
Abstract
Study Design
Cadaveric Biomechanical Study.
Objectives
Surgical treatment for adult spinal degeneration revolves around posterior instrumented fusion. Proximal junctional kyphosis (PJK) is a well-documented complication of this surgical treatment and theorized to occur due to excessive mobility at the proximal non-fused segments. The goal of this study was to identify whether increasing rod correction into greater lordosis correlates with a higher degree of mobility at proximal spinal levels.
Methods
Seven, native cadaveric human spines (T9-sacrum) were instrumented with bilateral pedicle screws posteriorly from T12 to sacrum. Native spines were maneuvered to determine the sagittal plane intervertebral range of motion (ROM). The spines were then instrumented with rods three times to achieve increasing levels of lordotic correction, and the same ROM tests were conducted. Flexion-Extension (FE) torque and adjacent level intervertebral flexion/extension rotations were measured.
Results
Significant decreases in Cobb Angle between corrections were measured. Max Flexion Torque increased significantly with increasing correction. The proximal spinal levels saw increased Max Flexion ROM and decreased Max Extension ROM as a function of correction. The FE ROM of the proximal spinal levels increased compared to the Native condition but sequentially decreased slightly with increased correction.
Conclusions
This study indicates that, while increasing lordotic correction does not increase total proximal spinal mobility, it does change its distribution. This segmental motion distribution change implies that additional flexion mobility is introduced to adjacent spinal levels as a correction increased. Future work will explore how to better quantify risk factors intraoperatively for increased adjacent segment mobility to better prevent PJK.
Keywords
Introduction
The prevalence of degenerative spinal disease continues to rise due to an aging general population. 1 Spinal degenerative changes can lead to significant loss of function and independence for patients due to neural compression, debilitating pain, and spinal deformity. 2 After non-operative treatments for symptom management have been exhausted, patients require surgery to decompress, stabilize, and correct spinal deformities. Surgery for adult spinal deformity almost universally involves posterior instrumented thoracolumbar fusions with potential osteotomies, fusion to the sacrum, thoracoplasties, and supplemental anterior fusion to restore physiologic sagittal and coronal balance. These surgeries are morbid procedures, associated with a high potential rate of complication and revisions.3-6
Proximal junctional kyphosis (PJK) is a well-known complication following long-segment posteriorly instrumented thoracolumbar fusions where a kyphotic deformity progresses anteriorly in the sagittal plane proximal to the most superiorly fused segment also known as the uppermost instrumented vertebrae (UIV).7-9 It is defined as a sagittal plane Cobb Angle greater than ten degrees and must be at least ten degrees higher than the preoperative sagittal Cobb Angle. 10 While PJK can represent a radiographic abnormality that is minimally symptomatic, a portion of patients suffering from PJK also present with proximal junctional failure (PJF) which is a more symptomatic and critical form of PJK associated with severe pain, neurologic compromise, instability, and hardware failure.11-13 Furthermore, the presence of PJK in all its forms has been correlated with worse Scoliosis Research Society pain scores. 14 Literature reports the incidence of PJK and PJF to range from 17% to 39% and 5.6% to 40%, respectively.11-15 The large variability in the incidence most likely stems from the relatively vague definition of PJK and PJF. Instead of being classified as two distinct entities, PJK and PJF may be treated as different points on a spectrum of proximal junctional pathology.16,17
There is no known study in the literature that has identified a consistent etiology for the development of PJK. Several modifiable and non-modifiable risk factors have been described in the literature including age greater than 55, a degree of preoperative sagittal imbalance, pedicle screw fixation, low bone mineral density, fusion to the sacrum, combined anterior-posterior fixation approaches, and magnitude of deformity correction.18-20 Rigid fixation is hypothesized to cause PJK due to the dramatic difference in stiffness between the fused and non-fused spinal segments. It is theorized that the proximal non-fused spinal segments are exposed to pathologic levels of motion accelerating adjacent-level degeneration.21-23 In a biomechanical model comparing several spinal constructs with varying upper segment stiffness and assessing proximal mobility changes, Metzger et al 24 found that supralaminar hooks at the superior level of construct eased the stiffness transition resulting in smaller increases in motion compared to rigid superior level fixation, a concept known as “soft landing”.
Excessive mobility at the cranial adjacent mobile segment has been biomechanically established as a proxy for adjacent segment degeneration and eventual PJK.24-27 The establishment of this relationship not only allows for further study of PJK but can give insight into the development of adjacent segment pathology. Rigid fixation has been shown to cause excessive mobility proximal to a posterior spinal fusion,21-23 but the influence of varying rod correction on proximal mobility is unexplored. Therefore, the goal of this study was to assess the influence of varying lordotic correction of the thoracolumbar spine on proximal spinal level mobility in human cadaveric spines as human cadaveric models have been established as a tool for the assessment of mobility as a proxy for adjacent segment degeneration.25-28 The hypothesis was that increasing rod correction generates a higher degree of mobility at spinal levels proximal to the construct. Answering this clinical question may inform strategies for optimizing rod correction to minimize the risk of proximal junctional kyphosis and enhance long-term patient outcomes following spinal deformity surgery.
Methods
Specimen Preparation
Seven fresh, frozen cadaveric human spines (5 male & 2 female) from T9 to sacrum without ribs were utilized in this study. The cadaveric spines were on average 63 ± 14 years old at death and had a mean BMI of 37 ± 6 kg/m2. Cadaveric spines with prior spine surgery, cancer with bony metastases, osteoporosis, osteopenia, spinal deformities, under 18 or over 80, scoliosis, and/or spinal fractures were excluded. Each specimen was dissected to remove all non-ligamentous soft tissue while preserving the vertebral bodies, discs, facet joint capsules, and ligamentous soft tissues.24-31 The superior (T9) and inferior (sacrum) portions of the specimen were each potted in a custom clamp system consisting of pedicle screws, wood screws, and Wood’s metal, a low-boiling point metal utilized to rigidly capture the portions of the spine within the clamps. The clamp system allowed for repeatable placement of the specimen within the testing system. Each spine was instrumented with bilateral pedicle screws posteriorly from T12 to the sacrum to later secure posterior rod constructs. Specimens were frozen at −20°C until dissection and testing.
