
Abstract
This scoping review collects methods and frameworks from three fields with a shared goal of improving healthcare practice with a focus on primary care settings: Human Factors, Implementation Science, and Quality Improvement. The approaches from these three fields have been synthesized in a conceptual model that builds on complementarities between fields and encourages interdisciplinary integration. The resulting integrative model provides a helpful guide for organizing healthcare improvement approaches into a cyclical process that is consistent with real-world practice. Users of this model can select from a collection of existing approaches to support their improvement projects, develop and test new transdisciplinary approaches that combine or mix existing approaches, or guide their interdisciplinary education in primary care change approaches. Future work will refine and expand this model to balance practicality and rigor.
Keywords
Background
With over 440 million office visits annually (Santo & Okeyode, 2018), improvements in primary care could equitably improve the lives and health of nearly every person in the US (Phillips & Bazemore, 2010). However, despite recent healthcare improvements disparities in care are still present and in some cases have widened (Boonyasai et al., 2022). Primary care physicians (PCPs) are the first resource for patients with many different illnesses or health concerns, this complexity makes primary care particularly difficult to improve (Crabtree et al., 2011; Holman et al., 2016; Shi, 2012). Despite these challenges, PCPs help patients build a valuable relationship with the health system overall, leading to better health outcomes like reduced mortality (Starfield et al., 2005). Improving primary care, while challenging, is critical to the improvement of the US healthcare system and patient lives. As such, research efforts should support and guide primary care improvements.
Unfortunately, primary care is structurally distant from clinical research. The people who generate clinical evidence (e.g., new drugs, therapies, and processes) are largely disconnected from the users of that evidence (i.e., patients, PCPs, etc.). This gap is not as much physical as it is temporal: It takes 17 years on average for research evidence to be used in regular clinical practice (Balas & Boren, 2000; Morris et al., 2011). The slow infrastructures of academia and its governing bodies make up much of the delay (Balas & Boren, 2000), but implementation of evidence into practice is the critical final step to improving primary care with evidence-based practices (Holtrop et al., 2018).
Objective
Our long-term mission is to support primary care improvement efforts with research knowledge. Improving primary care is a shared goal across many fields of study, each developing and using unique approaches to achieve better care outcomes. Thus, our objective for this scoping review is to collect approaches from several fields of study: Human Factors, Implementation Science, and Quality Improvement. The approaches gathered from these fields have been assembled into a proposed integrative conceptual model for primary care improvement that builds on complementarities between the fields.
Method
To begin identifying the gaps that exist across the three literatures of focus, we performed a scoping review of articles that offer approaches to identify and overcome local contextual barriers to change in primary care. This focus on “approaches” was intentionally broad to avoid narrowing our search to only models, methods, frameworks, or processes. To be included in this review articles must 1) describe a reproducible approach that identifies barriers or addresses barriers to change, 2) come from the fields of focus for this review (human factors, implementation science, or quality improvement), and 3) be generalizable to primary care settings in the United States. International studies, though potentially valuable, were generally excluded due to definitional differences in the term “primary care.” Articles for this review were collected pragmatically via Google Scholar searches and through back searches of citations from articles identified as relevant based on the above criteria.
Results
Human Factors
Human Factors (HF) is the study of how humans interact with technologies, environments, and everything else in the world around them (Wickens et al., 2004). This field offers many approaches to improve the quality and safety of healthcare systems (Xie & Carayon, 2015), for this review we generally focus on those relating to sociotechnical systems (STS) and design. STS theory underpins the idea of work systems, or systems of people and things that interact to produce work (Alter, 2013; Pasmore, 1988). User-centered design and participatory design approaches focus on end users and may even involve them in the design process to brainstorm, provide feedback, and design prototypes (Sanders & Stappers, 2008). HF broadly focuses on the people at the center of changing systems and how we can make changes that better serve them.
Implementation Science
Implementation science (IS) focuses on clinical evidence uptake in regular practice rather than pragmatic improvements (Eccles & Mittman, 2006; Grol & Grimshaw, 2003). IS has several approaches to identifying local barriers that are similar to HF including interviews, focus groups, or surveys (Huntink et al., 2014; Krause et al., 2014; Moullin et al., 2019). In addition, IS has many useful frameworks for understanding context (Damschroder et al., 2009; Flottorp et al., 2013; Michie et al., 2005), planning and tailoring implementations (Fernandez et al., 2019; Michie et al., 2013; Powell et al., 2015; Waltz et al., 2019), and defining outcomes (Damschroder et al., 2022; Glasgow et al., 1999, 2019; Proctor et al., 2011).
