
Abstract
Objective:
To investigate the effectiveness of clinical Pilates exercises performed through telerehabilitation in individuals who had undergone bariatric surgery (BS).
Design:
This is a prospective randomized controlled trial. A total of 20 individuals who had undergone BS patients were randomly allocated to the clinical Pilates exercise group (CPEG) and the control group (CG). The CPEG underwent telerehabilitation-based clinical Pilates exercises under physiotherapist supervision, twice weekly for 6 weeks. The CG received online physical activity (PA) counseling. The primary outcome was the functionality, which was assessed using the Senior Fitness Test Battery (6-min walk test [6-MWT], chair stand test, 8-foot up and go test [8-FUGT], arm curl test, back scratch test, chair sit, and reach test). Secondary outcomes were muscle strength, core stability, body composition, pedometer-recorded PA level, obesity-specific quality of life (QoL), and health-related QoL.
Results:
At the end of the study, statistically significant improvements favoring the CPEG were observed in the 6-MWT distance, arm curl, 8-FUGT, lower trapezius and gluteus maximus muscle strength, core stabilization, metabolic age, step count, Obesity and Weight Loss Quality of Life Instrument, and Nottingham Health Profile.
Conclusion:
Clinical Pilates exercises performed through telerehabilitation provide improvement in the parameters of functionality, physical fitness, and QoL in individuals who have undergone BS.
Keywords
Introduction
Bariatric surgery (BS) is an effective treatment for severe obesity. 1 The increasing prevalence of obesity and the development of surgical techniques have resulted in the popularization of BS. 2 It has been reported that BS is the most effective treatment for long-term weight loss in severe obesity, and surgery also helps reduce comorbidities, increase self-confidence, and quality of life (QoL). 3 However, a significant proportion of patients achieve less than expected benefits due to suboptimal weight loss or weight regain. 4 At the same time, patients have difficulty in functional capacity and daily living activities. The decrease in muscle strength negatively affects the patient’s metabolism, functional capacity, and daily living activities. 5
Physical activity (PA) and exercise are recommended both preoperatively and postoperatively.6,7 Although there is no consensus on the type, intensity, and frequency of exercise in clinical guidelines, aerobic and resistance exercises are mostly emphasized. In addition, postbariatric patients have low adherence to exercise programs.6–8 However, beyond general barriers such as time constraints and inability to find a suitable environment, specific obesity-related barriers such as fatigue, fear of injury, pain, and comorbidities also contribute to the avoidance of exercise. 9 Psychological factors such as enjoyment, self-efficacy, and social support are central to the decision to perform PA after BS. 10 Clinical Pilates, with factors such as low risk of injury, reduced fear of movement, inclusivity for individuals of all levels, and exercises promoting mind-body integration, is one such exercise approach that can enhance exercise adherence by motivating individuals. 11
Pilates is safe and effective for individuals with obesity. It has documented benefits for body composition, functional capacity, lung function, psychological health, and QoL. 12 There is no research available on the effectiveness of Pilates exercises during the postbariatric period, even though studies show its effectiveness in individuals with obesity. Considering the fundamental principles of clinical Pilates exercises and their role in the conservative treatment of obesity, these exercises may present a suitable option for individuals in the postbariatric process. In addition, in studies involving individuals with obesity, the impact of exercise has been mainly explored on body composition. Other parameters such as functional status and physical fitness remain understudied.
Telerehabilitation is one of the trending approaches that increase exercise adherence by helping to overcome time constraints, lack of a suitable environment, and traveling costs. 13 Telerehabilitation may be suitable for postbariatric patients by improving accessibility and participation, facilitating lifestyle behavior change, and enabling longer term home-based rehabilitation, thereby helping to overcome common barriers such as time, travel, and environmental constraints. 14 Moreover, evidence from different rehabilitation fields indicates that clinical Pilates delivered via telerehabilitation is safe, feasible, and effective.15–17
The aim of this study was to investigate the effectiveness of telerehabilitation-based Pilates exercises performed through telerehabilitation on functionality and physical fitness in individuals who had undergone BS.
Methods
Study design
This was a prospective, randomized controlled study. The study was approved by the University Ethics Committee (No: E-74555795-050.01.04-392595), and the study protocol was registered in ClinicalTrials.gov (NCT05454696). Verbal and written explanations were provided to participants, and each participant provided written informed consent. The study was conducted under the principles of the Declaration of Helsinki. The subjects were assigned to the clinical Pilates exercise group (CPEG) and the control group (CG) using a 1:1 randomized allocation. A numbered series of prefilled, sealed, opaque envelopes was used for group allocation, which was created using a computer-based random number generator (https://www.randomizer.org/). Randomization was performed by a researcher (G.K.A.) who did not take part in the assessments.
