
Abstract
Background:
Postoperative cognitive dysfunction (POCD) is highly prevalent after bariatric surgery, particularly among patients with obesity. This study aims to assess whether single-dose preoperative modafinil enhances cognitive outcomes and prevents POCD in patients undergoing sleeve gastrectomy under general anesthesia.
Methods:
This randomized, double-blind trial included 80 adults scheduled for sleeve gastrectomy, who received either 200 mg oral modafinil or placebo before surgery. Cognitive and emotional function were evaluated using the Addenbrooke’s Cognitive Examination (ACE), Mini-Mental State Examination (MMSE), and Depression Anxiety Stress Scale (DASS-21), with Bonferroni-adjusted significance thresholds.
Results:
Baseline cognitive impairment was highly prevalent (80% ACE < 88; 26.25% MMSE < 27). Both groups demonstrated significant postoperative improvement in global ACE scores, verbal fluency, and memory (all p < 0.001), but not in attention or visuospatial domains. The language domain improved significantly only in the modafinil group (p = 0.001). Critically, the modafinil group showed a 20% increase in patients achieving normal ACE scores and a 17.5% decrease in those with abnormal scores(p < 0.001), while changes in the placebo group were not significant. DASS-21 and MMSE scores remained stable, and adverse events were rare and mild.
Conclusions:
Sleeve gastrectomy led to robust cognitive improvement; single-dose modafinil provided categorical cognitive benefit but did not significantly impact global or emotional outcomes.
Introduction
Postoperative cognitive dysfunction (POCD) is a frequent and impactful neurological complication following anesthesia and surgery, with incidence rates reported as high as 10–54% depending on surgical type and patient risk profile. 1 Meta-analyses indicate POCD affects approximately 40% of patients within the first postoperative week and persists in 17–26% up to 3 months. 2 POCD is characterized by deterioration across domains such as verbal memory, attention, executive function, language comprehension, and visuospatial ability, resulting in measurable decline in recovery metrics. 3 Importantly, these cognitive deficits are accompanied by psychiatric symptoms—depression, anxiety, and fatigue—that collectively worsen health-related quality of life and increase health care costs and morbidity. 4
Sleeve gastrectomy is now the most common bariatric surgical intervention for severe obesity, accounting for nearly 60–80% of all bariatric procedures worldwide in recent years. 5 The operation achieves pronounced metabolic and anthropometric benefits but also induces changes that may increase psychological stress and complicate postsurgical adaptation. 6 Studies have demonstrated that 40–80% of bariatric candidates present with some degree of cognitive impairment prior to surgery, a prevalence influenced by assessment method and population factors. 7 Obesity further heightens risk for perioperative cognitive dysfunction through mechanisms including chronic inflammation, insulin resistance, and cerebral vascular alterations. 8 Such vulnerabilities highlight the need for perioperative cognitive optimization to reduce adverse neurological outcomes and hospital length of stay. 9
At present, no pharmacological intervention is approved to prevent POCD or postoperative delirium. 10 Modafinil, approved for narcolepsy and sleep disorders, has recently attracted interest for mitigating postoperative cognitive risks by enhancing wakefulness and attention. 11 Recent randomized trials and neuroimaging studies show modafinil improves memory and executive function in patients with cognitive deficits linked to depression and medical illness. 12 Animal and translational research demonstrates additional neuroprotective effects—including reduction of neuronal pyroptosis, inflammation markers, and upregulation of brain-derived neurotrophic factor. 11 Clinical experience with perioperative modafinil suggests a favorable safety profile with few interactions or abuse risk, supporting its tolerability immediately before surgery. 13 Single preoperative dosing of 200 mg modafinil has been shown to decrease postoperative fatigue and accelerate recovery without excessive adverse effects. 14
Given that modafinil is not approved for POCD but has a plausible mechanistic rationale, and considering the lack of pharmacological treatments alongside its potential to enhance postoperative cognitive function as a generally safe medication, 9 we aimed to evaluate its effectiveness in preventing POCD in patients undergoing general anesthesia for sleeve gastrectomy.
Materials and Methods
This randomized, double-blind clinical trial (IRCT20141009019470N76) was conducted at Ghadir Mother and Child Hospital, affiliated with Shiraz University of Medical Sciences, between September 2017 and March 2018, targeting obese adults scheduled for sleeve gastrectomy. A total of 80 patients aged 20–60 years were enrolled; exclusion criteria included a history of cardiovascular, endocrine, hepatic, renal, neurological, psychiatric, alcohol use, substance abuse, or active/uncontrolled disease. All eligibility criteria and study conduct adhered strictly to the Declaration of Helsinki and were approved by Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1396.63), with written informed consent obtained from all participants and clinical trial registration performed prospectively. Randomization was performed using a block randomization method via a secure web-based service, with assignments placed in sequentially numbered, sealed opaque envelopes by an independent staff member.
