
Abstract
Study Design
Retrospective Comparative Study.
Objectives
To evaluate Multi-Acquisition Variable-Resonance Image Combination Selective (MAVRIC-SL) versus conventional Short-Tau Inversion Recovery (STIR) sequences for metal artifact reduction and diagnostic capability in patients with lumbar titanium instrumentation.
Methods
84 patients with implants in lumbar spine (mean age 54.3 ± 14.7 years; 52.4% male), who underwent both STIR and MAVRIC-SL MRI at 1.5 T. A neuroradiologist and spine surgeon independently measured signal loss areas and evaluated geometric distortion and neural structure visibility using standardized scales. Statistical analysis included paired t-tests and Wilcoxon signed-rank tests with Bonferroni correction (P < 0.01).
Results
MAVRIC-SL reduced signal loss area by 39.1% compared to STIR (0.809 ± 0.205 cm2 vs 1.356 ± 0.266 cm2, P < 0.001, Cohen’s d = 2.04). Neural structure visibility showed substantial improvement: axial neural foramina (96.4% vs 0%), sagittal neural foramina (96.4% vs 7.1%), and sagittal spinal cord (98.8% vs 14.3%), all P < 0.001. Posterior vertebral border clarity improved from 33.3% to 94.0% (P < 0.001).
Conclusions
MAVRIC-SL provides superior metal artifact reduction and significantly improves neural structure visualization in lumbar spine instrumentation, with effect sizes among the largest reported in spine imaging studies. These improvements justify the longer acquisition time for symptomatic patients requiring detailed evaluation.
Keywords
Introduction
Magnetic resonance imaging (MRI) of the postoperative lumbar spine is challenging due to susceptibility artifacts from metallic implants, which cause signal loss, geometric distortion, and signal pile-up.1,2 These artifacts arise from magnetic field inhomogeneities and obscure critical structures and pathologies near implants. 3 The need for effective artifact reduction has grown with the rise in spinal instrumentation, with spinal fusion discharges increasing 137% from 1998 to 2008 and long construct fusions rising 141% from 2004 to 2014.4,5
Conventional MRI sequences like Fast Spin Echo (FSE) and Short-Tau Inversion Recovery (STIR) struggle with metal artifacts due to frequency encoding limitations. 3 Specialized techniques, including View Angle Tilting (VAT), Slice Encoding for Metal Artifact Correction (SEMAC), and Multi-Acquisition Variable-Resonance Image Combination (MAVRIC), mitigate these issues. 6 MAVRIC uses multiple spectral bins to capture shifted proton signals, reducing both in-plane and through-plane distortions.2,7
While MAVRIC has shown promise in joint arthroplasty imaging,8,9 its effectiveness in spine imaging is less studied. This is significant given the prevalence of spinal instrumentation and the need to evaluate complications like adjacent segment disease and neural compression. This study compares MAVRIC-SL with STIR sequences in postoperative lumbar spine MRI with titanium implants, hypothesizing that MAVRIC-SL will reduce artifacts and enhance visualization of neural structures, improving diagnostic confidence.
Methods
Study Design and Patient Population
This study is a retrospective analysis approved by our institutional review board (IRB) with approval number (ECR/34/Inst/KA/2013/RR-19), which waived the requirement for patient consent due to the use of anonymized clinical data, posing minimal risk to participants. We aimed to determine if MAVRIC-SL sequences provide superior diagnostic capability and image quality compared to conventional STIR sequences in postoperative spine patients with titanium implants. We consecutively reviewed records of 84 patients (44 males, 40 females; mean age 54.3 ± 14.7 years; BMI 26.7 ± 5.58) with titanium implants in lumbar spine between January 2024 and January 2025 and underwent MRI with both STIR and MAVRIC-SL sequences. All 84 patients had complete STIR and MAVRIC-SL imaging data and were included in the analysis. We restricted our study to lumbar spine patients to eliminate confounding from anatomical differences between spine regions.
Sample size was calculated based on available MAVRIC literature, as lumbar spine-specific effect sizes were not published at study initiation. Assuming a 40% reduction in signal loss (Cohen’s d = 0.6), 100 patients were required for 80% power (α = 0.01). Post-hoc power analysis revealed that our 84 lumbar patients provided >99% power to detect the observed effect size (Cohen’s d = 2.04).