Participants
Participants who had undergone BS and were followed up in the obesity polyclinic of the endocrinology and metabolic diseases outpatient clinic of a university hospital were screened. Twenty-two participants who met the criteria and accepted to participate in the study between June 2022 and November 2023 were recruited. Participants aged between 18 and 60 years, who had at least 2 months and a maximum of 24 months since their surgery and who had adequate technology skills to participate in the online exercise program, were included in the study. Participants with musculoskeletal and pulmonary conditions, neurological or systemic diseases, uncontrolled diabetes and hypertension, severe cardiovascular diseases, and psychiatric or psychological disorders affecting treatment adherence were excluded from the study.
Procedure
The CPEG underwent synchronous online clinical Pilates exercises under physiotherapist supervision, twice weekly for 6 weeks and the CG received one session of online PA counseling from a physiotherapist. The Clinical Pilates program was mat-based; targeted core stabilization, trunk mobility, and hip, knee, and shoulder strength; comprised approximately 10–12 exercises per session; and lasted approximately 50 min (10-min warm-up, 30–35-min main set, 5-min cool-down). Both groups continued their individualized diets and routine follow-ups in the obesity polyclinic. The exercise protocol is described according to the Consensus on Exercise Reporting Template. 18 A detailed description of the intervention is presented in Supplementary Appendix SA1.
Outcome measures
The primary outcome measure of this study was functionality. The Senior Fitness Test Battery was used to evaluate functionality. This battery consists of six tests: the 6-min walk test (6-MWT), chair stand test (CST), arm curl test, chair sit and reach test, back scratch test, and the 8-foot up and go test (8-FUGT). The tests were performed in accordance with the previously reported instructions of the Senior Fitness Test Battery. 19 The 6-MWT was performed according to the American Thoracic Society criteria. 20
Secondary outcomes were as follows: (1) muscle strength; (2) core stability; (3) body composition; (4) QoL; and (5) PA level.
A digital hand dynamometer (J-Tech Commander™, JTech Medical, USA) was used to evaluate muscle strength. 21 Isometric strength of the lower trapezius, iliopsoas, gluteus maximus, gluteus medius, quadriceps, and hamstrings was measured. Each measurement was repeated three times, and the average values were recorded.
The core stabilization assessment was conducted using the Sahrmann Core Stability Test with a pressure biofeedback unit (Chattanooga Stabilizer, USA). After inflation to a baseline pressure, participants executed progressively challenging leg-movement tasks while maintaining the target pressure within ± 10 mmHg; the score was the highest level completed with acceptable pressure control. Full-level descriptions and scoring criteria are provided in Supplementary Appendix SA1.
The participant was instructed to maintain the “draw-in maneuver” throughout levels.
22
Body composition outcomes were measured using bioimpedance analysis (Tanita BC-545N, Japan).
23
The following parameters were recorded: total body weight (kg), body mass index (kg/m2), body fat percentage (%), muscle mass (kg), bone mass (kg), and metabolic age. QoL is measured using the Obesity and Weight Loss Quality of Life Instrument (OWLQOL). This obesity-specific questionnaire comprises 17 questions and uses a Likert-type scale.24,25 Participants’ health-related QoL was assessed using the Nottingham Health Profile (NHP). The survey consists of 38 questions divided into six subscales: energy, pain, emotional reaction, sleep disturbance, social isolation, and physical mobility.26,27 The PA level of all participants was assessed using a pedometer. Participants were instructed to wear the pedometer for 1 week at baseline and at the 6th week. Subsequently, step counts per day were recorded.
Data analysis
The G*power (version 3.1.9.7.; Heinrich-Heine Universitat, Duesseldorf) sample size calculator was used to determine the sample size of the study. The sample size was calculated according to research, evaluating the effects of exercise training on the 6-MWT in individuals who had undergone BS, 28 given that the 6-MWT lacks minimal clinical significance in this population. Twenty subjects were determined to be required for each group with an 80% power (two-tailed, an alpha level [α] = 0.05, effect size [ES] d: 0.35).
Data were analyzed using the SPSS software (version 26; SPSS, Chicago, Illinois). Mean, standard deviations, and/or 95% confidence intervals were calculated for each variable. Data were found to be normally distributed using the Shapiro–Wilk test (p > 0.05). Baseline demographic and clinical variables were compared using the independent Student t-test for continuous data and the chi-squared test for categorical data. Analysis of covariance (ANCOVA) was used to compare the 6th-week differences between the two groups. The baseline values of the dependent outcome variables were entered as covariates. The partial eta-squared (ηp2) was used to calculate the ES for the significant ANCOVA. Values of η2 = 0.01 indicate a small effect, η2 = 0.06 indicates a medium effect, and η2 = 0.14 indicates a large effect. 29 p < 0.05 was accepted as statistical significance for all analyses.