Two hours before induction of anesthesia, intervention group patients received a single 200 mg oral dose of modafinil (two identical 100 mg tablets), while control group patients received a matched placebo, administered by an anesthetic nurse unaware of study details, maintaining blinding for patients, clinicians, outcome assessors, and investigators throughout the perioperative period. To preserve strict double blinding, the active drug and placebo were indistinguishable in appearance, packaging, and administration schedule; all clinical staff, including surgeons and anesthesiologists, had no access to the randomization list. Comprehensive perioperative safety monitoring was conducted with vital signs, cardiopulmonary status, level of consciousness, and inquiry for modafinil-associated adverse events, documented using CTCAE criteria and Visual Analog Scales. Blinding integrity was evaluated post hoc by asking participants and assessors to guess group assignment; the proportion of correct guesses was compared with chance using chi-squared testing.
Preoperative cognitive status was established using both the Addenbrooke’s Cognitive Examination (ACE) and the Mini-Mental State Examination (MMSE), with all assessments performed 1 day before surgery by a single trained examiner. The ACE threshold for normal cognition was set at ≥88, mild impairment as 82–88, and scores <82 defined as dementia, based on contemporary validation studies. 15 MMSE impairment was flagged for scores below 27, which better detects mild deficits compared with the classic <24 cutoff for cognitive impairment in bariatric populations. 16 Postoperative cognitive and emotional outcomes were measured via repeated administration of ACE, MMSE, and the Depression Anxiety Stress Scale (DASS-21), following surgery once patients were medically stable and transferred to the ward. The DASS-21 is validated for perioperative emotional assessment and consists of three 7-item subscales, scored from 0 to 3 per item across depression, anxiety, and stress; higher scores denote greater symptom severity. 17
Adverse events and perioperative complications were proactively monitored in all participants from administration of the study drug through discharge. Safety monitoring included regular assessment of vital signs, cardiopulmonary status, level of consciousness, and systematic inquiry for common modafinil-associated side effects (e.g., headache, nausea, insomnia, anxiety). All adverse events were documented on standardized case report forms; their severity was rated using a Visual Analog (CTCAE) criterion.
The sample size of 80 for this double-blind study was determined based on a prior study, 18 which found that 65% of placebo patients versus 12% of modafinil patients reported moderate to severe fatigue postoperatively, representing a 53% absolute risk reduction. Based on sample size for the comparison of proportions with a Type I error rate of 0.5 and a statistical power of 90%, at least 40 patients are needed in each group. Patients meeting eligibility criteria were randomized using the block randomization method (www.sealedenvelope.com) and assigned to either the Modafinil or Placebo group in 11 blocks of sizes 4 and 8. Group assignments were documented and placed in sealed envelopes by a single staff member with exclusive access to the randomization list.
The primary outcome was postoperative change in ACE score and its subdomains (attention, memory, fluency, language, and visuospatial), comparing baseline and postsurgical results between modafinil and placebo groups, as well as the percentage of patients reaching normal ACE scores (>88). Secondary outcomes included changes in DASS-21 and MMSE scores pre and postsurgery, and quantification of adverse events with severity grading. Categorical data were analyzed with Chi-square or Fisher’s exact test; continuous data were expressed as mean ± SD or median (IQR) and compared with t-test, Mann–Whitney U, or paired t-test as appropriate after normality evaluation by Kolmogorov–Smirnov test. Blinding success was analyzed by comparing correct guess proportions against chance. All statistical analysis was performed in SPSS v22.0; p < 0.05 was considered statistically significant. If needed, the Bonferroni-adjusted p value was applied.
Results
Eighty patients (mean age 32.25 ± 7.74 years, median BMI 43 [40.41–46.48]) completed the trial, with 40 assigned to modafinil and 40 to placebo (Fig. 1). Baseline demographics, clinical features, and surgery duration showed no statistical difference between groups (p > 0.05) (Table 1). Among all participants, 80% had baseline ACE scores below 88% and 26.25% had MMSE scores below 27, indicating a high preoperative prevalence of mild cognitive impairment.
