
Abstract
Strength data for children are needed to improve the safety of products. Currently, minimal information on strength is available for children under age 6 years. This paper describes the development of methods to measure functional, task-relevant strength for children ages 24 to 71 months. Strength measurement methods used for adults and older children must be adapted substantially to obtain meaningful data from this younger cohort. This paper discusses the challenges associated with gathering volitional, maximal force-generation capability for this age cohort with attention to applicability, repeatability, and reproducibility.
Introduction
Data on the strength of children are needed to improve the safety of products for children through testing and support for standards development. Functional strength capabilities of children are imperative to inform the design of products that children encounter to reduce or eliminate the risk such products pose to a child (e.g., breaking, collapsing, or liberating a small part). Currently, minimal information on strength is available for children under age 6 years. Brown et al. (1973, 1974) conducted a study of strength capabilities of children ages two through six. Two custom devices were developed: a push-pull and pull-apart tester to quantify hand and grip strength for a range of postures. Except for children aged 2-3, boys were found to have greater average maximal strength than girls, though the difference in absolute magnitude was small. Strength was also observed to increase linearly with age.
Owings et al. (1977) conducted a study of the strength of U.S. children ages 2-10 years. The study included 33 isometric exertion measures conducted on an instrumented reclining chair. Isolated joint strength was measured at wrist, elbow, shoulder, ankle, knee, hip, and trunk. Grip strength measurements were also collected including: 2-pt, 3-pt, 5-pt pinch grips, lateral grip, and squeeze with different degrees of hand closure. For most measurements, no significant differences were noted between boys and girls, but strength was found to increase with age.
Norris and Wilson (1995) published a comprehensive compendium of child anthropometry and strength measures titled “CHILDATA” that draws on a wide range of sources. Strength measures included push forward, push downwards, push sideways, pulling, lifting up against a range of handle configurations, in both vertical and horizontal orientations and in standing and seated postures. Hand grip strength measures included: hitting force with a fist, wrist twist, opening strength, squeeze grip and varying pinches. The U.K. Department of Trade & Industry (DTI), Government Consumer Safety Research (2000) conducted a strength study for design safety. Hand strength measures included: finger push, pinch-pull, hand grip, wrist-twisting, opening strength, push and pull strength. Whole-body strength measures included: maximal push and pull strength, push with thumb or 2-or-more fingers, push with shoulder, maximal pull with different grips, wrist twisting and push-and-turn strength, pull on a can ring-pull, and press and lift with foot (DTI, 2002). Strength was observed to increase with age and for most measurements no significant sex differences were found.
This paper discusses considerations in the development of methods suitable for measuring the strength of children ages 24 to 71 months. The widely varying verbal and physical development of this cohort in comparison with older children and adults necessitates adaptations that enable reproducible and relevant data.
Study Design Considerations
What is Strength?
The seemingly simple idea of human “strength” is of course very complex. Obtaining the “maximum” from any measurement that includes variability is always challenging from a statistical perspective, but measured human strength is influenced by a large number of factors that affect the applicability of the resulting values. The force values interpreted as strength are obtained in a context that includes the instructions to the participant, the required postures, the task interfaces (for example, handle size, shape, and friction), the environment, the participant’s motivation, and the nature of feedback, if any.
In addition, the methods for measuring the force exertions, such as the choice of load cells and signal processing, also influence the outcomes. Finally, distilling complex, time-varying multivariate force data into a single “strength” value requires decisions about filtering and averaging that do not have an obviously correct choice. Is the average of one or more seconds of data the appropriate value? How much variability should be allowed within that window? Using longer window for averaging (effectively, low-pass filtering) diminishes the influence of peaks, but peaks may be more relevant for some applications.
Making these decisions more complex is the fact that the average strength of a cohort (for example, three-year-olds) is not the primary metric interest. Instead, values in the upper tail of the distribution (for example, 95th or 99th percentile) are of more importance for safety related design guidelines and regulation. Consequently, the influence of these study design and data processing decisions on extreme values, not just population means, must be taken into account.
