
Abstract
Cancer patients are a high-risk population and often undergo strenuous testing. One type of testing is cytology testing, which is less invasive and simpler to attain than a traditional biopsy. However, there can be errors in the cytology testing process that can lead to a loss of results, thus a delay in treatment or retesting. The purpose of this work is to utilize a systems engineering approach to understand cytology testing ordering process and identify where errors may occur. The Systems Engineering Initiative for Patient Safety (SEIPS) framework was utilized to make visual process maps with the use of SEIPS 101 tooling methods. The use of SEIPS 101 tools showed the relationships between the components of a work system. Handoff points, where information is at risk of being lost, were identified. Future work can look at the implementation of solutions to gather data on the quality improvement measures.
Introduction
Cancer patients are a high-risk population, and it is important for patients to undergo testing quickly to begin the treatment process. Testing can be challenging for patients as they wait for a diagnosis, and it can be an emotional time that affects individuals and families. In 2022, there were an estimated 1.9 million new diagnoses of cancer and 609,360 associated deaths (American Cancer Society, 2015). Not only is there a physical and emotional toll with cancer, but there is also a financial burden. It was estimated by The National Cancer Institute (2015) that the total direct medical costs were $183 billion. Cancer can be diagnosed through several different methods of testing such as physical examinations, laboratory test, imaging tests, biopsies, and cytology testing (Mayo Clinic, 2021).
Cytology testing is the test of a single cell type (Johns Hopkins Medicine, 2019). It is used for diagnostics, screenings, and identifying abnormalities in cells such as cancer. A diagnostic test is for patients that show symptoms of a disease, whereas screening tests are performed for patients that have not shown symptoms (American Cancer Society, 2015). To gather a cytology test, fluids are taken from the areas that may have cancer or cells are scraped from the possible abnormal area (American Cancer Society, 2015). Cancer patients typically are given a cytology test due to it being less invasive and easier to attain than a tissue biopsy. It is a low-risk, quick, and simple procedure that is becoming more well-known among healthcare professionals. It is also cost-effective in comparison to the normal biopsy (Al-Abbadi, 2011).
The overall cytology testing process is complex and leaves room for error. There are instances where a sample can be lost, and no results are given to the oncologist. There are also events where a sample is not tested in an appropriate time frame before becoming unusable. Data may not be transferred from each of the departments, leading to a lack of information and results even if the physical sample is not lost. If no results are given to the oncologist regarding the fluid sample, the patient needs to undergo testing again.
The consequences of an error leading to retesting in the cytology order process can have great effects on the patient. Scheduling a new appointment could be difficult in a short time frame considering the overflow of patients within the healthcare system. An early diagnosis opens the doors to more treatment options, but the longer it takes to diagnose, the less likely treatment options will help (American Cancer Society, 2015). Also, retesting a patient several times could lead to patient harm, especially when the fluid needs to be taken from a more invasive area. In the case of retesting a patient, they are potentially harmed by the risk of infection, additional anesthesia, or painful testing procedures administered to the patient.
A systems engineering approach can assist in identifying where information could be lost and where other errors could occur within the process. The Systems Engineering for Patient Safety (SEIPS) framework can show how different parts of the work system interact and how those areas could potentially lead to errors (Carayon et al., 2006). The work system is composed of five components that work in relationship with one another. The components are environment, people, technology and tools, tasks, and organization. All of these components must work with one another to have a successful process and outcome. SEIPS 101 is a simplified approach to the SEIPS framework that visualizes work systems so that they are simpler and easier to understand (Holden & Carayon, 2021). Examples of SEIPS 101 tools include checklists, people maps, task and tools matrices, and journey maps. All of these tools allow for a visual representation of the current state of the process while identifying components and their relationships. By identifying and naming what components were in every step of the process, predetermined error points were able to be pointed out (Holden & Carayon, 2021).
SEIPS has been used in previous research to identify and mitigate errors in healthcare processes. A SEIPS framework was used to understand errors that lead to the surveillance of central line-associated bloodstream infections (CLABSI) that could occur with using central venous catheters (CVCs) in a home setting (Hannum et al., 2022). Another study utilized process maps based on SEIPS to find similarities and differences between the care transitions from the operating room (OR) to the intensive care unit (ICU) and the transition from the OR to the pediatric ICU (PICU; Wooldridge et al., 2022). A process map was created from interview data to show each step of the process and how the components of a work system were integrated.