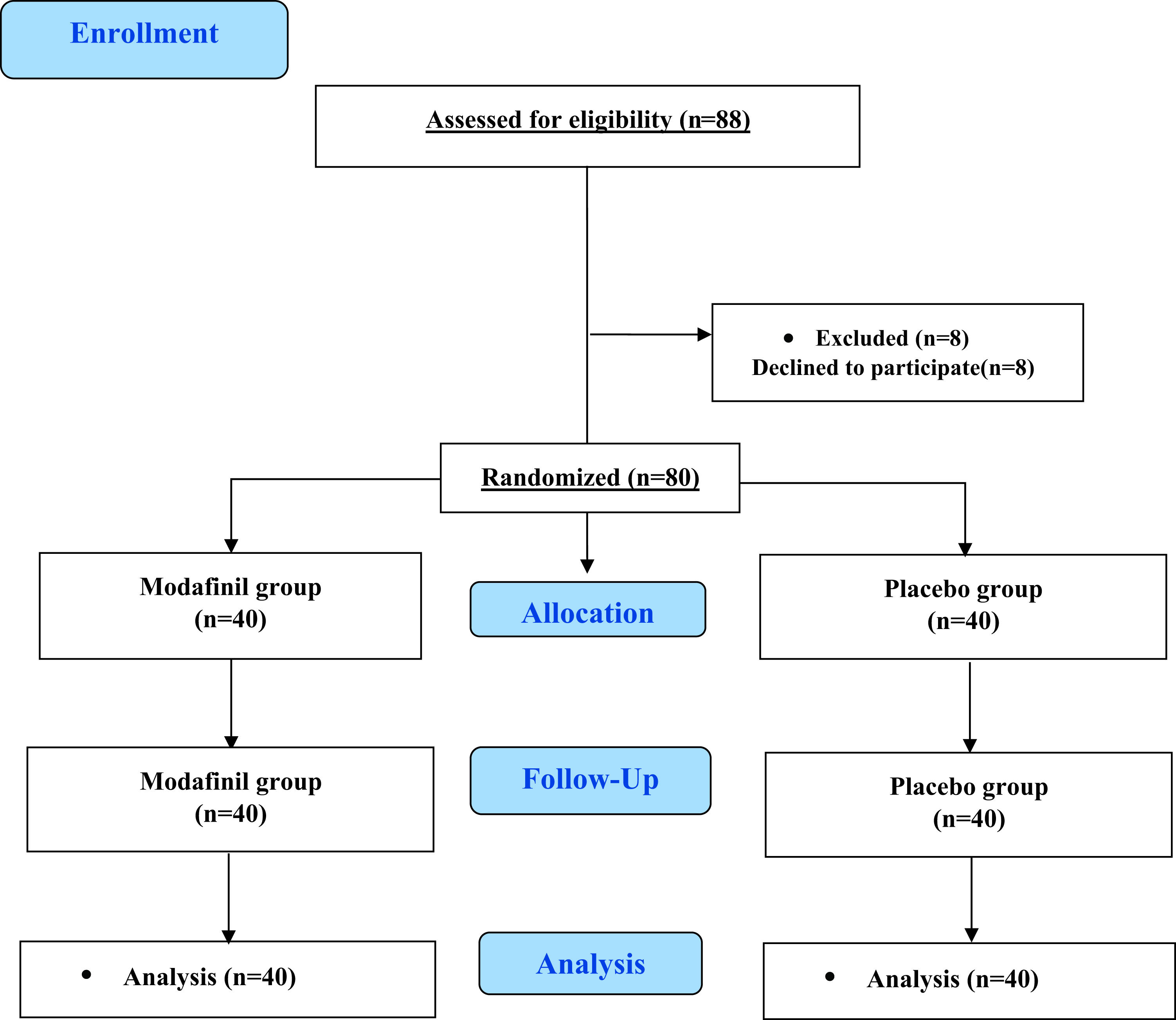
Consort flow diagram.
