
Abstract
Study Design
Retrospective cohort study.
Objectives
We aimed to identify factors associated with mortality and morbidity in geriatric patients with complete cervical spinal cord injury (cSCI) and compare outcomes to middle-aged patients using national trauma data.
Methods
We conducted a retrospective cohort study of 1147 patients aged ≥40 with complete cSCI from the 2019-2021 American College of Surgeons Trauma Quality Program. Patients were grouped as middle-aged (40-69 years, n = 798) or geriatric (≥70 years, n = 349). Those with severe head trauma or pre-admission death were excluded. Outcomes included in-hospital mortality, complications, intensive care unit (ICU) length of stay, and ventilator duration. Multivariate logistic and linear regression models assessed factors associated with each outcome.
Results
Geriatric patients had significantly higher mortality (60.7%) compared to middle-aged patients (23.2%, P < 0.001). Surgical management was associated with reduced mortality in both groups (OR 0.2, P < 0.001) but was less frequently performed in geriatric patients (59.9% vs 81.0%, P < 0.001). Complications were more common in middle-aged patients (47.6% vs 36.4%, P < 0.001), with surgery predicting increased complication risk. Geriatric patients had shorter ICU stays (11.2 vs 17.0 days, P < 0.001) and ventilator duration (11.6 vs 18.1 days, P < 0.001).
Conclusions
Geriatric patients with complete cSCI had higher mortality and were less likely to undergo surgery, despite its association with improved survival. Lower morbidity in this group may reflect earlier mortality or less aggressive care. Individualized surgical decision-making is essential to ensure equitable treatment for older patients.
Introduction
Cervical spinal cord injuries (cSCI) are the most common form of spinal trauma and can result in life-changing neurological impairment.1-3 These injuries, involving the C1-C7 spinal levels, cause varying degrees of motor and sensory loss depending on severity and location.4,5 Traumatic causes of cSCI, such as motor vehicle accidents, falls, sports injuries, and assaults, typically involve force mechanisms like flexion, extension, and translation of the spine resulting in contusion or compression of the spinal cord.4,6 Complete cSCI, classified as American Spinal Injury Association Impairment Scale (AIS) Grade A, is the most severe form and leads to total loss of motor and sensory function below the injury level with no sacral sparing. 5 This leads to profound disability, often tetraplegia, with high complication risk, mortality, and costs.7-9
Historically, cSCI has been most common in younger males due to high-energy trauma, but recent trends show a growing incidence in older adults, largely driven by an aging population and high incidence of falls among the elderly.10,11 Geriatric patients who sustain cSCI tend to have higher rates of mortality and morbidity, as well as lower rates of surgical intervention, often attributed to age-related comorbidities and greater neurological severity.12,13 Understanding the unique challenges of geriatric cSCI is essential to improving outcomes, there remains a paucity of research examining factors that influence outcomes in geriatric patients with complete cSCI.
To address this gap, we analyzed data from the American College of Surgeons (ACS) Trauma Quality Program (TQP) to identify factors associated with outcomes in patients aged 70 and older with complete cSCI, using middle-aged patients as a comparison group. Through this national retrospective analysis, we aim to elucidate the relationships between demographic and clinical factors and key inpatient outcomes, including mortality and morbidity, to inform clinical decision-making and guide future research in this high-risk population.
Methods
The ACS TQP database was used to identify patients with complete cSCI from 2019 to 2021. This database includes detailed demographic, clinical, and outcome data at the national level across all trauma center levels, including those without accreditation. This study analyzes deidentified patient data and was deemed exempt from institutional review board approval. The study followed STROBE guidelines. 14
Patients aged ≥40 with complete cSCI, identified by International Classification of Diseases, 10th Revision (ICD-10) codes S14.11 and S14.111-S14.119, were included if hospital discharge outcomes were documented. Patients who died before hospital admission or had a head trauma AIS score of 3 or higher were excluded to control for concomitant severe traumatic brain injury (TBI). Missing demographic and clinical data were coded as “unknown.”
The analysis included a wide range of predictor variables across demographic, injury, emergency department (ED), procedural, and diagnostic domains. Demographics included age, sex, race, and insurance type. Injury-related data captured ICD-10 external cause codes and protective device use. ED data included initial vitals, oxygen levels, and discharge status. Hospital procedures and diagnoses were identified using ICD-10 codes, along with Injury Severity Scores (ISS). Injury level, osseoligamentous injury type, and soft tissue injury type were determined using AIS codes associated with complete cSCI.15,16 The primary outcome was inpatient mortality, determined by discharge disposition. Secondary outcomes included respiratory, cardiovascular, infectious, and pressure-related complications, as well as ICU length of stay and duration of mechanical ventilation.
Statistical Analysis
Patient characteristics were summarized with means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Patients were divided into middle-aged (40-69) and geriatric (≥70) cohorts, consistent with prior spine trauma research. This age categorization of geriatric patients aligns with previous research examining prognostic factors in lumbar spine trauma. 17 Comparisons between the middle-aged and geriatric groups were evaluated using Student’s t-test for continuous data and Pearson’s chi-square test for categorical data, with Fisher’s exact test employed when cell counts were fewer than 5. Multivariate logistic regression identified predictors of inpatient mortality and complications, while linear regression assessed ICU LOS and ventilator duration. For linear regression models, results are presented as unstandardized regression coefficients (B), representing the expected change in the outcome per unit change in each predictor. All models were adjusted for relevant demographic and clinical confounders to enhance the robustness of the findings, with results reported as odds ratios (OR) or mean changes with 95% confidence intervals (CI). All analyses were conducted using Python 3.7 and a P-value threshold of <0.05 was used to determine statistical significance.