Results
Fifty-two subjects were screened for eligibility, and 22 were included in the study and randomized. The study was completed with 20 participants (Fig. 1). No adverse events were reported by the participants during the study. There was no statistically significant difference between the baseline demographic and clinical characteristics of the CPEG (n = 10) and the CG (n = 10) (p > 0.05) (Table 1).
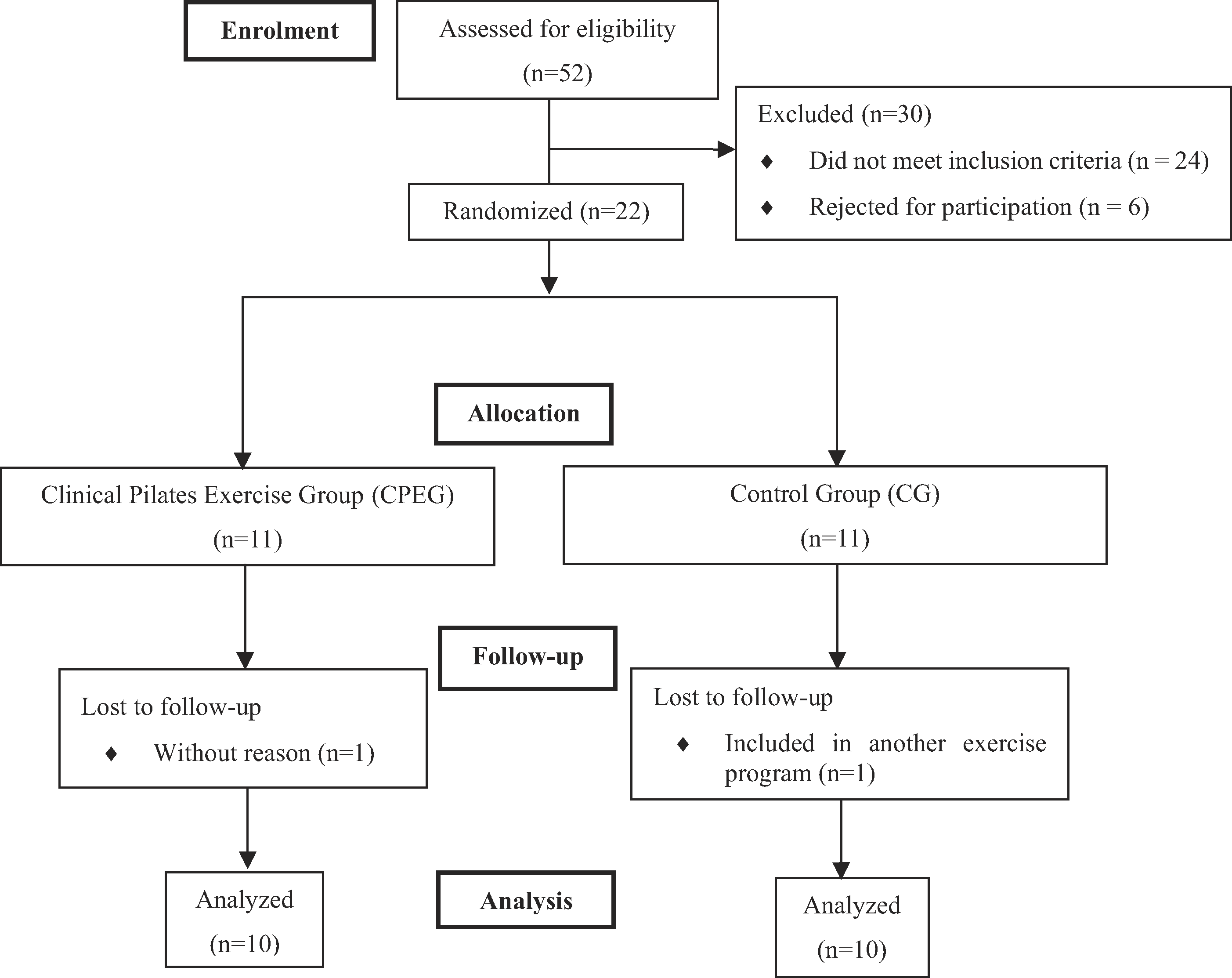
Flowchart of the study design.
Demographic and Clinical Features of the Participants

Bold values are statistically significant. Results are presented as mean ± standard deviation (95% confidence interval).
