
Abstract
Background:
Obesity is a multifactorial condition linked not only to physical health risks but also to significant psychological distress. Depression, weight-related experiential avoidance, and negative automatic thoughts are common in individuals seeking bariatric surgery, yet their interrelationships remain underexplored.
Objective:
This study aimed to examine the relationships between depressive symptoms, weight-related experiential avoidance, and negative automatic thoughts in individuals eligible for bariatric surgery.
Methods:
A total of 75 adult participants with a mean body mass index of 45.9 (SD: 6.13) who met clinical criteria for bariatric surgery were recruited from endocrinology and general surgery outpatient clinics. Participants completed the Beck Depression Inventory (BDI), the Automatic Thoughts Questionnaire (ATQ), and the Acceptance and Action Questionnaire for Weight-Related Difficulties—Revised (AAQW-R). Group comparisons were made based on BDI scores, and Pearson correlations and linear regression analyses were conducted.
Results:
Fifty-five (73.3%) of the participants reported clinically significant depressive symptoms. Significant group differences were found for ATQ, AAQW-R total, and its subscales related to self-stigma and life interference (p < 0.05) between the depression group and the minimal or no depression group. Regression analysis showed that negative automatic thoughts (ATQ) significantly predicted depressive symptoms (β = 0.595, p < 0.001).
Conclusion:
Negative automatic thoughts are a stronger predictor of depression than psychological inflexibility in bariatric surgery candidates. Interventions targeting maladaptive thinking patterns may improve psychological outcomes in this population.
Introduction
Obesity is a multifactorial disorder resulting from the interaction of genetic, environmental, and behavioral determinants. It is associated with an elevated risk of chronic comorbidities and increased mortality.1,2 According to the World Health Organization’s (WHO’s) Global Burden of Disease Report, obesity affected one in eight individuals worldwide in 2022. The report estimated that approximately 2.5 billion adults were overweight, of whom 890 million were obese. Since 1990, the global prevalence of adult obesity has more than doubled, while adolescent obesity has increased more than fourfold. 3 According to the WHO, 60% of adults in Europe are overweight or obese, with rates rising rapidly in countries such as the United Kingdom, Germany, and Italy. Türkiye has the highest prevalence, with 66% of its population affected. 4 Obesity is primarily diagnosed using body mass index (BMI), waist circumference, and assessment of health impairments related to excess body fat. BMI is calculated by dividing a person’s weight in kilograms by the square of their height in meters. The WHO classifies obesity by BMI: 30–34.9 is Class 1 obesity; 35–39.9 is Class 2 obesity; and 40 and above is Class 3 obesity. 5 Obesity is associated with an elevated risk of numerous diseases and conditions that contribute to increased mortality, including type 2 diabetes mellitus, cardiovascular diseases, metabolic syndrome, chronic kidney disease, hyperlipidemia, hypertension, nonalcoholic fatty liver disease, certain cancers, obstructive sleep apnea, osteoarthritis, and depression. 6
Obesity is frequently accompanied by social stigma and discrimination in settings such as the workplace, schools, and health care. Affected individuals often encounter negative stereotypes, social exclusion, and bias, which may contribute to diminished self-esteem, depression, and a reduced quality of life. 7 Obesity is associated with adverse psychological outcomes, including depression, body image disturbance, low self-esteem, and increased stress. These mental health challenges are frequently intensified by stigma and discrimination, further limiting social participation and diminishing quality of life. 8
Large meta-analyses and cohort studies indicate that bariatric surgery is associated with significant reductions in depressive symptoms, with the greatest improvements occurring within the first year. Notably, symptom improvement is observed in the short term (0–4 months), medium term (5–12 months), and long term (more than 12 months), with the most substantial effect reported in the medium term.9,10 However, these benefits may attenuate over time, and some patients develop recurrent or new-onset depression several years postoperatively.9,11 Research shows that many patients seeking bariatric surgery experience depressive symptoms. A 2018 study found that 58% exhibited mild to severe depression, along with changes in their eating behaviors. 12 In another study conducted in 2011, the prevalence of depressive disorder measured by SCID was found to be 35% among 107 patients before surgery. 13 In 2018, Alabi and colleagues reported that depression was present at baseline in 45.2% of patients before bariatric surgery. 14
Psychological flexibility, defined as the ability to adapt to changing circumstances and maintain engagement in valued behaviors despite distress, has been relatively underexplored, although related evidence highlights the importance of psychological and behavioral adaptability for successful postsurgical adjustment. Patients who cope flexibly, manage setbacks effectively, and adjust expectations realistically are more likely to adhere to lifestyle changes and achieve better psychological well-being.15,16 Psychological inflexibility refers to a low level of psychological flexibility skills and is associated with experiential avoidance (EA). 17 A 2013 study recruited participants from a bariatric surgery clinic during follow-up care. Weight-related EA in bariatric surgery patients showed moderate correlation with the Depression Anxiety Stress Scales, suggesting a link between psychological flexibility and depression. 18
No studies currently available in the literature specifically examine “automatic thoughts” (spontaneous, often negative, self-critical thoughts) in bariatric surgery patients. However, research consistently shows that cognitive and psychological factors—such as depression, anxiety, and cognitive function—play a significant role in postsurgical adjustment and mental health. Improvements in depressive symptoms and cognitive function are commonly reported after bariatric surgery, suggesting that negative thought patterns may also improve, although this has not been directly measured.19,20
This study aimed to investigate the relationships between depressive symptoms, psychological flexibility (measured as weight-related EA), and negative automatic thoughts in individuals eligible for bariatric surgery. Specifically, the study sought to examine whether higher levels of EA and more frequent negative automatic thoughts are associated with greater depression severity in this population. It was hypothesized that participants with elevated depressive symptoms would exhibit increased weight-related EA and a higher frequency of negative automatic thoughts compared with those with minimal or no depression.
