview measure (i.e., the SCID; First et al., 2002) to evaluate lifetime history of depressive disorder.
Measures
Demographics
Relevant demographic information was obtained using parental self-report on a brief demographic information questionnaire, similar to that described in Study 1. As in Study 1, gender identity was representing using a dichotomous variable reflection boy/man (0) or girl/woman (1) gender identity.
SCID
Parental history of depression before enrollment in the study was assessed using the SCID (First et al., 2002). Full details concerning interviewing training and supervision are reported elsewhere (see Hankin et al., 2015). As in Study 1, history of caregiver depression was represented using a dichotomous score indicating presence of caregiver lifetime definite MDD, probable MDD, or definite mDD following criteria described in the DSM-IV (American Psychiatric Association, 2000). In total, 121 (27.8%) parents reported an onset of depression occurring before enrollment in the study.
CDI
Youths’ depressive symptoms were measured at each assessment point via self-report on the CDI (Kovacs, 2003). Internal consistency ranged from α = .79 to .90 across assessment points, indicating good reliability.
BDI-II
Parental depressive symptoms were similarly measured at each assessment point via self-report on BDI-II (Beck et al., 1996). Cronbach’s αs ranged from .89 to .94 across assessment points, indicating strong internal reliability.
Data analytic plan
As in Study 1, analyses were implemented in the lavaan package for R (R Core Team, 2018; Rosseel, 2019) using the MLR estimator and FIML estimation to account for missing data. Study hypotheses and data analytic plan for this replication effort were preregistered before data analysis.
Hypotheses were tested using an RI-CLPM approach, as described above. Model specification proceeded according to the same steps outlined in Study 1, with the addition of four additional assessment points with which to estimate reciprocal change. Multiple group models were conducted to examine group differences in cross-lagged effects according to parental history of depression and adolescents’ gender, as described in Study 1, and sensitivity analyses were conducted to evaluate robustness of effects covarying for month of assessment, site, and relevant demographic characteristics, as described above.
Results
Preliminary analyses
Means and standard deviations for all assessments of parental and adolescent depression are reported in Table 3. When gender differences in adolescents’ depressive symptoms were observed, girls were found to report higher symptom levels than boys, consistent with prior research. As in Study 1, parental symptom scores did not vary according to adolescents’ gender at any assessment point. Across assessment points, an average of 4.84% of youths and 12.61% of parents reported depressive symptoms scores in the clinically significant range according to cutoff values of 16 or greater for CDI (Timbremont et al., 2004) and fourteen or greater for BDI 14 (Beck et al., 1996), respectively. 3 Among adolescent participants, 21.6% of youths reported having received some form of treatment over the course of the study. Among parents, information regarding psychological treatment history was collected only among individuals reporting high levels of symptoms on the SCID (n = 164); of these parents, 67.1% reported having received psychopharmacological, psychotherapeutic, and/or inpatient treatment at some time during their life.
Study 2: Primary Variables of Interest

Note: Values in parentheses are standard deviations unless otherwise noted. Boys were coded as 0, and girls were coded as 1. CDI = child depressive symptoms assessed using the Children’s Depression Inventory (Kovacs, 2003); BDI = parental depressive symptoms assessed using the Beck Depression Inventory–II (Beck et al., 1996); BSL = baseline assessment.
ICCs indicated that 46.5% of the variance in children’s depression (ICC = .54) and 41.9% of the variance in parental depression (ICC = .58) could be attributed to within-persons differences. Bivariate correlations (r) between parents’ and adolescents’ depressive symptoms at any given time point ranged in magnitude from .12 to .27. A full correlation matrix describing bivariate correlations between all parents’ and adolescents’ depressive-symptom scores is available on OSF (https://osf.io/swbc2/). Parental lifetime history of depression significantly predicted youths’ odds of having experienced a depressive episode at baseline, as assessed using the K-SADS-PL (OR = 3.99, p = .028).
Given that youths were recruited in distinct grade cohorts, multiple group models were conducted to evaluate potential grade differences in patterns of effects. Results indicated that a model in which cross-lagged paths were constrained to be equal across grade cohorts fit equivalently well relative to a model in which cross-lagged paths were permitted to vary, Δχ2(2) = 0.26, p = .880, ΔCFI = .001, ΔRMSEA < 0.001, indicating invariance across grades. Thus, data from both grade cohorts were combined in all analyses to maximize statistical power.
