
Abstract
Transferring a patient from a bed to a wheelchair is important for patient well-being. Research has shown that manually performing this task exposes healthcare workers (HCWs) to lower back kinetic demands that can exceed safety standards, necessitating the use of mechanical lift equipment. However, HCWs still commonly perform this task manually, especially for lighter patients who are capable of assisting. Although lower back kinetic demands are presumably dependent upon the patients (in)ability to assist during the transfer, this has not been systematically tested. Therefore, the primary aim of this research was to compare the peak L5/S1 intervertebral joint (IVJ) compressive force demands during a bed-to-wheelchair manual transfer across different levels of simulated patient assist (0%, 18%, and 36% of patient bodyweight). We also compared peak IVJ compressive forces from an approach using external forces directly measured at the hands of the HCW, with an alternative traditional approach that assumed the patient’s mass was fully lifted by the HCW throughout the transfer. Peak L5/S1 IVJ compressive forces were lower (p < .001) during the 36% than the 0% and 18% bodyweight patient assist conditions when applying the measured forces at the hand. Overall, peak compressive forces were lower (p < .001) and tended to occur at different phases of the transfer when applying the measured forces at the hand versus assuming all the patient’s mass was being lifted. Our results emphasize the importance of accurately modeling the forces at the hands when estimating in vivo demands. Further, these findings suggest that encouraging the patient to assist during transfers may reduce IVJ forces on HCWs, but for heavier patients even a modest degree of patient assistance is not likely to protect the HCW from elevated spine loads. In most circumstances, lift equipment is warranted.
Introduction
Transferring a patient out of bed is a standard and important daily task for healthcare workers (HCWs; Anderson et al., 2014). Patient transfers support proper hygiene and patient well-being. A common transfer is relocating a patient from bed to a chair or wheelchair located nearby (Garg et al., 1992). The task is often performed on patients that are largely dependent, but some patients can assist the HCWs during the transfer. It is recommended that transfers occur with the support of lift devices (American Nurse Association, 2015) but they are often performed manually with either one or two HCWs. In environments where resources are limited, manual transfers by a single HCW are common (Anderson et al., 2014; Yassi et al., 2001). Manual patient transfers are associated with high lower back kinetic demands and injury to HCWs (Engkvist et al, 2000).
The peak lower back kinetic demands on the HCW(s) during bed-to-chair or bed-to-wheelchair transfers have previously been estimated to range from 1,881 – 6,420 N of compressive force in the lumbar intervertebral joints (IVJ; Garg et al., 1991; Marras et al., 1999). These estimates, which are based on mathematical models, generally exceed established ergonomic thresholds (Waters et al., 1993). Estimations based on mathematical models are necessary because directly recording in vivo forces is infeasible (Dreischarf et al., 2016). Therefore, having accurate biomechanical measures and realistic modeling assumptions are imperative. Measuring ground reaction forces can be erroneous if the HCW’s lower limbs come in contact with other objects or the patient touches the force plate (Skotte, 2000). An alternative to solving the lower back kinetics from the bottom-up with the measured ground reaction forces is a top-down modeling method using either measured forces at the hands or assumptions about the mass being lifted (de Looze et al., 1992). The latter approach has been applied in several studies (e.g., Tang et al., 2018; Ulin et al., 1997) but can adversely influence the estimated demands in situations where the patient is not fully lifted, the burden is not evenly distributed between the limbs of HCW, or the patient assists (Ulin et al., 1997). To date, directly measured forces at the hands have not been utilized with a detailed dynamic musculoskeletal model when estimating lower back IVJ demands throughout bed-to-chair transfers.