Inclusion criteria were: (1) history of spine surgery with titanium implants (verified through surgical records and medical bills), (2) completion of both STIR and MAVRIC-SL scans in the same session, and (3) availability of complete medical records including symptoms and follow-up data. Exclusion criteria included: (1) severe motion artifacts rendering images unusable, (2) incomplete scans, (3) non-titanium implants (eg, stainless steel or cobalt-chromium, as confirmed by surgical records), and (4) standard MRI contraindications. No patients meeting inclusion criteria were excluded due to motion artifacts or incomplete sequences, indicating good tolerability of both imaging protocols.
MRI Protocol
All MRI examinations were performed on a GE Healthcare 1.5 T Signa scanner (GE Healthcare, Chicago, IL, USA) using a dedicated spine coil. A 1.5 T field strength was chosen due reduced artifact severity for titanium implants compared to 3T, as supported by Filli et al (2017). MAVRIC-SL was selected for comparison with conventional STIR sequences because our institution’s GE scanner is optimized for MAVRIC-SL, offering robust metal artifact reduction for titanium implants. Each patient underwent both STIR and MAVRIC-SL sequences during the same session, with identical slice positioning ensured by using anatomical landmarks (eg, vertebral body margins) and verified by the same technician and radiologist. Both sequences used a 2 mm slice thickness to balance high resolution for neural structure visualization with clinically feasible scan times, with axial and sagittal views acquired for direct comparison.
STIR Sequence Parameters
• TR/TE/TI: 3116/40/140 milliseconds • Slice thickness: 2 mm • Field of view: 28 × 28 cm • Matrix size: 200 × 200 • Number of excitations (NEX): 1 • Acquisition time: 1 minute 43 seconds (average)
MAVRIC-SL Sequence Parameters
• TR/TE: 4400/56 milliseconds • Slice thickness: 2 mm • Field of view: 28 × 28 cm • Matrix size: 200 × 200 • Number of excitations (NEX): 0.75 • Acquisition time: 6 minutes 23 seconds (average)
Sequence parameters were optimized for clinical use, with differences in TR/TE reflecting standard protocols for STIR (fat suppression) and MAVRIC-SL (metal artifact reduction). All images were anonymized and transferred to a picture archiving and communication system (PACS) for review.
Image Analysis
Quantitative Assessment
A neuroradiologist with 8 years of experience and a spine surgeon with 20 years of experience independently evaluated all images using standardized protocols. To minimize bias, images were presented randomly with a 4-week interval between reviews, and sequence labels were anonymized in PACS.
Quantitative measurements included. 1. 2.
Qualitative Assessment
The images were also evaluated for quality using standardized scales. The 3-point scales were chosen for simplicity and to capture gross differences in visibility and distortion, given the expected large effect of MAVRIC-SL on artifact reduction. 1. Geometric distortion along the posterior vertebral border (3-point scale): ○ 1: Clear (entire border visible) ○ 2: Partially unclear (some parts not visible) ○ 3: Obscured (most or all border not visible) 2. Image quality for neural structures (3-point scale): ○ 1: Good contrast (structure clear with strong tissue contrast) ○ 2: Blurred contrast (structure visible but less clear) ○ 3: Not visible (structure cannot be seen)
This assessment was performed for four key neural structures: axial neural foramen, axial spinal cord, sagittal neural foramen, and sagittal spinal cord. For reporting purposes in the Results section, structures receiving a score of 1 (good contrast, clearly visible) were classified as “visible,” while structures scoring 2 or 3 were classified as “not visible.” This binary classification was used because only structures with good contrast (score 1) provide diagnostically adequate visualization for clinical decision-making.
Disagreements between the two primary reviewers were resolved by a third senior radiologist with 20 years of experience, whose evaluation served as the final determination.
Clinical Assessment
Medical records were reviewed to collect. 1. Patient demographics (age, sex, BMI, surgery date, time since surgery) 2. Symptoms (back pain and/or leg pain) 3. MRI findings (adjacent segment disease, compression fracture, disc degeneration, hardware issues, etc.) 4. Subsequent surgical interventions (revision surgeries, fusion extensions, etc.)
Statistical Analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Data distribution was assessed for all paired differences using the Shapiro-Wilk test. For normally distributed data, comparisons were made using a paired t-test. For data that violated the assumption of normality, the non-parametric Wilcoxon signed-rank test was employed. To account for multiple comparisons, Bonferroni correction was applied, setting the significance threshold at P < 0.01.
