
Abstract
Disrobing of a casualty on the battlefield is a key step in treatment to ensure injuries have been properly treated. Hesitancy to fully disrobe female patients may result in poorer treatment provided to female casualties. The goal of this study was to determine whether patient gender predicted the occurrence of complete or partial chest exposure and whether the type of undressing method predicted complete or partial exposure. Second, we sought to determine whether simulator gender, undressing method, and chest exposure predicted differences in the treatment of a gunshot wound (GSW) to the chest. Thirty-six soldiers treated GSW on male and female patient simulators. Complete chest exposures were more likely with male patients or when shears were used. For male patients, there were fewer errors, chest was exposed completely, and tearing methods were used. Results indicate opportunities to improve wound discovery and decrease GSW treatment errors, particularly for female patients.
Responding to a combat casualty on the battlefield requires a combat medic to fully disrobe the patient to determine all points of injury. As such, combat medics should use the most efficient and effective clothing removal technique upon initial assessment (Sibley et al., 2018). However, rescuers often take longer to expose a female patient (i.e., are more reluctant) and more medical errors occur when treating a female patient (Kramer et al., 2015; Mazzeo et al., 2021). The failure to fully expose (i.e., disrobe) a patient may lead to differences in wound discovery (i.e., missed wounds, delayed identification of wounds) and differences in treatment decision making or performance (i.e., lack of treatment, improper treatment).
Undressing Methods in Trauma Care
Research investigating trauma care undressing methods, their efficacy, and patient gender differences is limited. Although rapid exposure to a trauma patient is necessary when first assessing the patient, there are no standardized methods for optimal clothing removal (Sibley et al., 2018). A limited number of studies have investigated the efficacy of using cutting hooks over trauma shears to expose simulated trauma patients (Cummings et al., 2022; Hurtado & Montoya, 2009; Tang et al., 2014). Another study found that using a cut and rip technique was faster and could save time when assessing a critically ill trauma patient (Sibley et al., 2018). Studies examining how clothing removal techniques are used in the field appear to be absent from existing literature, particularly in the context of patient gender and clothing styles.
Gender Differences in Patient Exposure
Previous research suggests that many students experience anxiety when treating sensitive areas of the body that require clothing removal (e.g., performing pelvic exams) due to fears about causing harm or the intimate/personal nature of performing a pelvic exam (Pugh et al., 2009). A sizeable body of research suggests that bystanders are more reluctant to treat female patients due to misconceptions about women in medical distress, fears of causing injury (e.g., beliefs that women are fragile), concerns over physical barriers (i.e., female breasts), and fears of having to remove clothing (i.e., exposing the patient) (Ahn et al., 2016; Becker et al., 2019; Blewer et al., 2018; Perman et al., 2019). Hesitancy to treat women has even been identified in groups as young as middle schoolers, whose boys were less likely to feel comfortable administering CPR on their female classmates (Wingen et al., 2022). Further, lay rescuers report they felt they only need to remove enough clothing to place defibrillator pads according to the AED instructions rather than ensuring the brassiere would not affect CPR, even when provided with a front-opening brassiere during simulation (Kramer et al., 2015). However, simulation-based training can reduce this anxiety and improve rescuer comfort (Orsi et al., 2020; Pugh et al., 2009).
Gender Bias and Medical Decision Making
One explanation for the observed differences in patient exposure may be due to patient gender differences. Patient characteristics (e.g., gender) can lead to stereotyping and biases that might influence diagnosis, treatment options, and outcomes (Goel, 2018). For example, gender biases in medicine may result in overdiagnosis of favored gender and underdiagnosis of the neglected gender (Croskerry, 2002). For example, women with chest pain are less likely to be treated within the first hour of arrival to the hospital and are less likely to be treated with urgency, even when they present similar symptoms as their male counterparts (Clerc Liaudat et al., 2018; Mnatzaganian et al., 2020). Moreover, rescuers avoid touching a female patient’s breasts with their hands when performing CPR compared to male patients (Kramer et al., 2015). Consequently, women receive less bystander care for cardiac arrest overall, regardless of situation (Blom et al., 2019; Jarman et al., 2019).