Methods
Sample and procedure
An a priori power analysis was performed using G*Power software to assess between-group differences, with alpha set at 0.05, power = 0.80, and a large effect size (Cohen’s d = 0.80). The analysis showed that at least 21 participants per group (42 in total) were needed. In addition, for a multiple regression analysis with two predictors, assuming alpha = 0.05, power = 0.80, and an expected partial R2 of 0.30, the required sample size was 40 participants.
Patients who visited the outpatient endocrinology and general surgery clinics were invited to participate in the study. Participants aged 18–65 who were eligible for bariatric surgery and gave consent were included. In this study, bariatric surgery eligibility criteria from the European Association for the Study of Obesity were used. Indications included a BMI ≥40 kg/m2 or a BMI ≥35 kg/m2 with obesity-related comorbidities. 21 Participants were individuals who met these criteria and agreed to take part in the study after providing informed consent. Individuals who did not meet the above criteria or did not provide informed consent were excluded from the study. A total of 165 eligible patients were informed about the study. The 83 volunteers gave consent, and 75 provided sufficient data for analysis. Data for 75 participants were obtained entirely from medical records, and all participants completed the study questionnaires in one session with no missing items. In contrast, 12 individuals with incomplete data were excluded from the study. Participants who were under endocrinology care as bariatric surgery candidates were invited to the study, as this provided a practical and feasible way to recruit them within a clinical setting where the target population was readily accessible. No incentives were given to the participants.
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Başakşehir Çam and Sakura City Hospital Ethics Committee (Date: July 10, 2024; No: 83). Interviews were conducted with participants, during which they were informed of the study’s nature and purpose. Written informed consent was obtained from all participants before data collection. The study was conducted at a research hospital in Istanbul, Türkiye, with a capacity of 2,721 beds that actively performs bariatric surgery. The data collection team consisted of an endocrinologist and a psychiatrist who evaluated the eligibility of bariatric surgery candidates prior to surgery. Following the interviews, participants completed a set of self-report questionnaires. Data were collected between July 2024 and October 2024 using a demographic information form, Beck Depression Inventory (BDI), Acceptance and Action Questionnaire for Weight-Related Difficulties—Revised (AAQW-R), and the Automatic Thoughts Questionnaire (ATQ).
Measurements
Demographic data form
Developed by researchers for this study, it includes questions about age, gender, BMI, and medical history.
Beck Depression Inventory
This instrument was developed by Beck to assess the severity of depression. This scale includes 21 items. Each item is scored from 0 to 3, and the total score is calculated by summing all item scores. Higher scores reflect greater depressive symptoms. The BDI demonstrates high internal consistency (r = 0.86–0.93), good interrater reliability, and strong construct and criterion validity (r = 0.65–0.67). The BDI uses cutoff points to classify depression severity as minimal or no depression (0–9), mild (10–18), moderate (19–29), or severe (30–63). 22 The Turkish version of the BDI was adapted by Hisli (1988), who established its validity and reliability in a Turkish sample, demonstrating satisfactory internal consistency and test–retest reliability (r = 0.65). A Pearson correlation of r = .50 was found with the depression scale of the Minnesota Multiphasic Personality Inventory. 23 In this study, Cronbach’s alpha was 0.908, indicating excellent internal consistency.
The Acceptance and Action Questionnaire for Weight-Related Difficulties—Revised
This form was developed by Palmeira et al. to measure weight-specific EA. It consists of ten items across three subscales: food as control (AAQW-R-fc), weight as a barrier to living (AAQW-R-wb), and weight stigma (AAQW-R-ws). The AAQW-R-fc assesses the tendency to use food as a coping strategy for negative emotions. The AAQW-R-wb evaluates how much one’s weight or body shape impedes the ability to lead a valued life. The AAQW-R-ws captures experiences of self-stigma related to weight. Higher scores reflect greater EA. The AAQW-R total score and its three subscales demonstrated good internal reliability, with Cronbach’s alpha values ranging from 0.73 to 0.88. 24 The AAQW-R has been adapted into Turkish by Burhan and Kuru. Cronbach’s alpha coefficients for the AAQW-R subscales ranged from 0.781 to 0.825, indicating good internal consistency for both the overall scale and its subscales in the adaptation study. 25 In this study, Cronbach’s alpha coefficients for the AAQW-R total score and subscales ranged from 0.656 to 0.870, indicating acceptable to good internal consistency.