Therefore, a SEIPS approach can be used to study the cytology testing ordering to understand the process and identify where errors may occur. The objective of this work is to use a systems engineering approach to study the cytology testing order process and identify potential risks for errors.
Methods
An observational study was performed at a cancer clinic, and interviews were conducted with stakeholders of the cytology testing order process. Tools such as process maps were initially utilized to create a baseline of the process. The process maps were broken down into an information task flow, to understand how information is transferred across units, and a physical task flow, to understand how the physical cytology sample navigates the process. A SEIPS approach was applied to both the information and task process maps to show different components of the flows.
Observational Setting
The observational study was performed at <Institutional information removed for review>. The study observed a cancer clinic, diagnostic lab, and pathology lab. The diagnostic and the pathology lab are located in the same hospital as the cancer clinic and are utilized for several types of testing, including cytology.
Data Collection
Observations and interviews were conducted with oncologists, nurses, and pathologists. A series of questions about the process were prepared for each interview to ensure that complete information was gathered based on the SEIPS framework. The questions covered the role of the person being interviewed, the steps that took place in their area for cytology samples, and their perception of where the errors could be occurring. Interviews were performed in-person, on phone calls, and over virtual meetings. Observations of the radiology and surgery departments were also conducted as cytology samples could be gathered from many different departments within the cancer center. Notes were recorded electronically by three people and compared to ensure that all the information was gathered and consistent. If there were inconsistencies, follow-up emails and phone calls were made with the stockholders to clarify information.
Data Analysis
First, initial process maps were developed to understand both task and information processes. Then, two separate SEIPS-based task flows were developed: a physical task process map and an information task process map were created from the observational and interview data. The two SEIPS-based task flows were developed separately because there are two different factors of the cytology testing process: the physical task process and the information task process.
Physical Task Process Map
The physical task process map showed the physical handling and testing that nurses, providers, pathologists, and other personnel would perform as the sample is collected and tested.
Information Task Process Map
The information task process showed how data in electronic medical record (EMR) systems of the sample move throughout the process. It is focused on the electronic input and confirmation of the patient and the sample data. In the process studied, there were two different EMR systems used.
After creating the two process maps to layout the steps in the process, SEIPS 101 tool methodology was integrated into the process maps. To integrate SEIPS 101 into the initial process maps, each component was color-coded to represent a component of the work system. This is shown in Figure 1. The environment was color-coded green, organization was color-coded yellow, and the tools and technology component was color-coded purple. The people involved were represented by a blue person symbol with an abbreviation of the role that the person was in. For example, “MD” represents that a medical doctor is actively participating in the task. Every task was labeled with the relevant color-coded information. The environment could be labeled as the cancer clinic, diagnostic lab, or pathology lab. The organizational components included anything related to organizational policy and procedure. The tools and technology could be labeled as EMR 1 or EMR 2 as two separate EMR systems were utilized in the observational setting. The people possibly involved in each step were patients, providers, nurses, pathologists, and others such as lab technicians or medical assistants.

Key for SEIPS Analysis.
Results
Six interviews were conducted with nurses (n=3), oncologists (n=2), and a pathologist from the pathology lab. Observations were performed in the pathology lab of the pathology technicians, surgery, and radiology. Surgery and radiology within the clinic were observed to understand the beginning of the cytology process and how the EMR system was used to input data. The pathology lab was observed to understand the ending location of the sample. Three hours of observations were conducted. Each interview lasted around 1 hour for a total of 6 hours.
Initial Process Maps
After the interviews and observations, a physical task process map and an information task process map were created.
Physical task process map
Figure 2 shows the tasks that were taken by clinicians and pathologists with the physical sample. The physical task process map includes the patient arriving at the hospital, the physician or nurse creating a cytology order, and the patient undergoing the procedure to retrieve the sample for testing. The scope of the project is focused on cytology testing, therefore the steps for testing other samples, like biopsies, are not included in the process map.

Physical task process map.