Biomechanical Testing Setup
A simVITRO® robotic testing system (Cleveland Clinic, Cleveland, OH) consisting of a KR16 robot (Kuka, Ausburg, Germany) and a Delta 6-axis load cell with a SI-330-30 calibration (ATI, Apex, NC) were utilized to apply motions and loads to the spines throughout testing. Each spine was rigidly attached to the test system at its superior (T9) and inferior (sacrum) aspects. Motion tracking markers (Optotrak, Northern Digital Inc, Waterloo, Canada) were secured to T10, T11, and T12 to track the relative motion between various spinal segments (Figure 1). Robotic Experimental Set-Up. Human Cadaver Spine (T9-Sacrum) Mounted to the Testing Robot, With Motion Tracking Markers Attached to T10, T11, and T12 Vertebral Bodies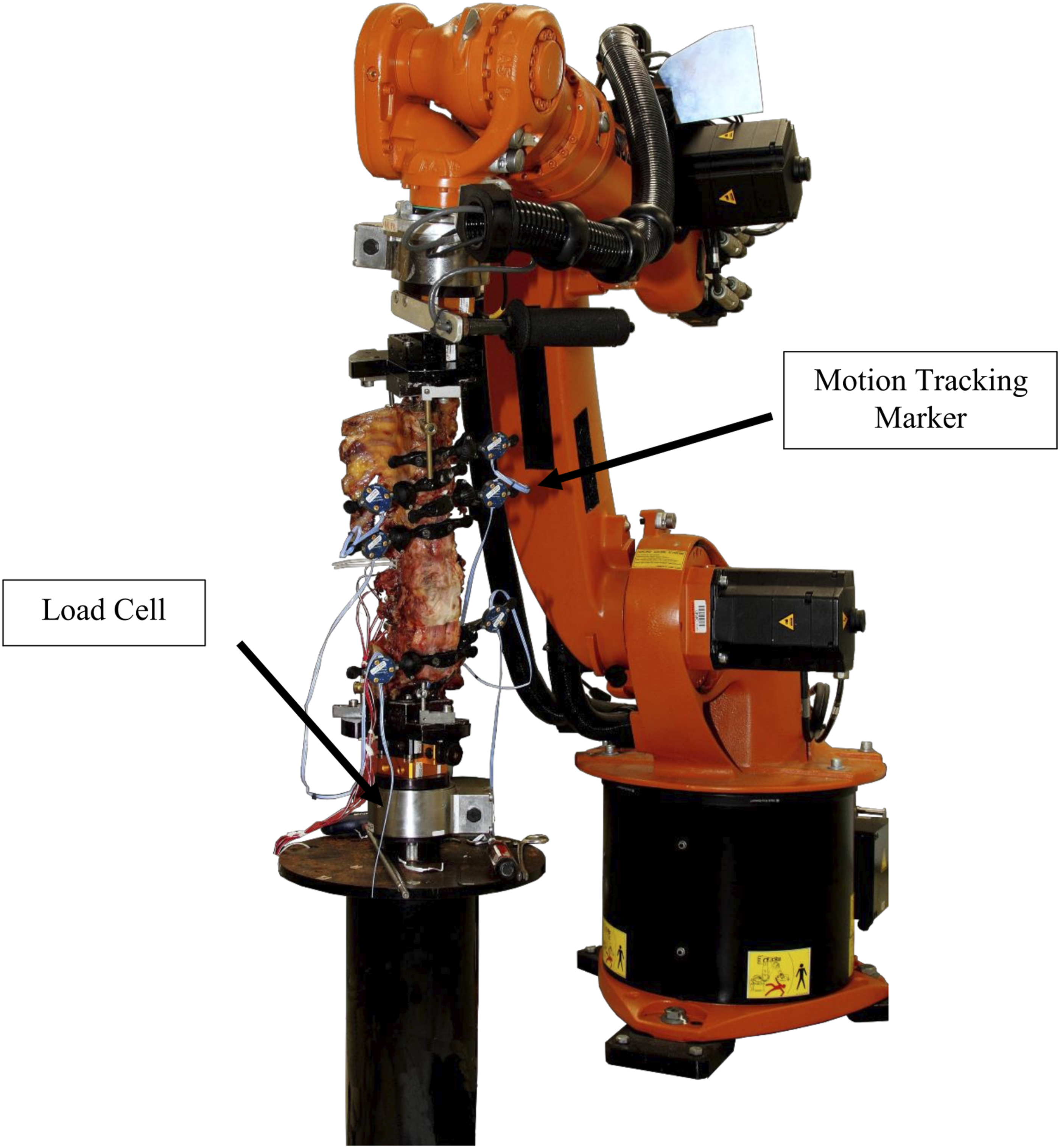
The spatial relationships between the robot, vertebral bodies, and load cell were established using a digitizer outfitted with motion tracking markers. Coordinate systems on the pertinent vertebral bodies were generated according to Techy et al 32 to allow real time force feedback control as a function of the robot’s end effector and the 6-axis load cell measurements. The Global spine range of motion (ROM) was measured based on the robot’s end effector position but transformed to consist of the motion between T9 and the sacrum. Intervertebral ROM was measured as a function of relative motion capture marker positions transformed into clinically meaningful coordinate systems and decomposed per International Society of Biomechanics standards for reporting spine kinematics. 33
The native Neutral Position was established for each specimen to relate motions measured during testing to a neutral pose. The Neutral Position was identified by commanding the robot to find a zero-load position of the spine that best represented a standing neutral posture. Insight from the clinical team was utilized to confirm the spine’s orientation as the Neutral Position.