Objectives
As such, the goal of this work was to first determine whether patient gender predicted the occurrence of complete or partial chest exposure when treating a patient with GSW to the chest and whether the type of undressing method predicted complete or partial exposure. Second, the research team sought to determine whether simulator gender, undressing method and chest exposure type predicted differences in the treatment of a GSW.
Method
Participants
A total of 36 participants (n = 8 or 22.2% female) completed the study. Fifteen participants had the designation of combat lifesavers (CLS), nineteen were combat medics, one participant had other designations (e.g., Ophthalmic Tech), and one participant had no medical training. Participants' medical training experience ranged from at least 2 days to 17.5 years. Nine (25.0%) of the trainees had less than one month experience, 10 (27.8%) of the trainees had between one month and two years of experience, 15 (41.7%) of the trainees had more than 2 years of experience, and two (5.6%) did not report their experience. The age range was 18 to 41 years old, with 27 (75.0%) of participants between 18 to 29 years, and 9 (25.0%) were between 30 to 41 years.
Study Design
Participants treated two simulated patients, one female and one male. The study was a mixed factorial with patient simulator gender as the within-subjects variable and Patient Simulator Order as the between-subjects variable. This resulted in a 2 (Female Simulator, Male Simulator) by 2 (Female First, Male First) design, with participants randomly assigned to each condition. The study was reviewed by the University of Minnesota IRB (STUDY00013436) and the U.S. Army DEVCOM Soldier Center (UN-210003), both of which determined it was “Not Human Subjects Research” as defined by DHHS and FDA regulations. However, participants read a study information sheet and provided verbal consent to research staff prior to their study participation.
Procedure
Trainees treated two SimMan3G simulated patients or simulated casualties, one male and one female fitted with the Simetri gender retrofit kit (GRK), in counterbalanced order. Each patient had a GSW to the chest (i.e., entrance wound near the breast and exit wound on the back) that required complete chest exposure to reliability detect and treat. Patients were dressed in an Army Combat Uniform (i.e., trousers, blouse, t-shirt, and, for the female patient, tan sports bra). Participants were instructed to treat the patient using the patients individual first aid kit (IFAK) which included shears. Participants were fitted with a combat helmet with mounted camera to record a first-person perspective of their treatment of each patient.
Three trained coders rated video footage of the tactical field care scenario for the undressing behaviors including the start time (time stamp), the article of clothing being removed (e.g., bra, undershirt, blouse), the method of article removal (i.e., cut, cut/tear, lift), and the body part or clothing that was exposed. A complete chest exposure was coded as either exposing the patient’s right breast with the areola, left breast with the areola, or both. A partial chest exposure was coded as either exposing the patient’s right breast without the areola, left breast without the areola, or both. Two videos from each participant, one treating a female patient and another treating a male patient, were coded using this methodology resulting in 72 tactical field care scenarios coded for this analysis.
Coded Variables
Gunshot wound treatment errors
Three trained coders reviewed participant video footage to assess performance in properly treating patients for GSWs. Performance metrics coded as being done correctly (yes), not completed, done incorrectly (no), or unable to define (unknown). For each participant, raters coded the exposing of each wound, finding of each wound, and the proper wound treatment via chest seal application. Any metrics coded as Unknown were reviewed by the entire coding team to determine final coding as either ‘Yes’ or ‘No’. The performance metrics were aggregated into a total error count variable (i.e., summed score of all 'No’s’), resulting in a maximum error count of 6 for the chest seals.
Undressing and chest exposure variables
Undressing and chest exposure variables were coded using a binary coding system (yes/no). Coded variables included the article of clothing, undressing method, and chest exposure type. Article of clothing included the blouse, undershirt, and bra. Undressing method was coded as the method used to undress or dress the patient, which included tearing, cutting, and lifting. Chest exposure type was coded as a partial chest exposure (i.e., partial right breast with no areola exposure) or partial left breast with no areola exposure, and as a complete chest exposure (i.e., complete right breast with areola exposure or a complete left breast with areola exposure).

Example of partial chest exposure, lifting method for t-shirt and bra, female patient simulator.

Example of complete chest exposure, cutting method, male patient simulator prior to applying chest seal.