The primary aim of this work was to estimate the peak L5/S1 IVJ compressive forces during manual patient bed-to-wheelchair transfers by single HCWs. This work is unique in that it concerns variation in the level of patient assist using a system that controls the upward assistive force on the patient. Further, HCW-specific forces at the hands were synchronously recorded with kinematics. L5/S1 IVJ compression was estimated using a validated thoracolumbar spine musculoskeletal model (Bruno et al., 2015). For comparison to previous work, L5/S1 IVJ compressive forces were also estimated by assuming the patient’s mass is being fully lifted and evenly distributed between the HCW’s hands. We hypothesize that compressive forces will be lower relative to the patient assist level and when estimated with measured forces from the hands versus assuming the HCW lifted the patient’s bodyweight. By measuring the forces at the hands and systematically controlling the level of patient assist, this work can improve our understanding of the lower back kinetic demands in HCWs during bed-to-(wheel)chair transfers.
Method
Participants
Thirteen (n=13; ♀=11) HCWs were recruited and consented to individually perform manual single person bed-to-wheelchair transfers. All enrolled HCWs were healthy and presently employed in a job requiring daily bed-to-chair or bed-to-wheelchair patient transfers. The study protocol was approved by an Institutional Review Board (Advarra, Inc., USA)
The “patient” was a healthy able-bodied male, 1.7 m in stature, 64 kg in mass, and part of the research team (N.E.W.). During all transfers the patient maintained an upright torso but attempted not to provide any assistance with his upper or lower limbs. The patient’s feet were allowed to contact the floor during the transfer.
Equipment and Apparatus
All experimental activities took place in a biomechanics laboratory. The lab housed a motion capture system (Motion Analysis, USA), hospital bed (Hillrom, USA), standard 60-inch cotton transfer gait belt (COW & COW Care, China), load cells (Omega Eng. Inc., USA), and a wheelchair with a 50 cm seat height (Medline, USA). The motion capture system recorded (50 Hz) thirty-eight passive reflective markers systematically placed on the skin and over clothing of the HCW and two markers in line with the three-dimensional force vector