The Automatic Thoughts Questionnaire
This form was developed by Hollon and Kendall to assess the frequency of negative automatic thoughts associated with depression. It consists of 30 items rated on a 5-point Likert scale, where respondents indicate how often they experience each thought. It has five subscales: Negative Self-concept, Confusion and Escape Fantasies, Personal Maladjustment and Desire for Change, Loneliness/Isolation, and Automatic Giving up/Helplessness. This tool is used to evaluate automatic negative thinking patterns. The ATQ demonstrates excellent internal consistency, with split-half reliability of 0.97 and Cronbach’s alpha of 0.96 (p < 0.001). 26 Şahin conducted the Turkish validity and reliability. Cronbach’s alpha was 0.93, indicating excellent internal consistency in the adaptation study. 27 In this study, Cronbach’s alpha coefficients for the ATQ total score and subscales ranged from 0.728 to 0.967, indicating good to excellent internal consistency.
Statistical analysis
The data were evaluated using Jamovi version 2.3.19.0. The level of statistical significance was set at p < 0.05, with correction for multiple comparisons applied to adjust p-values and reduce the risk of false-positive results arising from conducting statistical tests. Continuous variables (age, BMI, and scores of psychological measurements) were presented as means and standard deviations or medians with interquartile ranges, while categorical variables were shown as frequencies and percentages (%). To compare differences in continuous variables between independent groups with potentially nonnormal data, the Brunner–Munzel test with 10,000 random permutations was used. The more common Wilcoxon–Mann–Whitney test relies on equal variances, making it less robust when these assumptions are violated. In contrast, the Brunner–Munzel test requires fewer assumptions within the parametric framework and is therefore recommended as a more reliable and robust alternative. The Brunner–Munzel relative effect indicates that values closer to 0.50 reflect smaller group differences, whereas values further away from 0.50 indicate larger group differences between the compared groups. 28 To analyze relationships between continuous variables of BDI, ATQ, and AAQW-R, Pearson correlation and regression analyses were performed. Due to the experimental nature of the Brunner–Munzel test and the sensitivity of regression analysis to missing data, participants with missing data were excluded from the analyses.
Results
Demographic and clinical data
Participants’ ages ranged from 18 to 65, with a mean age of 36.3 (SD: 10.2). Of the total, 66 were female (88.0%), 53 (70.7%) were married, and 22 (29.3%) were single. The average BMI was 45.9 (SD: 6.13) with a minimum of 39.0 and a maximum of 68.9. Demographic and clinical data are summarized in Table 1.
Demographic and Clinical Data, Difference Between Groups
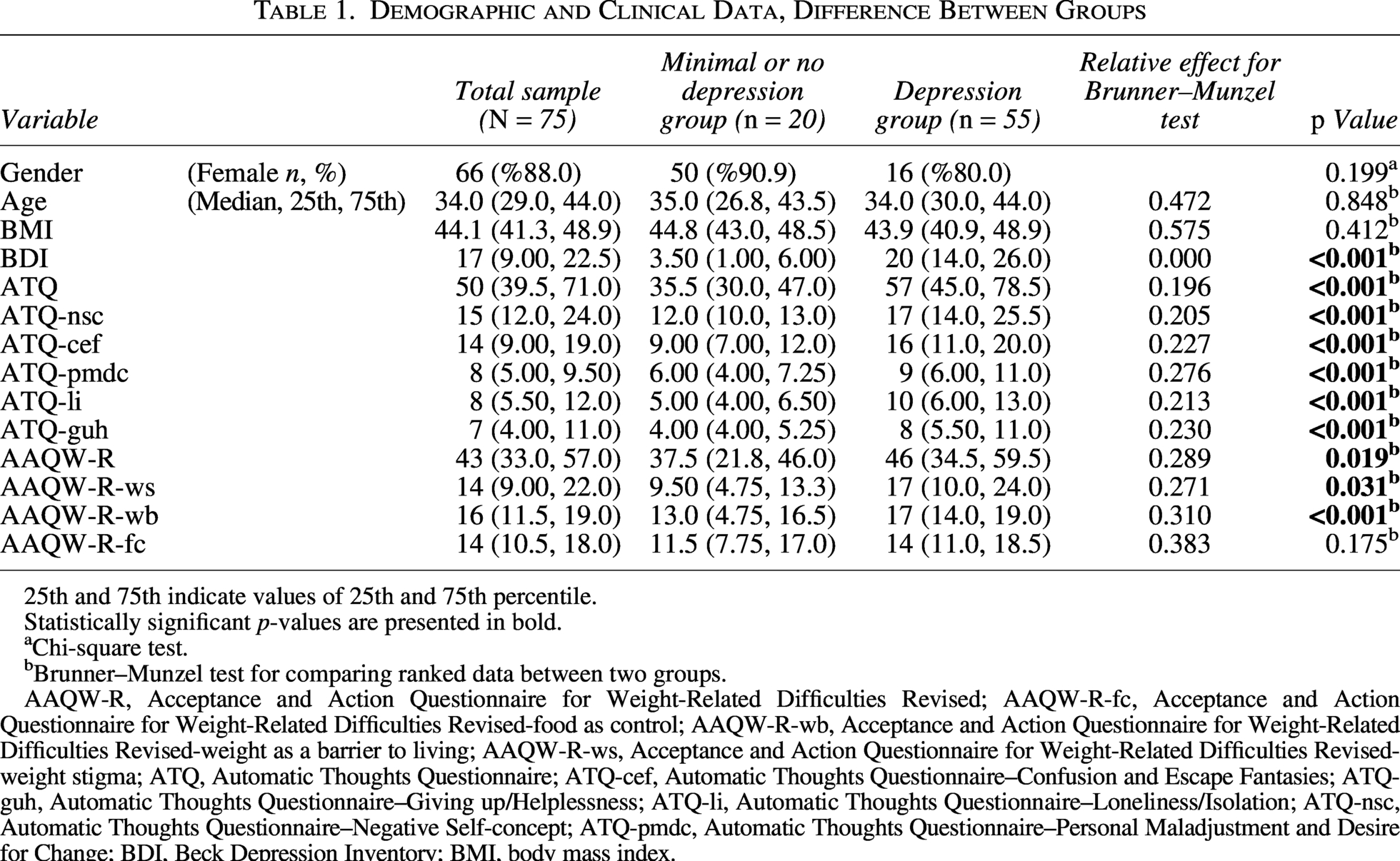
25th and 75th indicate values of 25th and 75th percentile.
Statistically significant p-values are presented in bold.
Chi-square test.
Brunner–Munzel test for comparing ranked data between two groups.
