
Abstract
Background:
Severe obesity is associated with an increased prevalence of hiatal hernias (HH) and gastroesophageal reflux disease (GERD). Both fundoplication (FP) and gastric bypass (GB) are utilized in this population, but comparative outcomes are not well-established. This review aims to compare surgical outcomes of FP versus GB for managing GERD and HH in adults with severe obesity.
Methods:
A systematic search was conducted for studies published up to June 2025. Inclusion criteria: adult patients with obesity (BMI ≥ 30) with HH/GERD undergoing first FP or GB. Key outcomes were postoperative reflux, complications, recurrence, and reoperation.
Results:
Five studies met inclusion criteria. Both FP and GB effectively manage GERD. In a propensity-matched cohort, GB significantly reduced early hernia recurrences compared to FP, but long-term recurrence and reoperation rates were similar between groups. Another study found similar recurrence rates between GB and FP; however, fewer symptomatic recurrences occurred with GB. A large retrospective study reported a lower complication rate for GB versus FP (7% vs. 10%, p < 0.05) and no significant differences in reflux scores.
Conclusions:
Both FP and GB offer benefits in managing GERD and HH in patients with severe obesity. Future research should focus on comparing efficacy, standardizing outcome measures, and evaluating patient-centered outcomes.
Introduction
According to the World Health Organization in 2022, obesity affects 1 in 8 people, which causes undesirable associated systemic diseases and negatively affects patient health and satisfaction. 1 The increasing prevalence of hiatal hernias (HH) and gastroesophageal reflux disease (GERD) is up to 20% in patients with obesity, creating challenges and debate regarding various management strategies. From a surgical standpoint, both fundoplication (FP) and gastric bypass (GB) can serve as techniques to manage HH and GERD in patients with obesity.
Numerous prospective and randomized studies in the literature report the positive outcomes associated with FP in GERD and HHs management.2–5 A consensus among researchers highlights the effectiveness of FP procedures in controlling reflux symptoms over the long term, including heartburn, regurgitation, and chronic cough. A success rate of 90% has persisted after a decade, with minimal morbidity and mortality rates recorded.6,7 However, findings concerning FP’s outcomes in patients with obesity present conflicting reports revealing higher complication and recurrence rates.8–10 Alternatively, another approach for GERD treatment supported by guidelines is GB surgery. 11 RYGB surgery has been shown to have antireflux properties that correct or improve GERD in a vast majority of patients with obesity, although a minority do continue to have symptoms or even develop de novo GERD. 11
There is a limited number of publications directly comparing FP and GB. This systematic review aims to compare surgical outcomes between FP and GB for the management of gastric reflux in adult patients with severe obesity diagnosed with HH or GERD. An important surgical outcome is postoperative reflux—a term used to describe reflux symptoms that occur after the surgical intervention, not necessarily indicating a failed procedure. 12 Studies can capture this outcome in several ways, such as the need for acid suppression medication, lack of symptom resolution, or using scoring methods and questionnaires. Additionally, surgical complications (i.e., bleeding, anastomotic leaks, and infection), recurrence of reflux symptoms, and the need for reoperation will be evaluated to understand the comparative effectiveness and safety of both interventions.
This review serves as an evidence-based tool for surgical management of reflux patients in the clinical setting, while simultaneously improving patient satisfaction through resolution of reflux symptoms without any additional complications. By systematically examining and comparing these outcomes, physicians can enhance treatment decisions and optimize patient care in the management of HH and GERD.
Methods
This review is in accordance with the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 13 An in-depth PRISMA flow diagram that summarizes the process of article screening and selection is provided (Fig. 1).