Interrater Reliability (IRR)
Each participant’s footage was reviewed by two coders that scored whether each of the two GSW (chest and shoulder) were found by the participant for both the male and female patients (4 categories of agreement). For the male patient, there was perfect agreement between the two coders for finding the chest GSW. For finding the GSW on the shoulder, there was perfect agreement between coders. For the female patient, there was perfect agreement among coders for finding the GSW on the chest. For finding GSW on the shoulder, there was a Cohen’s κ of .929. Any disagreements between the coders were reassessed by the coding team to determine a final singular dataset.
For method and exposure, agreement was determined by concurrence between at least two of three raters, and concordance on the timestamp within four seconds, the action, the method and either the article or body part/clothing exposed. Interrater reliability was examined for the action type (e.g., exposing, covering), article (e.g., blouse, bra), method (e.g., cut, tear, lift), and body part or clothing exposed (e.g., bra, partial left breast). Because there were multiple raters, Fleiss’ Kappa was used to determine the interrater reliability amongst the three coders (Fleiss, 1971). The agreement coefficients ranged from moderate to good. For article ratings, Fleiss’ κ = .645, for undressing method ratings, Fleiss’ κ = .685, and for exposure ratings Fleiss’ κ = .568. Disagreements in coding were again reassessed by the coding team to determine a final singular dataset.
Results
Frequencies and percentages were computed for each undressing method and type of chest exposure (i.e., complete exposure or partial exposure) by trainee experience and simulator gender. Data was analyzed using R (R Core Team, 2021). Overall, partial chest exposures occurred 30.6% (n = 22) of the time while complete chest exposures occurred 88.9% (n = 64) of the time. The use of the lift method was observed most often (n = 54 or 75.0%), followed by tearing method (n = 36 or 50.0%), while the cutting method was observed the fewest times (n = 11 or 15.3%).
Undressing method and chest exposure varied by simulator gender. The lift method and cut method were used more often on female patients, while the tear method was used more often on male patients. There was a significant difference between simulator gender and the use of the cut method, χ21 = 6.91, p = .009. Additionally, partial chest exposures occurred more often on female patients (n = 14 or 38.9% of participants) while complete chest exposures occurred more often on male patients (n = 35 or 97.2% of participants).
Frequencies and percentages were calculated for undressing methods across trainee experience levels. Trainees with less than one month experience (n = 15 or 83.3%) used the lifting method the most often, trainees with less than two years’ experience used the cutting method most often (n = 10 or 50.0%) and trainees with more than two years’ experience used the tearing method most often (n = 19 or 63.3%). There was a significant effect of using the tear method by trainee experience, χ22 = 7.97, p = .019. Additionally, those with less than one month experience had the most partial chest exposures (n = 9 or 50.0%), while trainees with more than two years’ experience had the most complete chest exposures (n = 28 or 93.3%).
Predictors of Chest Exposure
Binary logistic regressions examined the effect of simulator gender, trainee experience, and undressing methods, while blocking for order of treatment (i.e., female first, male second or male first, female second) on a binary outcome of whether or not the patient’s chest was completely exposed (i.e., right breast, left breast, or both) and a binary outcome of whether the patient’s chest was partially exposed (i.e., partial right breast, partial left breast, or both).
Complete chest exposure
Results indicated there was a significant effect of simulator gender on complete chest exposure. Male patients were significantly more likely to have a complete chest exposure, B = 3.52 (SE = 1.20). Additionally, there was a significant effect of using the cut method on complete chest exposure, B = 4.63 (SE = 1.83). The more the cut method was used, the more likely the patient would have a complete chest exposure. See Table 1 for a summary.
Model Summary for Predictor of Complete Chest Exposure.

Note. R2 = .42, χ2(7) = 21.02, p = .004.
Partial chest exposure
For the partial chest exposure model, there was a significant effect of simulator gender on whether a partial chest exposure occurred. Male patients were significantly less likely to have a partial chest exposure, B = -1.44 (SE = .66). Table 2 presents a model summary of predictors of a partial chest exposure.
Model Summary of Predictors of Partial Chest Exposure.
