
Abstract
Background:
Understanding nurses’ awareness, experience, and recommendations regarding the prevention of patient falls during bariatric surgery is critical to strengthen patient safety and improve the quality of care. This study aimed to determine in depth the experiences of operating room (OR) nurses regarding patient falls during bariatric surgery and their opinions and suggestions for the prevention of patient falls.
Materials and Methods:
The study is qualitative. It was conducted with 14 OR nurses working in a hospital in Turkey. Data were collected through in-depth interviews using a semistructured questionnaire. MAXQDA Software, a qualitative data analysis tool, was used.
Results:
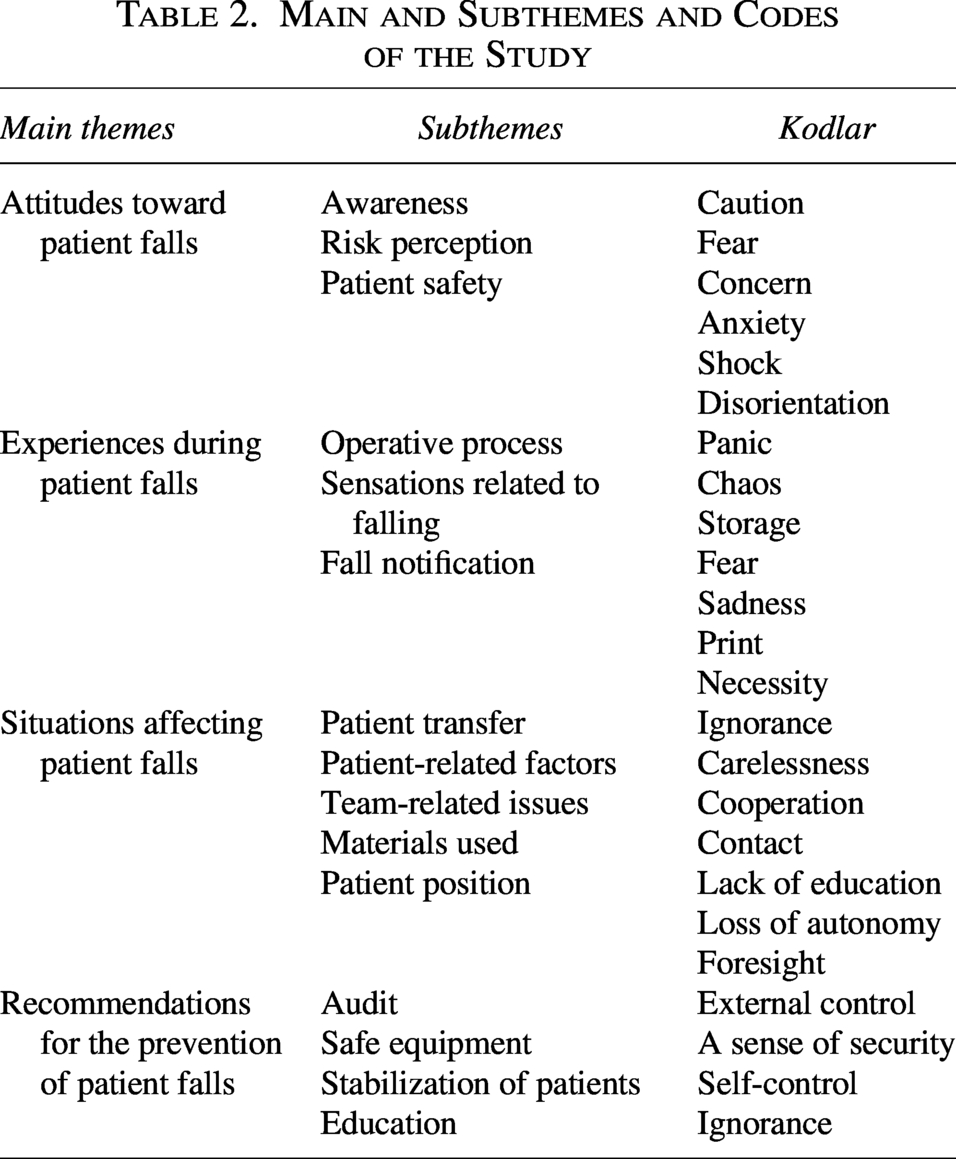
In the findings of the study, a total of 4 themes (attitudes toward patient falls, experiences during patient falls, situations affecting patient falls, and suggestions for preventing patient falls), 15 subthemes, and 23 codes were identified.