RI-CLPM
An RI-CLPM examining within-persons/dyads patterns of change in parents’ and adolescents’ depressive symptoms demonstrated adequate fit to the data across most fit indices, χ2(317) = 597.86, CFI = .93, RMSEA = 0.05, SRMR = 0.09. Random intercept factors capturing between-persons variance in parental and adolescent depression were positively correlated (β = 0.27, b = 5.15, SE = 1.25, p < .001) such that individual differences in parental trait-like depression were associated with individual differences in offspring trait-like depression. Results of within-persons/dyads analyses are reported in Table 4. Both parental and adolescent depression demonstrated autoregressive stability over time (b = 0.17, p < .001 and b = 0.23, p < .001, respectively) such that deviations from an individual’s expected depression score at time t predicted same-direction deviations in that individual’s depression at time t + 1. Within time-point covariance, estimates indicated that within-persons fluctuations in parental depression were positively related to contemporaneous within-persons fluctuations in offspring depression (b = 1.57, p < .001). In contrast, no prospective within-dyads cross-lagged associations were observed; fluctuations in parental depression at time t did not predict fluctuations in adolescent depression at time t + 1 (b = −0.04, p = .138), nor did fluctuations in adolescent depression at time t predict fluctuations in parental depression at time t + 1 (b = 0.01, p = .557).
Study 2: Random Intercept Cross-Lagged Panel Model Results Describing Patterns of Within-Persons/Dyads Change

Note: Values in parentheses are standard errors. Paths represent the prospective association between parents’/adolescents’ depressive symptoms at any time t with parents’/adolescents’ symptoms at time t + 1 across all nine time points. CDI = child depressive symptoms assessed using the Children’s Depression Inventory (Kovacs, 2003); BDI = parental depressive symptoms assessed using the Beck Depression Inventory–II (Beck et al., 1996); b = unstandardized coefficient; CI = confidence interval.
Multiple group models
Complete model-fit statistics for multiple group models, including fully constrained and relatively unconstrained model-fit statistics, are reported in Table S7 in the Supplemental Material. Regarding group differences based on parental history of depression, a fully constrained model in which cross-lagged associations were constrained to be equal across parental diagnostic groups fit no worse than a model in which cross-lagged associations were free to vary across groups (Δχ2 = 4.91, Δdf = 2, p = .09, ΔCFI = .001, ΔRMSEA < 0.001), indicating that prospective within-dyads associations between parental and adolescent depression did not differ on the basis of parental history of depression. Regarding group differences based on adolescents’ gender, a χ2 difference test indicated that the relatively unconstrained model fit the data slightly better than the fully constrained model (Δχ2 = 6.26, Δdf = 2, p = .04); however, models were equivalent according to ΔCFI = .001, ΔRMSEA < 0.001. Differences in AIC and BIC values similarly demonstrated equivalent fit across models (ΔAIC = 4.36, ΔBIC = 2.55). Thus, results suggest that within-dyads patterns of cross-lagged associations did not differ on the basis of adolescents’ gender. 4
Sensitivity analysis
As in Study 1, patterns of results held after accounting for effects of month of assessment, recruitment site, parental educational attainment, and parents’ and children’s gender identity and age at baseline (see Table S9 in the Supplemental Material).
Comparison with CLPM
As in Study 1, a traditional CLPM was also fit to the data. Model fit for this CLPM was poor (CFI = .71, RMSEA = 0.09, SRMR = 0.25) and significantly worse than that of the RI-CLPM (Δχ2 = 430.29, Δdf = 3, p < .001, ΔCFI = .22, ΔRMSEA = 0.04). Model parameter estimates are provided in Table S10 in the Supplemental Material. Cross-lagged paths from parents’ to children’s depression (b = 0.03, p = .002) and from children’s to parents’ depression (b = 0.04, p = .046) were significant, although caution is needed in interpretation given poor model fit.
Discussion
Results of Study 2 replicated and extended findings from Study 1 in an independent sample of parent–adolescent dyads. As hypothesized, random intercepts representing parents’ and adolescents’ between-persons, trait-like levels of depression were positively related, and the effect size was consistent with effects observed in Study 1 as well as in previous meta-analytic findings (Goodman et al., 2011). Positive within-persons autoregressive stability paths were also observed for both parents and adolescents, and effect sizes were similar to those observed in Study 1. Moreover, positive contemporaneous within-persons/dyads associations between parent–offspring depression indicate that within time points, parental and adolescent levels of depression cofluctuate with one another such that deviations from a parent’s expected level of depression at a given time point are associated with same-direction deviations in their adolescent’s expected level of depression at that time point, as suggested in Study 1. Consistent with hypotheses, no prospective cross-lagged associations were observed; within-dyads fluctuations in parental depression did not predict future fluctuations in their offspring’s depression. Patterns of effects held across girls and boys as well as dyads with and without a parental history of depression.