Surgical Conditions
Four surgical conditions were tested during this study. The first condition was Native (Figure 2) where the specimen was tested with the T12 to sacrum pedicle screws instrumented but no posterior rods. This condition was collected as baseline for each specimen to compare against the corrected conditions. Before rod instrumentation, the spine was returned to the Native Neutral Position. While mounted to the robot, a left and right rod were manually bent by a neurosurgery resident using rod benders to match the contours of the spine at the Native Neutral Position with a slight lordotic correction. The condition with these rods instrumented to the T12-sacrum pedicle screws was called Correction 1 (Figure 2). After instrumentation, the specimen was offloaded, the Neutral Position for the surgical condition was measured, and the specimen was then tested. After testing Condition 1, the rods were taken off the spine and bent with rod benders to increase the degree of the lordosis. The entire length of rod was adjusted between tests at the resident’s discretion. After bending, the rods were reconnected to the existing pedicle screws, and the surgical condition after rod bending was called Correction 2 (Figure 2). The Neutral Position of Correction 2 was quantified and the specimen was again tested. This cycle was conducted one additional time for Correction 3 (Figure 2), where the degree of lordotic correction of the rods was again increased from Correction 2. Specimen Posterior Instrumentation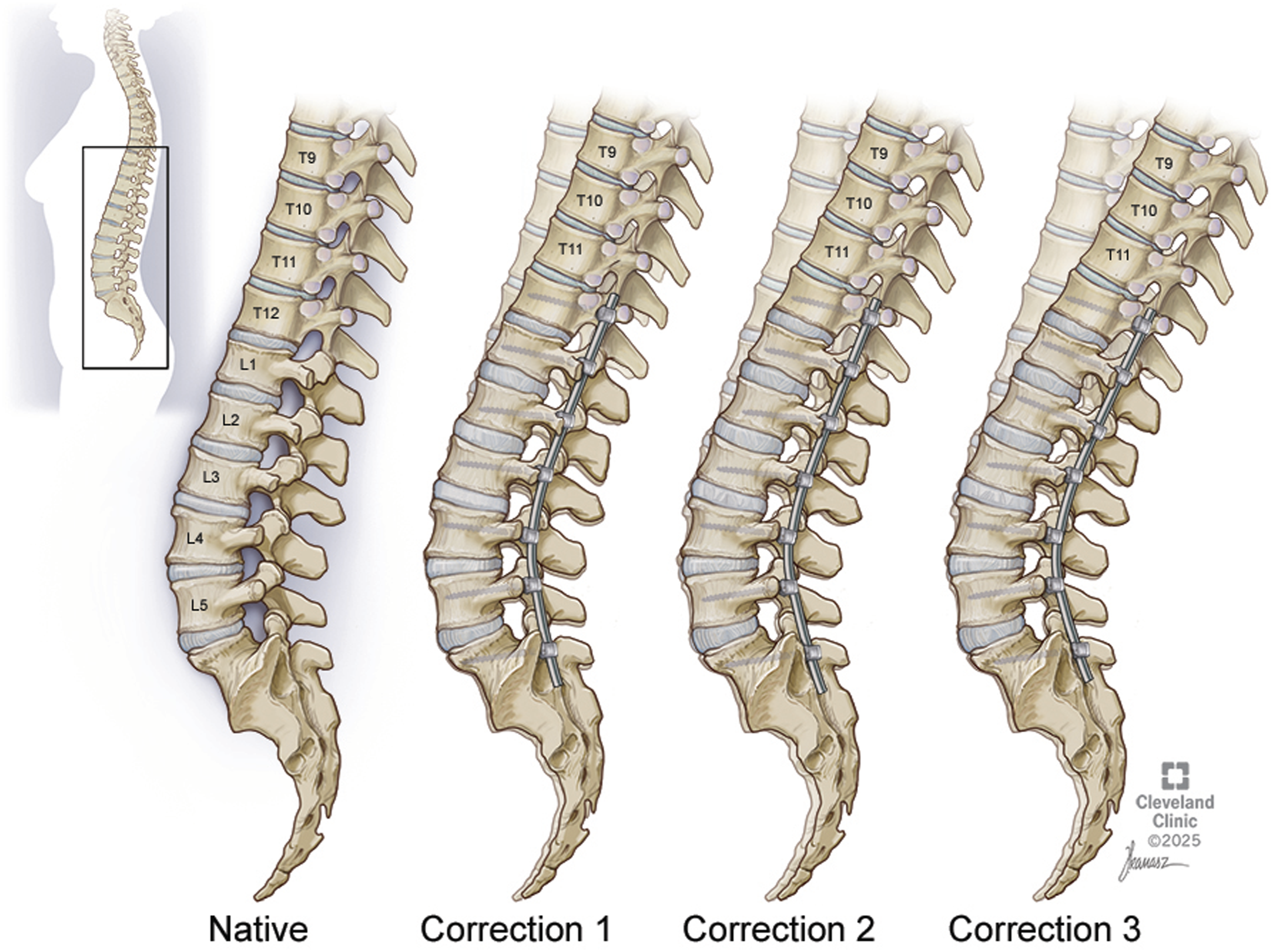
Testing
All Native specimens were subjected to three preconditioning sinusoidal cycles of Flexion-Extension (FE), Lateral Bending (LB), and Axial Rotation (AR) at an applied moment of ±1.5 Nm with all off-axis forces or torques minimized.
The hybrid test protocol developed by Panjabi et al was used to determine the adjacent level motion for each construct pattern.26-28 The protocol was a two-part process. The first part of the hybrid process was only conducted on the Native spine. First, multidirectional flexibility tests were conducted on Native specimens by applying ±1.5 Nm of pure-moment loading to determine the resulting Global ROM endpoints for FE, LB, and AR under load control. From the resulting Global ROM endpoints, rotational traces in the primary degree-of-freedom (DOF) were recorded.