Demographic and Clinical Baseline Data of Patients under Study
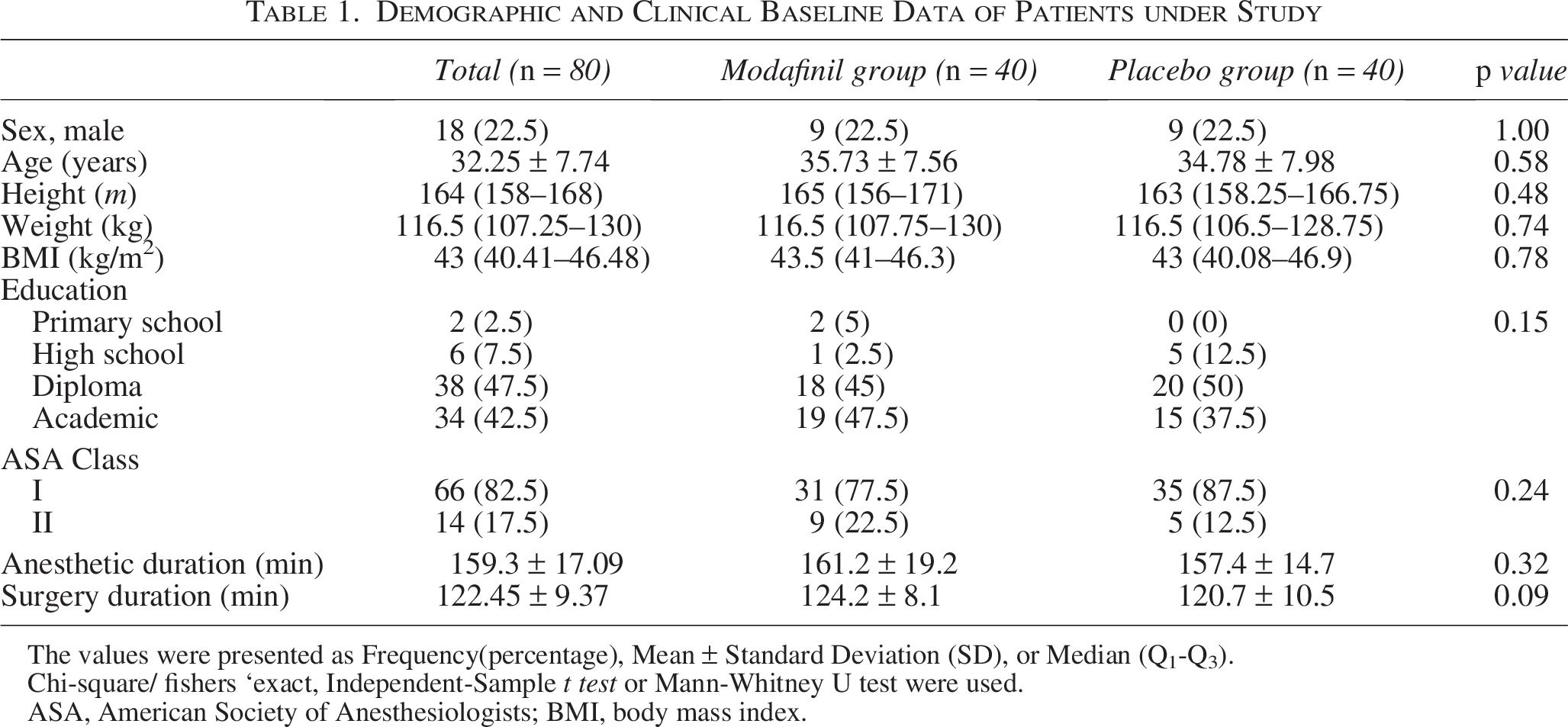
The values were presented as Frequency(percentage), Mean ± Standard Deviation (SD), or Median (Q1-Q3).
Chi-square/ fishers ‘exact, Independent-Sample t test or Mann-Whitney U test were used.
ASA, American Society of Anesthesiologists; BMI, body mass index.
After applying Bonferroni-adjusted significance thresholds for multiplicity (ACE: p < 0.01; DASS21:p < 0.016), both the modafinil and placebo groups demonstrated significant postsurgical improvements in ACE total score, fluency, and memory domains (p < 0.001, each), but no significant changes in the visuospatial or attention domains in either group (p = 0.25–0.840). In the modafinil group, a significant improvement was seen in language (p = 0.001), while the language domain in the placebo group only showed a modest change (p = 0.038), failing to meet Bonferroni-adjusted significance. No between-group difference in postoperative ACE, fluency, language, memory, or MMSE scores reached statistical significance after adjustment, with all between-group p values well above the correction threshold. cThe DASS-21 total scores and subscales (depression, anxiety, stress) did not show significant postsurgical change in either arm under Bonferroni correction (all p > 0.016), indicating emotional state remained stable for both groups (Table 2).
