
Abstract
Trombonists, like other musicians, are at risk for developing use-related musculoskeletal symptoms. This study investigated an ergonomic aid for playing the trombone, the Neotech Trombone GripTM, which assists a trombonist’s left hand in supporting the instrument. The objective of the study was to investigate effects of this device on the left upper extremity while playing the trombone in comparison to the standard, unaided method of grasping it. Seven trombone players used the grip for two weeks prior to providing objective and subjective data in a laboratory environment. They played a scale and a piece of their choice under four conditions: sitting or standing with or without the device on their trombone. While playing, muscle activity in the trapezius, anterior deltoid, middle deltoid, extrinsic finger flexor, and extrinsic finger extensor muscle groups on the left side of the body were collected. Perceptions on the device using a survey were also assessed. Results indicated a consistent decrease in muscle activity in the finger flexor group when using the device. Smaller, less consistent effects were seen in activity in the trapezius (decrease), finger extensor group (increase), and anterior deltoid (increase) muscles, while using the device. Effects were more pronounced in players with smaller hands (among the group of participants). Most players subjectively found the device beneficial and all would recommend it to other players.
Introduction
Interacting with musical instruments can cause musculoskeletal (MSK) problems for many players due to the instrument’s weight, postures required for playing, and duration of playing (K. Chesky et al., 2002; Cruder et al., 2021; Paarup et al., 2011). Previous studies have observed full orchestras and groups of instruments, but there have been few that have looked specifically at the trombone. In studies that have looked at results by individual instruments, trombonists showed problems in the left shoulder and left hand, more than players of other instruments (Ackermann et al., 2014; K. Chesky et al., 2002; Cruder et al., 2021). This is likely due to the majority of the instrument’s weight being supported by the left upper extremity. From this previous research, one can see that playing an instrument can be a detriment to one’s MSK health, and musicians should take precautions to reduce the chance of developing these problems.
One way to reduce the risk of injury is through use of ergonomic aids for instruments, which exist for a variety of instruments to alleviate some of the problems that musicians face that arise from the need to continuously support the weight and position of the instrument. The support provided from a player comes from continuous recruitment of muscles in the upper extremity and/or shoulder, and this continuous recruitment can result in fatigue in the short term and actual damage to muscle fibers in the long term (Thorn et al., 2002; Visser & Van Dieën, 2006). Previous studies have investigated the effectiveness of violin chin rests and clarinet neck straps (K. S. Chesky et al., 2000; Okner & Kernozek, 1997; Steinmetz et al., 2006), with these studies suggesting that the supports can help alleviate the players’ problems.
When it comes to trombones, there has been little research into the supports specific to it. One study on trombone aids found that adding splints for the left hand was more comfortable and helped reduce pain for two female players (Quarrier & Norris, 2001). Another study investigated the ERGObrass® support for the trumpet, French horn, and trombone (Price & Watson, 2018), and found that, in general, musicians displayed less muscle activity when playing using the device. This finding was greatest for trombone players, who no longer needed to support the full weight of the instrument (~1.4-3.1 kg) on the left side of the body. These studies highlight how certain specific interventions can help and what help they provide; however, untested ergonomic aids exist that can be investigated in a similar manner.
One such aid is the Neotech Trombone GripTM (Figure 1). This aid exists specifically for the trombone with the intent of reducing the grip force produced by the left hand that is needed to grasp the instrument. The Neotech grip has anecdotal support from players claiming that the intervention helps alleviate problems in the left hand while playing; however, these claims have not been objectively tested. Because left hand discomfort has been documented in trombonists, knowledge about the effectiveness of this device may be of use to trombonists who experience MSK symptoms and would like to continue playing. This knowledge may also benefit those who want to take a proactive measure against symptoms. It was expected that the study could inform players about effects they could reasonably expect.

Neotech Trombone GripTM.
The objective of this study was to investigate effects of the Neotech Trombone GripTM on the left upper extremity while playing the trombone in comparison to the standard, unaided method of grasping a trombone. Understanding players’ perceptions and opinions of the device was another objective. To achieve these objectives, a laboratory experiment followed by a questionnaire were completed by trombonists. The study was approved by the Institutional Review Board of the university.