AAQW-R, Acceptance and Action Questionnaire for Weight-Related Difficulties Revised; AAQW-R-fc, Acceptance and Action Questionnaire for Weight-Related Difficulties Revised-food as control; AAQW-R-wb, Acceptance and Action Questionnaire for Weight-Related Difficulties Revised-weight as a barrier to living; AAQW-R-ws, Acceptance and Action Questionnaire for Weight-Related Difficulties Revised-weight stigma; ATQ, Automatic Thoughts Questionnaire; ATQ-cef, Automatic Thoughts Questionnaire–Confusion and Escape Fantasies; ATQ-guh, Automatic Thoughts Questionnaire–Giving up/Helplessness; ATQ-li, Automatic Thoughts Questionnaire–Loneliness/Isolation; ATQ-nsc, Automatic Thoughts Questionnaire–Negative Self-concept; ATQ-pmdc, Automatic Thoughts Questionnaire–Personal Maladjustment and Desire for Change; BDI, Beck Depression Inventory; BMI, body mass index.
Differences between groups based on levels of depressive symptoms
The total sample was divided into two groups based on BDI scores. Participants with a scale score greater than 9 were classified into the depression group (mild: 10–18, moderate: 19–29, and severe: 30–63), and those with a score of nine or below were categorized as the minimal or no depression group. Accordingly, 55 (73.3%) participants were classified into the depression group, and 20 (26.6%) participants were classified into the minimal or no depression group. The Brunner–Munzel test showed significant differences between the groups on ATQ and the subscales AAQW-R, AAQW-R-ws, and AAQW-R-wb (p < 0.05). No significant differences among Age, BMI, or AAQW-R-fc (p > 0.05). The results are presented in Table 1.
Relations among scales
Pearson correlation and linear regression analyses were performed to explore the relationships between depression, psychological rigidity, and automatic thoughts. Regression analysis showed that negative automatic thoughts significantly predicted depressive symptoms, while weight-related EA did not explain unique variance. The model accounted for 47.4% of the variance in depression scores. A multiple linear regression analysis was conducted to examine whether ATQ and AAQ-WR scores significantly predicted depression severity as measured by the BDI. Low multicollinearity (VIF = 1.34) indicates that the predictors contribute independently. Normality of residuals was assessed using Shapiro–Wilk and Kolmogorov–Smirnov tests, both of which were nonsignificant (p > 0.05), indicating that the assumption of normality was met. Homoscedasticity was assessed using the Breusch–Pagan, Goldfeld–Quandt, and Harrison–McCabe tests, all of which were nonsignificant (p > 0.05). Residuals showed no clear pattern and were randomly scattered, indicating that the assumptions of linearity and homoscedasticity were met. The overall model was statistically significant and explained a substantial proportion of the variance in BDI scores (R = 0.688, R2 = 0.474), indicating that approximately 47.4% of the variability in depressive symptoms was accounted for by the predictors. ATQ emerged as a strong and significant predictor of depressive symptoms (B = 0.252, SE = 0.0419, t = 6.021, p < 0.001), with a standardized coefficient (β = 0.595) indicating a large effect size. The 95% confidence interval [0.398, 0.792] further supports the robustness of this association, suggesting that higher levels of negative automatic thoughts are strongly linked to increased depression severity. In contrast, AAQW-R did not significantly predict BDI scores (B = 0.113, SE = 0.0708, t = 1.601, p = 0.114), although its standardized coefficient (β = 0.158) indicated a small, nonsignificant positive association. The results of Pearson correlation and linear regression analyses are shown in Tables 2 and 3.