Comparison of Mental and Cognitive Tests Between Modafinil and Placebo Groups before and after the Operation
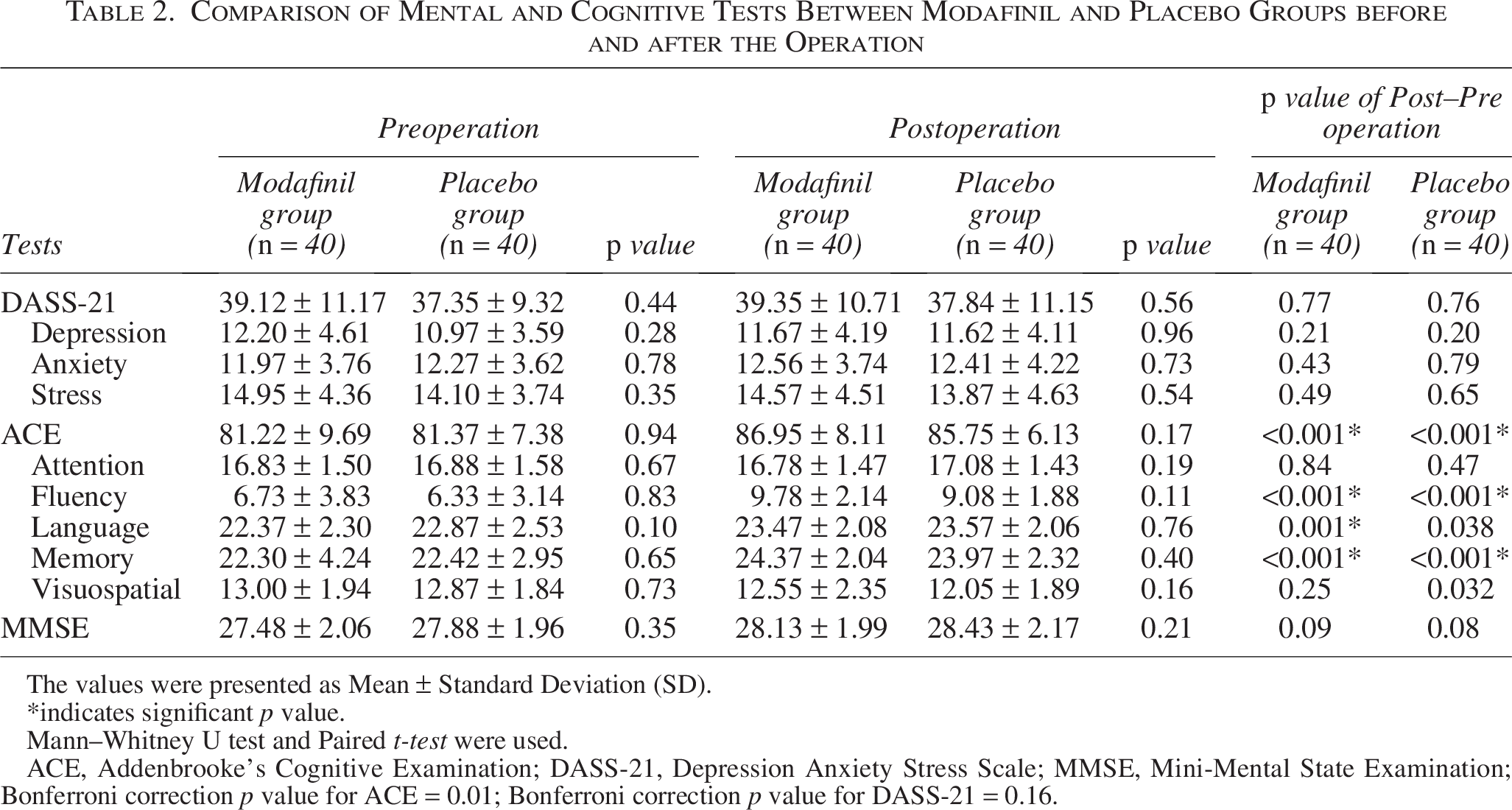
The values were presented as Mean ± Standard Deviation (SD).
*indicates significant p value.
Mann–Whitney U test and Paired t-test were used.
ACE, Addenbrooke’s Cognitive Examination; DASS-21, Depression Anxiety Stress Scale; MMSE, Mini-Mental State Examination; Bonferroni correction p value for ACE = 0.01; Bonferroni correction p value for DASS-21 = 0.16.
Effect size analysis supported these findings: moderate gains (Cohen’s d ≈ 0.6) were observed for ACE total and memory in both groups, and large effects (Cohen’s d ≈ 0.95) for fluency; language improved only in the modafinil group per corrected thresholds (Table 3).