Methods
Participants
Participants were eligible if they were between 18 and 70 years old, knew how to play the trombone, were willing to play with the new grip device, and were willing to participate in two research sessions (1-grip introduction, 2-grip/no grip comparison). They were excluded if they would be unable to physically play the instrument for more than 30 minutes or had a current injury that markedly affected how they played the instrument. There was no criterion for years of playing experience.
Instrument
Participants completed a set of questionnaires based on the Nordic Questionnaire about musculoskeletal symptoms (Kuorinka et al., 1987). The questionnaires asked about troubles in the neck, shoulders, elbow/forearm, hand/wrist, upper back, and lower back along with specific questions about the left and right hands. The questionnaire covered the past 12 months and past 7 days before the first (of two) sessions. Another questionnaire covering the past 7 days before the second session was also completed.
Participants also completed a questionnaire about their perceptions of the device. This questionnaire asked about usability (e.g., how easy was it to use, how quickly did you get used to the device), usefulness (e.g., how useful was the device, what impact did using this device have on your performance), desirability (e.g., would you use this device, what setting would you use this in), and barriers to adoption.
Surface electromyography (EMG) data were collected using five wireless electrodes (legacy Delsys Trigno Wireless EMG System, Natick MA) to collect muscle activity from the trapezius, anterior deltoid, middle deltoid, extrinsic finger flexor group, and extrinsic finger extensor group. EMG data were sampled at 2000 Hz in The Motion Monitor data collection software (Innovative Sports Training, Inc, Chicago).
Procedures
Each participant participated in two sessions. In the first session, the participant was introduced to the study, completed the first set of musculoskeletal health questions, and was given the device along with guidance on how to use and adjust it. They were instructed to practice with the device at least every other day for two weeks (due to scheduling conflicts, 3 subjects had more than 14 days between sessions).
In the second session, the participant completed the second questionnaire about musculoskeletal health. The subject’s hand dimensions were then measured. These measurements included hand length (from the distal crease of the wrist to the tip of the middle finger), hand breadth (the widest points across the base of the fingers), and thumb length (from the base of the thumb to the tip of the thumb).
The subject’s skin was shaved and cleaned with alcohol, then the surface electrodes were placed on the left side of the body over the trapezius, anterior deltoid, middle deltoid, extrinsic finger flexor, and extrinsic finger extensor muscle groups. Along with resting data, the subject performed two repetitions of five maximum voluntary contraction (MVC) isometric exercises targeting each muscle group for purposes of data normalization.
The subject then completed two playing activities, repeated 3 times, in each condition (sitting and standing, with and without the device on the trombone). The condition order was randomized for each subject. The first activity was a B-flat scale set to 60 beats per minute. During this activity a researcher would give cues to move between different playing phases (resting, lifting, playing the scale, holding, and lowering) while marking these phases with a marker electrode. The second activity was playing the same 20 second passage of a piece of the subject’s choosing, to provide a more realistic, free style of playing.
Data processing and analysis
The EMG data were processed in MATLAB (version R2021b) with functions from the Statistics and Machine Learning Toolbox. EMG data were normalized using resting and MVC values. The scale playing was sectioned into the 5 different phases, and 10th, 50th, and 90th percentile values in these phases (along with the free choice playing) were found. These statistics were averaged across the three repetitions.
Due to a small sample and variety of responses between the participants, inferential statistical analysis was not deemed appropriate for this study. Instead, descriptive analysis was performed by discovering trends in the mean values of each condition and comparing differences between conditions on an individual basis.
Results
Participants
Recruitment efforts yielded seven participants (6 male, 1 female) in the allotted time frame. Table 1 shows the subject anthropometry values for the hand, along with trombone playing measures, for each individual. In the 2 weeks, players practiced between 155 and 2040 min., with the grip device being used between 15.7% and 100% of the time.