Pearson Correlations Among Scales
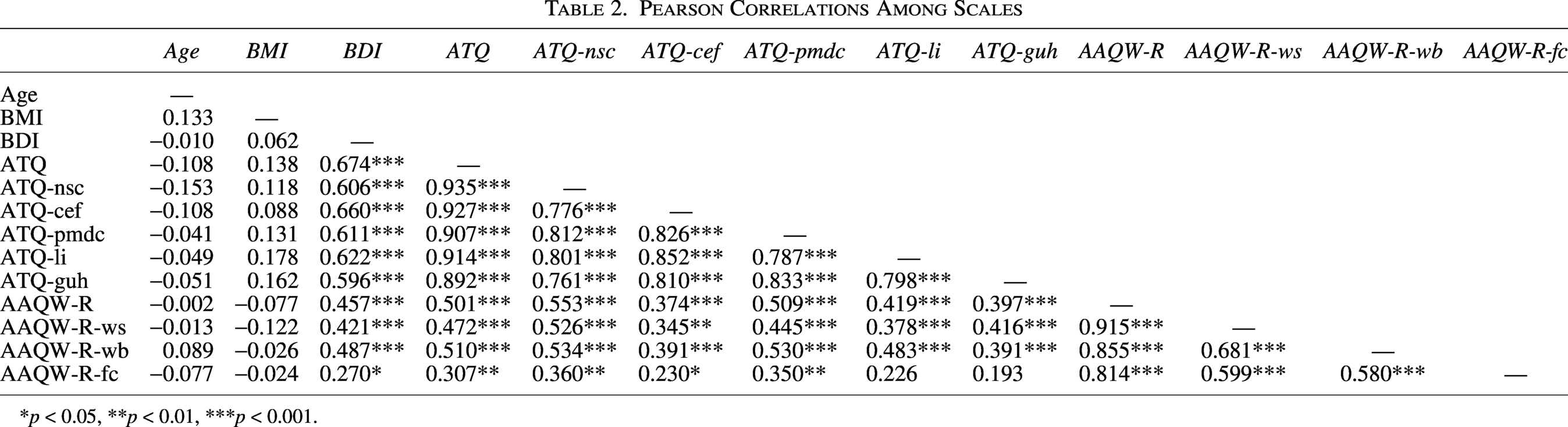
*p < 0.05, **p < 0.01, ***p < 0.001.
A Linear Regression Model Was Used to Predict BDI Scores Based on ATQ and AAQW-R as Predictors
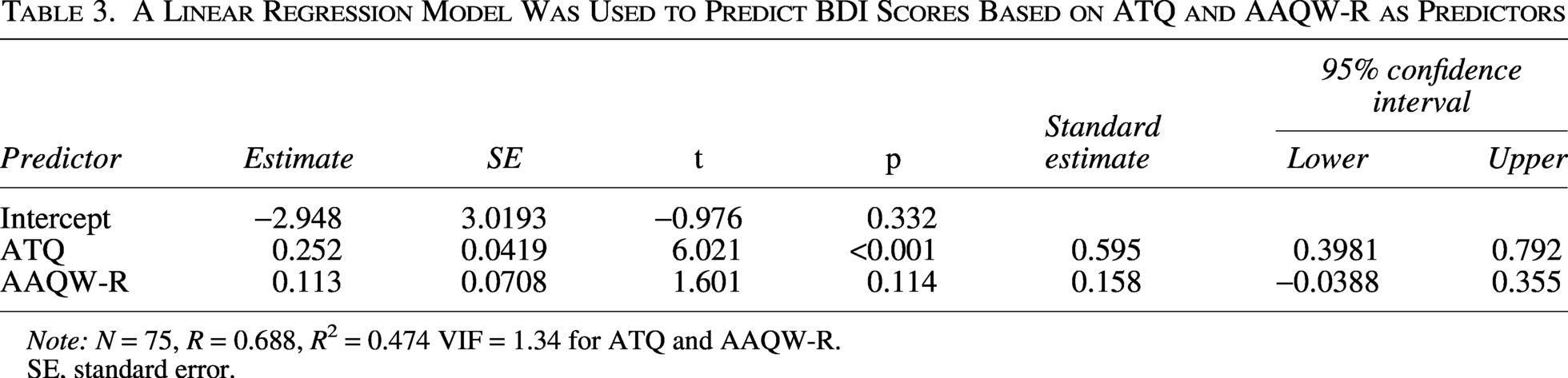
Note: N = 75, R = 0.688, R2 = 0.474 VIF = 1.34 for ATQ and AAQW-R.