Independent sample t-test.
Chi-squared test.
BS, bariatric surgery; CG, control group; CPEG, clinical Pilates exercise group; kg, kilogram; m, meter; OSA, obstructive sleep apnea.
Adjusting for baseline outcomes, there was a significant group × time interaction for the 6-MWD, arm curl, and 8-FUGT. Participants in the CPEG experienced greater improvement in 6-MWD (p = 0.004), arm curl (p = 0.047), and 8-FUGT (p = 0.020) at week 6 than those in the CG. Between-group ESs for the 6-MWD, arm curl, and 8-FUGT were large (ES; ηp2: 0.387, 0.213, and 0.279, respectively) at 6 weeks in favor of the CPEG. There was no statistically significant difference in CST, back scratch, and chair sit and reach tests (p > 0.05) (Table 2).
Comparison of Senior Fitness Test Battery Results Between the Groups
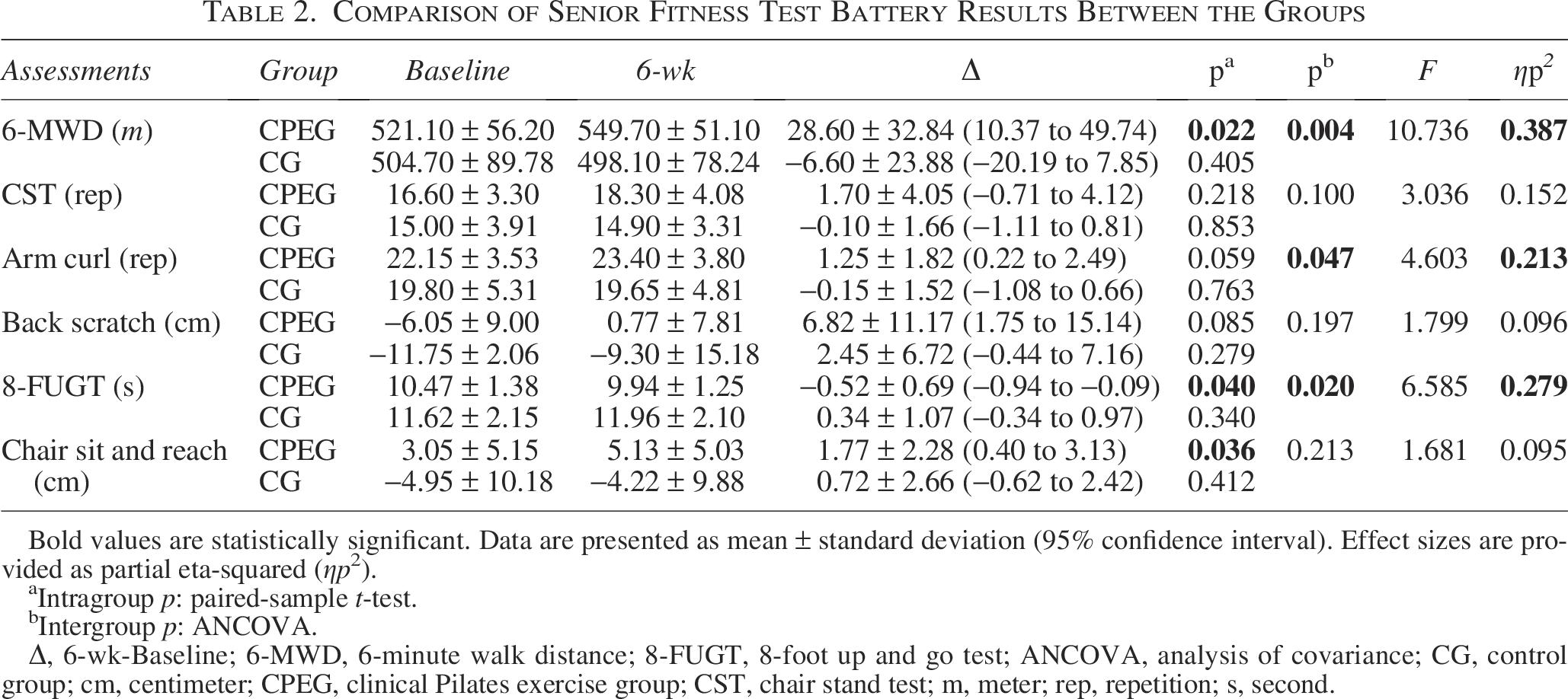
Bold values are statistically significant. Data are presented as mean ± standard deviation (95% confidence interval). Effect sizes are provided as partial eta-squared (ηp2).
Intragroup p: paired-sample t-test.