Subject anthropometry and trombone playing measures.
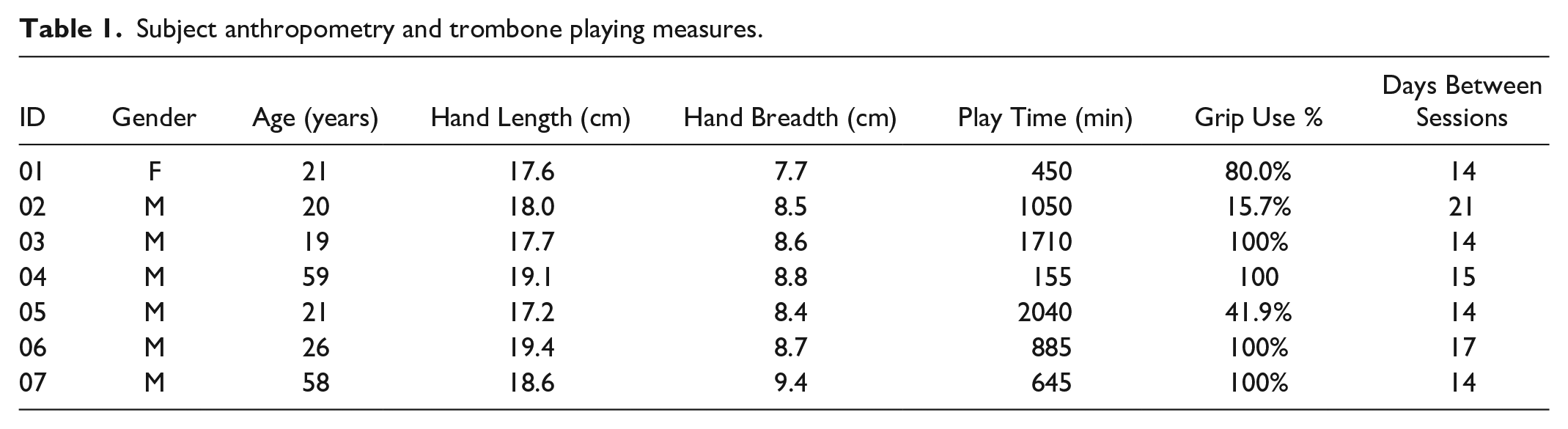
Table 2 shows results from the MSK health surveys for the most relevant regions. The areas with the highest prevalence in the 12 months before the first session were the left/both hand/wrist (n=6) and the left thenar eminence (n=4). Prevalence remained constant or decreased within the 7 days prior to the second session.
Musculoskeletal health questionnaire responses.
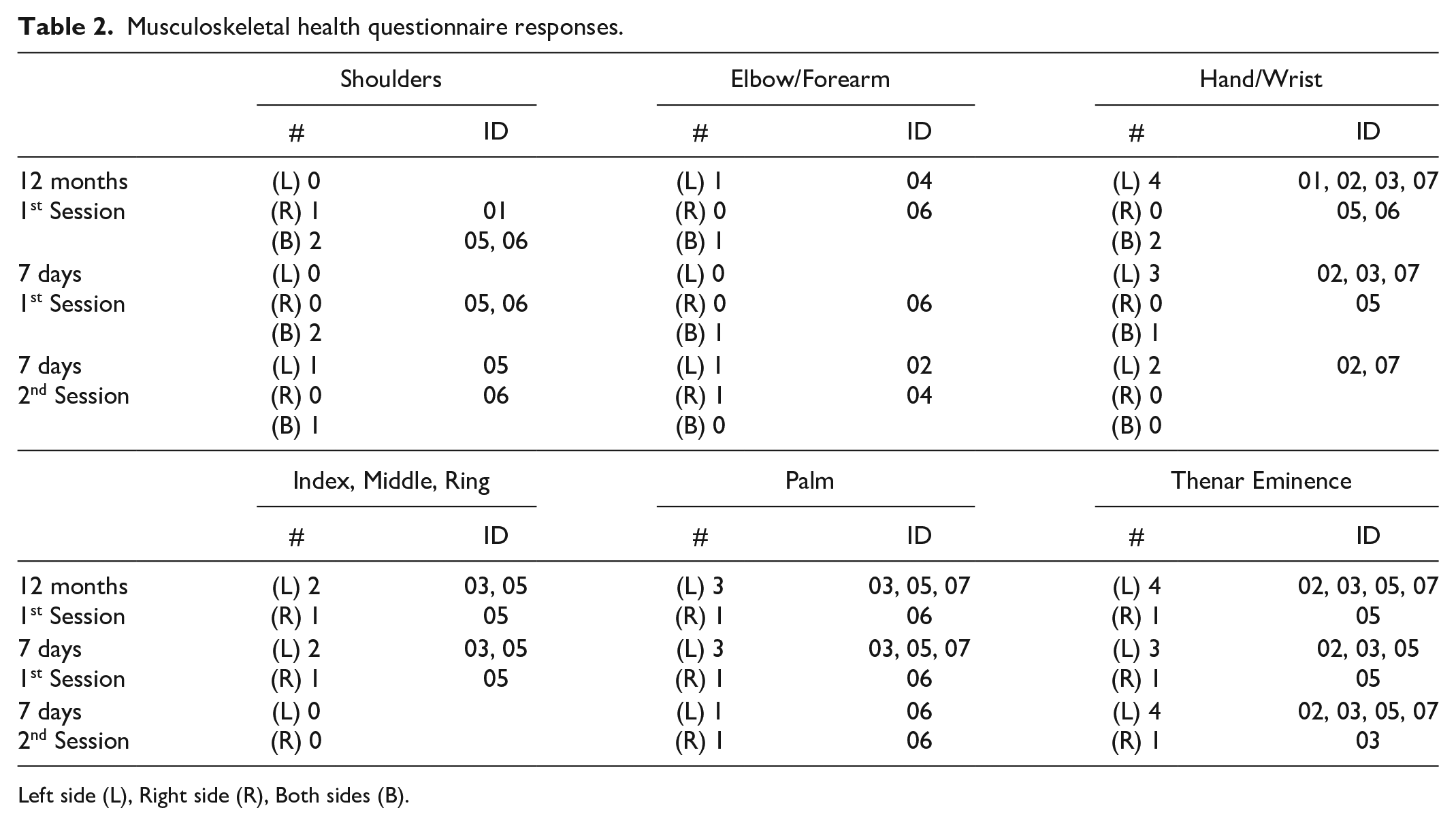
Left side (L), Right side (R), Both sides (B)
Muscle Activity
Figure 2 shows the mean 50th percentile muscle activity values from all participants. Across the sit and stand conditions, the trapezius had the highest activity, with median values averaging 22.4% and 20.5% MVC while free playing, without and with the device, respectively. The middle deltoid had very low activity relative to the other muscles. Across the sit and stand conditions, the median extrinsic flexor activities were 11.5% and 7.7% MVC during the free playing, without and with the device, respectively, and the median extrinsic extensor activity values were 9.3% and 10.9% MVC for the free playing, without and with the device, respectively.