SE, standard error.
Discussion
The current study examined the relationships among automatic thoughts, psychological inflexibility related to weight, and depressive symptoms in a sample of bariatric surgery candidates. Correlation and regression analyses showed connections between depressive symptoms and both negative automatic thoughts and weight-related EA. When comparing participants with and without clinically significant depressive symptoms, those in the depression group reported significantly higher levels of negative automatic thoughts and weight-related EA.
BMI shows weak or nonsignificant correlations with most psychological variables. This is likely due to the limited variability in BMI within the sample, as all participants were classified as obese, with BMI values ranging from 39.0 to 68.9. The restricted range reduces the likelihood of detecting meaningful associations between BMI and psychological constructs. Prebariatric surgery patients with obesity experience poorer physical and mental health-related quality of life, linked to weight bias internalization, low self-esteem, and increased psychological distress, including anxiety and depression. In a study of 73 patients, 45.2% had baseline depression, with 2.7% having severe symptoms. Overall, these patients show high rates of psychiatric disorders, with affective disorders, anxiety disorders, and binge eating disorder being the most common. Depression prevalence among morbidly obese patients varies between 23% and 69%.13,14,28 In the current research, 73.3% of participants were classified into the depression group (mild, moderate, or severe), which is somewhat higher than the previously mentioned rates. This difference may be due to variations in measurement methods. Cultural and regional differences should also be taken into consideration.
Significant differences were observed in depressive symptoms and related psychological measures. The depression group had significantly higher scores on the ATQ total score, and all its subscales, including Negative Self-Concept (ATQ-nsc), Confusion and Escape Fantasies (ATQ-cef), Personal Maladjustment and Desire for Change (ATQ-pmdc), Loneliness/Isolation (ATQ-li), and Giving Up/Helplessness (ATQ-guh) (all p < 0.001). Based on existing research, there are no studies like the current results that examine the relationship between depression and automatic thoughts in obesity. However, some studies have explored the relationship between automatic thoughts and other psychological factors. A 2019 study with adult obese participants found strong negative correlations between automatic thoughts and both self-esteem and mindfulness, indicating that higher automatic negative thoughts are associated with lower self-esteem and mindfulness levels. 29 A longitudinal study conducted in 2013 with 55 adolescents, aged 15–18, investigated the association between automatic negative thoughts, eating disorder symptoms, and weight discrepancies, revealing that higher levels of negative thoughts were linked to increased disordered eating behaviors and greater dissatisfaction with body weight. 30 A survey carried out in 2014 found that the Binge Eating Obesity group scored higher on the ATQ and depression measures compared with the non-Binge Eating Obesity group. 31 Current results may state a potential relationship between automatic thoughts and eating behaviors in obesity. It can be concluded that further research is needed to explore the interplay between depression, automatic thoughts, and eating attitudes in individuals with obesity. BDI shows strong positive correlations with the total ATQ score and all its subscales, this can be highlighting a robust association between depression and automatic negative thoughts. However, the current analysis does not explore how individual ATQ subscales might uniquely contribute to depression. Given the high intercorrelations among the subscales, possible multicollinearity could be a concern in multivariate analyses. Future studies should consider using multiple regression with collinearity diagnostics or mediation analysis to clarify the unique and indirect effects of specific automatic thought patterns. BDI shows a strong correlation with ATQ and all its subscales, supporting the connection between negative automatic thoughts and depression. 26
At a general level, high ATQ scores may indicate persistent negative automatic thoughts, aligning with the Cognitive Theory of Depression. 32 In daily life, this may manifest as constant self-criticism, reduced confidence in routine tasks, and a tendency to interpret neutral situations negatively. Each subfactor may be associated with problems in different areas of life or with different psychological difficulties. Lower self-esteem and fear of criticism from others or oneself can lead individuals to try to escape or suppress uncomfortable thoughts and emotions rather than address them directly. 25 These patterns can impair productivity, decision-making, and motivation. Negative self-concept is closely tied to body image and self-worth. Obese participants showed more negative thinking patterns and greater body dissatisfaction than normal-weight individuals. 33 Individuals may internalize societal stigma weight, leading to beliefs of inadequacy or unattractiveness. The harmful impact of stigma is associated with depressive symptoms, impaired psychological functioning, worsening medical conditions, and a tendency toward avoidance behaviors such as reduced participation in social, professional, or physical activities. 34 Confusion and escape fantasies reflect cognitive overload and a desire to disengage. In everyday functioning, this may appear as difficulty concentrating, indecisiveness, or reliance on avoidance coping (e.g., excessive screen time, emotional eating).35,36 Such patterns can disrupt routines, reduce the ability to sustain goal-directed behavior, and may constitute a form of EA. Personal maladjustment and the desire for change reflect dissatisfaction with one’s current state and may motivate lifestyle efforts; however, they often coexist with frustration and a sense of being “stuck,” while cycles of negative, maladaptive thoughts and coping patterns such as binge eating in response to minor weight gain can be counterproductive and demotivating, with repeated unsuccessful attempts further intensifying this cycle and reducing persistence over time. 37 Loneliness/Isolation captures perceived social disconnection. Weight-related stigma and self-consciousness can contribute to withdrawal from social interactions, reducing access to support networks and increasing vulnerability to emotional distress. 38 Giving up and helplessness reflect a sense of futility and are linked to weight regain.37,39 This can impair daily functioning by reducing initiative, adherence to health behaviors, and resilience in the face of setbacks. This state of helplessness and hopelessness may be related to depressive symptomatology.