Quality Improvement
Quality improvement (QI), like HF, takes a pragmatic approach to problem-solving; starting by identifying local issues and then focusing on problem-solving (Batalden & Davidoff, 2007; Sollecito & Johnson, 2013). Classic QI approaches are often organized into toolkits like the “7 new management and planning tools” (Mizuno, 1988), or the “7 quality control tools” (Ishikawa, 1984). The approaches in these toolkits can be used together to form an improvement process (Anjard, 1995), but QI also gives us the “Plan-Do-Study/Check-Act” or PDSA process model (Deming, 1986) to guide improvement projects. Apart from specific process improvements, a secondary goal of PDSA projects in healthcare is to facilitate continuous improvement capabilities (Batalden & Stoltz, 1995).
Integrative Model
To facilitate impactful joint solutions to primary care challenges, we propose an integrative model (Figure 1) to highlight interdisciplinary complementarities between approaches from HF, IS, and QI (i.e., frameworks, models, taxonomies, and methods). We organized the complimentary approaches from all three fields based on the stages of the widely used PDSA process model from QI: Plan, Do, Study, Act (Deming, 1986).
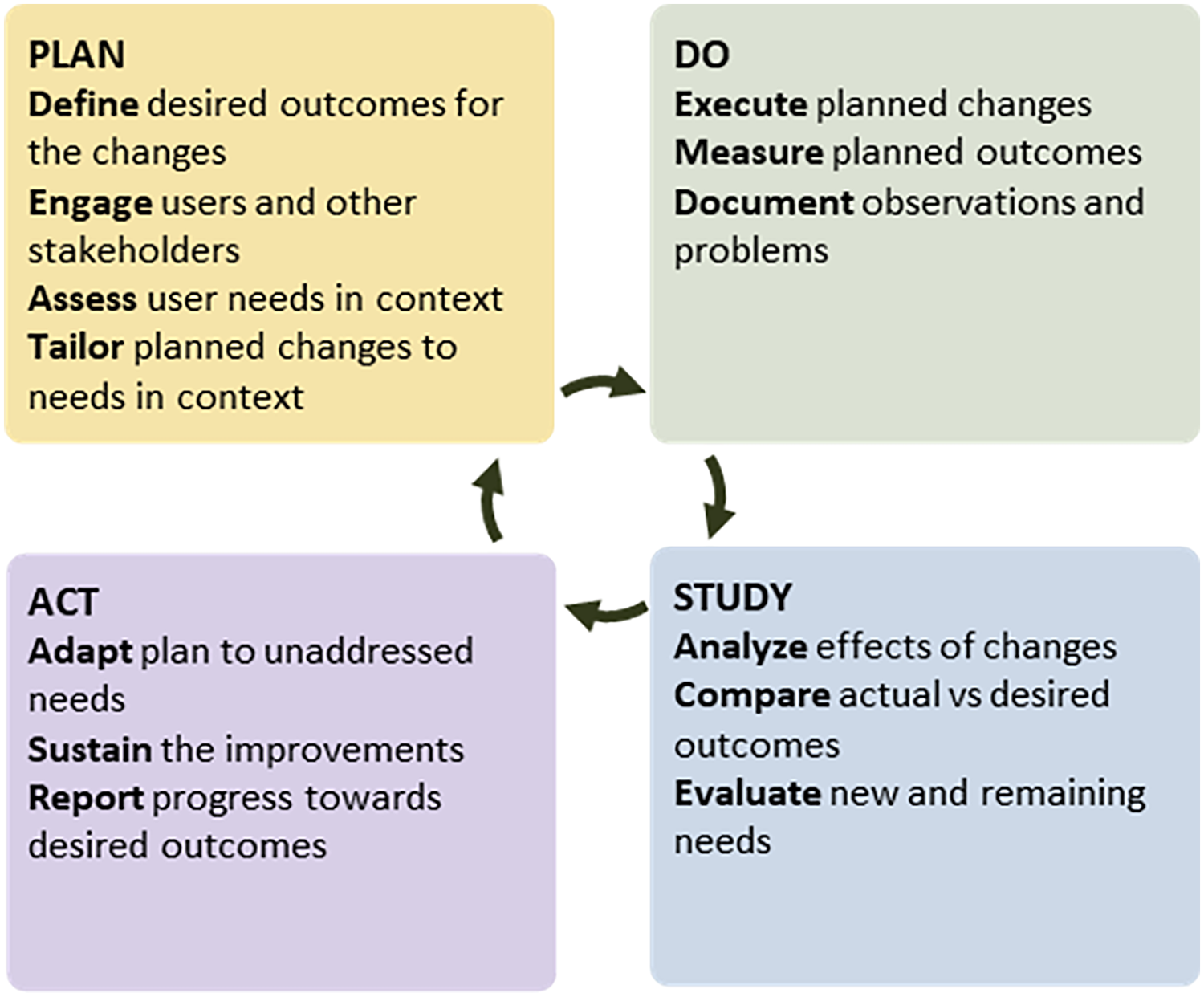
Integrative model for Change in Primary Care, an extension of Plan-Do-Check-Act (Deming, 1986).