Results
Patient Demographics and Injury Characteristics
Demographic and Clinical Characteristics of 1147 Middle-Aged and Geriatric Patients Admitted to the Hospital Following Complete cSCI
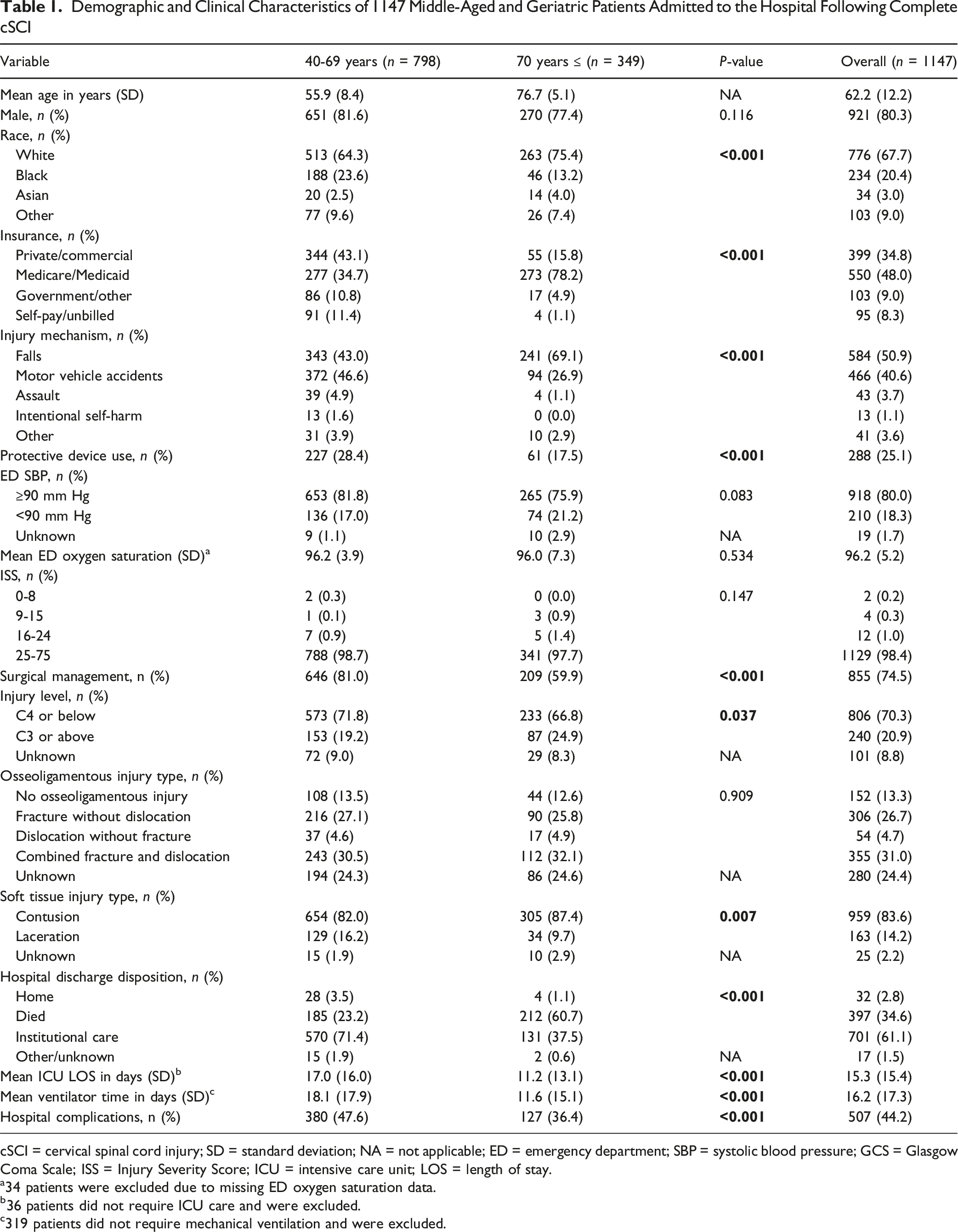
cSCI = cervical spinal cord injury; SD = standard deviation; NA = not applicable; ED = emergency department; SBP = systolic blood pressure; GCS = Glasgow Coma Scale; ISS = Injury Severity Score; ICU = intensive care unit; LOS = length of stay.
a34 patients were excluded due to missing ED oxygen saturation data.
b36 patients did not require ICU care and were excluded.
c319 patients did not require mechanical ventilation and were excluded.