Intergroup p: ANCOVA.
Δ, 6-wk-Baseline; 6-MWD, 6-minute walk distance; 8-FUGT, 8-foot up and go test; ANCOVA, analysis of covariance; CG, control group; cm, centimeter; CPEG, clinical Pilates exercise group; CST, chair stand test; m, meter; rep, repetition; s, second.
There was a significant group × time interaction for lower trapezius (p = 0.004) and gluteus maximus (p = 0.025) muscle strength in favor of the CPEG. There was no statistically significant difference in other muscles (p > 0.05). Between-group ESs were large for lower trapezius and gluteus maximus muscle strength (ES; ηp2: 0.39 and 0.26, respectively) (Table 3).
Comparison of Physical Fitness Results Between the Groups
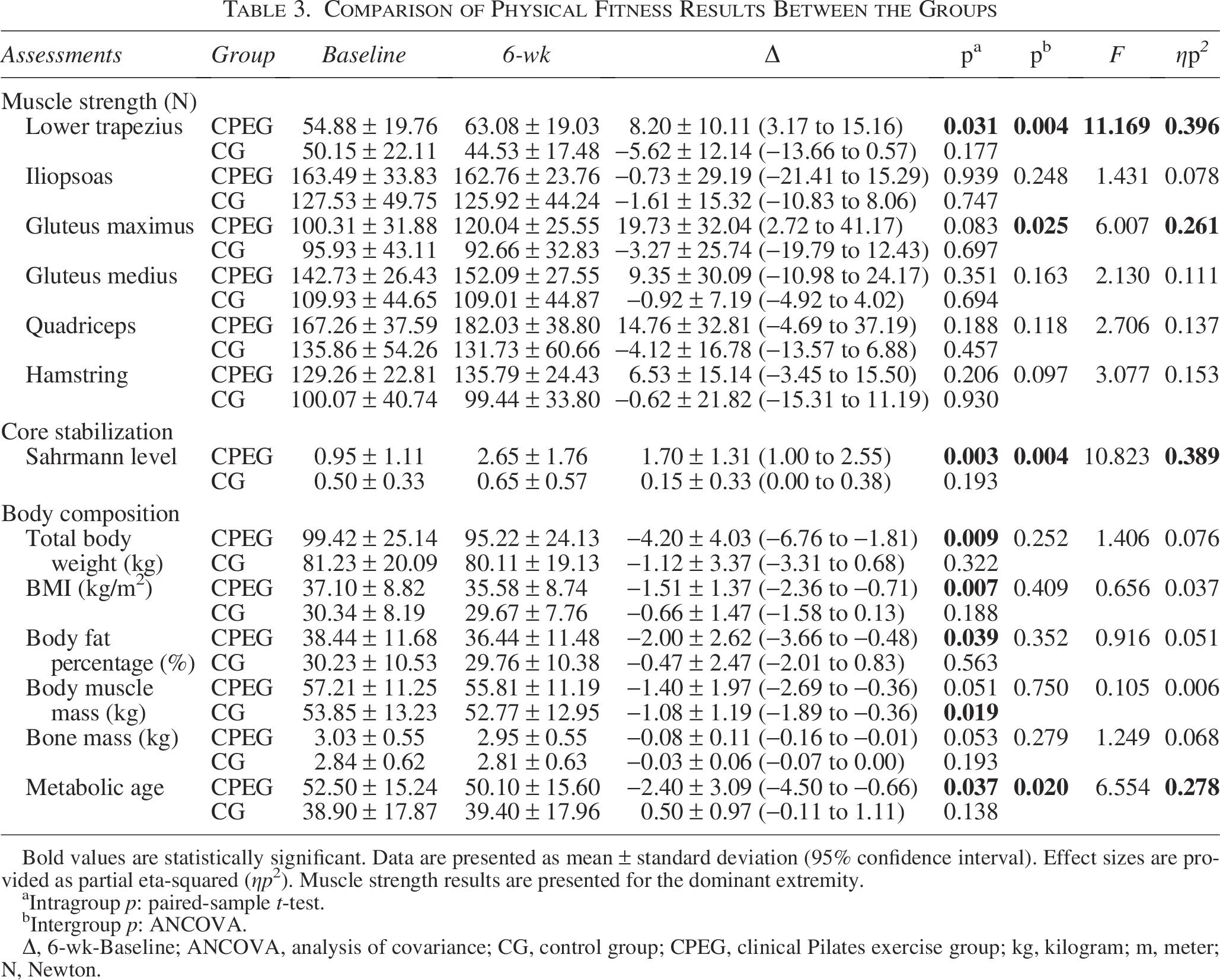
Bold values are statistically significant. Data are presented as mean ± standard deviation (95% confidence interval). Effect sizes are provided as partial eta-squared (ηp2). Muscle strength results are presented for the dominant extremity.