Summary of Effect Sizes (Cohen’s d) for Cognitive and Emotional Outcomes in Modafinil and Placebo Groups
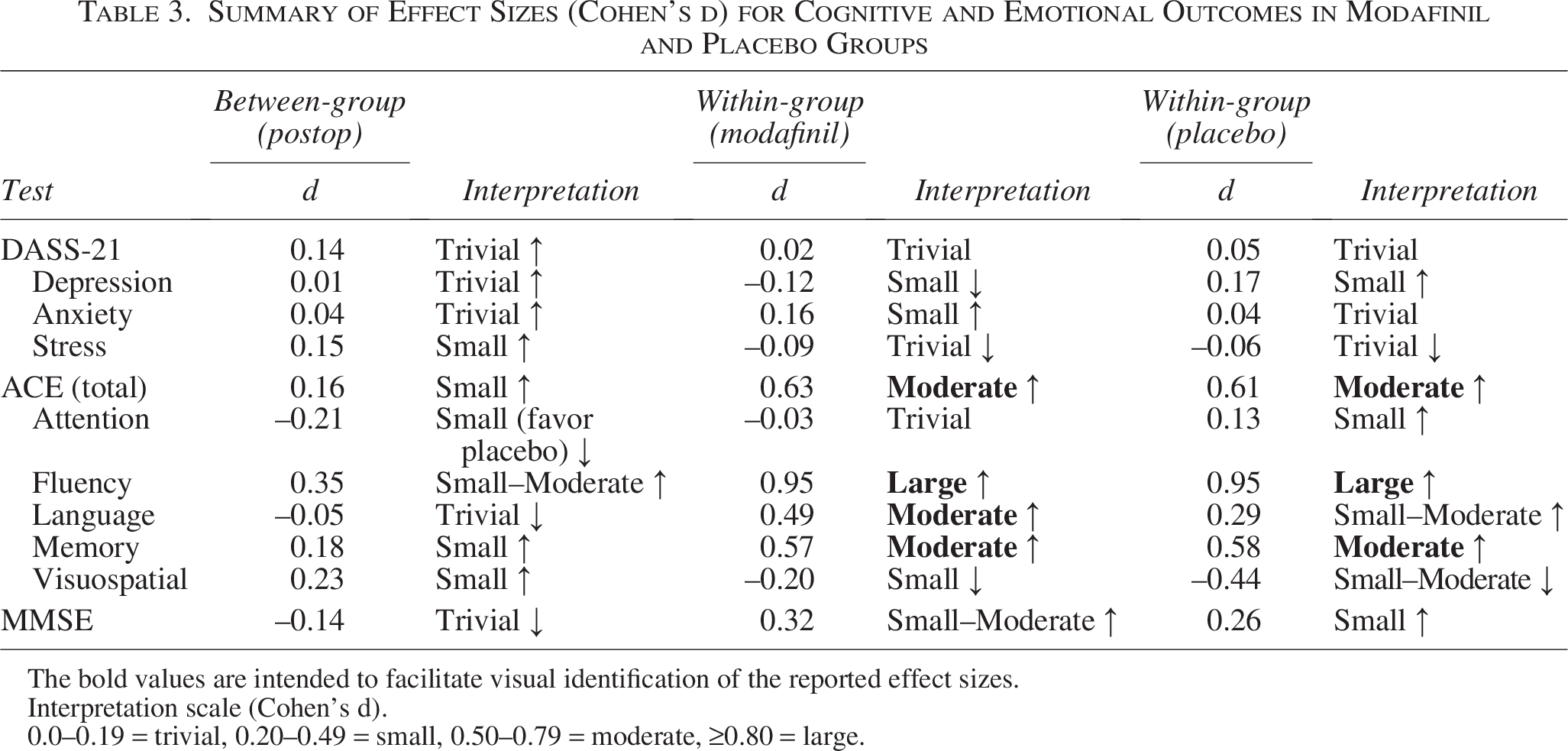
Interpretation scale (Cohen’s d).
0.0–0.19 = trivial, 0.20–0.49 = small, 0.50–0.79 = moderate, ≥0.80 = large.
The bold values are intended to facilitate visual identification of the reported effect sizes.
Categorical analysis further revealed that the proportion of patients with normal cognition (ACE > 88) increased by 20% in the modafinil group and 12.5% in the placebo group; the reduction in abnormal cognition (ACE < 83) was 17.5% and 7.5%, respectively. However, only the modafinil group’s shift reached statistical significance (p < 0.001), while the placebo group’s improvement did not (p = 0.06) (Table 4).