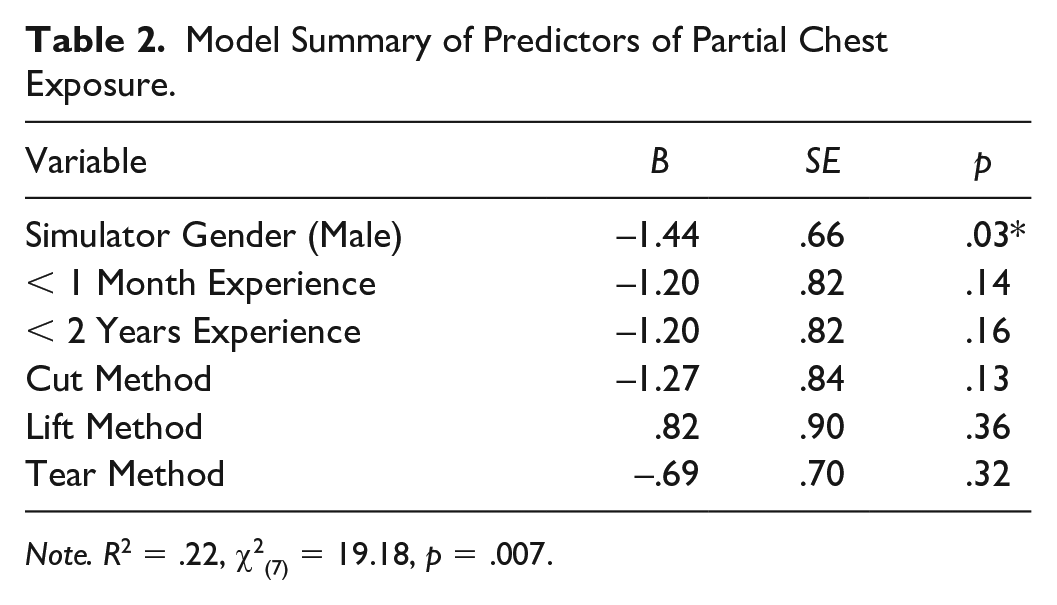
Note. R2 = .22, χ2(7) = 19.18, p = .007.
Undressing Method and Chest Exposure Type as Predictors of GSW Errors
Negative binomial regression models examined whether the frequency of undressing method (i.e., cutting, lifting, and tearing) and whether the frequency of chest exposure type (i.e., complete and partial) predicted the number of GSW treatment errors, while controlling for treatment order and trainee experience. Data was analyzed using the MASS package in R (R Core Team, 2021; Venables & Rupley, 2002).
Undressing method, gender and GSW treatment errors
For the undressing method model, there was a significant effect of simulator gender on the number of GSW treatment errors, with male patients being significantly less likely to have a GSW treatment error, B = -.68 (SE = .30). There was also a significant effect of the tearing method on the number of GSW treatment errors, with fewer tears leading to more GSW treatment errors, B = -.45 (SE = .18). See Table 3 for a summary of undressing method as a predictor for GSW errors.
Model Summary for Undressing Method as a Predictor of GSW Errors.

Note. R2 = .20, χ2(7) = 44.68, p < .001.
Chest exposure, gender, and GSW errors
For the chest exposure model, there was a significant effect of the number of complete chest exposures on the number of GSW treatment errors, B = -.22 (SE = .10). The findings suggest that fewer complete chest exposures led to more GSW treatment errors. See Table 4 for a summary of chest exposure type as a predictor of GSW treatment errors.
Model Summary for Chest Exposure Type as a Predictor of Gunshot Wound Treatment Errors.