A primary conclusion from synthesizing and attempting to apply the prior literature in this area is that a rich dataset must be gathered and maintained for future analyses as application needs change. In the past, the only outcomes retained from most studies were summary statistics for age cohorts, or more rarely single values per participant. The task postures are not available except as prescribed, and the actual force vectors exerted are not reported. The lack of time-series data means that alternative calculations (say, using a different time window for averaging) cannot be performed.
To address the need for data for this young age cohort, new laboratory methods were developed through an in-depth process of research and pilot testing. The following sections discuss some of the considerations that have gone into the design of the study.
Safety
When working with children, safety considerations must be given the highest priority. All study team members who interact with minors participating as subjects must complete comprehensive training modules focused on polices and issues related to the health, wellness, safety and security of children, and consent to a background check. In adherence with best practices for research with children, all research staff interactions with children must be witnessed by an adult third party. As such, caregivers must accompany their child throughout testing sessions, in addition to two research investigators.
A purpose-built laboratory outfitted with force measurement equipment, child-friendly furniture, and surfaces was developed. Transparent partitions enable the lab to separate a dedicated rest space from the testing apparatus for the child participant, caregiver, and siblings. This provides a safe place to take breaks and rest when the testing fixtures are being re-configured, and for caregivers and siblings to watch and support the child participant during the testing session.
To mitigate risk associated with slips or fall while interacting with the testing apparatus, the handle locations are scaled to the child’s body dimensions and padding is applied to key components. Figure 1 shows a view of the laboratory, showing the partitioning, dedicated rest space, and padding.

Consent room and laboratory for child strength measurement.
Laboratory Layout
Importance must be placed on the engagement and interaction between the child participant and investigator. Initially two investigators meet the child and caregiver in a child-friendly, consent room, one to focus on the caregiver and one to support the child. The intent of the consent room is to provide an environment that enables an investigator to engage the child in age-appropriate, play-based interaction and to briefly assess the child’s temperament, physical, and verbal development.
The laboratory is designed to help the child feel safe but alert. The color scheme, testing apparatus, and handle interfaces are intentionally muted to emphasize the engagement between the child and investigator. The presentation of the measurement apparatus is minimized to not cause distraction or look scary. The most visually interesting object in the testing environment is the force feedback display. The physical laboratory space also ensures privacy and sufficient space for caregiver, investigator, participant. Figure 1 shows the child-friendly consent room, laboratory layout, and color scheme.
Task Selection and Definition
When considering strength data for design, the interest is always in children doing something, i.e., performing a purposeful exertion. Research with adults has shown that isolated joint strength is not usefully predictive of strength in more functional activities such as pushing and pulling (Hoffman et al. 2011; Jones et al. 2013). Moreover, the interfaces used to obtain isolated joint strength are not task relevant and difficult to reproduce. Consequently, functional exertions with application relevance will be most useful. However, the exertion task must be defined in such a way that it is age-appropriate and reproducible.
With these considerations in mind, forces exerted by the hands and feet are paramount, and the overall body posture and level of constraint are also important. The posture constraints should be application relevant, which means that the children should be allowed to select their postures within the range permitted by the task definition. Following the prior literature, we have divided tasks into standing and seated and developed tasks that involve exertions with the hands and feet. The number of tasks of interest is potentially very high, when considering the variety of potential interfaces, postures, and force directions. The desire to gather data for a large number of exertions must be balanced against considerations of attention, motivation, and fatigue.
Interfaces
Forces are exerted on the environment through interfaces that affect the outcomes. For example, a sharp edge on an interface could limit the force that a child is willing to exert. Some of the considerations are:
Application relevance – The choice of interface limits the applicability of the data. Laboratory tasks are idealized versions of real-world tasks but, to be useful, must map well to tasks of interest for design.