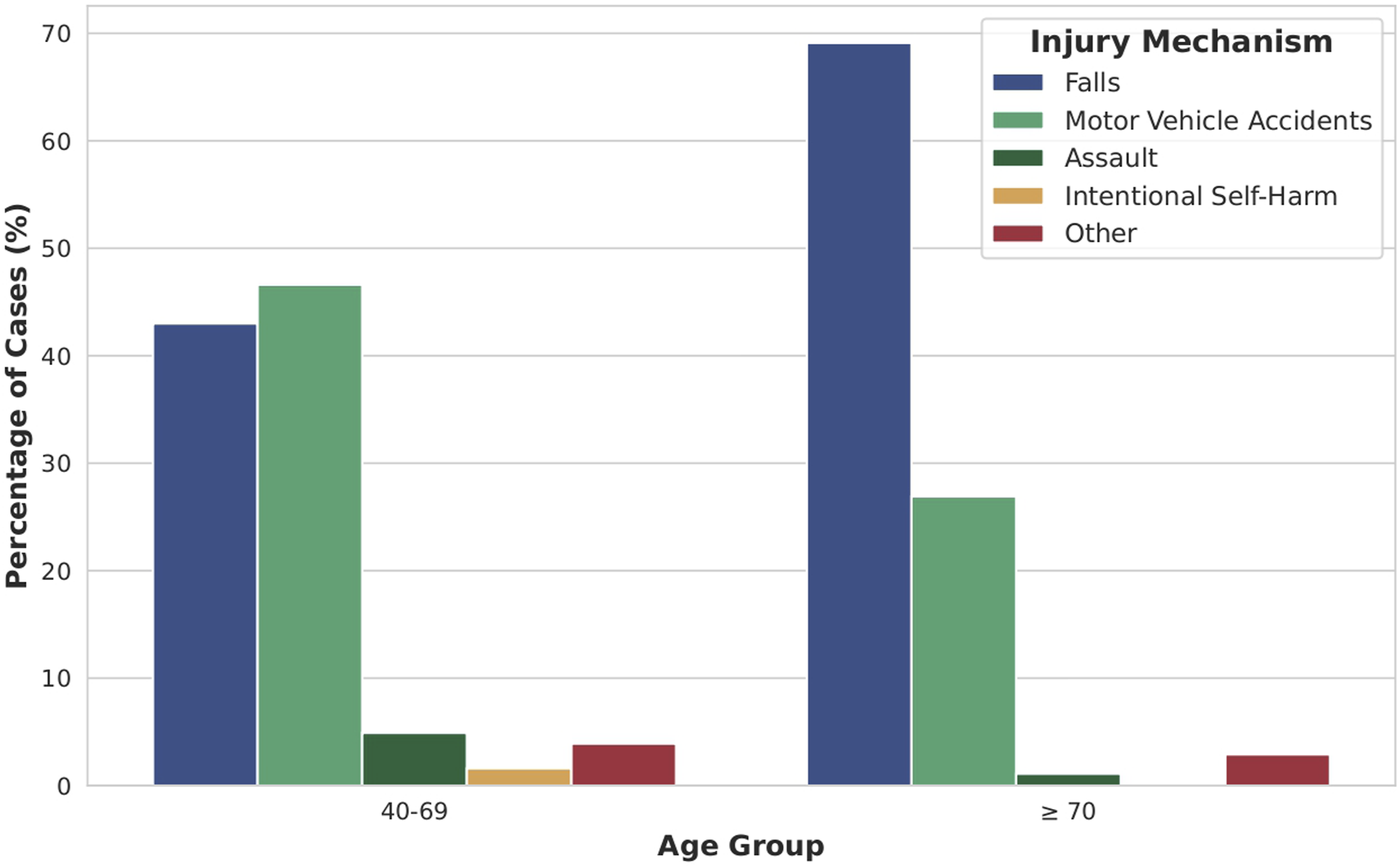
Distribution of Injury Mechanisms in Middle-Aged and Geriatric Patients With Complete Cervical Spinal Cord Injury
Clinically, 80.0% of patients had a systolic BP ≥90 mm Hg, with no significant age-group difference (P = 0.083). Most patients (98.4%) had severe injuries (ISS 25-75). Geriatric patients underwent surgery less often than middle-aged patients (59.9% vs 81.0%, P < 0.001). Upper cervical injuries (C3 or above) were more frequent in geriatric patients (24.9% vs 19.2%, P = 0.037). Combined fracture and dislocation was the most common osseoligamentous injury (31.0%). Contusions were more common in geriatric patients (87.4% vs 82.0%, P = 0.007), while lacerations were more frequent in the middle-aged group (16.2% vs 9.7%). Soft-tissue injury type reflects local cord morphology rather than external trauma mechanism and is included for additional context across age groups. Injury distributions by age are shown in Figure 2. Distribution of (A) Injury Levels, (B) Osseoligamentous Injury Types, and (C) Soft Tissue Injury Types in Middle-Aged and Geriatric Patients With Complete Cervical Spinal Cord Injury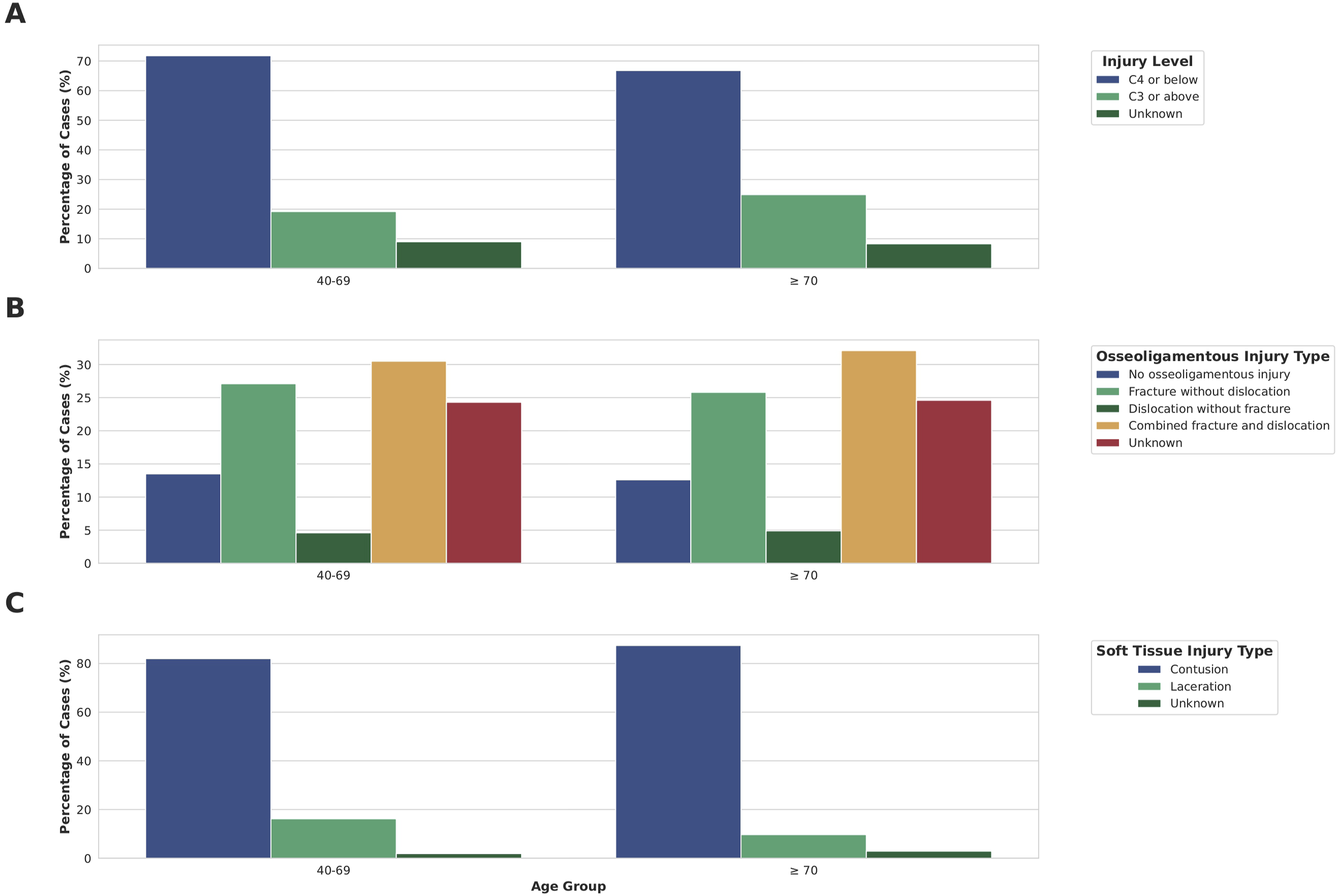