Conclusions:
It was determined that OR nurses who experienced patient falls were meticulous about taking precautions intraoperatively. During bariatric surgery, the patient should be immobilized, safe surgical equipment should be used, and health care professionals should be trained in this regard.
Introduction
Patient falls are a common and significant patient safety issue worldwide and continue to be a problem. 1 Patient falls can occur in a variety of settings, including both inpatient and outpatient locations. It can also occur and is important in perioperative areas, such as the operating room (OR), preoperative area, postanesthetic care unit, and ambulatory surgical facilities. 2 In falls occurring in perioperative services, patients are in the high-risk group due to reasons such as surgery, narcotic medication, and limited mobility. 3 Falls in the perioperative area, unlike falls in traditional ward or outpatient settings, can be conceptualized as uncontrolled patient movements and fall risks occurring during preoperative transfer, stretcher-to-operating-table transitions, positioning, and intraoperative patient movement/transfer. 4 Patients with obesity require special care to prevent falls during surgery. The obesity of patients undergoing bariatric surgery and the special positions (especially upright Trendelenburg, reverse Trendelenburg, or side-to-side rotation) during surgery increase the risk of falls. Related patient falls can result in fatalities. 5 If the necessary precautions are not taken in this position, patient falls are inevitable. 6 Perioperative personnel have an important role in preventing OR falls. 5
The risk of obese patients falling during surgery increases due to an inappropriate operating table for the patient and inadequate stabilization of the patient. In addition, faulty movements of the surgical team and sudden, unexpected movements of obese patients contribute to this risk. 2 In a study of 15 Chinese bariatric surgery case management nurses, it was observed that bariatric surgery patients were specialized, and the focus was on their general care needs. However, the lack of data regarding falls in patients undergoing bariatric surgery is striking. 7 In the study of Kouhestani et al., it was reported that the OR staff’s specific knowledge of care in laparoscopic bariatric surgery was moderate and that they did not adequately comply with the standards of care for patients undergoing laparoscopic bariatric surgery. 8 It was determined that this noncompliance was due to inadequate training or lack of established standards in hospitals. 8 In addition, it has been reported that positioning obese patients increases the risk of injury in the perioperative environment. 9 It has been reported that an obese patient whose seat belt was not sufficiently secured fell off the table during surgery and died after the incident. 10 It has been found that nurses do not want to care for obese surgical patients because of fear of dropping the patient and inability to meet the care needs of the patients. 11 Although there have been studies on the challenges of caring for obese patients in intensive care 12 and clinical settings, 13 research on the safety of these patients during an invasive procedure, such as bariatric surgery, is limited. 14 This suggests that further research is needed to better understand the specific safety risks encountered during bariatric surgery and strategies to reduce these risks.
It may be very difficult to find solutions without identifying the difficulties and problems experienced in nursing care and analyzing in-depth experiences. 15 Considering these studies, the experiences of OR nurses regarding patient falls during bariatric surgery should be reviewed in terms of patient safety. This study aimed to determine the experiences of OR nurses regarding patient falls during bariatric surgery, as well as their opinions and suggestions for the prevention of patient falls.
Research question
What are nurses’ awareness, experiences, and recommendations for preventing falls during bariatric surgery?
Methods
Research approach
The study is a qualitative content analysis study conducted through semistructured interviews to understand individuals’ experiences of patient falls during the bariatric surgery procedure. 16 The design and conduct of our study conformed to the Consolidated Criteria for Reporting of Qualitative Studies checklist. 17
Setting
The study was conducted between March and April with nurses working in the OR units of a tertiary research and practice hospital located in the Central Anatolia Region of Turkey.