Second, for all surgical conditions (including Native), the robotic system executed the recorded rotational traces in the primary DOF in kinematic control while minimizing off-axis loads (ie, for the Flexion-Extension commands, the FE direction was controlled kinematically and driven along the FE kinematic trace while the AR and LB torques and all other forces were minimized).
Biomechanical Metrics
In this study, only the data collected from the Global FE ROM endpoints were analyzed for all surgical conditions. Due to the human variability introduced through manual rod bending, five metrics were collected to quantify the amount of rod correction throughout the testing conditions. These metrics included the 1. Neutral Position for each surgical condition in the sagittal plane for the Global spine (T9 to sacrum), T10-T11, and T11-T12. The Neutral Position of the Global spine was defined as Cobb Angle.
Four FE torque values were used as secondary metrics to quantify correction. 2. Max Flexion Torque is defined as the torque in the sagittal plane at maximum flexion rotation. 3. Max Extension Torque is the torque in the sagittal plane at maximum extension rotation. 4. Torque Range is the sum of the Max Flexion and Extension Torques. The 5. Torque Ratio was defined as the ratio of Max Flexion Torque to Max Extension Torque.
Four ROM metrics of the Global spine, T10-T11, and T11-T12 were obtained throughout testing to quantify kinematic changes between each correction. 6. Max Flexion ROM was defined as the maximum flexion rotation with respect to the native Neutral Position. 7. Max Extension ROM was defined as the maximum extension rotation with respect to the native Neutral Position. 8. FE ROM was defined as the sum of the Max Flexion and Extension ROMs. 9. ROM Ratio was defined as the ratio of Max Flexion ROM to Max Extension ROM.