of each load cell (Wiggermann, 2016). The load cells measured the external force at the HCW’s hands via direct attachment between the gait belt and cotton woven handles. The handles and load cells were located bilaterally on the gait belt near the patient’s iliac crests. The amplified output voltage from each of the load cells was synchronously recorded within the motion capture software.
A custom patient assist simulation system was designed to consistently simulate different patient assist levels by lifting a portion of the patient’s weight (Fig. 1A). This system allowed the patient to act dependent across all trials, eliminating the subjectivity of attempting to provide partial assistance. The patient was “lifted” via a series of ceiling mounted pulleys guiding a cable attached to the patient on one end and a counterweight on the other. The lift force was transferred to the patient through a lift vest (Liko® MasterVest; Hillrom, USA) connected to the overhead cable by a carabiner. The assist simulation system was employed only for the trials where simulated assistance was included as a factor.
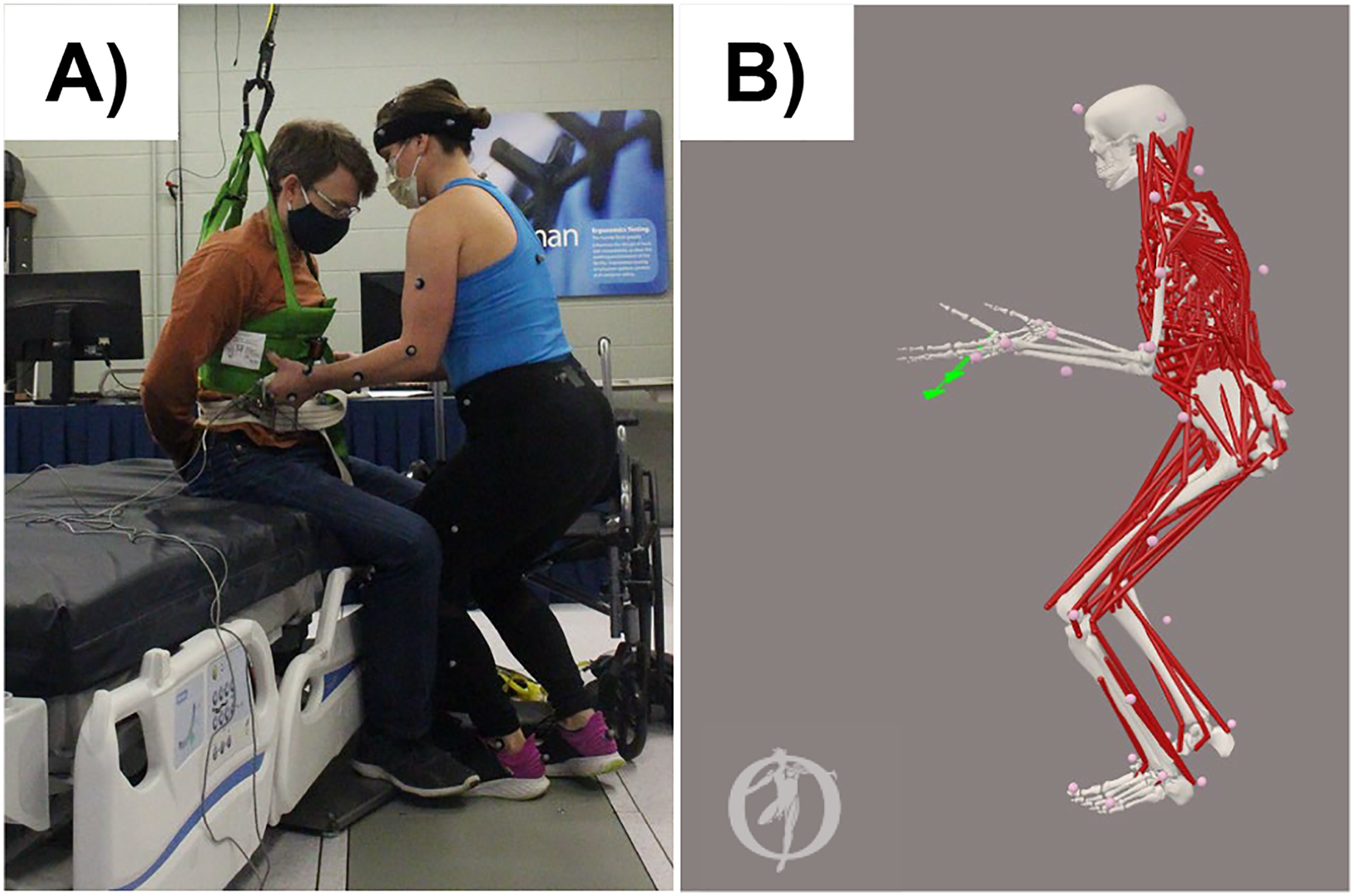
Panel A) Setup during an experimental trial, and B) full-body OpenSim thoracolumbar musculoskeletal model which estimated the L5/S1 intervertebral joint compressive force.
Experimental Design and Procedure
Prior to data collection, each HCW adjusted the height of the bed to their preferred location and practiced the bed-to-wheelchair transfer tasks. Transfer tasks consisted of manually moving the patient, prepositioned in an upright seated position on the edge of the bed, to a wheelchair located to the immediate right of the HCW and next to the bed (Fig. 1A). The wheelchair front wheels were locked in place and the right (i.e., most proximal) armrest and both foot pedals were removed to allow a direct path from the bed to wheelchair, which is standard clinical practice. HCWs were required to use the handles attached to the gait belt. Transfers were performed for three repetitions at each randomly assigned patient assistance level. The patient assist levels were 0%, 18%, and 36% of patient bodyweight. Two-minute rest periods were provided between each of the nine (3 repetitions × 3 assist levels) transfer trials to reduce fatigue and allow the patient to reposition himself on the bed.