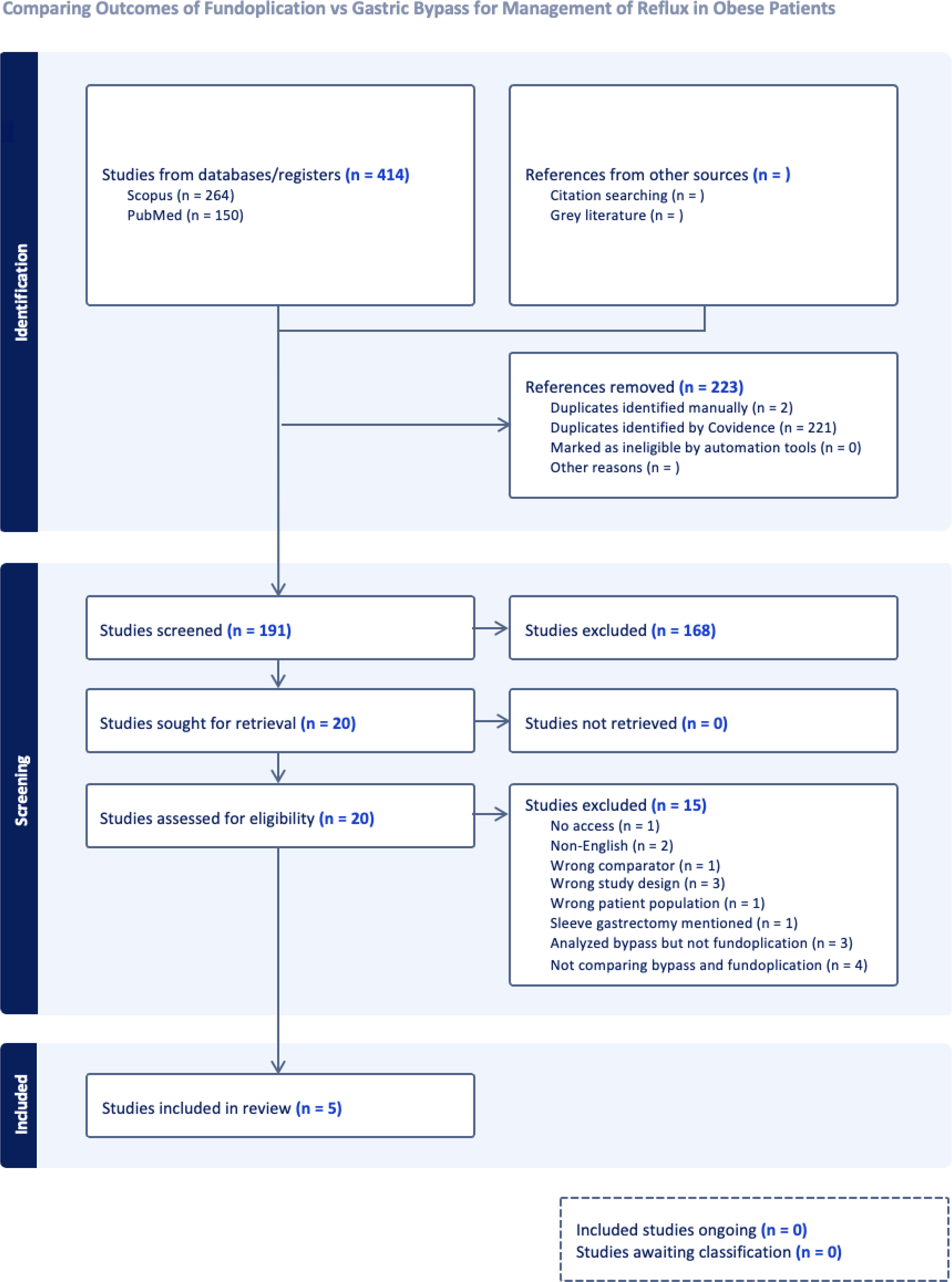
PRISMA flow diagram visually reporting the study selection process. PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Study selection and search strategy
We conducted a systematic search of literature published on Scopus and PubMed as of June 2025, as these sources can provide broad coverage of surgical literature relevant to our research question. There was no restriction on publication dates. Non-English articles were excluded. Medical subject headings terms relevant to our topic were used to generate search results. Search terms used included: “Obesity,” “Fundoplication,” “Gastric bypass,” “Reflux surgery,” “Antireflux surgery,” “Hiatal hernia surgery,” “Fundoplication outcomes,” “Gastric bypass outcomes,” “Reflux,” “GERD.”
Data extraction and synthesis
Our eligibility criteria were preimplemented into the Covidence screening and extracting tool. Two authors independently reviewed all titles, abstracts, and full text using Covidence to identify studies that are relevant to the review topic and fulfill the criteria. Disagreements were resolved by consensus or in liaison with the principal investigator. All authors had a shared understanding of the inclusion and exclusion criteria.