Sampling strategy
Criterion-based sampling, one of the purposeful sampling types, was used to determine the participants in the study. Criterion sampling is the selection of individuals who will participate in the sample according to certain criteria. 18 In this study, the criteria of “working in the OR for at least 5 years” and “actively participating in bariatric surgery” were taken as a basis for nurses to observe patient falls in the OR. In the literature, it is emphasized that the sample size in studies using the qualitative research method can be determined according to the saturation point of the answers given to the research questions, and generally 5–25 participants are sufficient. 19 In this direction, the interviews continued until the answers received from the participants started to repeat and the research was completed with a total of 14 nurses.
Protection of participants’ rights (IRB)
Ethics committee approval was obtained from the “Ethics Commission” of a state university to conduct the study (Decision No: 12/54 Date: 20.03.2024). Then, institutional permission was obtained from the hospital where the study was conducted. In addition, OR nurses were informed about the study before starting the study, and written and verbal consent was obtained from the participants. The study was conducted in accordance with the principles of the Declaration of Helsinki (WTO General Assembly, Fortaleza, Brazil, October 2013) and the Law on Medical Research Involving Human Subjects.
Data collection methods and instruments
Data were collected using a semistructured interview form. Interview is an effective data collection tool for understanding the feelings, thoughts, attitudes, and experiences of individuals. 20 During the interview, the researcher has the opportunity to examine the private expressions of the participant. 21 In particular, semistructured interview forms allow the researcher to make changes in the questions (changing the question, adding or removing new questions) within the general framework during the interview and to reveal different dimensions of the subject. 20 For this reason, semistructured interview form was preferred in this study.
In the process of preparing the semistructured interview form, the researcher first conducted a literature review on the subject and prepared a semistructured interview form consisting of five open-ended questions using the data obtained.2,22,23 Three experts, one of whom is an academic in the field of measurement and evaluation and two of whom are academicians in the field of nursing and have completed their doctorate degrees, were consulted about the interview form. In line with the data obtained from the expert opinions, the interview form was re-examined by the researcher in terms of clarity, appropriateness, and adequacy of the questions, and one more question (sixth question) was added to the interview form to further deepen the interview questions. The interview questions used in the study are given in Table 1.
Semistructured Interview Questions

To evaluate the comprehensibility and applicability of the semistructured interview form, three nurses were preapplied, and the OR nurses were asked for their opinions about the form. OR nurses stated that the research questions were appropriate and did not have any suggestions. Nurses with whom a preapplication was made were not included in the study.
Participants were informed about the subject of the interview in advance, and appointments were made for a time when surgery was not planned and they were available. Each participant was given a code (Participant/P1,…P14) before starting the interview. Interviews were conducted by the first researcher in a quiet, brightly lit, and appropriately heated room in the hospital where the participants worked. The second researcher also participated in the interviews to take notes on important points. The interviews were recorded using a voice recorder. The first researcher maintained constant eye contact with the participants during the interviews and provided feedback to the participants’ answers. The shortest interview was 20 min with participant 5, and the longest interview was 37 min with participant 4. The audio recordings were replayed, and a total of 36 pages of raw data documents were obtained in Microsoft Word. All researchers had academic experience in qualitative research. Data saturation was determined based on the following criteria: no new codes or themes emerging in new interviews, repetition of existing themes, and theoretically sufficient saturation of conceptual categories. The sample size was reduced as data repetition increased and no new meaningful conceptual content emerged as the interviews progressed.
Data management, analysis, and transferability
Thematic analysis was used to analyze the data obtained from the research. Thematic analysis is a method that aims to systematically identify and organize the themes in a data set and present meanings related to them. 24 Braun and Clarke proposed a six-stage model for thematic analysis. In accordance with this model, in the first stage of the research, the interviews were listened to several times to familiarize with the data and then transcribed. 25 The transcribed data were numbered from 1 to 14. The entire 36-page document was then re-examined to identify commonalities and expressions. In the second stage, the data were critically evaluated to create codes. Words or word groups within the scope of the research topic were identified as codes. In the third stage, themes and subthemes were obtained by combining the codes obtained from all research data. In the fourth stage, the themes and subthemes were evaluated by two researchers (second and third), and a consensus was reached. In the fifth stage, whether the themes met the answer to the research question and the names of the themes were checked again. In addition, to ensure internal consistency and confirmability, the opinions of the experts who gave opinions in the preparation of the research questions were taken again about the themes and subthemes. Necessary arrangements were made in line with the suggestions. In the sixth stage, the researchers created the report including 4 themes and 15 subthemes (Table 2).