Size – The diameters of interfaces such as cylindrical bars used for push/pull tasks affect outcomes, particularly for pulls. Ideally these would be varied, to quantify the effects, but this may not be practical given the limited amount of time available with a participant.
Shape – Similarly, the shape of the interface can have large effects, particularly for hand-intensive tasks, such as twisting smooth vs. knurled knobs.
Friction – The friction at the task interface is often a limiting factor, for example when pulling on a cylindrical handle. The choice of interface features affecting friction poses a conflict between the desire to maximize force generation and reproducibility. Flat, smooth metal surfaces provide the best reproducibility, but surfaces coated with high-friction materials will result in higher force values and may be more application relevant. A combination of both types of surfaces may be useful, provided they can be sufficiently well characterized.
Reproducibility – The challenge of creating reproducible methods means that all interfaces must be described well enough to be recreated in all details that affect results. For this reason, custom interfaces are generally preferred over commercial products, for example. The documentation must include relevant dimensions and materials. Ideally, a three-dimensional model or design drawings would be available.
Figure 2 shows some of the interfaces that have been developed. A 14-mm-diameter bar covered with 8-mm-thick foam is used for two-hand standing and seated exertions. A variant with the same diameter but shorter length is used for one-hand exertions. To ensure relevance for furniture and other applications, one-hand pulls with a range of real product interfaces is also included (Figure 3).
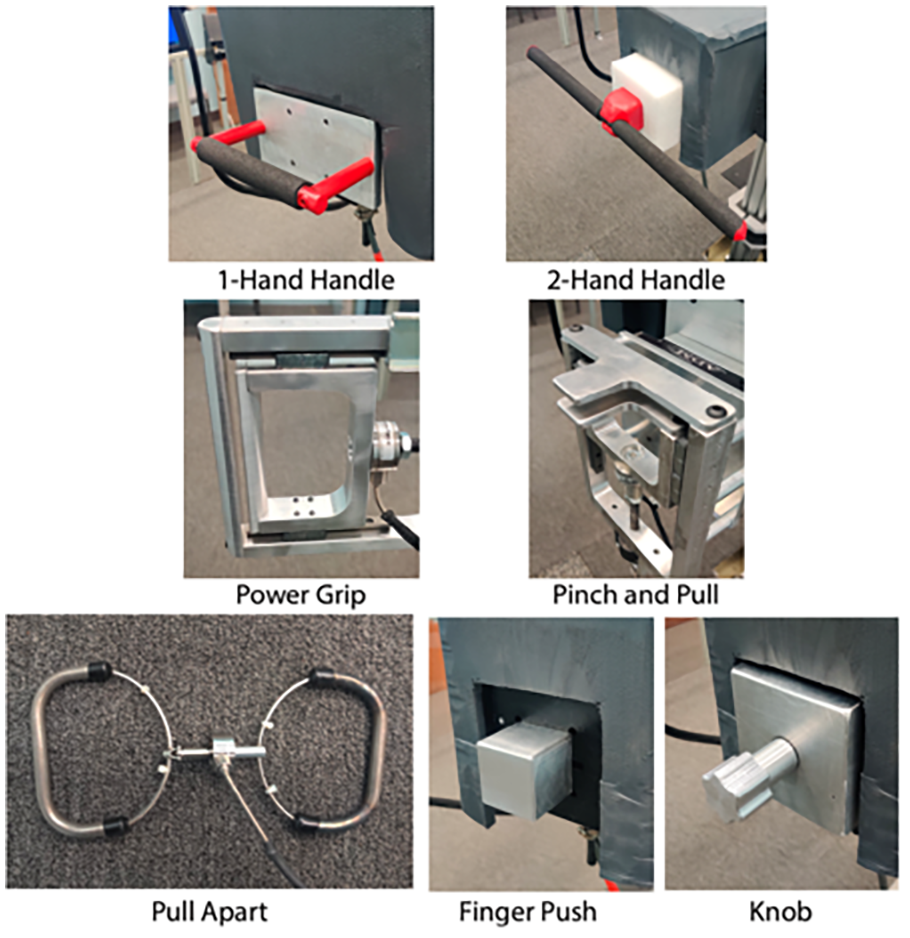
Idealized interfaces.