Information task process map
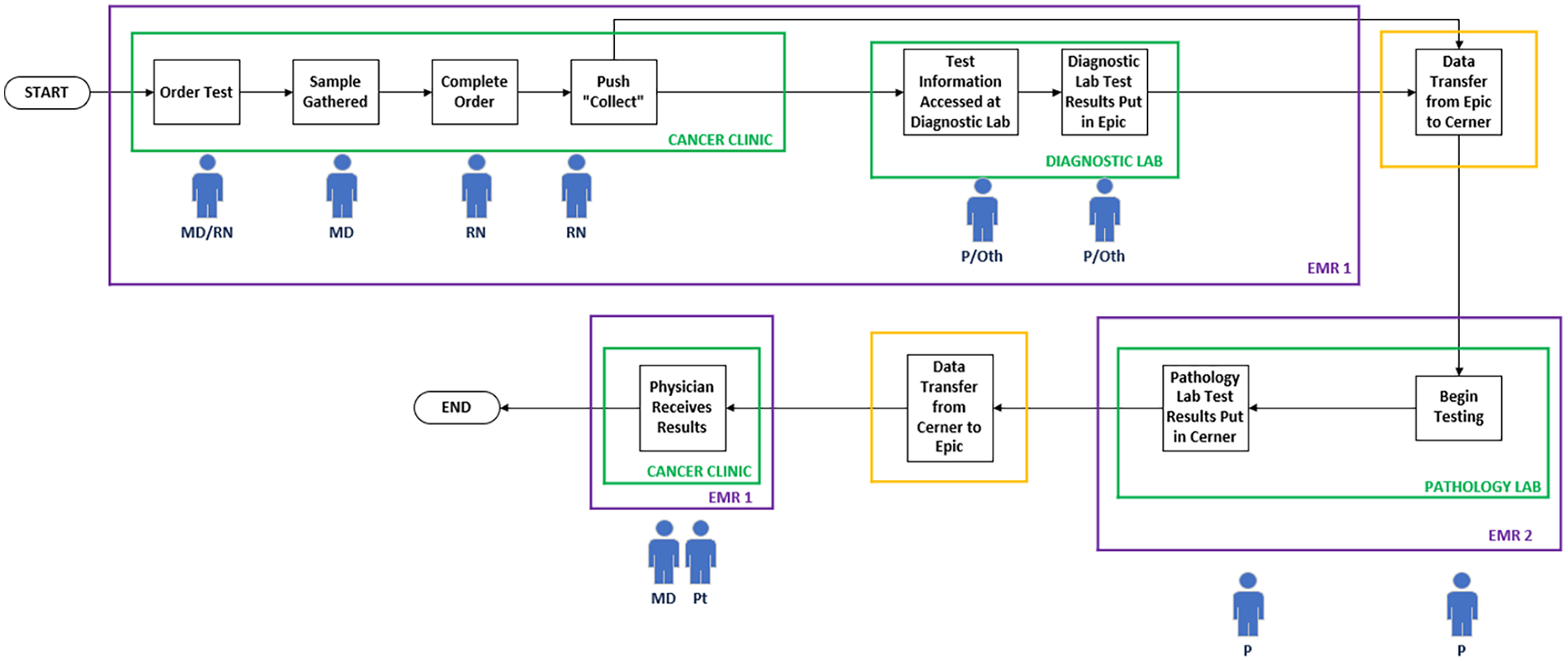
Figure 3 shows the process of tasks the clinicians and pathologists performed for the sample’s data that transitioned to the different departments of the hospital. For the information flow, two different EMR systems were used in the overall process. The cancer clinic and the diagnostic lab utilized the same EMR, while the pathology lab used another EMR. The information map demonstrates the process of the sample being gathered and tested.

Information task process map.
SEIPS-based Process Maps
Figures 4 and 5 show the process task flow and information task flow with the SEIPS framework, respectively.

SEIPS-based physical task flow.
SEIPS-based information task flow.