Main and Subthemes and Codes of the Study
The validity and reliability of the data obtained as a result of the research were addressed in line with the criteria of credibility, transferability, consistency, and confirmability determined by Lincoln and Guba. 26 To ensure credibility, the interview forms prepared by the researcher were presented to the expert opinion, and the participants were interviewed after the necessary arrangements were made. In addition, the credibility of the research was tried to be increased by directly transferring the data obtained from the participants in the findings section. To ensure the transferability of the research, the research model, participants, data collection tools, implementation phase, and the analysis of the data obtained were expressed in detail. To ensure consistency, voice recordings were made with the participants’ permission, and these recordings were stored in secure environments. In addition, all interviews were conducted by the first researcher. Confirmability was ensured by asking field experts to compare the raw data with the reported themes.
Results
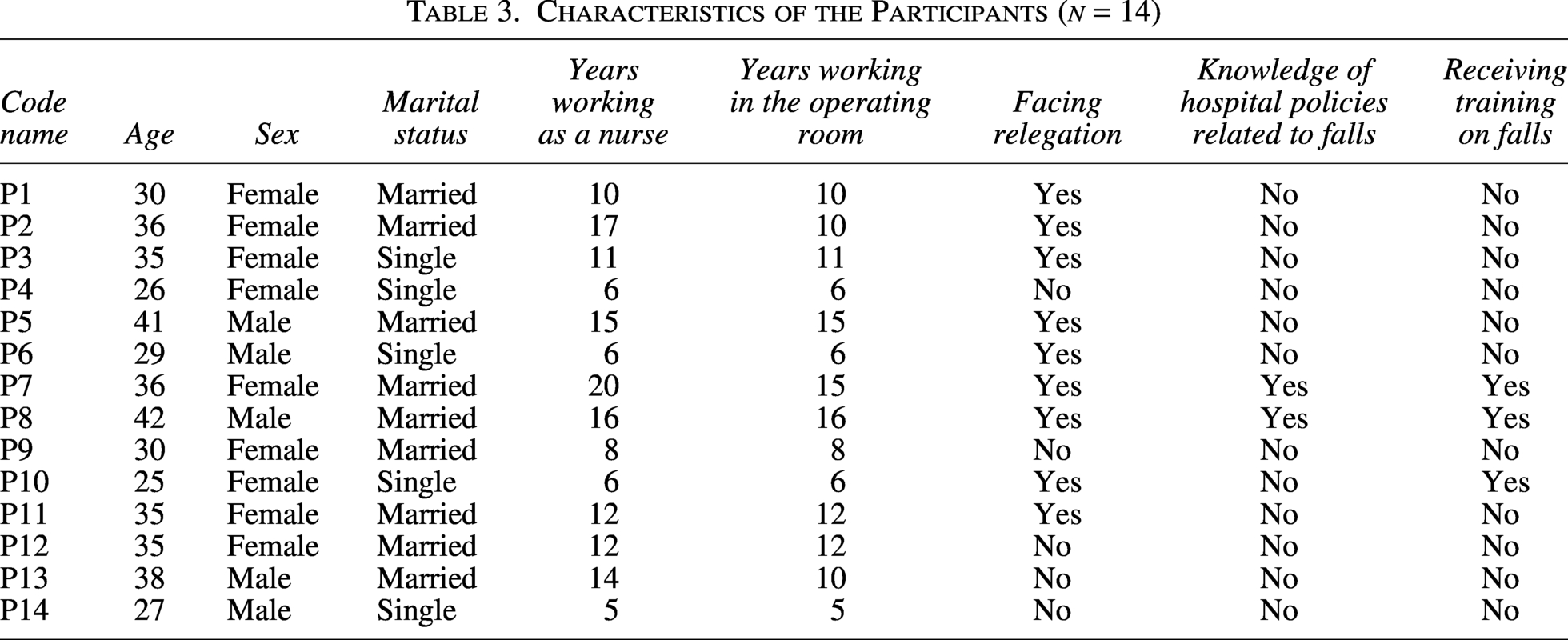
In the thematic analysis of the study, 4 main themes, 15 subthemes, and 23 codes were identified (Table 2). The descriptive characteristics of the participants are detailed in Table 3.