General Discussion
Interest in understanding mechanisms contributing to risk for depression among children of depressed parents has inspired a robust literature as well as a number of plausible hypotheses concerning the pathways by which risk is conferred (Goodman, 2020; Goodman & Gotlib, 1999; Gotlib et al., 2020). In the present series of studies, we aimed to evaluate the hypothesis that within-persons fluctuations in parents’ and adolescents’ depressive symptoms demonstrate prospective patterns of reciprocal relations at the within-dyads level. Results of Study 1 and Study 2 converge to suggest that between-persons/dyads individual differences and contemporaneous within-dyads effects at the same time point, and not prospective cross-lagged within-dyads change processes, characterize the longitudinal coupling of depressive symptoms among parents and adolescents across months-long time scales. Using an RI-CLPM approach that is appropriately suited to accurately disentangle between-sources of variance and within-sources of variance in prospective relations between parents’ and adolescents’ depressive symptoms, we found that these two independent samples yielded remarkably similar results. Parental and adolescent symptoms covary at the between-dyads level such that parents high in depressive symptoms relative to other parents are likely to have adolescents who exhibit high levels of depressive symptoms relative to other adolescents. Within-persons fluctuations in parental and adolescent depression also covary contemporaneously such that idiographic deviations in a parent’s depression (i.e., fluctuations around their own individual average) are related to same-direction deviations in their offspring’s depression at a given point in time. However, within-persons fluctuations in parents’ depression do not prospectively predict within-persons fluctuations in adolescents’ depression, or vice versa, over time. In both samples, results held across boys and girls as well as across dyads with and without a parental history of depression.
Across both studies, expected patterns of between-persons and within-persons autoregressive associations were supported by RI-CLPM results. Specifically, positive correlations between parental and adolescent random intercept factors align with a wealth of literature demonstrating familial clustering of depressive symptoms (Cicchetti, 1993; Cicchetti & Rogosch, 2002) and suggest that trait-like levels of depression covary among parents and their adolescent offspring. Moreover, effect sizes describing these associations in the present work are largely consistent with those indicated by meta-analytic findings, which demonstrate modest but significant associations between parents’ depression and children’s internalizing symptoms, with a mean effect size (r) of approximately .21 (Goodman et al., 2011), providing additional confidence in results. Furthermore, observed within-persons autoregressive stability of dyad members’ depressive symptoms aligns with research suggesting that symptoms of depression are highly stable across both adolescence and adulthood (e.g., Merikangas et al., 2003; Tram & Cole, 2006). Thus, findings reflect expected, reliable trends observed across the broader literature.
Leveraging advances in statistical modeling, in the present work, we advance knowledge of longitudinal coupling of parents’ and adolescents’ depressive symptoms by demonstrating that after accounting for between-dyads sources of variance, parental and adolescent depression demonstrate contemporaneous cofluctuations but do not demonstrate within-persons/dyads reciprocity over time. That is, at any given assessment point, incremental changes in a parent’s depression relative to their own idiographic mean were related to same-direction within-persons fluctuations in their adolescent’s depression, consistent with tenets of social learning and depressive contagion theories (Bandura, 1977; Coyne, 1976; Hames et al., 2013; Hatfield et al., 1993). Across 3 months, however, fluctuations in parents’ depression relative to their own means do not predict within-persons fluctuations in adolescents’ depression, or vice versa, suggesting that social learning and contagion processes may be operant across temporally brief (e.g., hours, days) time scales, but effects of social learning or depressive contagion processes may attenuate over the course of several months. This pattern of findings aligns with previous research by Gjerde et al. (2017) demonstrating contemporaneous but not prospective associations between parental depression and offspring internalizing symptoms among a large sample of preschool age youths. Null findings with respect to prospective cross-lagged, within-persons/dyads effects suggest that varying mechanisms of risk may be differentially salient across diverse developmental time scales, consistent with a developmental psychopathology framework emphasizing the role of developmentally contextualized, multiple pathways in contributing to adolescent risk (Cicchetti, 1993; Cicchetti & Rogosch, 2002).