Intragroup p: paired-sample t-test.
Intergroup p: ANCOVA.
Δ, 6-wk-Baseline; ANCOVA, analysis of covariance; CG, control group; CPEG, clinical Pilates exercise group; kg, kilogram; m, meter; N, Newton.
There was a significant group × time interaction for Sahrmann Core Stability Level (p = 0.025) in favor of the CPEG. For the core stability, the between-groups ES was also large (ES; ηp2: 0.38) at 6 weeks (Table 3).
There was no significant difference between the groups in terms of body composition parameters except metabolic age. Participants in the CPEG experienced greater declines in metabolic age (p = 0.020). For metabolic age, the between-groups ES was also large (ES; ηp2: 0.26) (Table 3).
In the comparison between the groups, there was a statistically significant improvement in favor of the CPEG in OWLQOL (p = 0.006), NHP total score (p = 0.015), and NHP subscores (pain: p = 0.019; emotional reaction: p = 0.027; PA: p = 0.022). Between-group ESs for OWLQOL, NHP total score, pain, emotional reaction, and PA subscores were as follows: ES; ηp2: 0.36, 0.30, 0.28, 0.25, and 0.27, respectively (Table 4).
Comparison of Quality of Life and Pedometer Results Between the Groups
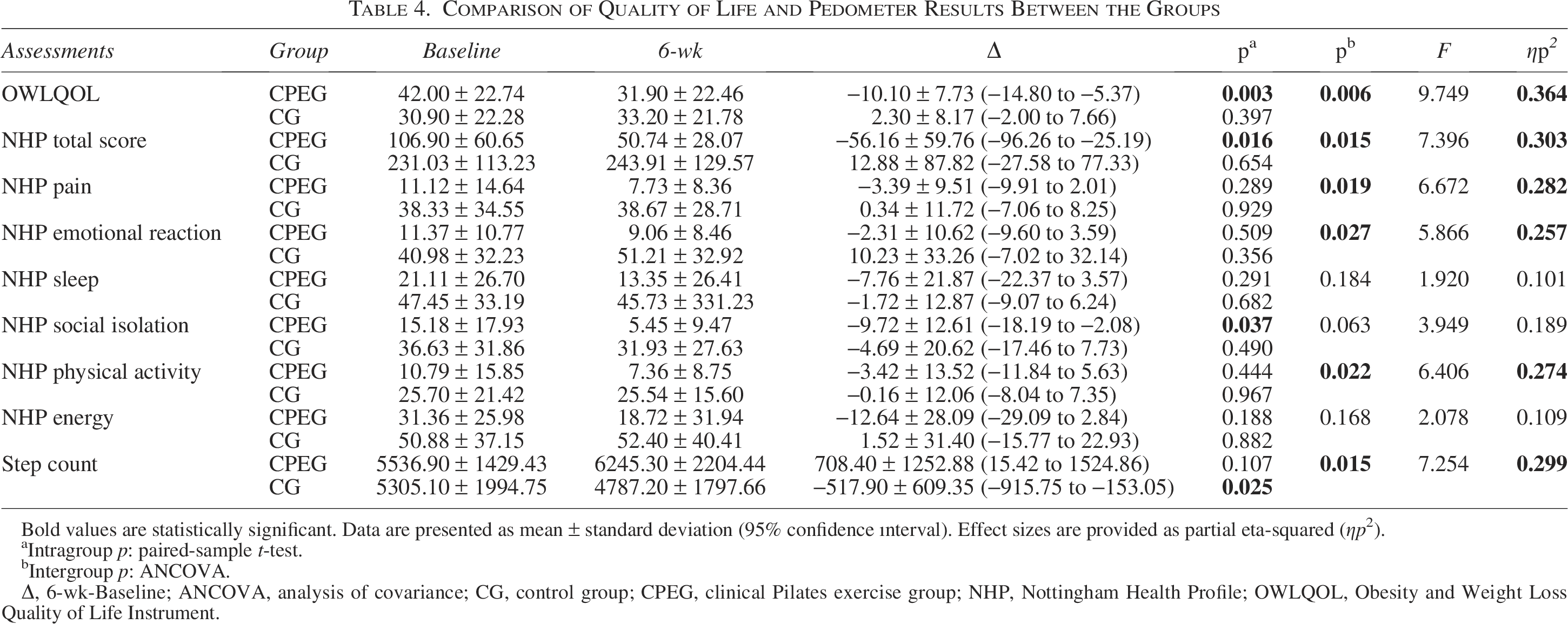
Bold values are statistically significant. Data are presented as mean ± standard deviation (95% confidence ınterval). Effect sizes are provided as partial eta-squared (ηp2).