Musculoskeletal Modeling Approaches
A top-down full-body musculoskeletal model (Fig. 1B; Bruno et al., 2015) based in OpenSim (Delp et al., 2007) was applied to estimate the peak L5/S1 IVJ compressive force from each transfer. In brief, HCW-specific musculoskeletal models were created based on gender, body mass, and marker positions from a static standing pose. Kinematics from each transfer were tracked by fitting HCW-specific models to the recorded marker positions. Static Optimization (Crowninsheild and Brand, 1981) estimated the necessary recruitment pattern necessary for 620 Hill-type (Millard et al., 2013) musculotendon actuators of the trunk to generate the kinematics and forces at the hands. Forces at the hands were prescribed by two distinct approaches. The first, and primary means, was with the measured force vectors at the hands (MFH). The second approach assumed the patient’s full bodyweight was evenly distributed between the HCW’s hands throughout the transfer (APW). For the APW approach, the patient’s mass was added to the hands of the model during the entire transfer time (see Data Analysis section details on how transfer time was defined) and varied based on each patient assist level. Both approaches applied the same HCW-specific model and kinematics. Muscle forces and reactionary joint forces were tallied to estimate the L5/S1 IVJ compressive force throughout all transfers from each approach. Prior to implementation, marker positions and hand forces were filtered using a fourth-order zero-lag low pass Butterworth filter with a 6 Hz cutoff frequency selected from a residual analysis (Winter, 2009). Tracked kinematics were filtered using a 4 Hz cutoff frequency for Static Optimization analysis. All modeling steps were conducted using OpenSim Tools (Delp et al., 2007) accessed with custom MATLAB (The MathWorks Inc., USA) API scripts (Lee and Umberger, 2016).
Data Analysis
Three dependent variables were obtained from each transfer: 1) transfer time, 2) measured vertical hand force at peak IVJ compression, and 3) L5/S1 IVJ peak compressive force. Transfer times were determined as the period where at least 10 N of force was measured at the hands. Measured vertical hand force at peak IVJ compression was defined as the vertical component of the three-dimensional force vector occurring at each hand at the instant of peak L5/S1 IVJ compressive force. L5/S1 IVJ peak compressive force was taken as the 95-percentile value calculated from each transfer and modeling approach. Transfer times and the vertical hand force at each hand were not part of the study aims but were included for added descriptive purposes.
The independent variables of interest were the three patient assist levels and, when applicable, the hand force modeling approaches. Individual repeated-measures one-way analysis of variance (ANOVA) compared the effect of assist level on the left and right vertical forces at the hand. The vertical force at the hands during the APW approach was not considered in the ANOVA as an independent variable because it was consistent and based on body mass. Similarly, as the times were comparably assigned between approaches, lift times were only compared across assist levels using a one-way repeated-measures ANOVA. Finally, a repeated-measures two-way ANOVA tested the main and interaction effects of both independent variables on the peak L5/S1 IVJ compressive force. Tukey’s Honest Significant Difference pairwise tests were used to compare all significant ANOVA findings (α < .05). All statistical tests were performed in custom MATLAB scripts.
Results
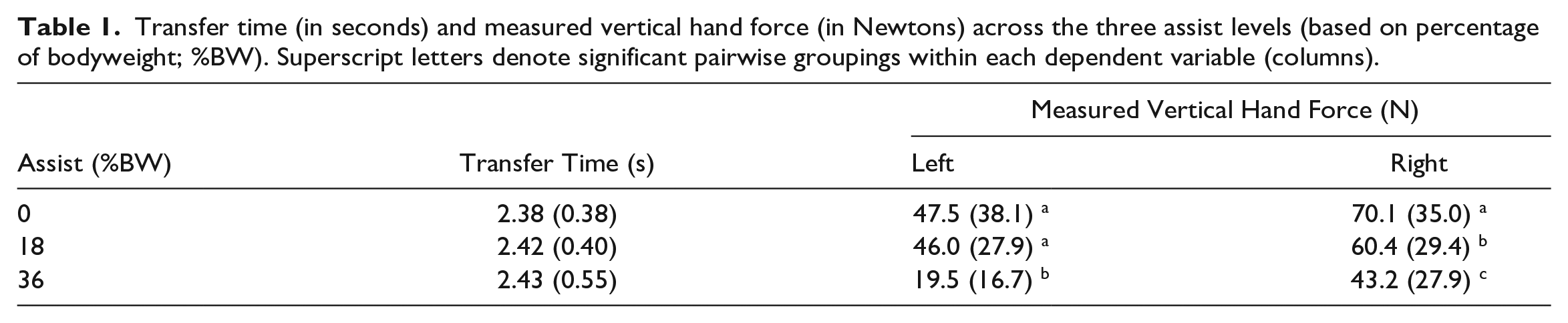
The time to transfer the patient from the bed-to-wheelchair was similar across the three assist levels (p-value = .864; ɳ p 2 = .012; Table 1). The measured vertical force at the left hand was different across assist levels (p-value < .001; ɳ p 2 = .526), with the 0 and 18% assist being similar and both less than the 36% assist level. At the right hand, peak measured forces were different (p-value < .001; ɳ p 2 = .514) across and inversely related to the three assist levels (Table 1).