Inpatient Mortality and Complications
Overall inpatient mortality was 34.6%, significantly higher in geriatric patients (60.7%) than in middle-aged patients (23.2%, P < 0.001) (Figure 3). Multivariate analysis showed surgical management significantly reduced mortality in both groups (OR 0.2, P < 0.001) (Table 2). Injuries at C3 or above were associated with increased mortality (geriatric: OR 1.9, P = 0.047; middle-aged: OR 1.9, P = 0.002), while non-White race was linked to lower mortality in both groups (geriatric: OR 0.4, P = 0.002; middle-aged: OR 0.6, P = 0.004). Other variables, including hypotension and osseoligamentous injury, were not significantly associated with mortality. Discharge Outcomes of Middle-Aged and Geriatric Patients With Complete Cervical Spinal Cord Injury Multivariable Logistic Regression of Predictors of In-Hospital Mortality and Complications Following Admission for Complete cSCI by Adult Age Group
a
cSCI = cervical spinal cord injury; CI = confidence interval; ED = emergency department; SBP = systolic blood pressure; GCS = Glasgow Coma Scale. aAll 1147 patients were included in these analyses.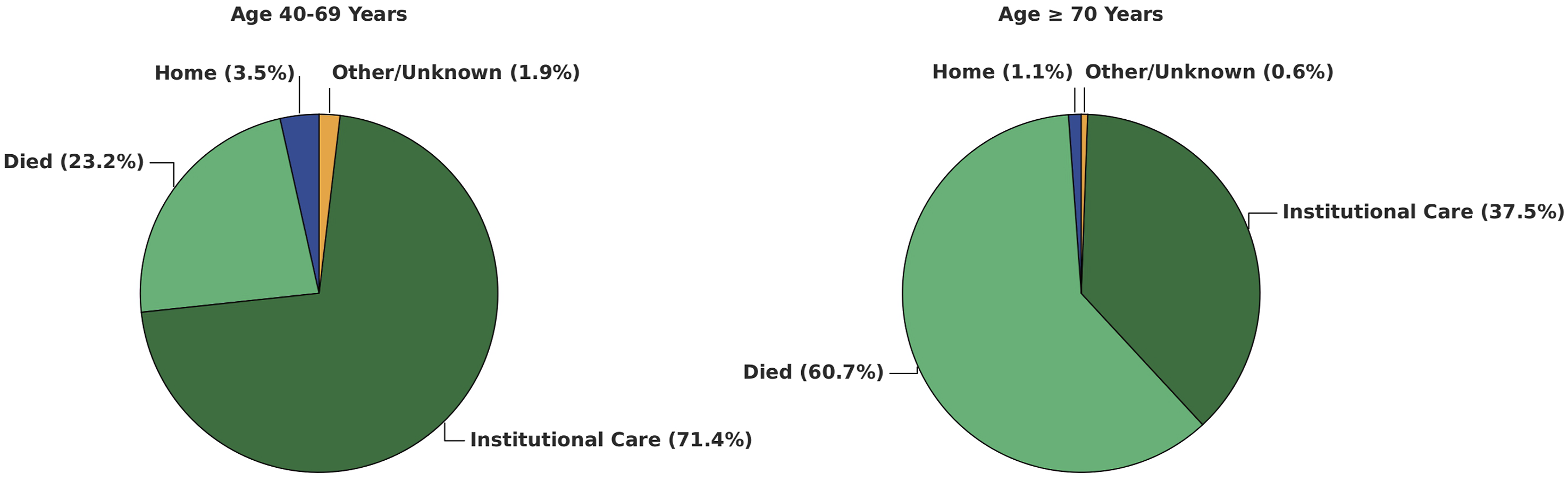
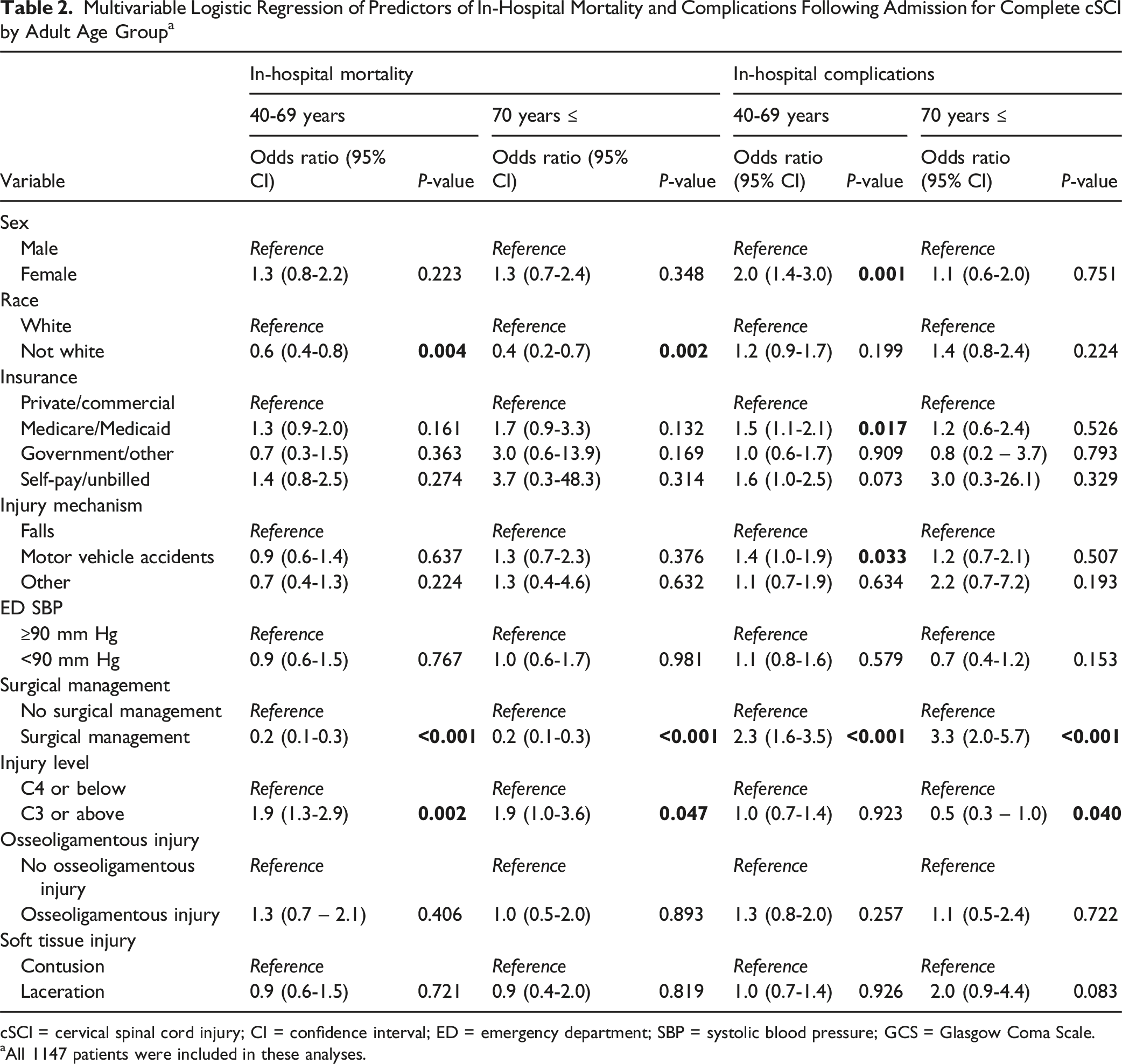
Complications occurred in 44.2% of patients, more frequently in the middle-aged group (47.6%) than in geriatric patients (36.4%, P < 0.001). In geriatric patients, the most common complications were unplanned intubation (15.5%), ICU admission (8.6%), and pressure ulcers (6.3%), while middle-aged patients most frequently experienced pressure ulcers (15.3%), unplanned intubation (14.0%), and cardiac arrest (12.2%). Surgical management increased complication risk in both age groups (geriatric: OR 3.3; middle-aged: OR 2.3; both P < 0.001) (Table 2). In middle-aged patients, female sex (OR 2.0, P = 0.001), Medicare/Medicaid (OR 1.5, P = 0.017), and motor vehicle accidents (OR 1.4, P = 0.033) were associated with increased complications. These associations were not observed in the geriatric group. Injury at C3 or above was associated with reduced complication risk in geriatric patients (OR 0.5, P = 0.040), with no effect in middle-aged patients.