Indeed, differences between the present results and previous findings by Kouros and Garber (2010) may be attributed to issues of time scale. In a sample of parent–adolescent dyads assessed annually across a period of 6 years, Kouros and Garber (2010) applied a rigorous analytic strategy to demonstrate longitudinal coupling between parents’ and children’s depressive symptoms such that within-persons change in parental depression was associated with within-persons change in adolescent depression across periods of 1 year. That such coupling was observed on the order of years in work by Kouros and Garber (2010), but not months in the present study, again highlights the salience of time scale in processes of depressive risk transmission and supports a multiple pathways perspective. Thus, the present work complements previous findings by further refining the time scale on which varying mechanisms of risk may unfold. On the scale of years, for example, the accumulation of life stress may contribute to co-occurring escalations in parent–offspring depression given the role of stress as both a risk factor for and consequence of depressive symptoms among both adolescents (e.g., Cole et al., 2006; Jenness et al., 2019) and adults (see Hammen, 2005, 2006). It is also possible that the magnitude of change represented by within-persons symptom fluctuations varies across divergent time scales. That is, relatively large fluctuations in parental depression, which unfold over the course of a year or more, may be needed to elicit prospective fluctuations in adolescents’ depression and vice versa. Further clarifying which mechanisms are active when and across what time scales represents a key area for ongoing research.
Differences between present results and other previous research (e.g., Ge et al., 1995; Hughes & Gullone, 2010) may be attributed to differences in both time scale and analytic approach. Ge et al. (1995), for example, used a traditional CLPM approach to demonstrate reciprocal associations between parental and adolescent distress as assessed annually across a 3-year period. Hughes and Gullone (2010) also tested hypotheses concerning bidirectional relations between parental and adolescent internalizing symptoms using traditional CLPM, demonstrating reciprocity in dyad members’ symptoms across 6 months. Traditional CLPMs conflate within- and between-sources of variance, rendering them ill-equipped to rigorously evaluate within-dyads patterns of relations and therefore clarify within-dyads mechanisms of depressive contagion (Hamaker et al., 2015). In the present work, CLPMs demonstrated poor fit to the data and yielded patterns of estimates that diverged both from one another and the better fitting RI-CLPMs. In the case of Study 2, results of CLPM may have contributed to Type I error, yielding inaccurate conclusions regarding the prospective relations between parents’ and children’s depression. Comparisons across these models in the present work converge with results of simulation studies (e.g., Hamaker et al., 2015) to suggest that results of traditional CLPM may be misleading in nature and to highlight the need to reevaluate patterns of relations using appropriately rigorous statistical models.
Strengths and limitations
The present work demonstrates a number of strengths that advance knowledge of within- and between-dyads patterns of association between parental and adolescent depression. Across both samples included in the present work, dyad members’ depressive symptoms were assessed every 3 months for a period of years, permitting rigorous analysis of autoregressive and cross-lagged associations as they unfold a period of several months. Moreover, hypotheses were tested using a sophistocated analytic strategy that was appropriately equipped to disambiguate within-sources of variance from between-sources of variance, representing a methodological improvement on previous work conducted within a traditional CLPM framework. Note that study aims were addressed, and results were replicated across, two independent samples of parent–adolescent dyads. This is particularly important given that primary results of Study 1 were unexpected a priori and is consistent with efforts to promote replicability and open science practices in the field of clinical psychology (Tackett et al., 2017).
Findings must also be interpreted in the context of several limitations, which represent important directions for future research. The present study design permitted analyses of contemporaneous as well as cross-lagged associations between within-persons fluctuations in parent–offspring depression as they occur across 3-month intervals; however, contemporaneous findings do not provide information regarding the directionality of effects. Research is needed to evaluate patterns of reciprocal within-persons/dyads change processes in parent–offspring depression as they unfold across microlevel time scales (e.g., hours, days) to elucidate directions of effects and further clarify mechanisms of risk. Research is also needed to account for potential third variables that, although outside the scope of the present investigation, may have influenced observed patterns of effects, including parenting styles, adolescent externalizing symptoms, and other contextual factors (e.g., broader family functioning and dynamics). More broadly, it is possible that patterns of findings observed in the present work were influenced by unmeasured genetic factors, including both genetic similarities between parents and offspring and passive gene-environment correlations (e.g., Harold et al., 2011; Reiss et al., 1995; Silberg et al., 2010). Genetically informed designs are needed to appropriately disaggregate genetic factors from environmental factors contributing to risk for depression among children of depressed parents.