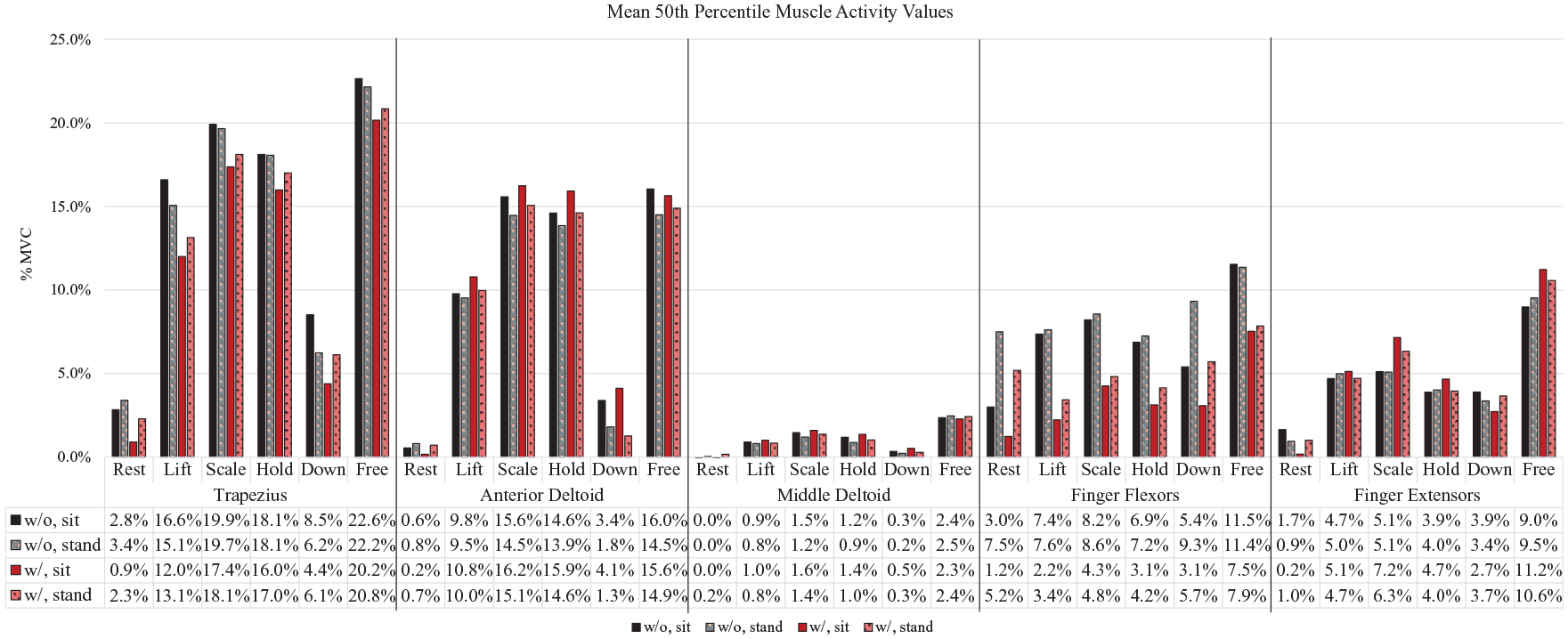
Mean 50th percentile muscle activity values.
Table 3 shows the difference between the “with grip” and “no grip” conditions in absolute values of percentage of MVC value for each muscle. A negative value indicates that activity was lower while using the grip device, and a positive value indicates that activity was higher. A larger portion of the cell is shaded green to indicate larger reductions in muscle activity; a larger portion of the cell is yellow to indicate larger increases.
50th percentile muscle activity difference between grip conditions.