Eligibility criteria
Inclusion
Adult (18 years or above) patients with severe obesity (BMI 35 or above) Patients with HHs or GERD Patients who underwent their first FP of any type or GB. Studies reporting one or more of our desired outcomes comparing FP and GB:
Postoperative complications Reoperations GERD/HH recurrences
Exclusion
Patients with previous bariatric surgical history (sleeve gastrectomy, failed previous FP and/or GB, or any other bariatric procedure) Studies without any reported results or findings Non-English articles Articles without full-text access, despite attempts through institutional libraries and direct author contact Case reports Case series Editorials
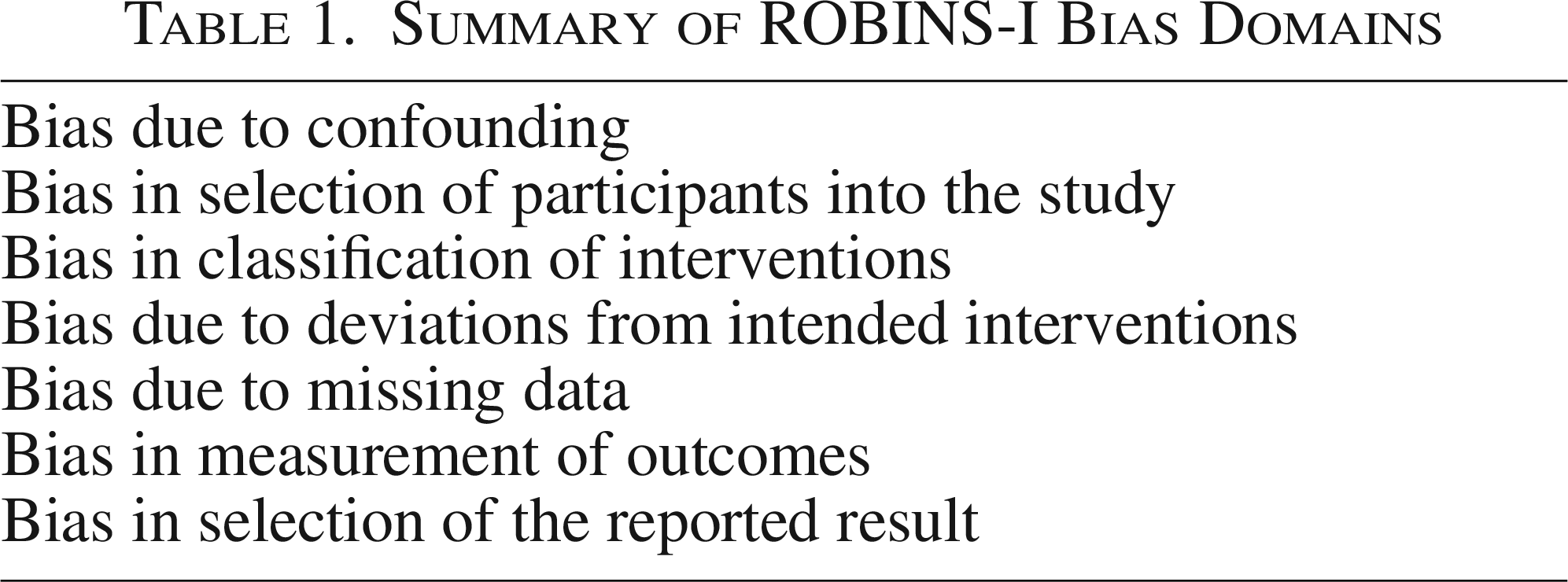
Evaluation of study quality was independently performed by two authors using the Risk Of Bias In Nonrandomized Studies—of Interventions (ROBINS-I) tool (Table 1). 13 Studies were screened to identify surgical outcomes of FP versus GB operations, as per the inclusion criteria.
Risk of bias was assessed independently by two reviewers using the ROBINS-I tool across seven domains: confounding, participant selection, intervention classification, deviations from intended interventions, missing data, outcome measurement, and selection of reported results. Each domain was rated as low, high or unclear risk of bias. Discrepancies were resolved by consensus.
