
Abstract
Traditional medical surgery has evolved in the past decade with advances toward robot assisted surgeries (RAS) taking over the healthcare industry. Regular hospital formalities experienced by surgeons and team members such as communication methods are now challenged to progress alongside RAS. Emerging trends such as diminishing hospital staffing and greater procedural outputs have required new demands. Current literature insufficiently addresses how team workload is distributed and communicated between a surgeon performing the surgical task with robotic aid while delegating work tasks to the assisting surgical team. This paper investigates how robotically assisted surgical team’s perception of workload is moderated by using more concise verbal and nonverbal communication methods employed by the operating surgeon and operating room team. As the development of robotic surgical systems become more widespread, it is essential to consider the interdependencies between human to robot to human medical interaction, verbal and nonverbal communication, and perceived workload.
Keywords
Introduction
Robots have been employed in the healthcare realm for a variety of services, such as disease detection, therapy, rehabilitation, disability care, and elderly care (Krebs et al., 2003; Leite et al., 2013; Thevenot et al., 2017). With the adoption of robotic technology, robots are increasingly becoming integrated into medical specialties like surgery. Robotic-assisted surgery (RAS) enables surgeons to utilize computer software technology to control and manipulate robotic surgical instruments to make incisions directly into a patient’s body (Center for Devices and Radiological Health, 2022). Surgeons using RAS may be observed to be seated on a separate console away from the patient and operational team while controlling a robot equipped with multiple arms of technical tools such as miniaturized incision instruments and high-definition three-dimensional cameras (Wilson et al., 2015). An example configuration of the console, instrument, and operational team in a robotic-assisted cardiac surgery is shown in Figure 1. These robot-controlled tools have emerged in medical technology providing several advantageous outcomes for both patients and operating room (OR) team members.
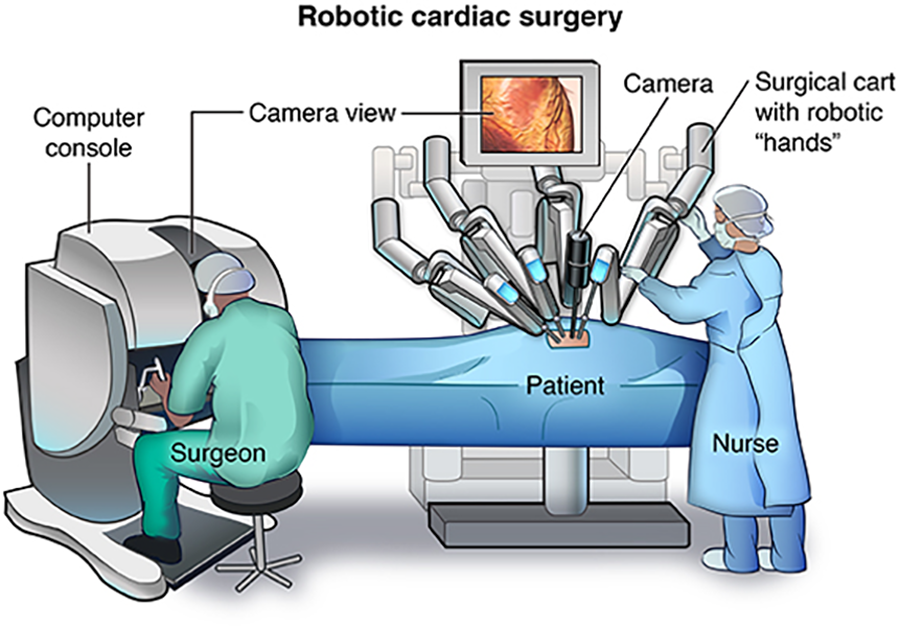
Example image of robotic surgery.
The implementation of RAS alongside trained OR team members familiar with RAS allows for a greater chance of a minimally invasive operation, a reduction of inpatient stay, and mitigation of pain post-surgery (Gerhardus, 2003; Palep, 2009). However, there has been apprehension surrounding the implementation of these technologies. Some researchers denote that there may be adverse effects to robotic surgeries such as an unease in acceptance of these technologies due to increased longer surgical procedures and increased patient mortality due to lack of non-technical skills training required within RAS (Nagyné & Haidegger, 2021). These challenges may be observed in OR teams who are unfamiliar with communicating their routine procedures while using RAS or in hospital settings that have a preferential bias to open surgery rather than RAS methods (Nagyné & Haidegger, 2021).