Statistical Analysis
The Friedman-Rank test was used to evaluate the relationship between the three correction levels and the nine biomechanical metrics described previously. Confidence intervals of 95% were generated based on pooled estimates of error variance across corrections. Assumptions of equal variances were all confirmed via Levene’s test. Comparisons between corrections among the specimens tested were performed using the Friedman-Rank test, a non-parametric test akin to the Wilcoxon Rank sum test, but for dependent data to account for multiple corrections on the same cadaveric specimens. Comparisons were made between corrections, but not with the Native state.
To evaluate the relationship between the correction metrics and spine mobility metrics, Cobb Angle, Max Flexion Torque, Max Flexion ROM, and Max Extension ROM were all normalized as the percentage difference between their values at Correction 1 and subsequent corrections. The normalized differences in Max Flexion or Extension ROM were compared relative to normalized differences in Cobb Angle or Max Flexion Torque. Linear regression equations were fit to identify any trends in the data. The relative importance of regression equations was quantified by calculating R2 values.
Results
This study investigated the influence of increased lordotic correction of posterior instrumentation on adjacent and overall spinal segment range of motion to identify potential risk factors for PJK development.
Figure 3 illustrates the relationship between Neutral Position and correction. As each specimen was increasingly corrected into greater lordosis, Cobb Angle moved significantly towards extension (P = 0.0058). With respect to T11-T12, increasing correction led to a statistically significant transition of the Neutral Position farther into flexion (P = 0.0058). T10-T11 Neutral Position followed a similar trend as T11-T12 with greater correction, but did not differ significantly between corrections (P = 0.1561). Neutral Position as a Function of Correction. The Relative Change in Neutral Position Relative to the Native Neutral Position as a Function of Correction for Cobb Angle, T11-T12, and T10-T11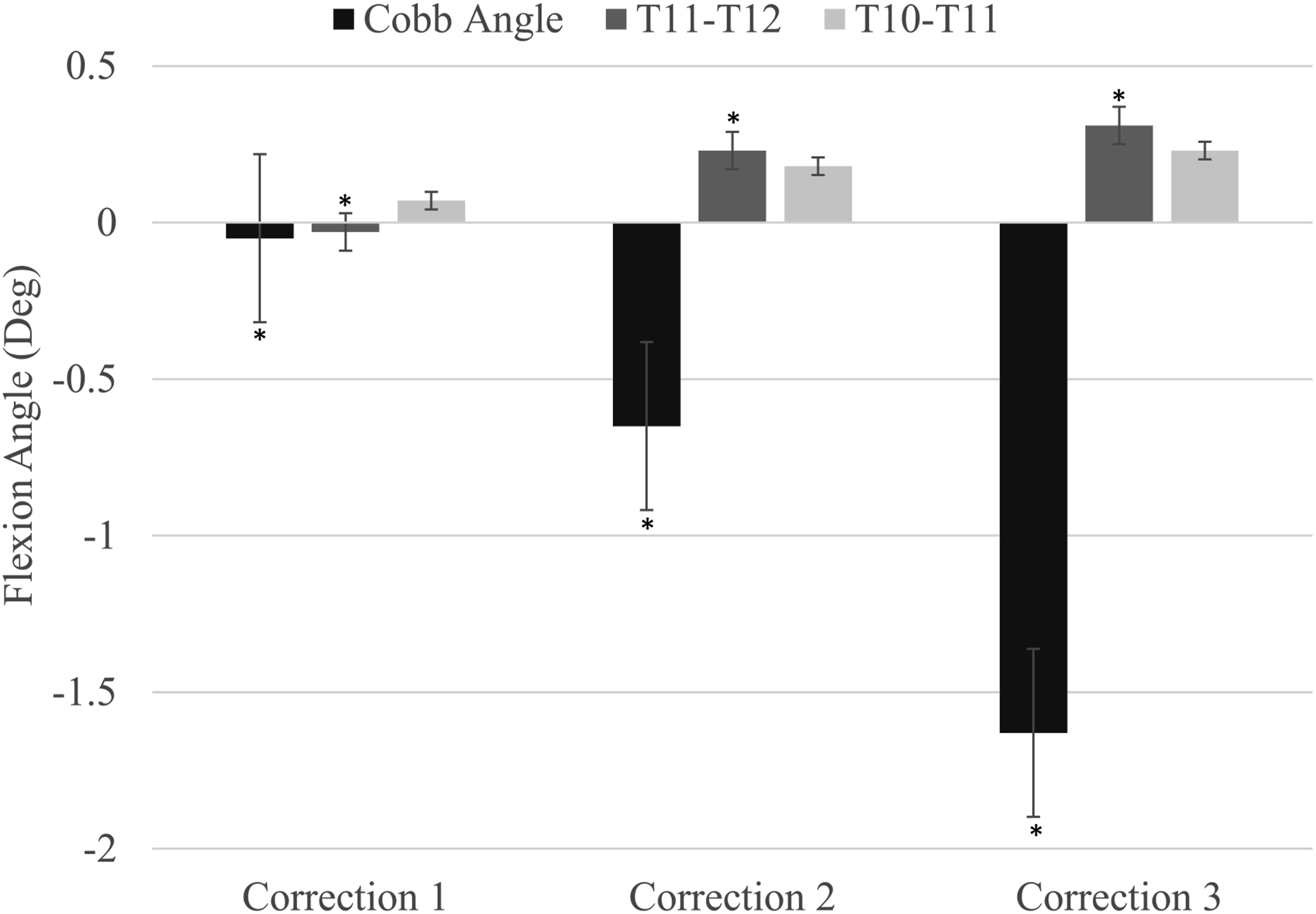
Figure 4 illustrates the relationship between torque and correction. Increased correction correlated with magnitude changes in applied torque. As correction moved the specimens into greater lordosis, Max Flexion Torque significantly increased (P = 0.0021) and Max Extension Torque significantly decreased (P = 0.0009). These torque changes accompanied a statistically increasing Torque Ratio (P = 0.0009). The Torque Range (not displayed in Figure 4) did not change significantly across the correction levels (P = 0.3679). Average With 95% Confidence Interval of Max Flexion Torque, Max Extension Torque and Torque Ratio as a Function of Correction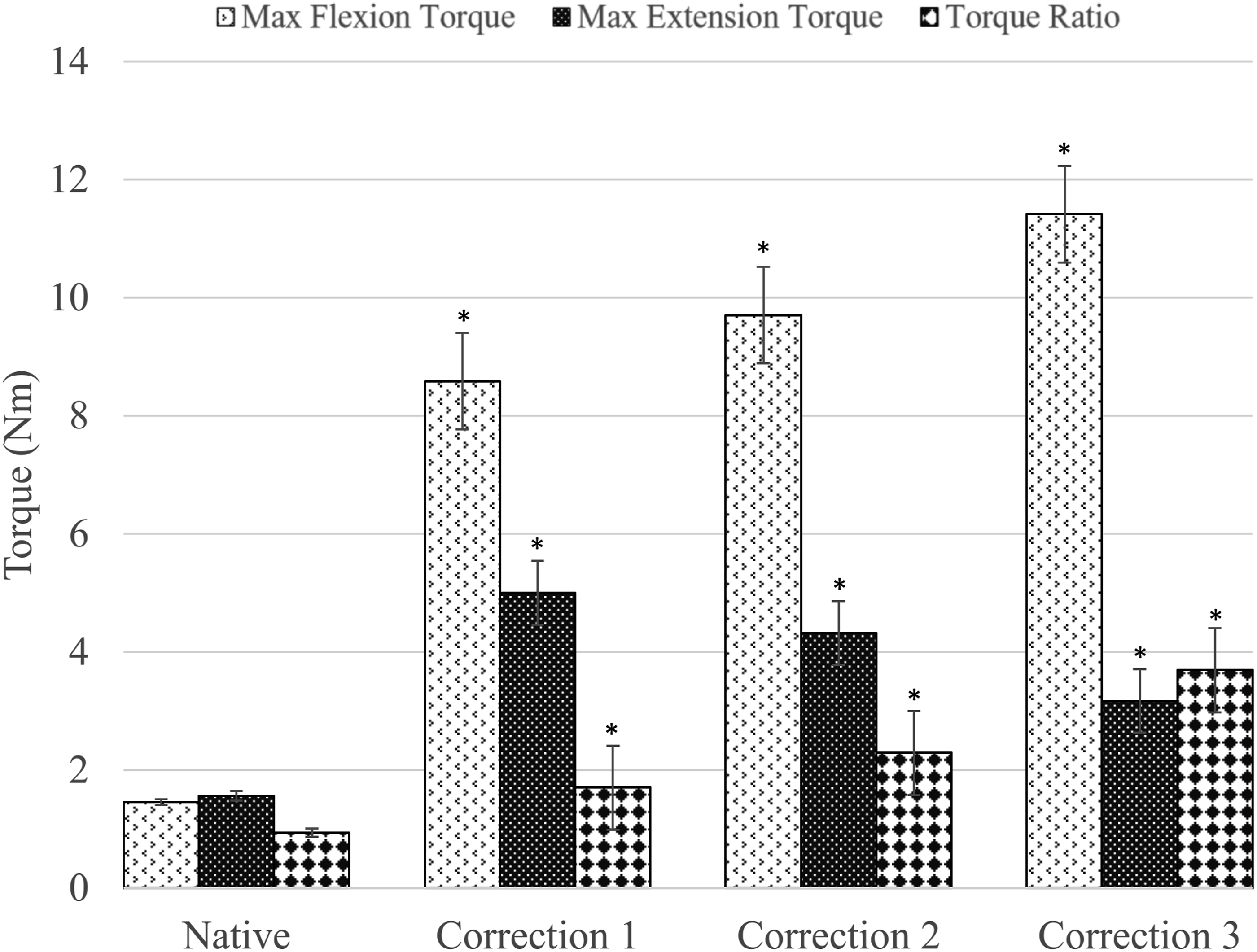
Association of ROM With Correction
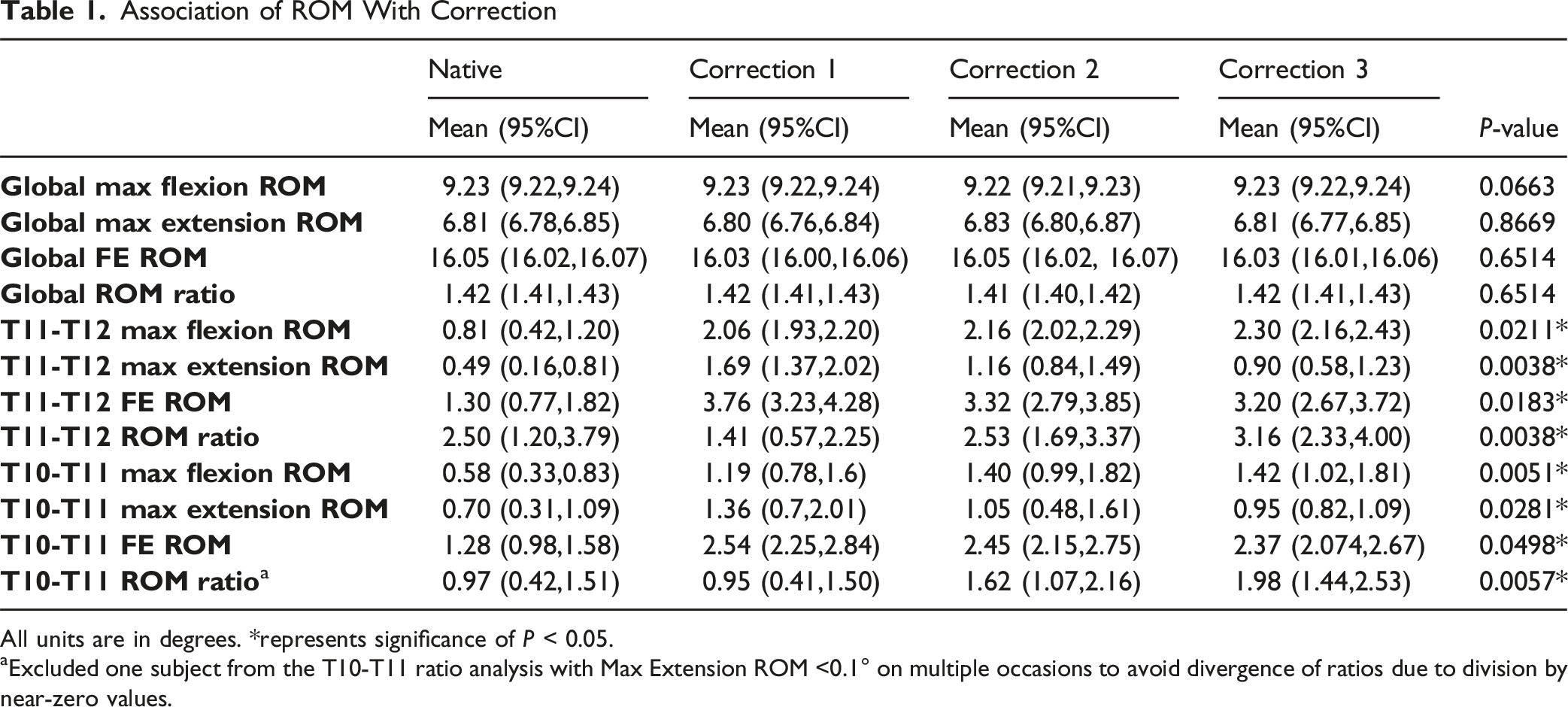
All units are in degrees. *represents significance of P < 0.05.
aExcluded one subject from the T10-T11 ratio analysis with Max Extension ROM <0.1° on multiple occasions to avoid divergence of ratios due to division by near-zero values.
Spine Mobility as a Function of Correction
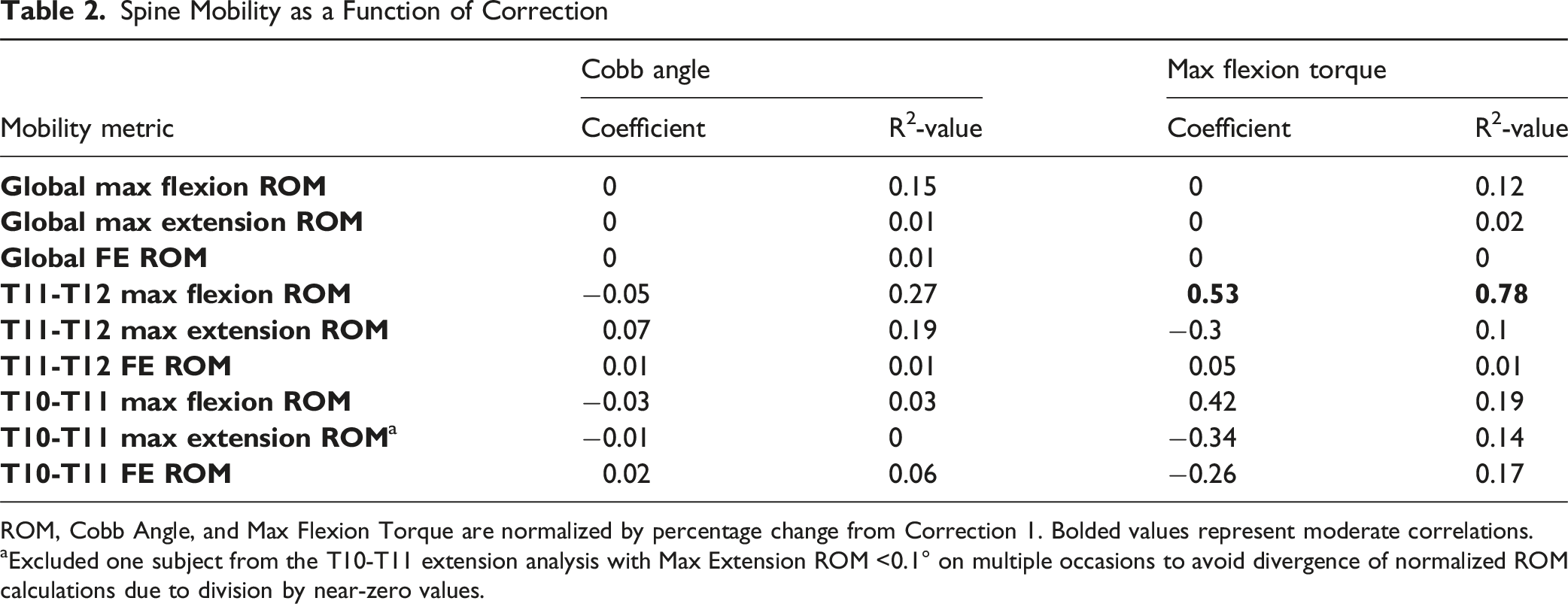
ROM, Cobb Angle, and Max Flexion Torque are normalized by percentage change from Correction 1. Bolded values represent moderate correlations.