Together, these cognitive patterns contribute to a cycle in which negative thoughts reinforce functionality, underscoring the importance of addressing cognition alongside physical health in overweight and obesity. All these subscales show moderate to strong positive correlations with BDI, which may emphasize the complex cognitive patterns associated with depressive symptoms. It is important to note that, in these comparisons, the total sample was divided into two groups based on BDI scores. Participants scoring above 9 were classified as the “depression group,” while those scoring 9 or below were categorized as the “minimal or no depression group.” It can be emphasized that this “depression group” includes individuals with at most mild depressive symptoms (BDI scores 10–18), which are not necessarily indicative of clinically diagnosed major depressive disorder. Therefore, the reported prevalence of depression should be interpreted with caution, as it may overestimate clinically significant depression rates compared with studies using diagnostic interviews or stricter clinical criteria. Furthermore, reporting the distribution of participants across the mild, moderate, and severe BDI categories would provide a clearer, more nuanced understanding of the sample’s symptom severity.
Regarding weight-related EA, the AAQW-R total score (p = 0.019), Weight Stigma subscale (AAQW-R-ws, p = 0.031), and Weight as a Barrier to Living subscale (AAQW-R-wb, p < 0.001) were significantly higher in the depression group. At the same time, no significant difference was found for the Food as Control subscale (AAQW-R-fc, p = 0.175). Moderate positive correlations also exist between BDI and the AAQW-R total score and its three subscales, highlighting the link between depression and weight-related EA. The AAQW-R includes three subscales: Food as Control (AAQW-R-fc), which assesses the tendency to use food as a coping strategy for negative emotions; Weight as a Barrier to Living (AAQW-R-wb), measuring how much a person’s weight or body shape interferes with living a valued life; and Weight Stigma (AAQW-R-ws), which captures experiences of internalized weight-related stigma. The significant differences observed in AAQW-R-ws and AAQW-R-wb may be explained by their stronger association with depressive symptomatology. Weight-related self-stigma and perceiving weight as a barrier to living can be closely linked to negative self-evaluation, social withdrawal, and reduced quality of life, which are core features of depression. The lack of a significant difference in AAQW-R-fc may be due to emotional eating being a common coping strategy across obese individuals, regardless of depressive symptom severity, combined with limited variability within the sample and the construct’s weaker specificity to depression compared with other subscales. These findings may demonstrate the complex relationship between depressive symptoms, negative thought patterns, and psychological inflexibility related to weight among bariatric surgery candidates. A potential limitation of the study is the limited variability in the sample, as all participants were individuals with obesity in a relatively high BMI range (39–68.9). Emotional eating, as measured by the AAQW-R-fc subscale, may already be elevated in this population, potentially leading to a ceiling effect. This limited variability may have reduced the statistical power to detect significant differences between groups. The relationship between psychological problems, including depression, and psychological flexibility in individuals with overweight and obesity is well established.34,35 In a study involving 468 individuals seeking behavioral weight loss treatment, depressive symptoms were found to have a significant association with psychological flexibility. 36 Unhealthy eating habits that contribute to weight gain, along with certain coping behaviors, may indicate EA. For example, ruminative thoughts about weight loss and eating to suppress unwanted emotions can lead to weight gain. 25 In adults with overweight or obesity seeking treatment, higher levels of EA and lower engagement in valued actions were significantly associated with reduced quality of life, decreased satisfaction with social roles, and increased symptoms of depression, anxiety, and binge eating. 40 Obesity-related self-stigma, including self-devaluation and fear of stigma, is linked to EA, which may contribute to overall psychological symptoms such as depression and shame, thus worsening mental health and emotional well-being.18,24,35,41
A linear regression analysis was conducted to examine the predictive power of automatic thoughts (ATQ) and weight-related EA (AAQW-R) on depressive symptoms (BDI) among bariatric surgery candidates. The overall model was significant (p < 0.001), indicating that the predictors accounted for a meaningful proportion of variance in depression scores. As shown in Table 3, ATQ emerged as a significant predictor of BDI scores (β = 0.595, p < 0.001), suggesting that higher levels of negative automatic thoughts are strongly associated with increased depressive symptoms. In contrast, AAQW-R did not significantly predict BDI scores (β = 0.158, p = 0.114). These findings indicate that while weight-related EA is related to depression at the univariate level, it does not contribute unique variance when controlling for general automatic thoughts. BDI and ATQ, both grounded in the cognitive theory of depression, may have shown a stronger relationship due to shared focus on negative thoughts and patterns, leading to greater conceptual overlap than weight-related EA. A study that also used the BDI to assess depressive symptoms reported that treatment gains were greater with cognitive therapy, which follows cognitive hypotheses, than with Acceptance and Commitment Therapy (ACT), which is based on the psychological flexibility model. 41 However, studies also indicate no significant difference between the two therapies.42,43