Transfer time (in seconds) and measured vertical hand force (in Newtons) across the three assist levels (based on percentage of bodyweight; %BW). Superscript letters denote significant pairwise groupings within each dependent variable (columns).
Peak L5/S1 IVJ forces were different across the main effects of assist level (p-value < .001; ɳ p 2 = .880; Fig. 2) and hand force modeling approach (p-value < .001; ɳ p 2 = .979). Peak compressive force decreased as the level of assist increased and was lower when applying the MFH versus the APW approach. There was also a significant interaction effect between the assist level and the hand force modeling approach (p-value < .001; ɳ p 2 = .846). Post-hoc analyses of the interaction showed that all compressive forces estimated from APW were distinct from one another and those from MFH. However, the compressive forces from MFH during the 0 and 18% assists were not different from one another, but both were larger than the 36% assist level.
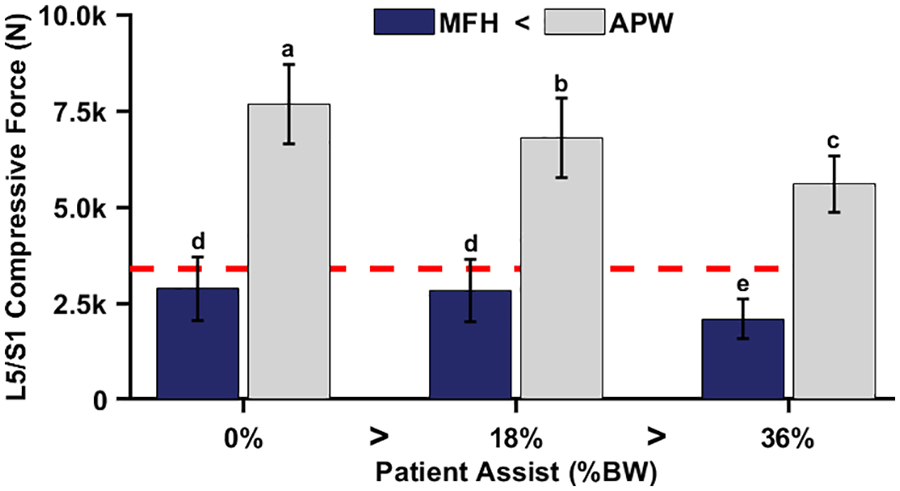
Peak L5/S1 intervertebral joint compressive forces (in Newtons) across patient assist levels (expressed as a percent of patient bodyweight; %BW) and between measured (MFH; dark blue bars) and assumed (APW; grey bars) approaches. Bars and data whiskers represent the average and standard deviation across participants, respectively. Greater and less than symbols and superscript letters indicate significant effect (α < .05) post-hoc relationships and pairings. The red dashed line provides a reference for an established ergonomic action limit of 3,400 N (Waters et al., 1993).
Discussion
The objective of this work was two-fold. First and foremost, we aimed to estimate the peak L5/S1 IVJ compressive forces during single HCW manual patient bed-to-wheelchair transfers at different patient assist levels from forces directly measured at the hands. Secondarily, we aimed to compare the compressive forces from our novel hand measurement approach (MFH) to those estimated using a more traditional approach which assumes the forces were the patient’s mass being fully lifted (APW). Our results supported our initial hypotheses and indicated that compressive forces on the HCW were lower when the patient assisted during the transfer and MFH were applied in the model in place of APW.