aExcluded one subject from the T10-T11 extension analysis with Max Extension ROM <0.1° on multiple occasions to avoid divergence of normalized ROM calculations due to division by near-zero values.
Discussion
This study identified three key relationships between correction level, spinal mobility, and torque on the spine: (1) The Neutral Position of the total spine and supra-adjacent levels moved in opposite directions as a function of correction, (2) the distribution of applied torque changed as a function of correction, and (3) the distribution of spinal mobility changed as a function of correction. These findings validate that the degree of correction is a potentially important contributor to the incidence of PJK and PJF.
Neutral Positions Changed Antagonistically as a Function of Correction
Cobb Angle transitioned into greater extension as correction increased (Figure 3). To compensate for the global spine moving into extension, the Neutral Positions at the levels adjacent to the construct became increasingly flexed between corrections. Moreover, the supra-adjacent level to the construct (T11-T12) was more affected than the other adjacent level (T10-T11) based on its proximity to the construct. The antagonistic relationship between Cobb Angle and adjacent level Neutral Positions as a function of correction predisposes proximal spinal levels to potentially pathologic orientations as correction becomes more lordotic, serving as an indicator for possible development of PJK.
Generally, while increasing correction significantly changed mobility (Table 1), our regression models found little correlation between mobility, Cobb Angle, and Max Flexion Torque (Table 2). In the case of Cobb Angle, the lack of a correlation may be caused by many ‘neutral’ positions that the vertebra between the construct and the robot end effector (T12-T9) might occupy. The many ‘neutral’ positions could create a large force-neutral zone, which might add noise to the Cobb Angle metric which is based on the robot end effector position.
The Distribution of Applied Torque Changed as a Function of Correction
While Torque Range did not significantly change with correction, the distribution of torque was significantly affected by correction (Figure 4). As the spine was corrected into greater lordosis, the two components of Torque Range diverged with Max Flexion Torque increasing significantly and Max Extension Torque decreasing significantly.
Outside of the change in torque distribution across corrections, the torque values themselves indicate the likelihood of PJK. After instrumentation, the Max Flexion Torque increased by approximately 600%, Max Extension Torque increased by 300%, and Torque Range increased by 500%. This is somewhat obvious because it takes greater torque to move an instrumented spine through the same FE ROM as the Native condition. If a patient were to move their spine through the same Global FE ROM after surgery, the rods would provide greater resistance to that motion than the Native spine.
More interestingly, Max Flexion Torque continued increasing with correction, and by Correction 3 was approximately 800% higher than in the Native condition. Each level of the spine is subject to identical torque, and while the rods absorb a majority of that torque at instrumented levels of the spine, the biological structures at the adjacent levels must resist the entire torque. Therefore, the torque results in Figure 4 indicate that (1) the onset of PJK might be related to the increase in torque in addition to mobility and (2) increasing lordotic correction may increase the likelihood of PJK due to increases in Max Flexion Torque.
The Distribution of Spinal Mobility Changed as a Function of Correction
The results of this study are consistent with literature showing that the FE ROM of spinal levels proximal to the construct would significantly increase after instrumentation as lost motion at the fused levels is taken up at the adjacent levels (Table 1).21-23 The supra-adjacent level to the construct (T11-T12) had a 300% increase in FE ROM post-instrumentation while the superior level (T11-T10) had a 200% increase. This supports clinical observations that the supra-adjacent level to the construct is most likely to fail first after instrumentation.21-23
Global FE ROM did not change significantly between corrections, validating that spine motion remained unchanged between intact and instrumented spines and the Punjabi Hybrid Protocol was implemented correctly. Similar to the torque data, both T10-T11 and T11-T12 had increased Max Flexion ROM and decreased Max Extension ROM as a function of correction. The supra-adjacent level Max Flexion ROM increased 300% while the Max Extension ROM decreased 200% between Correction 1 and 3. This implies that a sagittal imbalance develops with increasing correction and the biological structures that resist Flexion ROM are stressed more than the structures that resist Extension ROM. FE ROM also decreased with correction at both adjacent levels. Though the cause of this decrease is unclear, it seems likely that the fused portion of the spine took on greater motion as the Max Flexion Torque increased. One mechanical reason for this could be that the pedicle screw bone interface might loosen at high flexion torques because there is a lack of healing and osseointegration in cadaveric specimens.
The key takeaway from the adjacent level ROM data is that Max Flexion ROM increases with correction, and increased mobility has been previously correlated with the onset of PJK. Further, the supra-adjacent level to the construct is more at risk because it has greater mobility (Table 1).