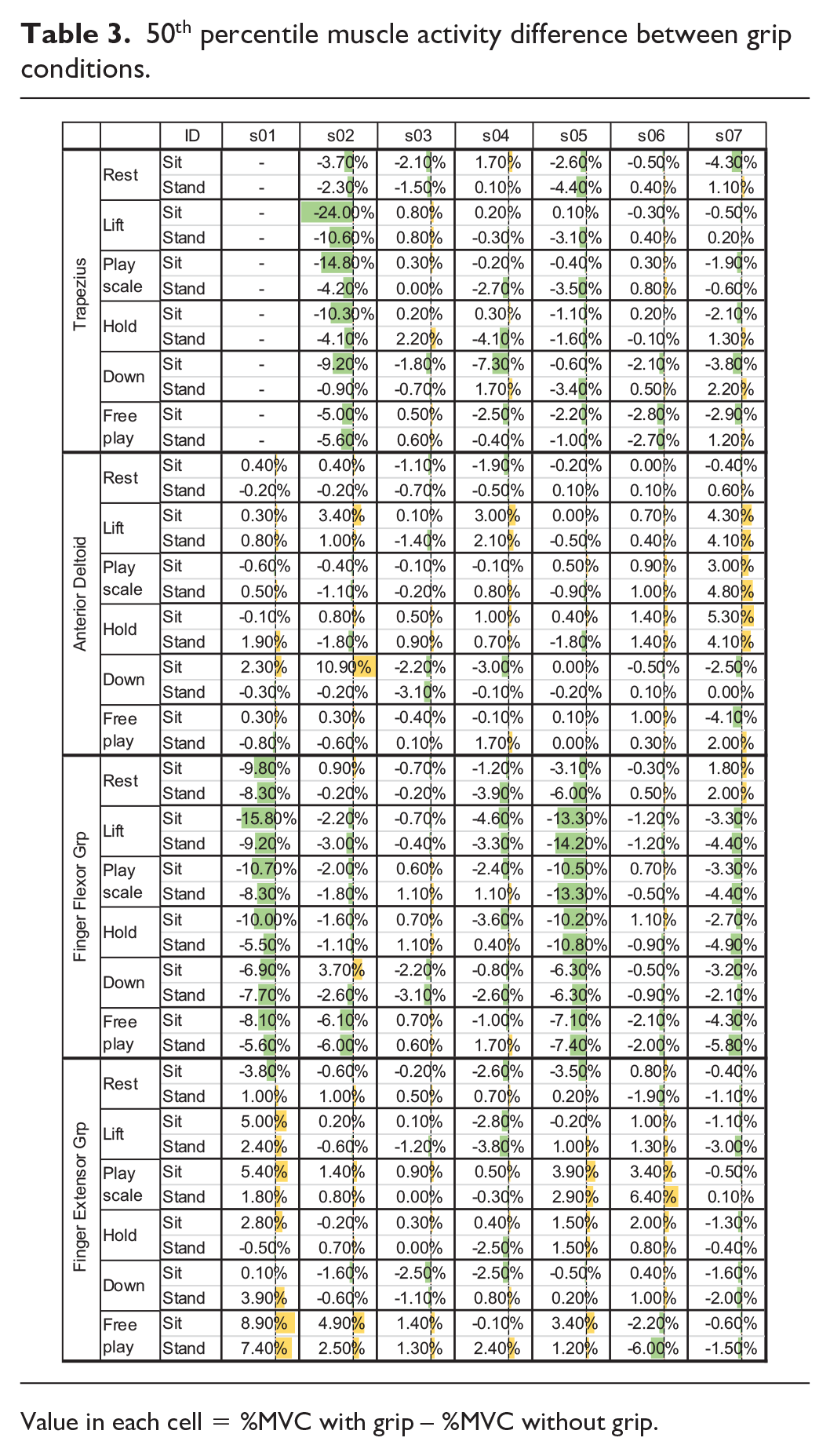
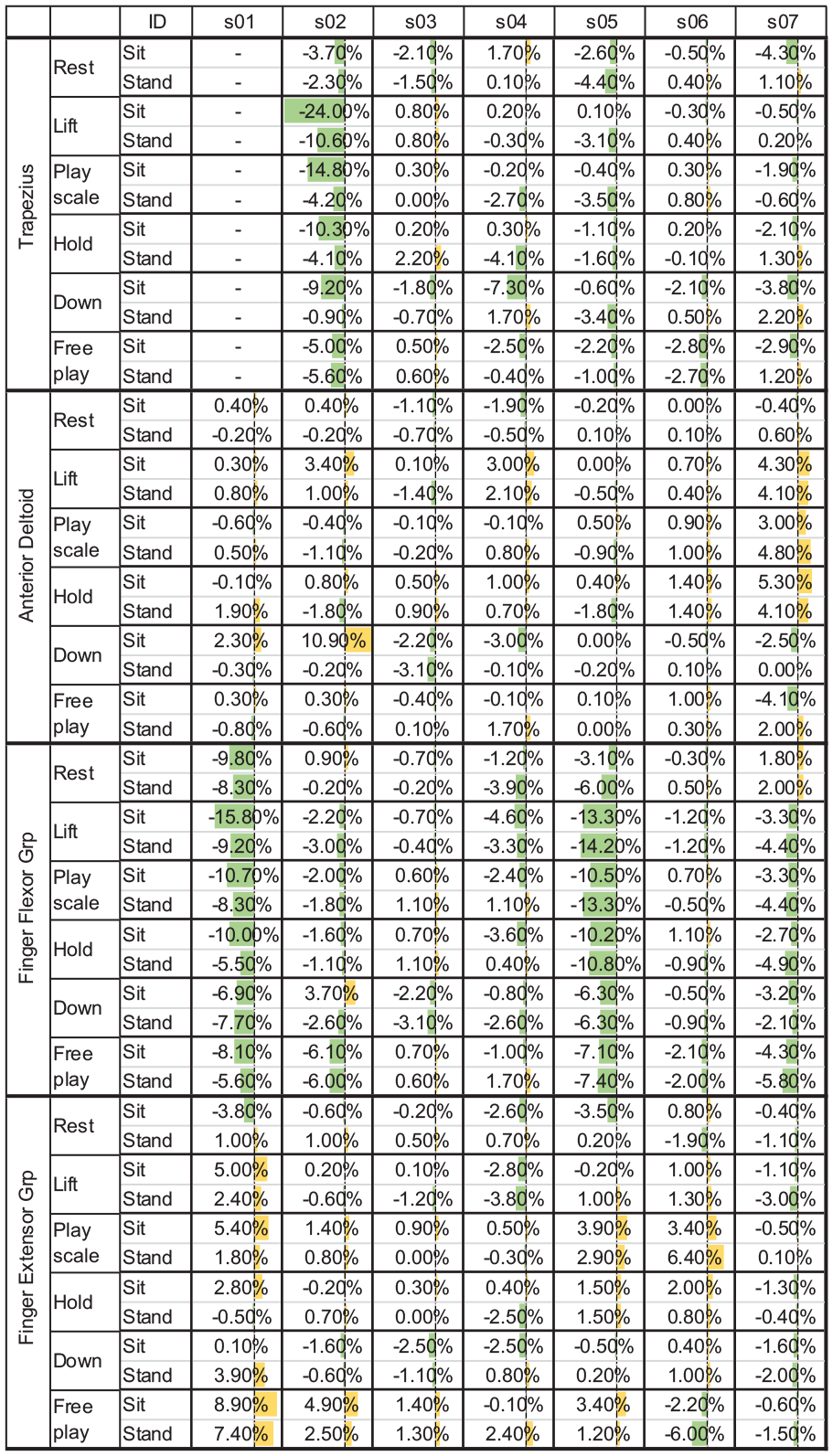
Value in each cell = %MVC with grip – %MVC without grip.
For the trapezius, differences between the median muscle activity were between -24% and +2% MVC, with subject 02 having markedly larger reduction in trapezius activity than other participants. For S02 and S05, across all phases, there was either no difference or a negative difference in the trapezius, with resting and scale playing have more negative differences. Small decreases during playing (play &/or free) were seen for three others. For the anterior deltoid, differences in median muscle activity were -4% to +11% MVC. Across all phases, most differences were between +/- 2% MVC, with S07 displaying somewhat more positive differences. For the middle deltoid (not shown in Table 3), the differences were between -1% to +1% MVC, with all subjects having essentially no difference in activity across all phases. For the extrinsic finger flexor group, the differences were between -16% to +4% MVC across all phases and participants, and -13% to +2% MVC while playing (play &/or free). All subjects had virtually no difference or a negative difference, with a majority having a negative difference, in the lifting, scale playing, holding, and free playing phases. For the extrinsic finger extensor group, across all participants and phases differences were between -6% to +9% MVC, with larger positive differences observed most often in the scale (4 participants) and free playing phases (5 participants).
Perceptions
Participants’ overall opinions of the device were positive (n=5), neutral (n=1), or negative (n=1). In general, participants perceived that the device was easy to use but may take some players more time or assistance to use well. They indicated that the device was comfortable and helped players hold the trombone without negatively impacting playing quality. Five players indicated that they would use the device in the future, and all said that they know others who would want to use it. The two non-positive participants did not think they needed the device.