However, there is still a gap in research to fully capture how team members may benefit from RAS. Much of the cited literature focuses on how RAS may benefit the surgeon specifically such as improving posture, stance, and an overall physical burden rather than the entire surgical team (Randell et al. 2016). The purpose of this paper is to contribute to the knowledge gap in robotic surgery research and to propose a method for exploring team-perceived workload while also considering verbal and nonverbal communication. In the first section, we will explore the literature of robotic surgery. Next, we will define and explore the perceived workload regarding robotic surgery. We will then give an examination of the different forms of verbal and nonverbal communication. In the closing section, we propose an experimental study and discuss the relevance of conducting this research.
Background
Challenges with RAS
The introduction of RAS has frequently been met with fast-growing approval among successful surgeons and OR teams, however, growing challenges with RAS are also portrayed. As concerns adopting new RAS methods, Mehaffey et al., (2017) observed a decline in laparoscopic surgeries and an overall decline in residential participation due to increased operative time and substantial hospital costs. Other forms of opposing challenges with RAS include residential gaps in non-technical skills during RAS contributing to errors, patient morbidity, and mortality (Alken et al., 2018). These non-technical requirements during RAS include situational awareness, decision-making, stress resilience, communication, and leadership which largely influence overall teamwork and the clinical outcome of the surgery (Nagyné & Haideggar, 2021). Furthermore, the role of non-technical skills among the surgeon and OR teamwork highlights the importance of how interpersonal, cognitive, and personal resourcing skills are imperative to successful procedural outcomes.
Workload
Perceived workload, also referred to as mental workload, is an “operator’s subjective experience of the demands of a task” (Hart & Staveland, 1988). Robotic surgery accelerates traditional surgical procedures by providing minimally invasive operations and reducing potential stress, demonstrated in the usage of smaller surgical incisions. For example, traditional laparoscopy, an abdominal surgical operation, presents surgeons and OR team members with difficulties including limited dexterity, 2-D resolution of view, and high mental and physical demands (Moore et al., 2015). These mental demands negatively impact the surgeon and the OR team's ability to focus and produce stress. When an operator experiences a high mentally demanding task, they can often become stressed, increasing chances of communication breakdown. Poor communication may be observed by requiring the surgeon to clarify specific tasks to the OR team increasing chances for mistakes, prolonging the length of the operation, and increasing the chances of patient mortality. Gradually introducing more RAS procedures in hospitals may provide a reduction in team perceived workload including decreased workflow disruptions, better team coordination among OR staff, and a reduction in overall surgeon fatigue (Rogers, 2020). With the implementation of RAS, surgeons can spend less time during the procedure allowing the OR team to perceive less stress and overall workload. However, more research is needed with further consideration of the moderating role of improved non-technical skills in teamwork communication. Future research on robotic surgeries may provide an understanding of workload effects.
Non-verbal and verbal communication
Miscommunication among OR surgical teams has often been cited to be one of the major causes of non-technical surgical error (Ahmad, 2016). Human to human to robot (H-H-R) medical interaction within RAS is characterized by the surgeon operator utilizing the robotic device to communicate procedural information to the operating team. Tiferes et al. (2016) describes utilizing a combination of verbal and nonverbal gestures as an optimal method of improving team communication. In addition to verbally directed surgical queues, Tiferes et al. (2016) examined nonverbal forms of communication such as visual gaze in direction, body positions and movements, facial expression, or tool manipulations. Specifically during RAS, the surgeon was observed to ask the bedside assistant to hold retracted tissue while targeting remotely with robotic arms. The bedside assistant would then exchange nonverbal affirmation by holding the requested retracted tissue with the surgeon confirming the action request with a “yes.” The findings highlight that 67% of the interaction events between the surgeon at the console and the right bedside assistant were nonverbal (Tiferes et al., 2016). The combination of verbal and nonverbal gestures is promising because it allows the surgeon to provide concise verbal instruction accompanied with nonverbal gestures through the robotic devices to minimize unnecessary movement and reduce team perceived workload (Catchpole et al. 2019, Tiferes. J., Hussein, et al., 2016).