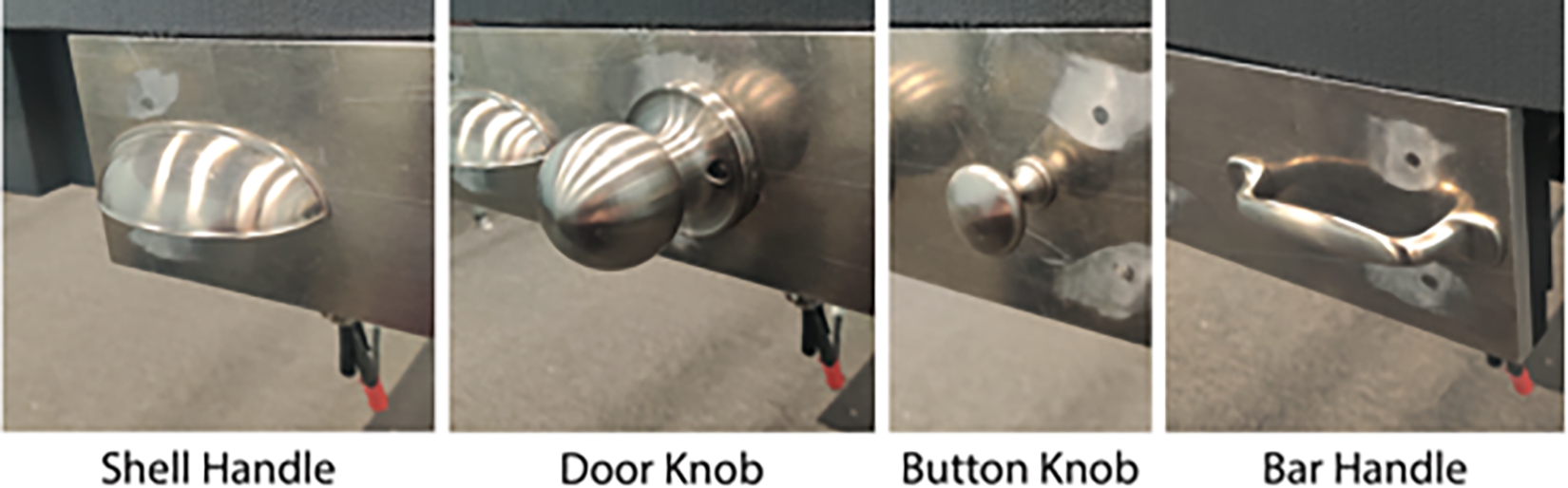
Real interfaces.
Postures
One of the limitations of prior work in this area is inadequate description of both the posture instructions and the criteria for defining an acceptable posture (beyond “standing” or “seated”). In our pilot work, we found that children find many creative ways to perform requested exertions, necessitating decisions at several levels. First, guidelines and methods are needed for the investigators to coach the desired postures. For example, a one-hand push must have only one hand on the handle and the other hand cannot be “helping” by grasping onto the forearm above the task hand. Second, we need to have post-hoc criteria for reviewing an exertion to decide which postures are acceptable. For example, we have determined that, for standing one-hand pushes, the only contact with the ground can be with the shoes (i.e., no kneeling) but a single foot contact (other foot lifted) is acceptable. Figure 4 shows some of the postural variability in standing exertions. The large amount of variability necessitates careful documentation (photos of each trial) as well as documentation of the participant instructions and subsequent screening methods. To obtain more complete postural data, we have equipped the laboratory with a 3D markerless motion capture system (Park et al. 2020).