PDSA provides an ideal, action-oriented structure for our integrative purposes, for three reasons. First, healthcare organizations and professionals widely use it to guide change efforts. Second, scientists and practitioners across all three fields are familiar with it. Third, this is a simple and intuitive model that promotes rapid cycle iterations, which all three fields recognize as necessary in change efforts.
Plan
Define
Defining the desired outcomes for a change effort can be guided by approaches from HF (Karsh, 2004; Nielsen, 1994), IS (Glasgow et al., 1999, 2019; Proctor et al., 2011), and QI (Kumar & Thomas, 2010; Munro et al., 2015). Improved process efficiency and improved patient care are shared outcomes across all three fields (Berwick et al., 2008; Bodenheimer & Sinsky, 2014). In addition, HF aims to increase use behaviors by attending to usability as an outcome (Nielsen, 1994; Tamilmani et al., 2021; Venkatesh et al., 2012). HF and QI outcomes focus on local needs (e.g., error reduction), in contrast to the externally developed evidence-based practices of IS. A complementary set of outcomes would address local needs while leveraging external solutions.
Engage
Engaging the right people, both end-users and other relevant stakeholders (e.g., patients), is conducted similarly across these fields with approaches like interviews, focus groups, and brainstorming (Loomis & Montague, 2021; Munro et al., 2015; Sanders & Stappers, 2008; Tabak et al., 2017). However, QI affinity diagramming takes a structured and rapid approach to brainstorming, condensing themes from participant ideas for use in other QI tools (e.g., interrelationship digraphs) (Anjard, 1995).
Assess
Each field takes a different approach to assessing user needs and these methods may be useful substitutes pending data or resource limitations. Assessing complex user needs is a particular strength of HF, with approaches like work systems analyses capturing the local system and the interacting barriers and facilitators therein (Carayon et al., 2006; Musuuza et al., 2019). IS offers frameworks to allow for deductive coding of needs, but these are not intended for understanding interactions (Damschroder et al., 2009; Flottorp et al., 2013; Michie et al., 2005). QI takes a more pragmatic approach using the aforementioned affinity diagrams along with tools like fishbone diagrams to assess needs (Anjard, 1995; Mizuno, 1988; Munro et al., 2015).
Tailor
Tailoring is a useful concept most explicitly used in IS that includes many approaches for selecting or designing implementation strategies to address barriers (Lewis et al., 2018; Powell et al., 2017; Waltz et al., 2019; Wensing et al., 2011). However, tailoring is also central to HF approaches like participatory design (Sanders & Stappers, 2008) and QI approaches such as prioritization matrices and PDSA itself (Anjard, 1995; Deming, 1986; Hartkopf et al., 2020). Ideal integrations could balance the evidence-focus of IS approaches that avoid changes to core intervention components (Damschroder et al., 2009; Perez Jolles et al., 2019) with the iterative nature of HF and QI approaches.
Do
Execute
Execution of the planned change can be guided by approaches from HF (Bastien, 2010; Cheng et al., 2020; Harte et al., 2017), IS (Michie et al., 2013; Powell et al., 2015), or QI (Hartkopf et al., 2020; Kumar & Thomas, 2010). While QI and HF approaches focus on iterative local testing and redesign of solutions (Clemensen et al., 2017; Mizuno, 1988; Sanders & Stappers, 2008), IS has an explicit focus on repeatability, using strategy taxonomies to guide execution (Michie et al., 2013; Powell et al., 2015).