SEIPS-based physical task process map
For the process task flow, there are handoffs between the different physical environments. The sample goes from the cancer clinic to the diagnostic lab, and then to the pathology lab. Within these environments, there are different people involved. In the cancer clinic, the patient, providers, and nurses are involved. The nurse then physically takes the sample to the diagnostic lab where either a pathologist or technician receives the sample. After testing, the pathologist or technician from the diagnostic lab walks the sample to the pathology lab and places it in the fridge. A pathologist then retrieves the sample and performs necessary testing. Overall, there is a total of three handoffs in the physical sample process.
SEIPS-based information task process map
In the information flow, there are handoffs between the two different EMR systems. The data and information is created by a cancer center provider or nurse in EMR 1. The information remains in the same EMR as the sample is transitioned to the diagnostic lab. There, pathologists or technicians will do necessary testing and input any results into EMR 1. The information then undergoes a data transfer from EMR 1 to EMR 2 in the pathology lab. Data from testing in the pathology lab is inputted into EMR 2. At the conclusion of testing, results undergo a data transfer from EMR 2 in the pathology lab to EMR 1 in the cancer clinic. The producer will receive that information and communicate it with the patient. Overall, there are two information handoffs between the EMR systems.
Discussion
Cytology tests play an important role in the diagnosis of cancer. However, if there is an error that occurs in the physical task process or the information task process, this could become a patient safety issue. The loss of information of cytology orders is detrimental to patient care. If results are not given to given to a patient, this could delay diagnosis and treatment. Process maps utilizing SEIPS 101 were made to understand where errors could occur (Holden & Carayon, 2021). Applying each component of a SEIPS work system to each of the steps allowed for simple visual identification of potential error places. SEIPS is helpful for identifying parts of a work system in healthcare environments and is specifically helpful for focusing on patient safety (Carayon et al., 2006). The identification of the work system components allowed for simple analysis of the relationships between them and the tasks. It showed where handoffs occurred and where there could be other errors.
Overall, there were five handoffs in the cytology testing process: three in the physical sample process and two in the information process. The physical task process showed multiple handoffs between people and environments.
The information task process map showed that the handoffs between the two different EMR systems could be a possible area of error for data transfer. With handoffs between these environments and people, information can be lost (Abraham et al., 2017; Arora & Johnson, 2016).
Handoffs are necessary in healthcare settings as patients or patient samples need to be tested or treated in multiple departments. If proper steps are not taken to reduce error in handoffs, then information can be lost (Lyons, Standley, & Gupta, 2010). One reason for errors with handoffs is miscommunication (Beach, Croskerry, & Shapiro, 2003). Without information being communicated to the next person or department, then that information will be lost. Another area for error within handoffs is a lack of efficiency (Lofgren, Gottlieb, Williams, & Rich, 1990; Lyons, Standley, & Gupta, 2010). In testing a sample, there is time limitation on the plasma that is used in cytology tests (Balassanian, Ng, & van Zante, 2019). If the sample is expired, then validity in the test results can be questionable. Therefore, efficiency is necessary to have valid results for the patient.
With a loss of information or lack of efficiency that is possible in handoffs, patient results can be delayed or never received. There are many solutions for handoffs that have been studied. A study used a handoff bundle of training, standardization of verbal handoffs, and modifications to the handoff location and methods to decrease errors (Starmer et al., 2013). They also studied the use of an EMR as a handoff tool to hold the information that was needed for the handoff. The electronic tool included information such as “To Do Lists” and “Contingency Planning” to ensure all information was given to the receiving end of the handoff. It was found that implementation of this bundle was useful in decreasing errors. Electronic handoff tools can be useful to ensure no information is lost if the verbal handoff lacks essential information (Davis et al., 2015). Other studies have investigated the use of checklists to standardize handoff processes and improve the transfer of information (Agarwala et al., 2015; Halterman et al., 2019)
One limitation of this study was that there was a small sample of interviews and interviewing a wider variety of people would contribute to the work. Also, there was a small sample of observations and observations could be expanded. There was also a limited scope in that there was only one cancer clinic studied. Performing observations at multiple cancer clinics could also be done in future work. Also, the data was collected during only one time period of the year. Having a longer data collection period would be useful in understanding the process over time. Future work should investigate developing solutions for cytology handoffs to minimize errors that can occur in the process. Other version of SEIPS include the external environment, but it was not necessary for this study since the errors were occurring internally (Carayon et al., 2020). The external environment can be a future area of research.