Characteristics of the Participants (n = 14)
Main theme 1. Attitudes toward patient falls
Almost all participants stated that patient falls during bariatric surgery were an important problem for both themselves (such as distortion of the sterile field and fear of not being able to hold the patient) and patients. Nurses (n = 9) who had previously experienced intraoperative patient falls emphasized that all kinds of measures should be taken to prevent such incidents from happening again. In addition, more than half of the participants emphasized that the most important factor during surgery was ensuring patient safety.
“I mean, such falls are risky for the obese patient… In an instant, the whole position can be disrupted, the operating table can fall apart, sterilization can be disrupted. It is risky for an obese patient to fall in every respect.” (Participant 2)
“I would probably lose all my orientation in an instant. We get over it very fast. You have to go back to work immediately, we question what they can do at that moment. I mean for the patient.” (Participant 5)
“I am afraid of something happening to the patient. Sometimes we are more upset than the patients… the patient is obese, so the safety of these patients is more important than anything else.” (Participant 3)
Main theme 2. Experiences during patient falls
When the process experienced patient falls during bariatric surgery was questioned, OR nurses explained the process. Eight out of the nine participants who experienced a patient fall stated that after the patient fell during the operation, they put the patient back on the operating table, checked whether there was a fracture or dislocation, and decided whether to continue the operation according to the patient’s condition. Furthermore, the majority of participants who experienced a fall were very upset, scared, and panicked during the fall. While some of the participants who experienced patient falls during bariatric surgery emphasized that patient fall notifications were made, another part stated that they did not know what was done about these notifications.
“As a team, we lift the obese patient and put them in place. We put the patient in supine position. The radiologist comes to see if there is a fracture or dislocation. So, of course, we interrupt the surgery at that time. If the patient has an open area, we concentrate on finishing the procedure immediately. We have to continue. The operation is continued in a sterile way and the patient is washed and dyed again.” (Participant 4)
“I don’t know about informing in the next process…” (Participant 7).
“Now there are incident reports. Since our patient collapsed directly on the doctor, we did not send him for an extra x-ray or anything like that. We immediately grabbed him and put him on the table. We had a lot of difficulty.” (Participant 1)
Main theme 3. Situations affecting patient falls
When all participants were asked about the situations affecting patient falls during the OR, all participants emphasized that patient falls were caused by patient positioning. Most participants (n = 11) stated that patient falls were not caused by patient-related factors, while the rest (n = 3) stated that they were patient-related. Some participants also stated that patient falls occurred during patient transfer or due to faulty practices by the surgical team. More than half of the participants stated that the materials used during bariatric surgery were unsuitable for obese patients.
“Since the patient is kept asleep for a long time, I think that there are patient falls caused entirely by the personnel and the materials used. In other words, the causes of patient falls are only not factors arising from the patient.” (Participant 12)
“… this situation is a problem caused entirely by the team.” (Participant 11)
“There may be cases of patients falling during the transfer from the transfer stretcher to the operating table. Because we usually use sheets in this transfer… we hold the edges of the sheets and transfer the patient from the transfer stretcher to the operating table with the command. In other words, we did not have special equipment to slide the patient onto the operating table. Therefore, if the sheets used (while transferring the patient to the operating table) tear, the patient can fall directly onto the floor.” (Participant 14)
“The biggest risk factor is that the patient is obese…” (Participant 6)
“One of the important factors is that the materials must be strong and there must be special obesity equipment. Therefore, we are trying to do our best as much as possible…” (Participant 9)
“Because bariatric surgery takes a long time and the patient is asleep for a long time, the most important risk factors here are not restraining the patient and not being careful when positioning.” (Participant 13).