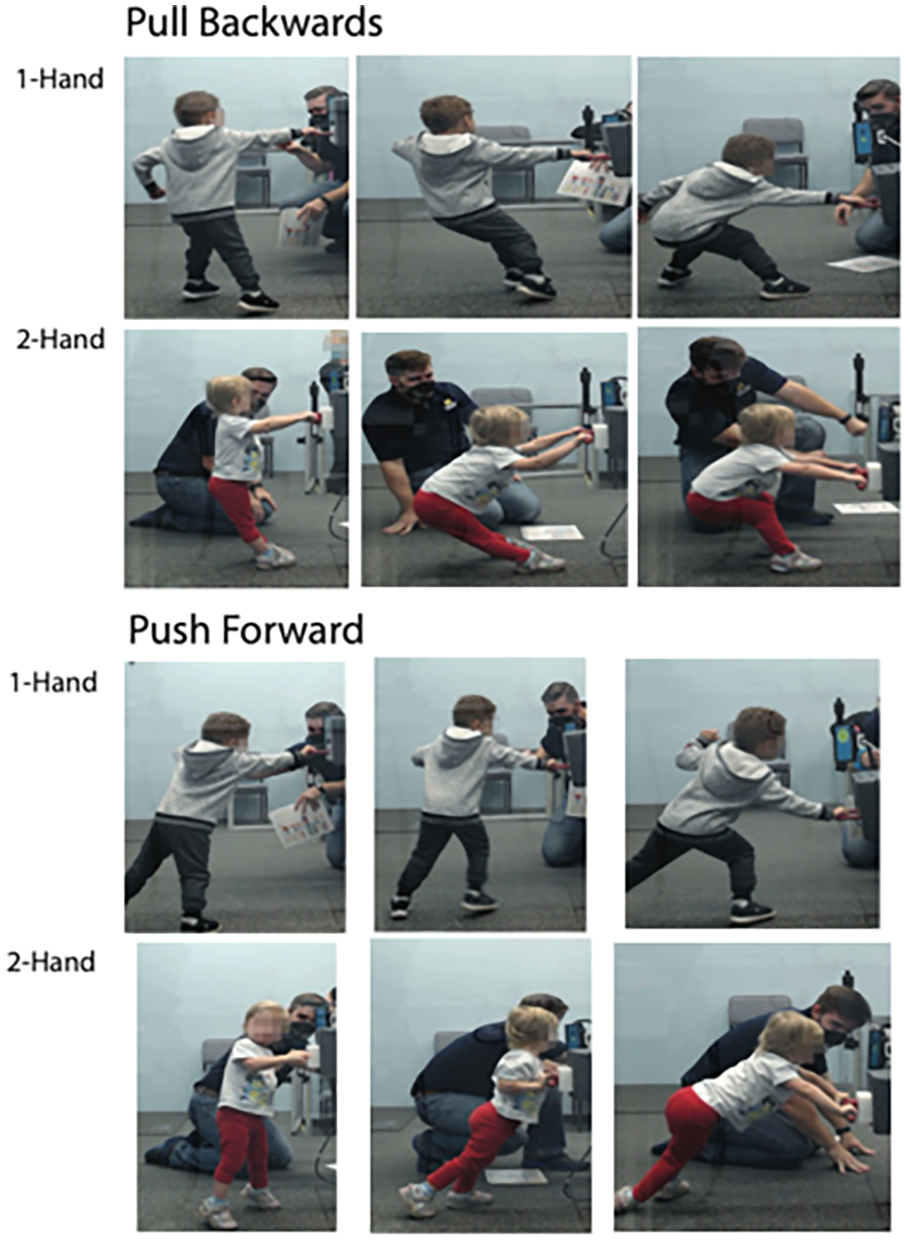
Postural variability in standing exertions.
Task Scaling
One important component of task definition is whether or how to scale for anthropometric variability. Consider for example the handle height for a standing push. Using a fixed height (say, the height of a typical baby gate) simplifies interpretation of the results for design and regulatory applications. However, it means that the task is substantially different dependent on the child’s body size. Following our prior work with adults (Hoffman et al. 2011; Jones et al. 2013), we have scaled the majority of the task conditions based on body size. This enables a focus on the strength of the child, rather than the population capability for the task. For example, standing push/pull tasks are performed at thigh, elbow, shoulder, and overhead heights, each defined as fraction of stature. We also present push/pull tasks for a simulated baby gate at a fixed height for all participants. Seated tasks are scaled to achieve approximately equivalent knee and elbow angles across participants.