ICU LOS and Ventilator Time
Multivariable Linear Regression of Predictors of ICU LOS Following Admission for Complete cSCI by Adult Age Group a
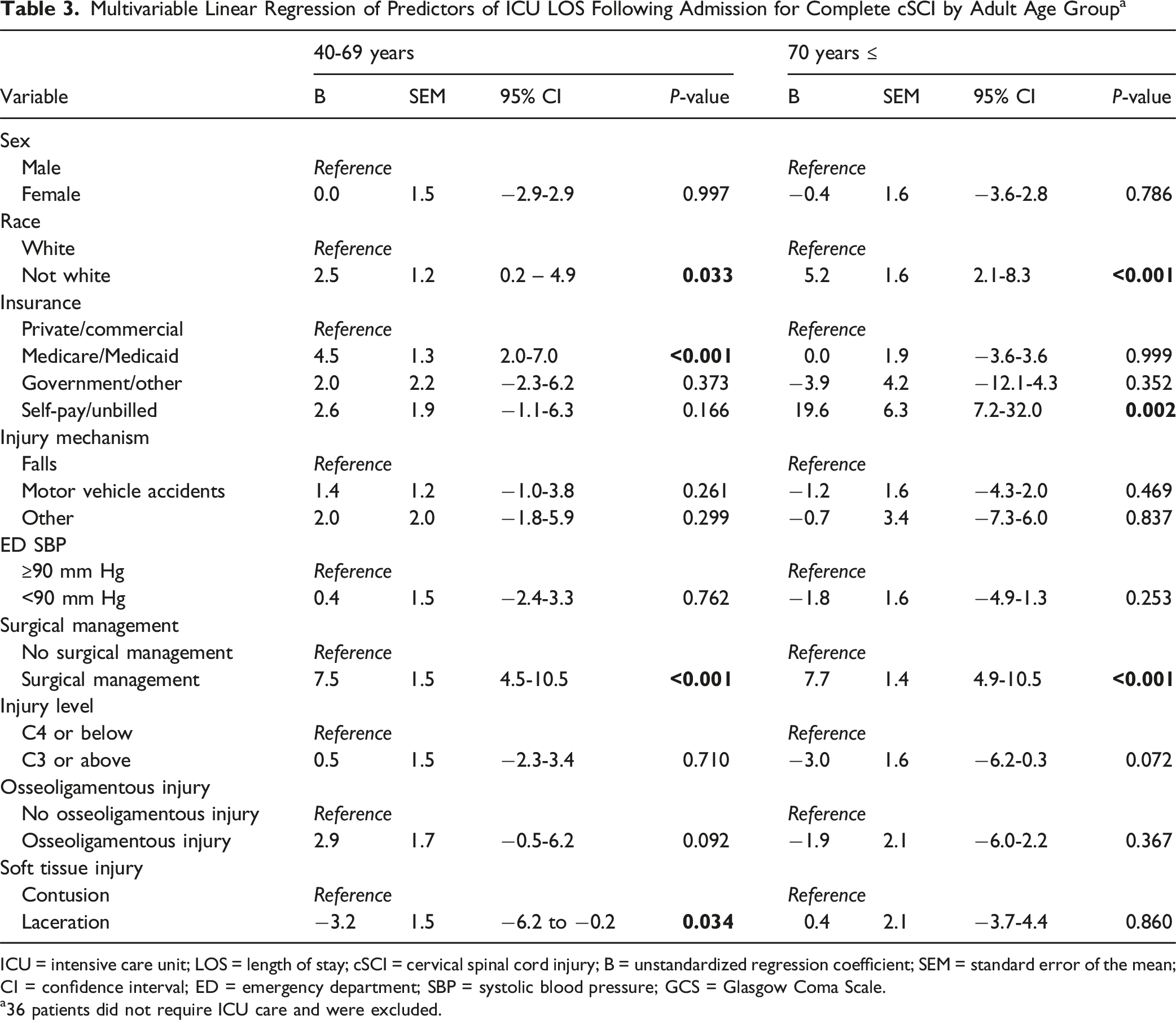
ICU = intensive care unit; LOS = length of stay; cSCI = cervical spinal cord injury; B = unstandardized regression coefficient; SEM = standard error of the mean; CI = confidence interval; ED = emergency department; SBP = systolic blood pressure; GCS = Glasgow Coma Scale.
a36 patients did not require ICU care and were excluded.