Intragroup p: paired-sample t-test.
Intergroup p: ANCOVA.
Δ, 6-wk-Baseline; ANCOVA, analysis of covariance; CG, control group; CPEG, clinical Pilates exercise group; NHP, Nottingham Health Profile; OWLQOL, Obesity and Weight Loss Quality of Life Instrument.
In the between-group comparison, there was a greater decrease in step count in the CG (p = 0.015). The between-group ES for step count was large (ES; ηp2: 0.29) (Table 4).
Discussion
This study demonstrated that 6-week clinical Pilates exercises performed through telerehabilitation could improve functionality, physical fitness, and QoL in individuals who had undergone BS.
There are a few studies that have shown the effects of exercises following BS on body composition, functional capacity, and QoL. However, there is no consensus on the type, duration, and intensity of exercise.6,7 In the literature, only one study was found that examined the effects of core exercises after BS. Abdelraouf et al. 30 reported that 8 weeks of core exercises performed through telerehabilitation resulted in an improvement in 6-MWD and core stability. The present study found that Pilates exercises might have similar effects even when performed for shorter periods and with less frequency.
It is reported that exercise and PA after BS will generate additional benefits in functional capacity, and these gains are greater within the first 6 months. 31 In this present study, there was an increase of ∼29 m in 6-MWD in the CPEG and a significant decrease of ∼7 m in CG at the end of the 6 weeks. According to Wooldridge et al., the minimal clinically important difference for the 6-MWD in adults with obesity is 100 feet (≈30 m). 32 In the CPEG, the change in 6-MWD was statistically significant and nearly met the threshold for clinical meaningfulness. Studies found that 6-month functional exercise programs consisting of a combination of aerobic and resistance exercise provided a ∼30–36.55 m increase in 6-MWD after BS.33,34 Another recent study examining the effectiveness of an 8-week core exercise program showed that there was an increase of ∼35 m in the exercise group in 6-MWD after BS. 30 The present study also revealed that Pilates exercises performed at less intensity had a similar effect on functional capacity. In addition, in this study, individuals were included in the exercise program within an average of 6 months after BS. This supports the literature, showing that gains in functional capacity are greater in the first 6 months, even though the type and intensity of exercise are different.
The 8-FUGT is a practical measurement tool for assessing agility and dynamic balance in different diseases. Ozturk and Duruturk 35 stated that a 6-week exercise training performed through telerehabilitation during the COVID-19 isolation period in individuals with overweight and obesity provided a significant decrease in the 8-FUGT time of the online exercise group, similar to the present study. Also, Coleman et al. 33 reported an improvement in 8-FUGT performance in the exercise group in the short-term, following a functional resistance exercise program after BS. It is known that Pilates enhances balance and agility in individuals with obesity. 12 The results of the present study show that there are similar effects after BS.
In a study comparing sit-and-reach test distances measured before BS, at 6 and 12 months postsurgery, it was demonstrated that increased postoperative weight loss corresponded to increased flexibility and a correlation was found between flexibility and weight loss. 36 Another study revealed that 12 weeks of resistance exercise resulted in a significant increase in sit-and-reach distance. 37 As a result of the present study, although there was an improvement in the chair sit-and-reach test distance in the CPEG, this was not statistically significant compared with the CG. This may be due to the participants not achieving adequate weight and BMI loss to achieve an improvement in flexibility, as mentioned in the above studies.
A systematic review 38 showed that exercise, especially resistance training, effectively increased both upper and lower extremity strength after BS. When extremity movements and resistance equipment are added to the basic principles of clinical Pilates exercises, muscle strength increases. 12 It has been noted that 8 weeks of online mat Pilates exercises with resistance equipment increase muscle strength without any change in body composition in individuals with obesity. 39 On the other hand, Mundbjerg et al. 5 found no significant increase in muscle strength after a 6-month endurance and resistance exercise program. In the present study, a significant increase was observed in the muscle strength of the lower trapezius and gluteus maximus as evaluated using a hand dynamometer, as well as in the upper body strength assessed with the arm curl test. The difference in the results of the studies may be due to differences in muscle strength measurement tools. A systematic review found a large ES (1.37) for muscle testing determined using a 1 MT after BS, while reporting a medium ES (0.47) for a dynamometer. 38 Especially considering the muscle mass and maximum contractions of individuals with obesity, hand dynamometers become a more assessor-dependent evaluation tool.