Comparison of ACE Score Categories in Each Group before and after the Operation
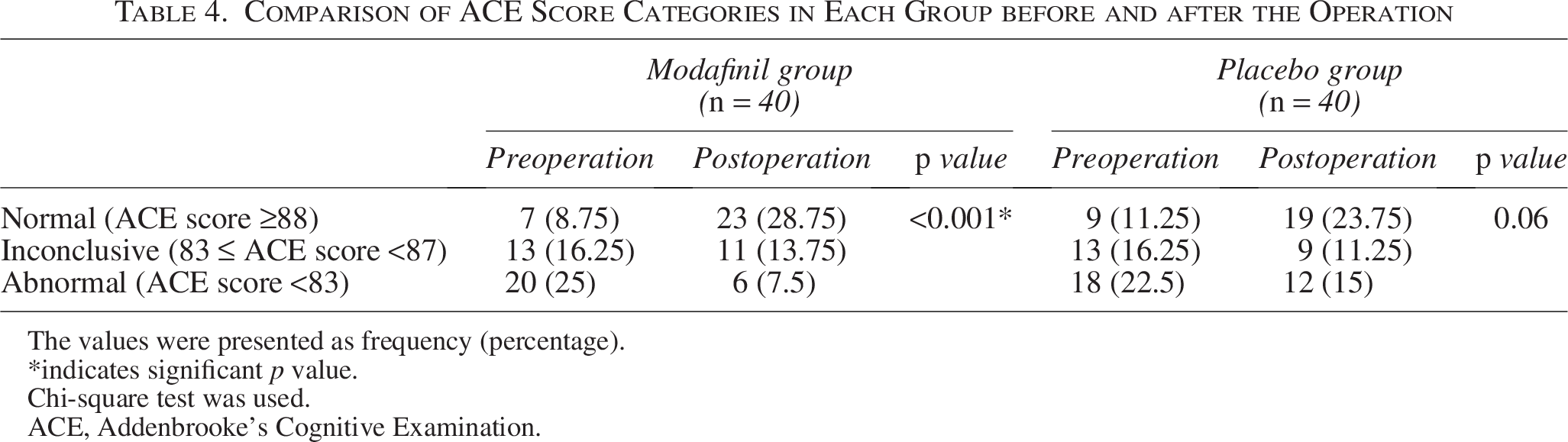
The values were presented as frequency (percentage).
*indicates significant p value.
Chi-square test was used.
ACE, Addenbrooke’s Cognitive Examination.
Blinding integrity was preserved, as only 11.25% of patients correctly guessed group assignment (7 (17.5%) in modafinil group, 2 (5%) in placebo group; p = 0.154), not different from chance; assessors’ guesses also showed no significant accuracy above the expected rate (10 [25%] in modafinil group, 8 [20%] in placebo group; p = 0.789). Adverse events were uncommon: one instance (2.5%) of mild headache in the modafinil group resolved spontaneously; rates of postoperative nausea were similar (modafinil 27.5%, placebo 30%, p = 0.834), and no serious adverse reactions, insomnia, agitation, or cardiovascular instability were observed in either group.
A post hoc power analysis indicated statistical power was adequate (∼0.78) to detect moderate within-group ACE improvements, but likely underpowered for smaller between-group effects.
Discussion
This randomized controlled trial shows that both modafinil and placebo groups experienced significant improvements in global cognitive scores (ACE), verbal fluency, and memory after sleeve gastrectomy, according to Bonferroni-adjusted thresholds, but not in attention or visuospatial domains. Notably, only the modafinil group demonstrated a significant gain in language domain scores after surgery (p = 0.001), whereas the placebo group’s improvement in language was not statistically significant with the corrected threshold (p = 0.038). No significant differences were found between groups for postoperative ACE, MMSE, or DASS-21 scores, nor did emotional states (depression, anxiety, stress) or overall cognitive status exhibit between-group changes that survived multiple comparison correction.