The patient assist level had a significant effect on compressive loads and forces at the hand. A relatively moderate 36% of bodyweight assist for our 64 kg patient reduced the compressive forces below the recommended ergonomic standard of 3,400 N (Waters et al., 1993). The 18% level of patient assist did not have a significant effect compared to the 0% level when using the MHF approach. Anecdotally, the lack of difference between the 0% and 18% assist levels may reflect how some HCWs become more willing to “lift” as opposed to “push” or guide the patient when they knew there was some level of assistance. The HCWs were not blinded to the presence of the assist. However, this is not unlike having prior knowledge of clinical patient’s weight or assist level. Regardless the overall difference between peak compressive forces highlights the importance of encouraging patients to participate in their transfers and thereby aid HCWs whenever possible.
The magnitude of peak compressive forces found in this study for single HCW transfers with 0% patient assist using the MFH were generally much lower than previous reports (Daynard et al., 2001; Garg et al., 1992; Marras et al., 1999; Silvia et al., 2001; Tang et al., 2018; Ulin et al., 1997). This discrepancy highlights the importance of using directly measured external forces whenever possible and the relatively low body mass of our patient. Regardless, the average peak compressive forces in this study from the MFH estimates still approach and in some instances exceed the recommended standard of 3,400 N (Waters et al., 1993). These high estimated compressive loads support the use of lift devices whenever possible, especially for heavier patients than the one transferred in this study.
The total measured vertical force at the hand was not equivalent to the patient’s body weight (~117 versus 630 N) during the 0% assist condition and did not directly reflect the change relative to assist level. The discrepancy between hand force and body weight is no doubt impacted by allowing the patient’s feet to contact the ground, which is appropriate in the clinic. The comparable hand and peak compression forces between the 0% and 18% assist condition may also highlight a technique adapted by experienced HCWs during transfers. It would again appear that in lieu of fully lifting the patient, whenever possible, the HCW choses to push and guide the patient off the bed and into the wheelchair. A push and guide technique would be less sensitive to the level of dependence of the patient. Also worth noting, the distribution of forces between the left and right hands appears asymmetrical. This finding warrants further investigation as to whether the more dominate limb is driving this discrepancy or the direction of the transfer.
While not part of our initial research aims, post-hoc we compared the shape and timing of the peak L5/S1 IVJ compressive force during the transfer in relation to the approach used (Fig. 3). Peaks during the MFH approach generally occurred near the first or last quarter of the transfer time. Conversely, when using the APW approach, the peaks tended to occur at the initial and final portions of the transfer. This once again highlights the importance of using measured external forces to better identify the instances where peak demands occur.
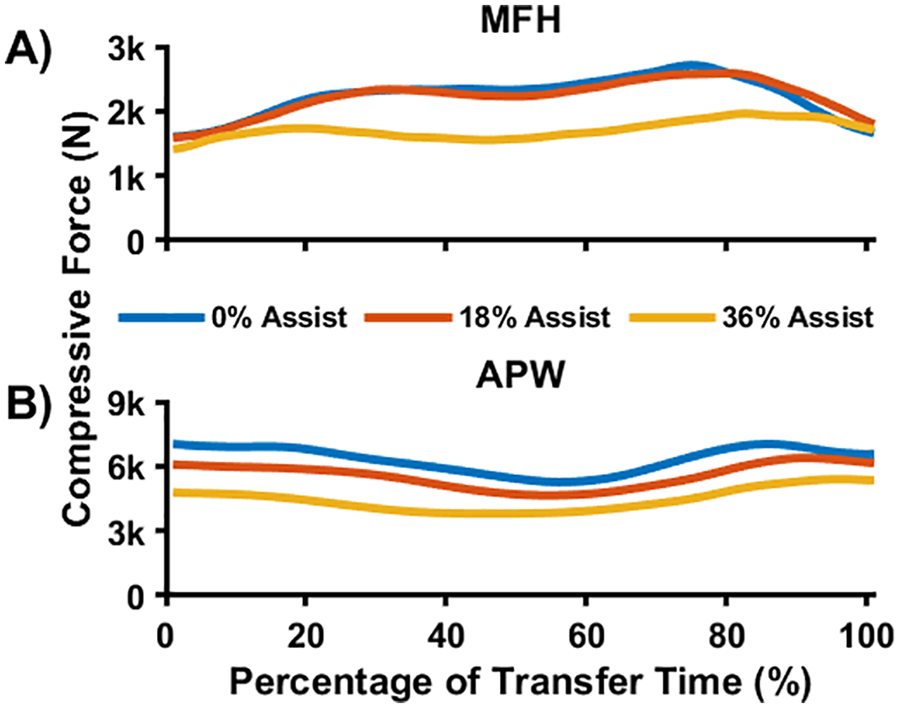
L5/S1 intervertebral joint compressive force (in Newtons) throughout the duration of the transfer time at the three assist levels (see accompanying legend for assist level delineation) when applying measured (MFH; panel A) and assumed (APW; panel B) forces.