Measure
Based on the outcomes targeted in the Plan stage, relevant quantitative and qualitative measures can be captured using the approaches from HF (Robertson et al., 2012; Xie & Carayon, 2015), IS (Fernandez et al., 2018; Glasgow et al., 1999, 2019; Proctor et al., 2011), and QI (Birkmeyer et al., 2004; Munro et al., 2015).
Document
Documenting observations about the change process, problems, and unplanned outcomes is critical to inform future changes. With their shared focus on error prevention, HF and QI offer clear approaches to documentation of unintended consequences (Campbell et al., 2006) and incident reporting (Wiegmann & Shappell, 2017). Conversely, IS approaches focus on the change process, tracking the adaptations and modifications to the planned implementation (Miller et al., 2021; Wiltsey Stirman et al., 2019).
Study
Analyze
Analyses, like measurements, include both quantitative and qualitative approaches. HF gives us retrospective approaches such as the Human Factors Analysis and Classification System (HFACS) (Wiegmann & Shappell, 2017). QI focuses on quality control (Ishikawa, 1984) and, in healthcare, clinical process evaluations (Birkmeyer et al., 2004). IS approaches focus on analysis of specific strategies, outcomes, or interventions (Curran et al., 2012; Smith & Hasan, 2020; Stetler et al., 2006). Mixed-methods analyses may aid integration of methods across these fields to generate clearer pictures of the change efforts (Creswell, 1999, 2021).
Compare
Comparison of actual versus desired, or pre- and post-change effects is a critical component of contextualizing analyses. Though this concept is most clearly present in IS with comparisons in randomized controlled trials (Cykert et al., 2020; Krist et al., 2013), it is also present in QI through iterative workflow modeling (Munro et al., 2015), and in HF with evaluations similar to trials (Katz et al., 2017).
Evaluate
Evaluation of new and remaining needs is a product of analysis and comparison which can be supplemented by additional HF approaches such as cognitive walkthroughs (Polson et al., 1992), ongoing user engagement (Sanders & Stappers, 2008), or usability testing (Bastien, 2010; Cheng et al., 2020). Alternative approaches from IS (Moore et al., 2021; Smith & Hasan, 2020) and QI (Hartkopf et al., 2020) are focused generally on process evaluation and outcomes as described above. There is an opportunity for integration of these IS and QI approaches with direct user feedback per HF.
Act
Adapt
Adapting plans to address unaddressed needs relies on approaches like the intervention adaptation process model from IS (Moore et al., 2021), and prioritization matrices and pareto chats from QI (Hartkopf et al., 2020; Ishikawa, 1984; Mizuno, 1988). These approaches help us update plans based on problems or unintended consequences identified during Do. While several, design methodologies widely used in HF adapt change efforts, IS and QI offer more explicit approaches to this task.
Sustain
Sustainability of changes is a central idea in IS and QI with outcomes focused on maintenance and control of changed practices (Glasgow et al., 1999, 2019; Kumar & Thomas, 2010; Munro et al., 2015; Proctor et al., 2011). This concept was not clearly detailed in HF approaches.
Report
Discussing results internally allows for ongoing stakeholder engagement in design or implementation processes (Sanders & Stappers, 2008) and reporting externally (e.g., publications), allows for synthesis in reviews like this and sharing of approaches.
Discussion
The proposed integrative model for change in primary care demonstrates interdisciplinary complementarities between human factors, implementation science, and quality improvement. This high-level overview of approaches reinforced the gaps, contributions, and potential synergies amongst these three fields (Hignett et al., 2015; Leeman et al., 2021) and their approaches to primary care change. Future work will include systematic reviews of approaches used in primary care change efforts and how they relate to outcomes.
Conclusion
Human factors, implementation science, and quality improvement have developed approaches to identify and address barriers to change in primary care. Though these fields do not routinely interact, the various approaches they have created serve unique, yet synergistic purposes in primary care change efforts. This review and conceptual model offer an initial look at the approaches to primary care change across these fields. Future work will expand and evaluate combinations of approaches from these and other fields. This study offers a roadmap for interdisciplinary integrations across these fields in pursuit of better primary care for all.
Application
This work may be applied in the exploration, preparation, execution, and sustainment of primary care change efforts and capacity building among primary care practitioners and researchers. Teams can use our integrative model to appraise and select approaches that best suit their available expertise and resources. Practitioners and researchers may also find this model useful to guide their education in methods outside of their primary area of study.
Footnotes
Acknowledgements
Dr. Ramly’s effort was partially supported by the Agency for Healthcare Research and Quality grant 1K01HS028926.