Importantly, analysis of ACE score categories revealed that the percentage of patients with normal cognition (ACE > 88) increased by 20% in the modafinil group and by 12.5% in the placebo group, while the proportion with abnormal cognition (ACE < 83) decreased by 17.5% and 7.5%, respectively; however, only the modafinil group’s changes were statistically significant (p < 0.001), while the placebo group changes did not achieve significance (p = 0.06). This suggests a possible added clinical benefit of modafinil in facilitating transitions from impaired to normal cognitive states after bariatric surgery, aligning with Carr and colleagues’ findings. 19
The baseline prevalence of mild cognitive impairment was high, with 80% of patients scoring below the normative ACE cutoff (>88) and more than a quarter below the sensitive MMSE cutoff (27 points), reflecting literature on cognitive vulnerabilities in obese patients who present for bariatric surgery.7,20 Bariatric surgery itself has consistently been associated with improvements in several cognitive domains, including memory and executive function, even among patients with pre-existing deficits. 21 Our findings corroborate those of recent systematic reviews and longitudinal studies that cognitive benefits following bariatric surgery are evident as early as the immediate postoperative phase and may be sustained for months to years postsurgery.2,22,23
This study did not detect an additional statistically significant effect of a single 200 mg preoperative dose of modafinil on postoperative cognitive or emotional outcomes compared with placebo under rigorous Bonferroni correction, although language domain improvement achieved significance in the modafinil group only. Prior research in surgical and nonsurgical patients has shown that modafinil’s cognitive enhancement is most robust in attention, wakefulness, and episodic memory, but its effect size among nonsleep-deprived or relatively healthy populations is moderate to modest.2,12,13,19,24 This is consistent with our small between-group effect sizes and the overall absence of a clinically meaningful group difference in global cognition, emotional state, or adverse events.
These results extend existing evidence that the main driver of early postoperative cognition improvement after bariatric surgery is likely the metabolic, nutritional, and inflammatory changes resulting from weight loss and no single-dose neuropharmacological intervention.21,22 The only domain for which modafinil showed clear within-group significance versus placebo was language, warranting further investigation across larger and more diverse samples, other dosing regimens, and repeated administration approaches to assess whether specific cognitive domains benefit from perioperative stimulant use. Our safety data, in line with meta-analyses of modafinil in surgical and nonsurgical cohorts, confirm the drug’s favorable profile at the studied dose, including low rates of mild adverse effects and no serious events.12,13,19
Main limitations of our study include a single-center design, short duration of follow-up, moderate sample size, and analysis limited to a single preoperative modafinil administration, restricting generalizability and long-term conclusions. Unmeasured confounders such as underlying sleep disorders, nutritional status, and the absence of objective sleep/wake measurements could influence cognitive recovery patterns in both study arms. In acknowledgment of the potential for evolving clinical and methodological standards over time, this study has incorporated a synthesis of recent literature and updated regulatory guidance within the discussion. The explicit integration of these contemporary sources serves to demonstrate that the fundamental clinical questions addressed by this work remain highly significant and valid within the context of current medical practice. By contextualizing our findings with up-to-date references, the article aims to assure readers and reviewers that, despite the interval between the original data collection and publication, the study’s methodology, analytical approach, and results remain robust, relevant, and directly applicable to modern bariatric surgical and anesthetic care. This approach underscores our continued commitment to the highest standards of scientific integrity and ensures that the contribution of this research is fully aligned with the dynamic landscape of contemporary clinical investigation.25,26
In conclusion, sleeve gastrectomy confers robust, immediate cognitive benefits in bariatric patients, including substantial categorical shifts from cognitive impairment to normal status. While modafinil did not yield statistically significant advantages for overall cognitive or emotional scores relative to placebo, significant improvements in ACE category proportions and the language domain indicate a signal for clinical benefit that should be explored in future trials targeting patients at greatest neurocognitive risk.
Footnotes
Acknowledgments
The present article was extracted from the thesis written by Kambiz Golestani and was financially supported by Shiraz University of Medical Sciences.
Authors’ Contributions
All authors contributed to the study design. M.S. and K.G. participated in proposal writing, article writing, and data curation. A. M. contributed to study conception, data interpretation, and served as a psychiatry consultant. S.-S.N. contributed to the study conception and article drafting. A.K., Z.F.S., L.D., and A.A. contributed to data collection, the revision of the article and edited the draft. M.B. participated in the data analysis, and data interpretation and article revision and preparation. All authors read the final version of the article and accept accountability for all aspects of this work.
Ethics Approval and Consent to Participate
The study protocol followed the Declaration of Helsinki and Good Clinical Practice guidelines and was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1396.63). Written informed consent was taken from all patients. This study is registered with the Iranian Registry of Clinical Trials (IRCT20141009019470N76), where the trial protocol can be accessed.
Availability of Data and Materials
All data will be available on request to Dr. Arash Mani (
Data Access and Responsibility
The principal investigator, Dr. Arash Mani, had full access to all the data in this study and was responsible for the integrity of the data and the accuracy of their analysis.
Author Disclosure Statement
The authors declare that they have no relevant or material financial interests that relate to the research.
Funding Information
No funding was received for this article.