Additional limitations relate to the generalizability of the present findings. Specifically, youths were sampled during a specific developmental stage; it is possible that younger children, for example, may be more sensitive to fluctuations in their parents’ depressive symptoms. Indeed, meta-analytic work has demonstrated stronger associations between parental symptoms and youths’ psychopathology among younger children relative to adolescents (Goodman et al., 2011), highlighting the need for research evaluating reciprocal associations between parents’ and children’s depression using appropriate statistical methods (e.g., RI-CLPM) among primary school age youths. No group differences were detected in patterns of effects on the basis of parental history of depression; however, participating youths represent adolescents sampled from the general community with relatively low levels of self-reported depression. Research is needed to evaluate patterns of effects among youths with clinical levels of psychopathology. Moreover, although approximately representative of the racial and ethnic composition of the communities from which they were recruited, samples across both studies included predominantly White, non-Latinx parent–adolescent dyads, limiting generalizability of findings. Future research should aim to examine transactional, within-dyads change processes as they unfold in samples of parent–adolescent dyads with more diverse racial, ethnic, and social identities. Note that equality constraints applied in the present study analyses, although providing parsimonious and reliable estimates of within-dyads effects, necessarily limit insight into the ways in which the strength of within-dyads associations may or may not change over time. Future studies with larger samples are needed to evaluate whether effect sizes meaningfully differ across successive measurement occasions to better describe longitudinal patternings in prospective within-dyads relations.
Larger samples are also needed to replicate multiple group model results given relatively limited numbers of parents with a history of depression included in the present work. It is likely that group comparisons in the present work were insufficiently powered to detect modest differences in effect size, and future work should include a priori power analyses to ensure sufficient power to detect group differences. Finally, only one parent for each child was included in the present study, predominantly mothers; it is critical that future work includes both mothers and fathers because previous work indicates that maternal and paternal depression may relate to youths’ depression in differing and interactive ways (Natsuaki et al., 2014).
Clinical implications
Results of the present study indicate that prevention efforts aimed at reducing adolescent risk for psychopathology would be well served to attend to between-dyads contextual factors influencing both parents’ and adolescent’s depression risk. In addition, interventions may wish to target parent–adolescent interactional processes unfolding on microsocial time scales, which may contribute to contemporaneous contagion of parents’/adolescents’ depressive experience. Parental expression of negative, conflictual affective behavior during interactions with youths, for example, has been linked to contemporanous decreases in adolescents’ momentary experience of positive affect in daily life (Griffith et al., 2018) as well youths’ prospective risk for an onset of depression (Griffith et al., 2019; Schwartz et al., 2014). Likewise, recent research suggests that augmenting youths’ interpersonal functioning through a skills-based preventitive intervention program may have downstream effects of parental depressive symptoms (Spiro-Levitt et al., 2019).
Conclusions
The present work employed an RI-CLPM approach to evaluate prospective, within-dyads relations between parental and adolescent depression. Findings across two independent samples converged to suggest that associations between parents’ and adolescents’ depressive symptoms covary on a between-persons level and demonstrate within-persons cofluctuation on a contemporaneous time scale; however, within-persons fluctuations in parental depression do not predict associated within-persons fluctuations in adolescent depression over a period of several months. Overall, results highlight the salience of time scale to inquiries of depressive risk transmission and support a multiple pathways perspective for understanding the etiology of depression among children of depressed parents.
Supplemental Material
sj-pdf-1-cpx-10.1177_2167702621998313 – Supplemental material for Longitudinal Coupling of Depression in Parent–Adolescent Dyads: Within- and Between-Dyads Effects Over Time
Supplemental material, sj-pdf-1-cpx-10.1177_2167702621998313 for Longitudinal Coupling of Depression in Parent–Adolescent Dyads: Within- and Between-Dyads Effects Over Time by Julianne M. Griffith, Jami F. Young and Benjamin L. Hankin in Clinical Psychological Science
Footnotes
Acknowledgements
We thank John R. Z. Abela for the significant contributions he made to this research before his untimely death.
Transparency
Action Editor: Michael F. Pogue-Geile
Editor: Kenneth J. Sher
Author Contributions
J. M. Griffith was primarily responsible for data analysis and manuscript preparation. J. M. Griffith and B. L. Hankin conceived of the ideas and were the primary drafters of the manuscript. B. L. Hankin was the co-principal investigator on Study 1 and was responsible for its data collection. J. F. Young and B. L. Hankin were the co-principal investigators on Study 2 and were responsible for its data collection. All of the authors provided feedback on drafts of the manuscript and approved the final manuscript for submission.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.