Statistical analysis and quality assessment of studied
The data extraction and analysis were conducted using Covidence. Analysis of outcomes followed the principle of intention-to-treat. To analyze the comparison of FP versus GB, relative risk was calculated using the preoutlined outcomes reported in each study and total participant number. Heterogeneity was assessed for using Covidence to calculate the I2. Low-level heterogeneity and high-level heterogeneity were set to identify I2 of less than 25% and 50%, respectively. Using ROBINS-I, for all outcomes, there was one study with a high risk of bias, three had low risk, and one had unclear risk. The latter did not mention bias within the article; therefore, we could not comment or assess for risk of bias. Characterization of these biases was necessary to demonstrate a level of confidence when interpreting the study’s conclusions.
Results
Study selection
The number of articles identified and screened was 191 after removal of duplicates (Fig. 1). A total of 168 articles needed to be excluded as per our preoutlined eligibility criteria because they did not report on our desired outcomes or directly compare FP with GB. Out of 191, 20 went on to be screened at the full-text review level. Ultimately, 5 articles were included in accordance with the eligibility criteria for systematic comparison of outcomes of FP vs GB for management of reflux in patients with severe obesity diagnosed with HH or GERD.
Postoperative complications, recurrences, and reoperations
As per Table 2, a recent study by Rahimi-Ardabily et al. followed 397 patients for 72 months after performing laparoscopic GB or laparoscopic paraoesophageal hernia repair with FP. 14 180 patients (90 in each group) were analyzed using propensity matching. The GB group demonstrated significantly lower paraesophageal hernia recurrence rates within the first 36 months of follow-up compared to the FP group (18.4% vs. 34.4%, p = 0.015). Proton pump inhibitor use at the time of recurrence was also compared and was found to trend lower in the GB group (10% vs. 4.4%, p = 0.06) (Table 2). However, by 72 months, recurrence rates between the groups converged, and the difference was no longer statistically significant (p = 0.60). Importantly, there was no significant difference in reoperation rates between the two groups throughout the follow-up period (p = 0.45). These findings suggest that while GB offers an early protective effect against recurrence, this benefit diminishes over time, yet without increasing the likelihood of requiring reoperation. 14
Summary of ROBINS-I Bias Domains
Summary Table of Reported Data from Included Studies
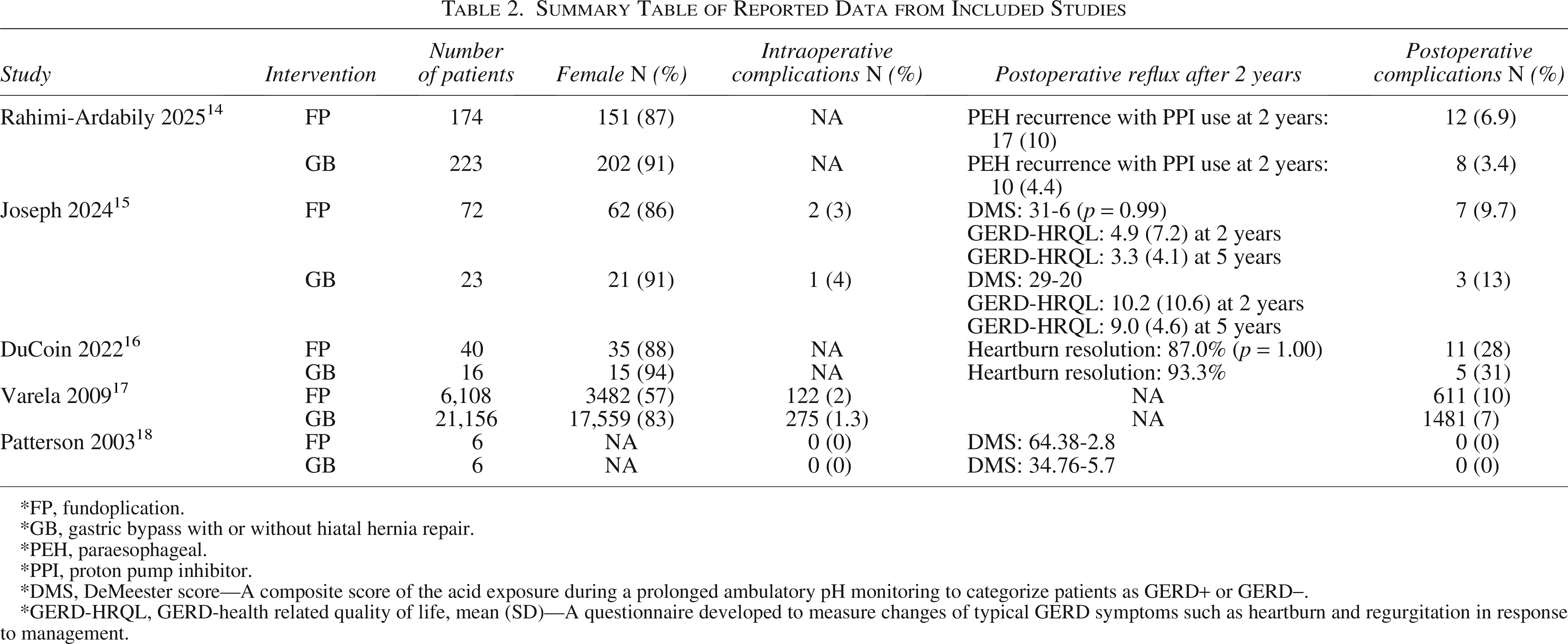
*FP, fundoplication.