Motivation and Feedback
Volitional strength is always dependent on the context, which includes the participant’s motivation and the manner in which feedback is presented. These aspects of strength testing are the most difficult to develop, standardize, and document for reproducibility, and yet are critical for interpreting the resulting data.
The motivation environment must be positive to enable continual engagement with the child. It would not be ethical to create surprise, fright, or other adverse stimuli to elicit exertions, even if these might be hypothesized to result in higher forces (Figure 5). Importantly, this age cohort generally cannot respond consistently to verbal instructions that might be sufficient for adults. In consultation with child development experts on the team, and after considerable pilot testing, we developed a visual feedback system shown in Figure 6 that is used in parallel with positive coaching and encouragement from the investigator.
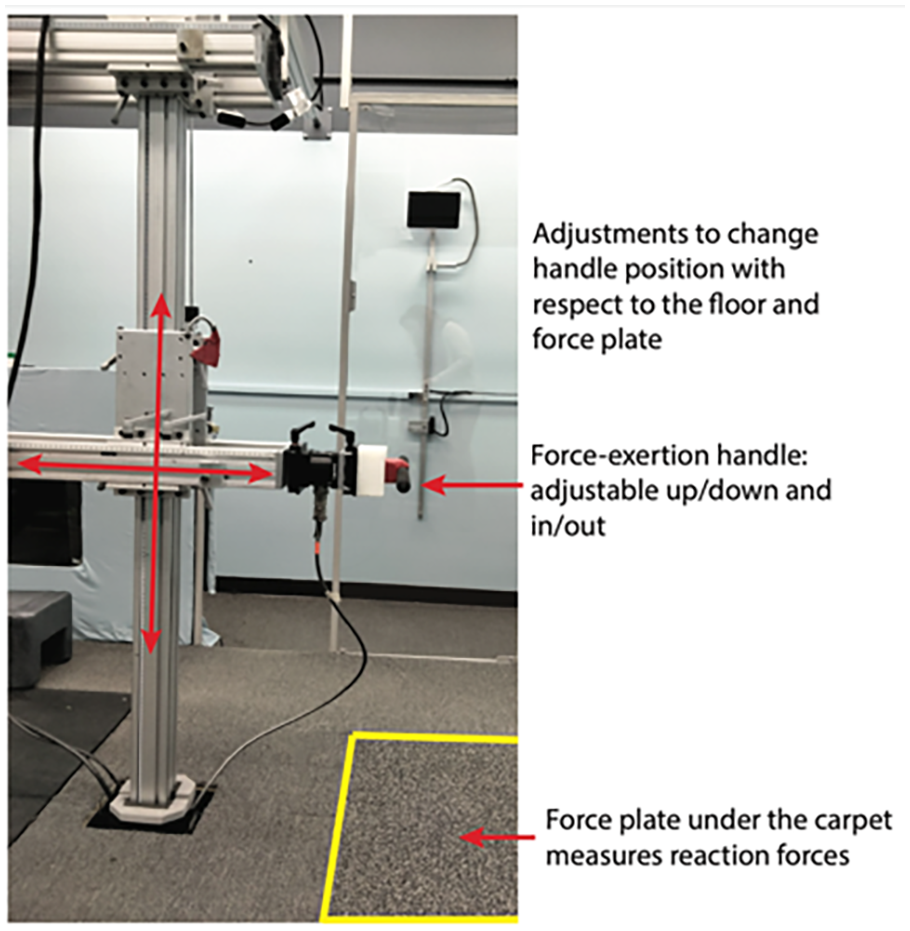
Images of the laboratory fixture for measuring strength in standing exertion tasks.