In obesity, factors such as increased intra-abdominal pressure, abdominal fat accumulation, and excessive load on the vertebrae can affect core stability. 30 Arman et al. 40 found that an 8-week core stabilization exercise program for individuals awaiting BS yielded positive results in postoperative core stability. Abdelraouf et al. 30 reported significant improvements in lumbopelvic stability after an 8-week core exercise training after BS. The results of the present study demonstrated that clinical Pilates exercise led to improvements in core stability, similar to the findings of previous studies.30,40 This improvement is an expected result considering the basic principles of clinical Pilates exercises.
After BS, patients typically experience an average weight loss of 32% of their preoperative weight within 2 years. This weight loss occurs in both fat and muscle mass. 41 In a systematic review, combined aerobic and resistance exercise programs were effective in weight loss after BS. 42 However, Carretero-Ruiz et al. 43 reported that exercise training did not provide additional weight loss compared with standard postoperative care. In a meta-analysis, it was concluded that exercise training after BS provided an additional weight loss of 2.5 kg and an additional loss of fat mass of 2.7 kg. However, it has been found that exercise is ineffective in preserving lean body mass after BS, and the difficulty in preserving lean body mass may be attributed to reduced protein intake. 44 In our study, both groups continued their individualized diets including appropriate protein intake and supplements in the obesity polyclinic. Although the clinical Pilates exercise program did not create intergroup differences, body weight, BMI, and body fat percentage decreased, metabolic age improved, and muscle mass was preserved in the CPEG. In the literature, the effect of exercise on body composition after BS shows contradictory results. This may be due to heterogeneity in the type and duration of exercise.
A recent systematic review demonstrated that both health-related QoL and obesity-specific QoL improved within 1–2 years following BS. 45 In addition, it has been reported that the improvement in QoL is associated with the amount of weight loss and satisfaction with the surgery. Jassil et al. 46 reported that the highest improvement occurred within 12 months following BS. Obesity-specific QoL and health-related QoL were questioned and showed improvement in favor of the CPEG in the present study. This improvement might be associated with enhancements in functionality and the positive effects of exercise on body image.
Previous studies suggested that it was more appropriate to evaluate PA after BS using objective tools. 6 In this study, the step counts were recorded weekly using a pedometer by following these recommendations. At the end of the 6th week, although the CPEG preserved its step count, there was a significant decrease in the step counts in the CG. These results may indicate that pedometers do not have an encouraging quality without follow-up with regular meetings and calls because, in the present study, the CG received a single session of PA counseling but was not followed up with weekly calls or face-to-face meetings throughout the study.
Telerehabilitation has been reported to help individuals undergoing BS adhere to recommended lifestyle changes and cope with exercise barriers. Also, it was reported that participants felt the positive effects of exercising at home, away from social stigma and the competitive environment of traditional gyms. 46 Consistent with the mentioned study, participant’s compliance with the exercise program was good, and no negative effects were experienced throughout the present study.
This is the first study to examine the effects of clinical Pilates exercises in the postoperative period after BS and one of the earliest to evaluate their delivery via synchronous telerehabilitation, providing early evidence for this population and contributing to the literature. The limitation of the study is that participants were included between the 2nd and 15th months after surgery. As discussed, gains in functionality are greater in the first 6 months after surgery. This wide time interval may have affected the response to exercise and the results of the study. In addition, in the CG, beyond the initial PA counseling session, no structured follow-up phone calls or motivational interviewing was provided to maintain exercise adherence, which may also be considered a limitation and could have influenced the participants’ PA levels and other outcomes in the CG.
Conclusion
To the best of our knowledge, this is the first randomized controlled study to investigate the effects of clinical Pilates exercises on functionality and physical fitness following BS. The results showed that clinical Pilates exercises performed through telerehabilitation 2 days/week for 6 weeks improved functional capacity, muscle strength, and core stabilization. Clinical Pilates exercises also improved both obesity-specific QoL and health-related QoL. Further studies are needed to examine the longer term results of clinical Pilates exercises and compare them with other types of exercise.
Authors’ Contributions
The role of the authors in this study is as follows: A.A.Y.: Conceptualization, data curation, investigation, methodology, and writing—original draft; G.K.A.: Conceptualization, methodology, formal analysis, resources, and writing—review and editing; B.F.C.: Conceptualization, methodology, formal analysis, and writing—review and editing; N.A.: Data curation, formal analysis, and writing—review and editing; E.K.: Conceptualization, methodology, formal analysis, and writing—review and editing. All authors commented on previous versions of the article and approved the final version of the article to be submitted.
Footnotes
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This work was supported by the Health Institutes of Turkiye Research Fund (grant number 28092).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.