*GB, gastric bypass with or without hiatal hernia repair.
*PEH, paraesophageal.
*PPI, proton pump inhibitor.
*DMS, DeMeester score—A composite score of the acid exposure during a prolonged ambulatory pH monitoring to categorize patients as GERD+ or GERD−.
*GERD-HRQL, GERD-health related quality of life, mean (SD)—A questionnaire developed to measure changes of typical GERD symptoms such as heartburn and regurgitation in response to management.
DuCoin et al. described a similar overall complication rate between RYGB (31%) and FP (27.5%) in a cohort of 56 patients with obesity (BMI > 30) with large (>5 cm) HHs (p = 0.75). 16 A large retrospective study including 27,264 patients by Varela et al. reported a lower overall surgical complication rate in the GB group (7%) as opposed to the FP group (10%) (p < 0.05). 17 Patients included in the study were similar in terms of hospital length of stay, observed mortality, risk-adjusted mortality, and hospital costs. 17
Symptomatic GERD/HH outcomes
In the study by DuCoin et al, four patients (10%) in the FP group experienced a symptomatic hernia recurrence as a long-term postoperative complication as opposed to none in the RYGB group (p = 1.00). 16 As well, there were approximately 10% symptomatic hernia recurrences in the FP group and none in the RYGB group, though no statistical comparison between groups was provided. 16
A prospective cohort study by Patterson et al. compared 12 patients’ baseline preoperative reflux to postoperative reflux using the DeMeester score. 18 The preoperative scores were 64.38 in the FP group and 34.76 in the GB group. 18 Patterson et al. revealed DeMeester scores improvement in both groups; however, it is to note that the p value reported (p = 0.21) reflects the comparison of arms postoperatively, rather than pre- to postoperative change within each group. 18 In this study, the patients were significantly more obese in the GB group (BMI 50.8) as opposed to the FP group (BMI 39.8) 18 (Table 2).
In a recent publication, Joseph et al. described the outcomes of a cohort of 95 patients with obesity with a BMI > 35 and GERD. 15 72 of them underwent FP, and 23 underwent a RYGB. There was no significant difference in the postoperative DeMeester score and 30-day complication rate. However, subjective symptom control assessed by GERD-health-related quality of life questionnaire was better in the FP group at 2 years (4.9 ± 7.2 vs. 10.2 ± 10.6 [p = 0.045]) and 5 years (3.3 ± 4.1 vs. 9.0 ± 4.6, [p = 0.041]). 15 Weight loss was greater in the RYGB group (%TBWL 26.04% vs. 4.03% [p < 0.05]) 15 (Table 2).
Discussion
This systematic review is the first to specifically compare the clinical outcomes between FP and GB surgery for the management of GERD and HH in patients with severe obesity. After reviewing five studies, our findings revealed some differences in efficacy and complication rates between these two surgical approaches.