Multivariable Linear Regression of Predictors of Days on a Ventilator Following Admission for Complete cSCI by Adult Age Group a
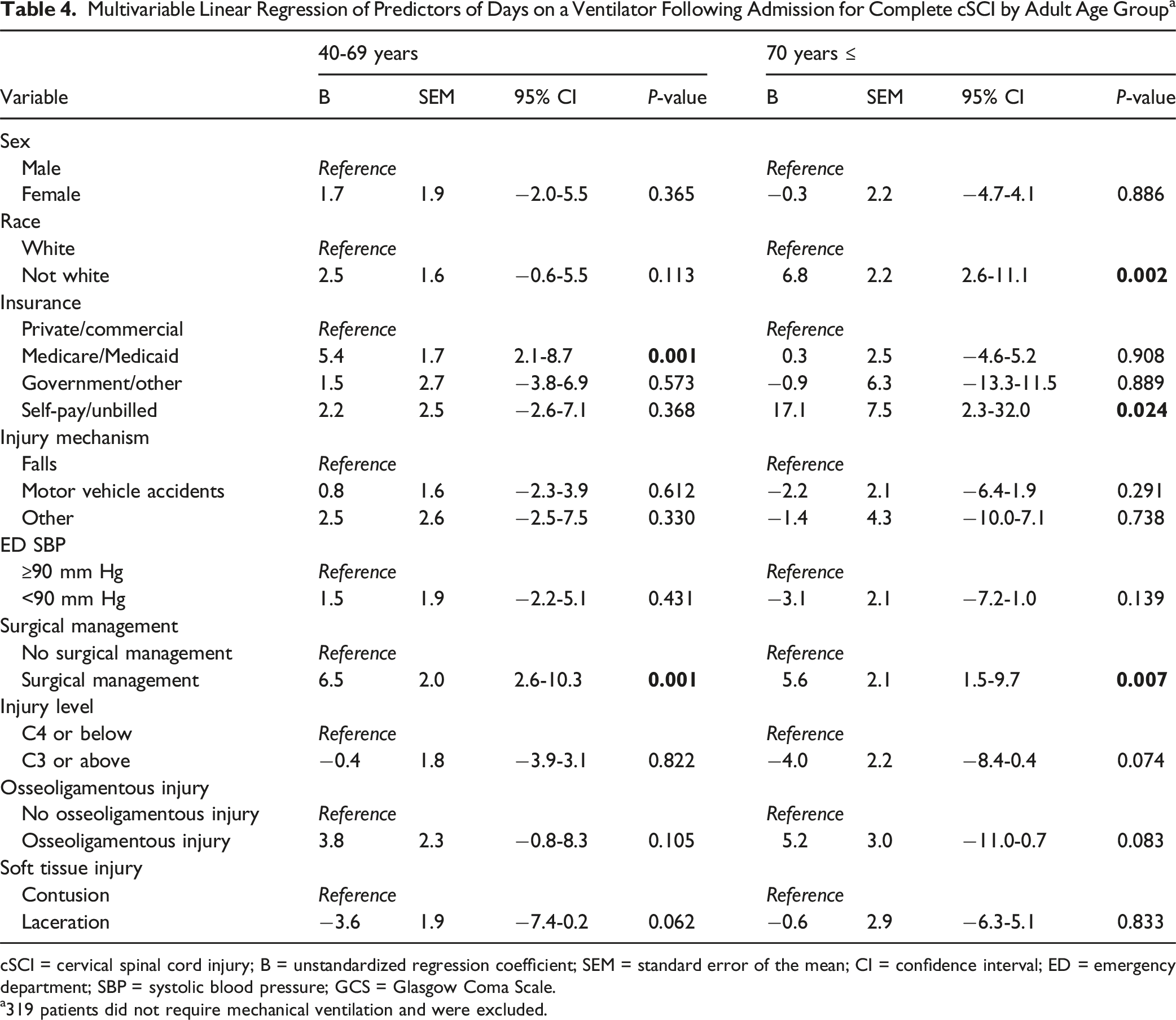
cSCI = cervical spinal cord injury; B = unstandardized regression coefficient; SEM = standard error of the mean; CI = confidence interval; ED = emergency department; SBP = systolic blood pressure; GCS = Glasgow Coma Scale.
a319 patients did not require mechanical ventilation and were excluded.
Discussion
Complete cSCI is a highly debilitating injury with substantial mortality, especially among geriatric patients, yet large-scale studies in this population are limited. While incomplete cSCI has been more extensively studied, complete injuries are often underrepresented, reducing statistical power. Prognostic analysis of mortality and morbidity is further challenged by the frequent presence of severe head trauma, particularly in high-impact mechanisms like motor vehicle accidents. 18 Recent research has highlighted the unique complexities of craniospinal injuries, especially those involving the upper cervical spine, which are associated with prolonged ICU stays and increased mortality. 19 To address these confounders, we excluded patients with severe TBI to better isolate the impact of cSCI. Using a nationally representative dataset from 2019-2021, this study is the first to comprehensively evaluate demographic, injury-related, and outcome predictors in geriatric patients with complete cSCI.
Age and Complete cSCI
Falls were the leading cause of complete cSCI in geriatric patients, while middle-aged patients had a more even distribution between falls and motor vehicle accidents. This aligns with prior studies linking falls in the elderly to functional decline and osteoporosis. 20 These lower-energy mechanisms likely explain the higher rate of contusions in geriatric patients, whereas middle-aged patients more often sustained lacerations from high-impact trauma. Similarly, a higher incidence of C3 and above injuries in geriatric patients compared to younger individuals has been reported in smaller cohorts, likely due to degenerative osseous changes that relatively reduce mobility in the C4-C7 segments in the elderly. 20 Additionally, the geriatric group had more White patients and higher Medicare coverage, factors that may influence healthcare access and outcomes.
Mortality and Complete cSCI
We observed markedly higher inpatient mortality in geriatric patients with complete cSCI (60.7%) compared to middle-aged patients (23.2%). Reported mortality in older adults ranges from 20% to 100%, influenced by surgery and comorbidities, while younger patients typically show lower rates (10%-37.5%).13,21-23 Despite lower mortality in the middle-aged group, 71.4% required institutional care, and home discharge was rare across both groups, highlighting the substantial morbidity of complete cSCI and a common outcome of either institutionalization or death. This contrasts with incomplete cSCI, where home discharge is more frequent regardless of age. 24
While our study offers valuable insights into cSCI mortality in both geriatric and middle-aged patients, it is important to interpret these findings as associations rather than causal relationships. Both age groups demonstrated similar mortality associations, with surgical management strongly linked to reduced mortality, highlighting its potential benefits even in older patients. A recent meta-analysis emphasized the role of early (<24 hours) surgical decompression in improving outcomes for complete cervical spinal cord injury, though previous studies found no such link for incomplete injuries (AIS B-D).8,13 Despite this, geriatric patients were significantly less likely to undergo surgery, possibly due to perceived risks related to age, frailty, and comorbidities, which make both surgery and recovery more challenging. 21 Additionally, patients selected for surgery may have had less complex cases, contributing to better outcomes. Given these findings, we recommend an individualized approach that evaluates the benefits of surgery for each geriatric patient, ensuring that viable candidates receive equitable surgical consideration comparable to their younger counterparts. Future studies incorporating physiologic and anesthetic risk factors are needed to better understand surgical decision-making in this population.