Clinical Significance
Excessive mobility at the cranial adjacent mobile segment has been biomechanically established as a proxy for adjacent segment degeneration and eventual PJK.24-27 This study establishes that Max Flexion ROM at the cranial adjacent segment increased as a function of lordotic correction while Max Extension ROM decreased. This imbalance in the Flexion-Extension ROMs directly supports the clinical presentation of PJK, which is defined here as a sagittal plane Kyphotic deformity that occurs proximal to the superior fused segment.
Based on the collected results, even small Cobb Angle changes between corrections (mean change in Cobb Angle of only 1.6° between Correction 1 to 3) generated large Max Flexion Torques (increased 33% between Correction 1 and 3) and supra-adjacent level Max Flexion ROM (increased 12% between Correction 1 and 3) changes. This data provides evidence that methods, such as osteotomies, should be utilized to provide sagittal plane corrections as opposed to attempting to “pull” the spine to a pre contoured spine. This is especially true at the proximal terminus of the construct. The data reflects deformity surgery in the adult spine, which would be expected to have less overall flexibility. In practice, even 5-10 degree of overall sagittal correction by reducing the spine to the rod may result in greater mobility at the supradjacent disc and increased risk of PJK. Furthermore, taking into account the increased torque provided by screws with good osseointegration, healing, and segment remodeling in patients as opposed to cadaveric specimens, increased Max Flexion Torque and Max Flexion ROM could create substantial changes in the Neutral Position and FE ROM of the adjacent levels to the construct leading to PJK.
This study sheds light on the biomechanical consequences of rod-based correction on the pathophysiology and prevention of PJK, especially in those with intact ligamentous complexes. While the rate of clinically significant PJK may increase at larger changes in angle such as 10-20° in the proximal junctional angle, 34 our study shows a staggering 33% change in flexion torque in just a 1.6-degree change in Cobb Angle on average made through rod correction. These findings highlight the clinical implication of trying to reduce the spine to a rod to correct a sagittal plane deformity. The data supports indirectly the use of techniques such as osteotomies, limit reducing the rod to the spine, and ensuring the rods are connected to the screws at the termini of construct “in situ”. Attempting to reduce the cranial extent of a sagittal plane deformity to a pre contoured rod greatly increases the flexion torque of the adjacent level and risk of PJK.
The Max Flexion Torque linear regression provides some clues as to a path forward for quantifying how much correction is potentially pathologic. Cobb Angle did not have any correlation to spinal mobility across corrections. However, the changes in Max Flexion Torque were correlated with cranial adjacent mobility (ie, Max Flexion ROM, R2 = 0.78, Table 2). Unfortunately, using this metric to quantify cranial adjacent mobility in the OR would be impractical. A more practical means of quantifying potentially pathologic correction could be measuring the sagittal plane rotational change of the fused spinal segment relative to intact spinal segment. Future work could explore techniques for quantifying sagittal plane rotational change and its correlation with cranial adjacent mobility. If correlated, then sagittal plane rotational change could be measured intraoperatively to estimate the risk of a particular correction causing adjacent segment degeneration and eventual PJK.
Limitations
This study is not without limitations. (1) There was a lack of healing after instrumentation in the cadavers used. This lack of healing could increase the likelihood of loosening at the interface between the pedicle screws and vertebra because there was no osteointegration. (2) Our testing focuses on the passive structures of the spine and did not take into account active structures (muscle jacket forces, etc.) during experimentation. (3) There was no method used for bending rods precisely and in a repeatable manner. However, current surgical practice is to manually bend rods, and so this variability is reflective of the operating room.1,17,25,30 (4) The Panjabi hybrid loading protocol26-28 assumes that the post instrumentation FE ROM will be the same as the Native spine. There is no known data at the time of publication quantifying how much a patient’s FE ROM changes between the Native and instrumented conditions. A low torque of 1.5 Nm was used to approximate a reasonable FE ROM after instrumentation. (5) The testing conducted in this study utilized pure-moment testing to generate the kinematic traces for the Panjabi hybrid loading protocol, which may not fully explore motions associated with activities of daily living.
Conclusion
The goal of this study was to assess the effect of increasing lordotic correction on mobility at spinal levels proximal to the construct. As correction increased, flexion mobility at the proximal levels increased, extension mobility decreased, and Cobb Angle moved into extension. Correction level had a stronger effect on the supra-adjacent level than levels farther from the construct. The change in the distribution of proximal level spine mobility with even small changes in Cobb Angle implies that larger, more clinically representative Cobb Angle changes will produce larger mobility changes than in this study. The additional flexion mobility introduced by increasing correction may be pathologic and introduce notable strain on the proximal levels of the spine. Future work could explore the relationship between sagittal plane rotational changes of the fused spine and adjacent level mobility to better assess the risk of adjacent segment degeneration and eventual PJK.
Footnotes
Acknowledgments
The authors would like to acknowledge Swetha Sundar, MD for her assistance with specimen preparation.
Author Contributions
Callan Gillespie: Idea Conception, Experimental Design, Data Collection, Data Analysis, Clinical Significance, Project Supervision, Manuscript Writing, Manuscript Review. Jeremy Loss: Data Analysis, Clinical Significance, Manuscript Writing, Manuscript Review. Seth Meade: Statistical Analysis, Clinical Significance, Manuscript Writing. Robb Colbrunn: Experimental Design, Project Supervision. Jamie Sheehan: Manuscript Review. Michael Steinmetz: Idea Conception, Experimental Design, Clinical Significance, Project Supervision, Manuscript Review.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was awarded under Cleveland Clinic Grant RPC #252.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Authors C.G, J.L, and R.C. receive royalties from the sale of simVITRO systems. Author M.S. receives royalties from Globus and Elsvier as well as payment from Globus and Broadwater for speaking appearances.