Efficacy in GERD resolution
The review demonstrates that both FP and GB are effective in resolving GERD symptoms.15–18 Subjective reflux symptoms might be decreased with a FP; however, these findings did not correlate with a significant difference in postoperative DeMeester scores, and they were inconsistent among studies.14,18 Additionally, one study found differing DeMeester scores preoperatively between groups, which places limitations on direct comparability since it could potentially be a confounding factor in assessing postoperative efficacy. 18 Variation in limb lengths for RYGB and FP techniques may explain these conflicting findings. 18 The proton pump inhibitor use at the time to recurrence was not significantly different between the two groups (p = 0.065). 14 However, a previous systematic review evaluating the safety and efficacy of GP after failed FP on antireflux outcomes demonstrated over 90% improvement in GERD symptoms. 19
Impact on hiatal hernias
In terms of HHs management, both surgical procedures are effective. FP directly addresses the hiatal defect and reinforces the esophageal hiatus, which is effective in most patients. However, a trend toward more recurrence postfundoplication is noted, especially in the context of significant obesity, which can exert additional pressure on the hiatus. Some evidence on GB reports lower early recurrence rates of HHs in patients with obesity. 14 Although this procedure was not specifically designed to repair HHs, future weight loss helps reduce intra-abdominal pressure, and the Roux limb anatomy provides an anchor to the proximal stomach to stay below the diaphragm. 20 Studies did not specifically report the proportion of HHs repaired at the time of GB surgery, which may influence postoperative reflux outcomes.
Weight loss and metabolic benefits
GB offers significant additional benefits in terms of weight loss and metabolic improvements, which are not achievable with FP.14–18 The substantial weight reduction post-GB not only alleviates GERD symptoms but also contributes to overall improved health outcomes, including better management of comorbid conditions such as type 2 diabetes and hypertension. 20 FP, while effective for GERD, does not address obesity, which is a major contributing factor to GERD and HHs in these patients.1,11,21
Complication rates and patient satisfaction
The complication rates between the two procedures show a nuanced picture. FP is generally perceived to cause less severe postoperative complications compared to GB. However, a recent large retrospective study demonstrated lower complication rates for GB compared to FP. 16 GB, while having a higher risk of perioperative complications such as anastomotic leaks and nutritional deficiencies, tends to have higher patient satisfaction due to effective GERD resolution and substantial weight loss. 18 Literature, included in this review, as well as broadly, has reported that long-term complications such as gas bloat syndrome, dysphagia, and hernia recurrence may negatively impact patient satisfaction following FP. 12 Of note, complication rates reported in earlier studies, such as Varela et al. in 2009, are unlikely to reflect the lower morbidity rates seen with modern laparoscopic bariatric and antireflux procedures today.
Limitations of the review
It is important to acknowledge the limitations of this review. The heterogeneity of study designs, publication bias, patient populations, outcomes, and follow-up durations may all introduce bias. Additionally, only 5 observational studies included without any randomized controlled trials directly comparing the two surgical interventions. This limits the ability to draw definitive conclusions regarding the superiority of one procedure over the other. Furthermore, symptoms and HHs recurrences were not consistently or explicitly reported in studies, limiting the ability to thoroughly compare these outcomes. Some included studies do not use standardized objective measures such as the DeMeester score to compare reflux pre- and postoperatively. In cases where it was used, there was a difference in preoperative baseline scores between patients included in the study, limiting direct comparison. As well, the comparative groups may likely have dissimilar baseline weight and obesity classes, potentially introducing confounding.
Future directions
Future research should focus on long-term, randomized controlled trials comparing a standardized technique of FP and GB for patients with severe obesity with either GERD or HHs. Such studies aim to standardize outcome measures, including GERD symptom resolution, hernia recurrence, weight loss, quality of life, and complication rates. Furthermore, patient-centered outcomes, such as satisfaction and quality of life improvements, should be prioritized to better guide clinical decision-making.
Conclusions
While both FP and GB are effective procedures in the management of GERD and HHs in patients with severe obesity, GB may offer durable long-term outcomes due to the associated weight loss and improvement of comorbid conditions.
A nonstatistically significant trend toward less recurrence of HHs after GB in patients with obesity was noted, while objective measurements of reflux were similar in the postoperative period. The choice of procedure should be individualized, considering the patient’s overall health, obesity severity, and preferences. Collaborative decision-making involving a multidisciplinary team is crucial to optimizing patient outcomes. Future prospective comparative trials are also needed to provide a higher level of evidence.
Footnotes
Authors’ Contributions
S.A.M.—Investigation and writing; M.A.—Investigation; A.M.—Investigation; J.H.—Supervision; C.M.S.—Supervision; A.E.—Supervision, conceptualization, and writing.
Ethics and Dissemination
This review does not require study participation or utilizing any confidential patient information. No ethical approval was necessary or obtained.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.