In addition to surgical management, injury level emerged as a critical predictor in both age groups. Our findings are consistent with previous studies showing that complete cSCI at or above the C3 level is linked to higher mortality, largely due to compromised diaphragm and intercostal muscle function, which leads to respiratory failure.25,26 Also, Lomoschitz et al. demonstrated that older adults, particularly those over 75 and injured from standing-height falls, were more prone to upper cervical injuries. 20 However, the impact of injury level on mortality remains debated, especially in geriatrics, with possible influence from factors like tracheostomy use.24,25 Additionally, non-White patients had lower mortality odds in both groups, contrasting with prior findings in the general cSCI population and highlighting a gap in research on older cohorts.27,28
Morbidity and Complete cSCI
Complications were common in both groups but occurred more frequently in middle-aged patients (47.6%) than geriatric patients (36.4%), possibly due to higher early mortality in the latter limiting the time for complications to develop. Prior studies have shown mixed findings regarding age and complication rates, and few have focused specifically on complete cSCI.29,30 The lower complication rate in geriatrics may also reflect more conservative management, as surgery, more common in the middle-aged group, was associated with higher complication odds, potentially due to greater baseline severity and prolonged recovery. Although C3 or higher injuries in geriatric patients were associated with fewer recorded complications, this likely reflects early mortality and reduced opportunity for complications to develop rather than a true protective relationship. Further research is needed to clarify factors associated with of specific complications in this population.
Geriatric patients had significantly shorter ICU stays (11.2 vs 17.0 days) and ventilator times (11.6 vs 18.1 days) than middle-aged patients, possibly reflecting more conservative care, earlier palliative transitions, or limitations due to frailty. 23 These shorter durations may also be influenced by differences in goals of care, including higher rates of do-not-resuscitate orders and earlier transition to comfort-focused management rather than improved physiological recovery. 31 While some studies report comparable ICU stays across age groups, longer durations have been noted in complete vs incomplete cSCI.23,30 Surgical management was linked to increased ICU and ventilator time in both cohorts, likely due to postoperative demands and injury severity. Additionally, non-White race and self-pay status were significant predictors of longer ICU stays and ventilator time in geriatric patients, suggesting disparities in access to care or variations in treatment practices.27,28
Limitations
A key limitation of our study is the lack of functional neurological outcomes, limiting the assessment of the long-term impact of complete cSCI. We highly recommend that national trauma databases, such as the ACS TQP, include functional neurological outcomes for spinal cord injuries to facilitate more comprehensive analyses in the future. Another limitation is that patients with complete cSCI who died before reaching the ED were not captured in the database, potentially leading to an underestimation of the true incidence and mortality of complete cSCI. Additionally, patients who were not hospitalized, including those who died in the emergency department, were excluded due to insufficient outcome data. The use of a national database limited access to detailed surgical information, such as procedure timing and type, preventing analysis of how specific surgical approaches may have impacted outcomes. This data source also confined our evaluation to in-hospital outcomes, without the ability to assess long-term recovery, functional status, or quality of life. Furthermore, excluding patients with severe head trauma (AIS score ≤3) may limit the generalizability of our findings, as many patients with spinal cord injuries also present with concomitant traumatic brain injuries. Lastly, it is crucial to interpret the associations found in this study as observational rather than causal. Despite these limitations, our results offer valuable insights into complete cSCI in geriatric patients. Future studies should aim to address these limitations by analyzing long-term disability and the impact of concomitant head injuries.
Conclusions
In both middle-aged and geriatric complete cSCI, surgical management was associated with reduced mortality. However, geriatric patients were significantly less likely to undergo surgery and had markedly higher mortality. This likely contributed to their shorter ICU stays and fewer recorded complications, which may reflect early mortality and less aggressive care rather than better outcomes. An individualized approach is needed to ensure viable geriatric candidates receive equitable surgical consideration similar to that offered to younger patients. Falls played a prominent role in geriatric cases, potentially contributing to a higher prevalence of upper cervical injuries and contusion injuries. Racial disparities and insurance type appeared to influence access to care and outcomes. Prospective studies are needed to refine surgical decision-making frameworks and explore the long-term impacts of surgical intervention in this vulnerable population.
Footnotes
Ethical Considerations
This study analyzes deidentified patient data from the American College of Surgeons Trauma Quality Program and was deemed exempt from review by the Icahn School of Medicine at Mount Sinai Institutional Review Board. IRB approval number: 22-01302.
Author Contributions
Conceptualization, SI, MK, and KM; Methodology, SI, MK, and KM; Software, SI; Formal Analysis, SI; Data Curation, SI; Writing – Original Draft Preparation, SI and PM; Writing – Review & Editing, SI, MK, PM, and KM; Visualization, SI; Supervision, KM; Project Administration, SI, MK, and KM.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Statement by ACS
The American College of Surgeons Trauma Quality Program and the hospitals participating in the ACS-TQP are the source of the data used herein; they have not been verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.