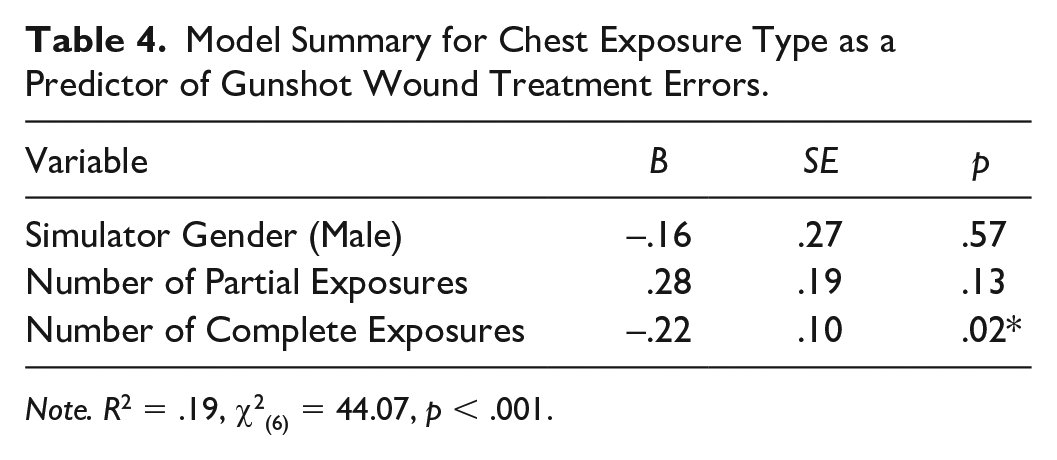
Note. R2 = .19, χ2(6) = 44.07, p < .001.
Discussion
Taken together, the results from this work suggest that trainees found the GSW more often on male patients compared to female patients and finding the GSW was associated with exposing the patient’s entire chest. There was also an effect of using the tearing method on GSW errors. This illustrates military medical training to perform rapid/tactical trauma assessments to quickly identify and address life threatening injuries in combat. Finally, more partial chest exposures were observed on female patients; however, these partial chest exposures were not associated with locating the GSW.
Women have served in active-duty combat roles since 2015 and require effective treatment and parity in treatment outcomes when possible. The results presented here indicate one possible contributing factor for the gender disparity in outcomes for chest and airway injuries on the battlefield (Barbeau et al., 2021; Cross et al., 2011); and suggest one path for training interventions to improve treatment outcomes for soldiers. Training standards should consider inclusive design when it comes to gender and emphasize not only treatment of both genders when practicing these procedures, but also consider practicing task steps that are not normally considered critical, such as undressing and disrobing.
Considering healthcare more broadly, there appears to be a paucity of research indicating best practices for disrobing and diagnosing patients, which becomes critical in a time-pressured context, including emergency medicine and battlefield medicine. The present research represents a tentative step in investigating human performance in this space. Besides gender, the cutting method appeared to be the most effective for complete chest exposures, and complete chest exposures were predictive of locating the injury in question. It remains to be seen whether this is true for all injury locations and types, or for all types of cutting, as some research has considered different types of shears.
Limitations and Future Directions
For this type of research, the study has a somewhat small sample size, which means some effects may not be detected due to low power. The relatively small sample size limits the ability to confidently extrapolate the findings and may lead to variable or biased results. Replication of this study with a comparative or larger sample is necessary. Furthermore, the wide range of trainee experience reported here may fail to capture some study effects. The observed differences in exposure rates may be explained by a lack of familiarity with bras or due to pre-existing attitudes and beliefs about female soldiers (i.e., preserving modesty/decency) resulting in differences in the degree of chest exposure. This study did not assess trainee attitudes and beliefs about female modesty, nor did it ask participants about previous experience treating female patients.
Future work should aim to determine the influence of pre-existing attitudes on decision making for the treatment of a female chest injury and test these findings with more constrained experience ranges (e.g., under 1 year or between 1 to 2 years of medic training). Other research should consider factors that may contribute to differences in outcomes, such as expression of symptoms. Living patients may communicate with their caregivers, and this communication and differences in communication styles and perception may affect the diagnosis and treatment of injuries. Finally, the lack of a formal undressing training protocol suggests a need to develop efficient, standardized clothing removal techniques that may be practiced by trainees to improve patient care for all soldiers.
Conclusion
The representation of female soldiers in the United States Armed Forces has been steadily increasing in recent years and the observed disparities in the discovery and treatment of GSWs to the chest experienced by female soldiers must be addressed. Understanding the underlying causes of these observed disparities in undressing methods to expose the chest and treatment decisions for a penetrating chest injury (e.g., lack of familiarity, gender biases, and/or maladaptive training) will inform how modifications to current battlefield medic training can best mitigate these observed differences to improve patient care and treatment on the battlefield. Findings from this work may be applicable to the medical field outside of combat medicine, particularly in emergency medicine.