Discussion
Participants
All but subject 04 reported a history of wrist/hand pain on the left side. This subject was recruited by word-of-mouth, while the others were recruited via a flyer, indicating some potential bias in who participated. Future studies should consider additional methods of recruitment to increase the sample size, which was a limitation in the current study.
The number of participants reporting symptoms in the left hand/arm/shoulder was consistent or decreased after the grip device was introduced to players during Session 1. There may be some symptom relief when using the device; further investigation of this trend, over a longer period of time, is warranted.
Muscle Activity
The extrinsic finger flexor muscle group appeared to benefit the most when using the device, especially in subjects 01 and 05. These two players also had the highest finger flexor muscle activity of the group. Three other subjects also seemed to have lowered flexor muscle activity while using the device, while the remaining two showed little difference between grip conditions. The extrinsic finger extensor group appeared to have a consistent increase in muscle activity, especially in the scale and free playing phases. The subjects that had the larger increases in extensor activity also had larger decreases in finger flexor activity, indicating some tradeoff between these groups while playing with the grip device. S05 and S07 displayed net benefit (flexor decrease > extensor increase) during scale and free playing; S01 displayed net benefit in scale playing and net decrement during free play; S02 net benefit during free play; S06 net decrement during scale and free (more so when standing).
The trapezius seemed to have an unexpected benefit when using the device, particularly in S02, who also had the highest trapezius muscle activity. The trapezius muscle displayed the highest activity overall, so any device or playing method that could reduce muscle activity could be beneficial, provided it did not lead to increases in other muscles. The anterior and middle deltoid appeared to be mostly unaffected by using the grip device, with one player experiencing an increase in anterior deltoid activity while using it.
The grip device seemed to have the largest impact on subjects 01, 05, and 02. This group had the smallest hands when compared to the others, signaling some potential interaction with hand size. This is consistent with Quarrier & Norris (2001), where female players who had small hands benefited from using splints on their trombones.
Overall, activity in the extrinsic finger flexors and the trapezius tended to decrease while using the grip, while the extrinsic extensor activity tended to increase. These trends were apparent during playing (scale or free play). Net benefits differed between participants. Previous studies have also found that ergonomic aids can have an objective benefit by reducing muscle activity in players (Price & Watson, 2018; Steinmetz et al., 2006) and a subjective benefit by increasing comfort while playing (Quarrier & Norris, 2001).
Perceptions
Subject 05 had a neutral opinion, subject 02 had a negative opinion, and the rest had positive opinions. Non-positive opinions were related to not finding adjustments that made playing comfortable (subject 02) and not finding any need for the device (subject 05). All subjects would recommend the device to other players.
Almost all subjects mentioned they experienced a better weight distribution while using the device. They no longer needed to tightly grip the trombone and could instead use their larger arm muscles to support the weight, rather than relying on their hand muscles. This relates to the flexor/ extensor tradeoff, along with other, unmeasured muscles, such as the biceps and intrinsic finger muscle groups. Future work should investigate additional muscles for trends.
Conclusion
The results indicated that extrinsic finger flexor group muscle activity, and trapezius muscle activity to a lesser extent, was consistently decreased, while extrinsic finger extensor group muscle activity, and anterior deltoid muscle activity to a lesser extent, was increased when using the device compared to a traditional grasping method. These increases and decreases were most pronounced in players with relatively smaller hands (among the group of participants). These decreases paired with increases, specifically in the extrinsic finger flexor and extensor groups, respectively, indicate some tradeoff between muscle groups, although this tradeoff produced net benefits (flexor decrease > extensor increase) for 4 of 7 participants during playing. Through exploring the players’ opinions, most found the device beneficial, and all would recommend it to others, even those with negative or neutral opinions. Players that did not subjectively find the device beneficial did, nonetheless, showed objective evidence of reductions in muscle activity.