Main theme 4. Recommendations for the prevention of patient falls
Almost all of the participants stated that patients should be stabilized carefully and consciously to prevent falls during surgery, and team cooperation should be ensured while positioning the patient. More than half of the participants (n = 8) emphasized that the OR team should be supervised to ensure that they take the necessary precautions to prevent falls during bariatric surgery. Some participants mentioned the importance of using appropriate and safe equipment for patients. More than half of the participants stated that the OR team should receive in-service training regarding patient falls.
“For example, there are apparatuses that facilitate transportation in the form of sliding only under the patient, they can be obtained from them.” (Participant 11)
“I think it would be better if there were restraints or stretchers for obese patients.” (Participant 6). “For example, trainings can be organized for health professionals to emphasize the importance of this issue to raise awareness.” (Participant 14)
“The thing that puts all of these at risk is that the employees are not experienced enough, they do not have enough training and they cannot successfully tie the patient.” (Participant 2)
Discussion
Unfortunately, despite the advances in technology and the health care system today, patient falls still occur in ORs and continue to be a problem. 27 Especially in bariatric surgery, the obesity of the patient and the position given to the patient further increase the risk of patient falls. 10 Therefore, OR nurses and other members of the team have important responsibilities to prevent obese patients from falling. 28 In this study, we examined in depth the awareness, experiences, and recommendations of OR nurses regarding patient falls during bariatric surgery. The study identified a total of 4 themes (attitudes toward patient falls, experiences during patient falls, situations affecting patient falls and recommendations for the prevention of patient falls), 15 subthemes, and 23 codes.
Almost all of the OR nurses included in this study stated that it is important to ensure patient safety during surgery and that there may be disruptions in the surgical process when a patient fall occurs. In the literature, it is emphasized that nurses who have adequate attitudes and awareness about patient falls play an important role in reducing the prevalence of patient falls and the rate of patient falls in the hospital. 29 Similarly, in this study, it was determined that OR nurses who experienced patient falls during bariatric surgery were more meticulous about the subject and supervised the patient more strictly in terms of patient falls during surgery. It can be said that the awareness of the OR nurses who experienced this situation increased even more.
In a case study on the fall process of an obese patient during surgery, a similar process was mentioned as in this study. In the case presentation of Prielipp et al., it was reported that a 60-year-old male obese patient was given the reverse Trendelenburg position and fell because the patient was not strapped to the operating table. 2 It was stated that the initial evaluation was performed by anesthesiologists, and then, a full-body computed tomography scan was performed. It was reported that the patient did not undergo any surgical intervention due to severe intracerebral hemorrhage. It was quite striking that there were no guidelines on the patient management process after a patient fall during surgery. It is necessary to establish evidence-based guidelines to ensure standardization in interventions performed after patient falls in the OR and to maintain effective care for patients. More studies on intraoperative patient falls are needed to establish evidence-based guidelines.