Limitations
The main concern of this study was the relationship between BDI and ATQ, as both were developed based on the cognitive theory of depression, which likely explains their stronger association. Since both assess negative mental patterns and automatic thoughts linked to depressive symptoms, they share considerable conceptual overlap. This overlap may lead to higher correlations compared with weight-related EA. Using depression scales that capture features beyond those assessed by the BDI could offer more diverse insights into the complexity of depression. In addition, the cognitive model may be more effective than the psychological flexibility framework in explaining depression. On the contrary, the BDI has long been used for over six decades in numerous studies to assess the level of depression, and its relationship with psychological flexibility has also been demonstrated. 17
First, the use of a nonrandom, convenience sampling method limits the generalizability of the results, as participants were recruited from a single hospital setting and may not represent the broader population of bariatric surgery candidates. Second, the cross-sectional design prevents any conclusions about causality between depressive symptoms, automatic thoughts, and weight-related EA. Longitudinal studies are necessary to clarify the directionality of these relationships. Third, all data were collected through self-report measures, which may be subject to response biases such as social desirability or inaccurate self-assessment. In addition, the relatively small sample size may have limited the statistical power to detect smaller effects, especially in regression analyses. Furthermore, depression was assessed using the BDI, which is a self-report screening instrument and does not provide a clinical diagnosis. Therefore, the identified “depression group” reflects elevated depressive symptoms rather than clinically diagnosed major depressive disorder, which is often what is measured in the comparative literature using structured clinical interviews such as the SCID. This distinction should be considered when interpreting prevalence rates and group comparisons. Finally, although the study focused on psychological inflexibility related to weight, other relevant variables, such as eating behaviors, body image dissatisfaction, or trauma history, were not examined. These could be important confounding or mediating factors. Future research should address these limitations to obtain a more comprehensive understanding of the psychological processes involved in this population.
Conclusion
This study examined the relationships among depressive symptoms, negative automatic thoughts, and weight-related EA prior to bariatric surgery. Individuals with more significant depressive symptoms experienced higher levels of negative automatic thoughts and weight-related EA compared with those with little or no depression. Results of regression analyses suggest that maladaptive cognitive patterns may be more central to depressive symptoms in this population than weight-specific psychological inflexibility, though some methodological and theoretical limitations warrant careful interpretation (e.g., sample size, conceptual overlap between the BDI and the ATQ). This result may reflect a measurement artifact, as the BDI places substantial emphasis on cognitive symptoms. Findings of the current research suggest that bariatric surgery candidates who experience depressive symptoms may exhibit a specific psychological vulnerability characterized by frequent negative automatic thoughts and heightened psychological inflexibility. This pattern indicates that individuals may be more prone to cognitive rigidity and EA, making it difficult for them to disengage from distressing thoughts and emotions. As a result, these maladaptive cognitive and emotional processes may contribute to both psychological distress and difficulties in long-term weight management. Clinically, these results suggest the importance of routinely screening bariatric candidates for depressive symptoms, automatic thoughts, and EA before and after surgery. Both cognitive behavioral therapy (CBT) and ACT are effective in supporting patients with weight-related issues. Clinicians can use both CBT and ACT to promote cognitive change. They can combine CBT and ACT by integrating cognitive restructuring and behavioral activation with mindfulness and acceptance to better address negative thoughts and psychological inflexibility.32,44,45 Together, they can target emotional eating, self-stigma, and body dissatisfaction. Clinicians should use CBT to challenge maladaptive beliefs and ACT to build psychological flexibility, distress tolerance, and commitment to long-term health goals before and after bariatric surgery, improving both psychological and behavioral outcomes. Future research should explore longitudinal pathways to better understand causal mechanisms and consider broader BMI ranges to assess whether these patterns generalize across weight statuses.
Authors’ Contributions
Concept/Design: S.B., H.Ş.B., and O.G.; data acquisition: S.B. and F.B.A.; data analysis/interpretation: S.B. and H.Ş.B.; drafting article: S.B. and H.Ş.B.; critical revision of article: F.B.A.; final approval and accountability: O.G.; technical or material support: O.G. and H.Ş.B.; supervision: O.G.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.