Overall Objectives
By analyzing more contextual methods of communication within OR settings, we believe a reduction of team-perceived workload may occur within robotic surgeries. To theoretically examine this reduction, an observational approach with video and audio recordings of robotic surgeries will allow appropriate measurement of these outcomes. With this knowledge, medical technology manufacturers, researchers, and hospital surgical teams, could be better informed about the non-verbal and verbal communication and perceived workload of robotic surgeries. Therefore, the objective of this proposed study intends to reveal differences in perceived workload under the moderation of nonverbal versus verbal communication of surgical OR team members. We propose the following hypotheses:
H1: H-R team perception of workload will be reduced with robotic surgery
H2: Robotic surgery and H-R team perception of workload are moderated by non-verbal vs. verbal communication
Method
Procedure
For the proposed study, data will be collected from observed robotic surgeries, followed by the SURG-TLX and semi-structured interviews. All surgeries will be recorded for video analysis and audio transcription. Interviews will be recorded and transcribed for analysis.
Participants
The study sample will consist of surgical team members from at least 20 robotic surgery operations. Depending on the team, eligible team members could include surgeons, residents, OR nurses, OR practitioners, anesthesiologists, surgeon trainees, and any other OR personnel. All participants will be over the age of 18.
Measures
Workload will be measured using SURG-TLX (Wilson et al., 2011) which is a multi-dimensional surgery-specific workload measure that determines the utility of providing diagnostic information about the impact of various sources of stresses on trained surgical operators. The six dimensions of stress include mental demands, physical demands, temporal demands, task complexity, situational stress, and distractions. These multidimensional measures were selected to provide a quantifiable measure of workload and stress during RAS.
Analysis
Based on the data obtained, a simple two-tailed independent t-test for two samples will be conducted to determine the mean difference between verbal and nonverbal behaviors between the surgeon using the RAS versus the OR team supporting the overall procedure.
For the observed live robotic surgeries, video and audio will be recorded to analyze verbal and nonverbal communication methods. Out loud communication between OR team members will be coded under verbal and movement of the body, hand, or head will be coded for nonverbal or gestural communication. Verbal communication will be coded based on call-outs, acknowledgments, read-backs, and clarification. Non-verbal communication will be coded based on gestural movements in combination with verbal directions including pointing directionally to targeted areas, gesturing to continue or stop, visual gauges, and facial expressions. Specific procedures involving communication between the surgeon and the physician assistant and the general OR team will be coded as suctioning, washing, holding, clipping, catheter insertion and removal, and stitching/needling. The semi-structured interviews will focus on team communication, performance, and human-robot interactions. Interviewees will be asked to think about their experience working with robotic surgeries and complete a survey measuring their stressors using the SURG-TLX. Audio of interviews will be recorded and transcribed for qualitative analysis. Data from interviews will be analyzed and mapped into a matrix to compare responses between surgical team members.
Discussion
As future approaches revolutionize technology, bridging the gap between how perceived teamwork is moderated by verbal and nonverbal communication within RAS is unclear. Our project serves to advance the field of knowledge by exploring the underlying effects robotic aids have on perceived workload in human-to-robot interactions. By coding and examining different types of verbal and nonverbal exchanges during specific RAS procedures, we will have a greater understanding of how communication effects the overall perception of workload. A mix of both verbal and nonverbal communication may also exist and demonstrate a more smoothly run operation and potentially reduce perceived workload.
By perceiving less work during RAS, current challenges that RAS face such as greater learning curves involving non-technical communication skills and technical gaps in using newer and finer-tuned robotic features may be mitigated by closely identifying and quantifying how communication is being moderated. By quantifying how information is exchanged verbally and nonverbally, future research may be able to comprehend the limitations of robotic surgery more accurately. By unpacking current challenges within RAS, we hope to observe an increasing acceptance in robotic technology of practicing physicians and patients as these technologies continue to strengthen.
Future studies should implement greater emphasis on non-technical communication skills due to the strict nature of procedural operations within RAS. Non-technical skills such as leadership, situational awareness, and decision-making may be of interest to investigate further in the OR team setting. Although it is a prerequisite to overcome initial learning curves regarding newer technological challenges such as finer-tuned RAS mechanics, valuing non-technical skills are crucial to a successful operation and may prove to be equally as important in the perception of surgical team workload.