This work has several key limitations that could have influenced our results. First, musculoskeletal models are inherently limited and should only be viewed as estimates of in vivo demands (Banks et al., 2022). Second, to measure the forces at the hands we slightly modified a gait belt and restricted the technique used by the HCWs. Compared to gripping a gait belt directly, this alteration created a small offset between the belt and hands to accommodate the load cells and handles. Furthermore, some HCWs will employ a “hug” technique where the patient’s arms are wrapped around the neck of the transferer. Including such a technique in our study would not allow for us to accurately measure the total external forces. However, the L5/S1 IVJ demands we estimated were still lower than those previously estimated for one-person manual lifts with a hug technique (Marras, 1999; Silvia et al., 2001), most likely due to the methods of estimating the external forces using the APW approach or an electromyography-driven model. Third, the forces we measured at the hand may be underestimated if the HCW’s hands contacted and squeezed the patient’s torso. We attempted to minimize this by asking the HCW to adjust their approach if the patient felt their technique was not being measured by the load cells. Fourth, although our novel system for simulating levels of patient assistance allowed us to apply repeatable lift assistance force, this force is not identical to how a patient assists a HCW to standing. Instead of applying a constant lift force, a patient would likely provide increasing levels of assistance as their knees and hips extend, and less at the beginning and end of the transfer. Because the IVJ forces can be particularly high when beginning to stand a patient, these simulated assistance levels may underestimate the physical stresses on caregivers compared to an equivalent percentage of effort from a patient. Fifth, our patient was healthy, relatively light weight, and not connected to any clinical devices. Future work could look at how the forces at the hands and L5/S1 compressive force estimations are impacted with actual patients in a clinical setting. Finally, the study design here signifies a poor ergonomic scenario for patient transfers. Best practice for safe patient handling and mobility is to use a motorized lift. One-person transfers should be avoided.
Conclusion
This was the first study to estimate peak L5/S1 IVJ compressive force demands using measured forces at the hands during a single HCW bed-to-wheelchair transfers across different simulated levels of patient assist. Our results indicated that 36% of patient assist can significantly lower peak compression on the HCW relative to a 0% (totally dependent) or 18% assist level. These findings suggest that encouraging the patient to assist during transfers may reduce spine loads on HCWs during this standard and important daily task. However, even a modest degree of patience is not likely to protect the HCW from elevated spine loads, especially when transferring heavier patients than the one studied here. In most all circumstances, lift equipment is still warranted. This study also found that the peak forces at the hand and resulting estimated compression forces were lower when using the actual measured forces rather than assuming the patient mass was fully lifted. This highlights the importance of properly modeling the external forces at the hand. Future work may consider examining how handedness and transfer direction impact the symmetry of the forces at the hand and how patient assist may impact HCW demands during other clinical situations (e.g., alternative transfers or sudden unexpected falls).