The fact that patient falls during surgery are rare 30 and the patient is obese may cause nurses to be afraid and panic. Almost all of the nurses included in this study stated that they were scared and panicked during the patient fall event and that they were very upset afterward. King et al. also reported that nurses experienced feelings such as stress, anxiety, guilt, and self-doubt about quality care after patient falls. 31 While a few of the OR nurses who participated in this study and experienced a patient fall stated that fall notifications were made, more than half of the participants stated that they did not know what was done regarding patient fall notification. The reason for this may be thought to be insufficient knowledge about incident reporting, fear of revealing the identity during incident reporting, and fear of losing their job and being sued. It may also result in investigations and lawsuits against team members after patient fall incidents and, consequently, compensation penalties. 32 Although there are very few studies in the literature focusing on patient falls in the OR, there are occasional reports of cases in the press and legal records. 10 Whereas identifying deficiencies, revealing strengths and providing the best service for patients depend on accurate and complete recording of incident reports of patient falls. 33
The causes of patient falls are complex, and patients with medical conditions, such as comorbid diseases, side effects of medications or balance, and strength or mobility problems, are particularly vulnerable and susceptible to falls. 34 In terms of these conditions, bariatric surgery patients are at significant risk for falls. In addition, obesity, age, altered consciousness, agitation, distraction and indifference of health care professionals, problems with the operating table, excesses in patient positioning, and lack of secure stabilization have been reported to cause patient falls during surgery. 2 Booth et al. emphasized that intraoperative patient falls may be caused by the operating table, staff carelessness, and obesity of the patient. 27 As stated in the present and other studies, situations such as patient-related conditions, team-related errors, inadequate equipment, and patient position increase the risk of patient falls intraoperatively. It is very important to prevent patient falls before they occur to protect both patients and health care professionals. 31 Previous studies have also emphasized the importance of training operating room staff about patient fall prevention, establishing risk screening protocols to identify patients at high risk of falls, using appropriate equipment for obese patients, ensuring adequate nursing expertise, maintaining awareness of potential hazards, and checking the operating table and locking mechanisms.23,27 These findings directly align with the patient transfer, positioning, and operating table safety principles emphasized in the World Health Organization’s Safe Surgery guidelines, The National Institute for Health and Care Excellence (NICE) perioperative safety guidance, and the Association of periOperative Registered Nurses (AORN) perioperative safety standards.35–37 The necessity of team coordination, appropriate equipment use, and standardized transfer protocols, particularly in bariatric patients with high BMI, is consistent with the themes of this study.
Limitations of the study
The most important limitation of the study is that the results cannot be generalized to the whole society since the study was conducted in one center.
Implications for perioperative nursing
This study addresses some important issues that OR nurses should pay attention to in order to minimize the risk of falls in the OR environment of patients undergoing bariatric surgery. It draws attention to important issues by evaluating the attitudes and experiences of OR nurses regarding patient falls during bariatric surgery, situations affecting patient falls, and necessary measures to prevent patient falls. In clinical practice, there is a need to increase the awareness of OR nurses regarding patient falls during bariatric surgery, early detection of risky situations, development of preventive strategies, determination of appropriate material needs, and budget planning. Further research on this subject will contribute to the development of evidence-based practices. This information is critical to ensure the safety of patients and to help the surgical process proceed smoothly.
Conclusion
As a result of the study, the awareness and event reporting of the OR nurses about intraoperative falls of obese patients undergoing bariatric surgery were inadequate. It was determined that OR nurses experienced emotional anxiety during and after the fall process. It was quite striking that there was no standard procedure in the institution after the fall. In addition, it could not be ignored that there were deficiencies in equipment and arguments for obese patients in the institution. It was necessary to take individual (training) and institutional (supervision, material supply) measures before the fall occurred. This is the first study to investigate the experiences of nurses regarding patient falls during bariatric surgery. Therefore, it is highly recommended to conduct both quantitative and qualitative studies in the future and to expand the literature on this subject.
Authors’ Contributions
All authors listed meet the authorship criteria, and all authors agree on the content of the article. O.S.A.: Conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, validation, visualization, writing—original draft, and writing—review and editing. E.O.A.: Conceptualization, data curation, formal analysis, investigation, methodology, resources, software, validation, visualization, and writing—original draft. R.H.A.: Data curation, formal analysis, investigation, methodology, resources, software, validation, visualization, and writing—original draft.
Ethical Statement
Ethics committee approval was obtained from the “Ethics Commission” of a state university to conduct the study (Decision No: 12/54; date: 20.03.2024). Then, institutional permission was obtained from the hospital where the study was conducted. In addition, OR nurses were informed about the study before starting the study, and written and verbal consent was obtained from the participants. The study was conducted in accordance with the principles of the Declaration of Helsinki (WTO General Assembly, Fortaleza, Brazil, October 2013) and the Law on Medical Research Involving Human Subjects.
Footnotes
Acknowledgments
The authors thank all participants of the study.
Author Disclosure Statement
None to report.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.