Force feedback display presented to the child participant at 0%, 50%, 100%, and 150% of the previous maximum force.
The feedback display consists of four parallel feedback elements. The previous maximum on-axis force is represented by a gray disk. Force exerted in a current trial is represented by the vertical position of a round yellow disk that is analogous to a face, the width and curvature of the face’s smile, and the size of the face. The metaphor is a balloon, as the child exerts force, the display adjusts in real time, with the face rising toward the target with higher force exertion. As the applied on-axis component approaches the previous maximum force, the vertical height of the yellow disk and the size of the smile increase. Forces above the previous maximum force are represented by an increase in the size of the yellow disk. During a trial, if the force drops, the yellow disk representing the face stays at the peak for the current trial, while a light-yellow disk continues to follow the current force values. No feedback is provided to the subject for the initial trial of a specific exertion task to determine an estimate for the initial maximum exertion force. The maximum of the subsequent trials is scaled to the previous best effort to elicit higher force exertions. The force feedback is displayed on a screen that can be adjusted to be in the child’s comfortable line of site for each condition.
Force Measurement
Much of the previous work on child strength has been conducted using uniaxial load cells. Our prior research has shown that people often generate task forces in different directions than requested, and these off-axis components can be substantial. For most tasks, we have designed our fixtures with load cells that measure forces and moments on three axes. For some exertions (knob twisting) the moments are of direct interest; in others, the moments allow compensation for different hand placements. For some tasks that are well defined by a single axis (e.g., two hand pull-apart; see Figure 2) a uniaxial load cell is used.
Data collection and filtering is also an important consideration. We are gathering data from all force/moment channels at 2 kHz. The relatively high frequency ensures that dynamic forces can be quantified. The force data are synchronized with the camera data used to document and quantify posture. We plan to retain the time-history data indefinitely to enable reanalysis using different methods and criteria.
Data Processing
The data from trials with young children are considerably more challenging to process and analyze than those from adults and older children who are able to follow instructions precisely. As noted above, video review is needed to characterize the postures to ensure that the force values were obtained in a valid trial. We have developed a software interface that allows the investigators to step through the data, viewing the synchronized video and force histories. The goal of the windowing is to identify the sequence of time within which forces were exerted within the parameters defining a valid trial with respect to force direction and posture (e.g., the child must exert force independently with the requested hand posture (one vs. two hands) and at least one foot in contact with the floor) (Figure 7). These time windows are then used for computing strength measures and associated statistics. As with posture, validation criteria are applied in selecting exertions for subsequent analysis. For example, the range and standard deviation of the forces within a moving one-second window can be used to exclude trials with excessive force variability. However, for some applications short-duration forces may be of interest, highlighting the need to retain the time-series data. For most exertions, the maximum across trials of the average value exerted over a short time window on the requested axis will be most compatible with values from prior studies. Other measures, such as the actual force magnitude, considering off-axis forces, will also be valuable data to quantify child force-exertion capability.

Data verification and window selection for a two-handed push exertion task.
Discussion
This paper discusses considerations for the design of a study to measure strength of children ages 24 to 71 months. Considerations were derived from a thorough review of the literature, experience with strength measurement of adults, and an iterative approach including pilot work. Study design considerations included: safety, laboratory layout, task selection and definition, interfaces, postures and tactics, task scaling, motivation and feedback, force measurements and data processing. All these factors need to be considered in the development of valid, repeatable, and reproducible data collection protocols that will produce applicable data. Ultimately, the resulting methodology and data gathered using this protocol will improve the safety of products children encounter.
Footnotes
Acknowledgements
This project has been funded with federal funds from the United States Consumer Product Safety Commission under contract number 61320618D0004. The content of this publication does not necessarily reflect the views of the Commission, nor does mention of trade names, commercial products, or organizations imply endorsement by the Commission. We thank our collaborators at CPSC as well as the many UMTRI staff who have assisted with this work.