Results
Patient Demographics and Clinical Findings
Demographics and Clinical Characteristics (N = 84)

Demographic and Clinical Characteristics of 84 Patients With Lumbar Titanium Instrumentation Undergoing Postoperative MRI. Data Include Patient Demographics, Clinical Presentation, Pathological Findings Identified on Imaging, and Subsequent Surgical Interventions. Values are Presented as Mean ± Standard Deviation for Continuous Variables and Number (Percentage) for Categorical Variables.
SD, standard deviation; BMI, body mass index.
aHardware Complications Represent Various Implant-Related Issues Identified on Imaging or During Subsequent Surgery
Quantitative Analysis
Comprehensive Comparison of MAVRIC-SL vs STIR Performance (N = 84)
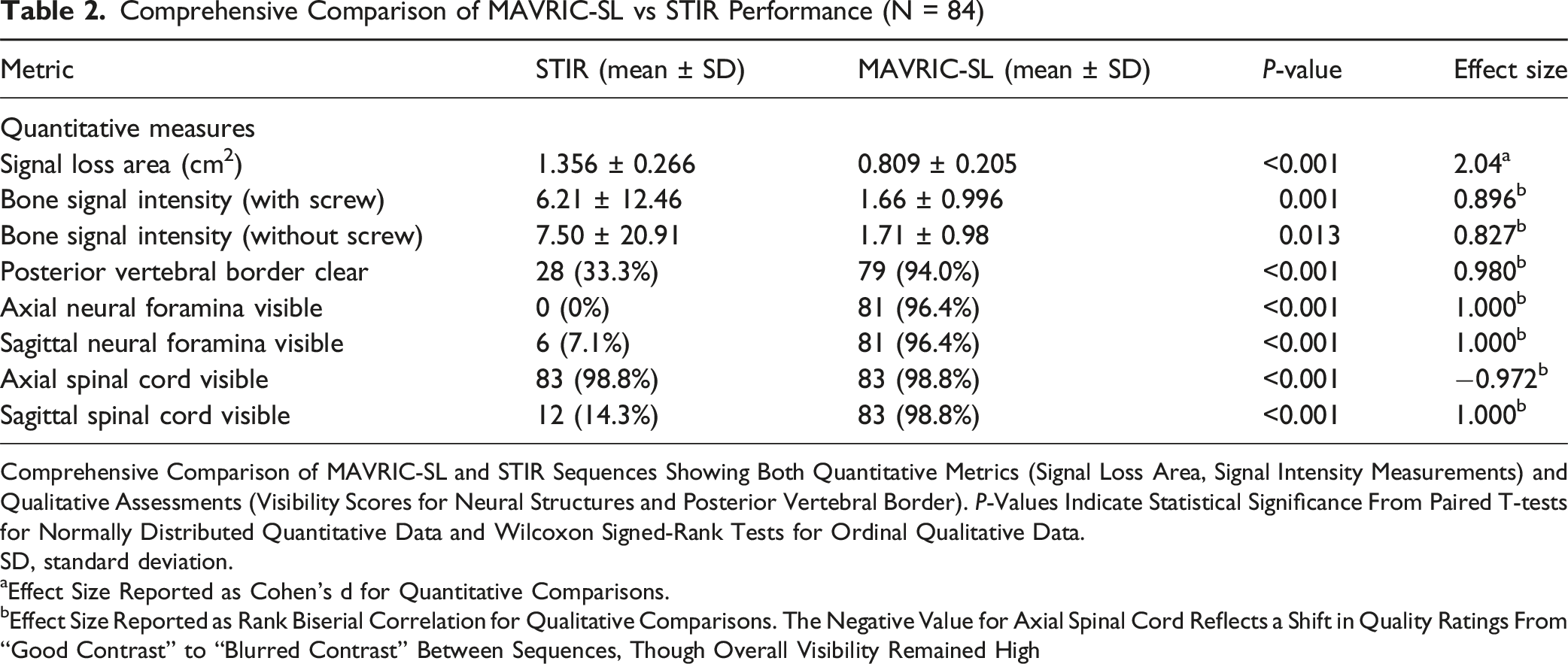
Comprehensive Comparison of MAVRIC-SL and STIR Sequences Showing Both Quantitative Metrics (Signal Loss Area, Signal Intensity Measurements) and Qualitative Assessments (Visibility Scores for Neural Structures and Posterior Vertebral Border). P-Values Indicate Statistical Significance From Paired T-tests for Normally Distributed Quantitative Data and Wilcoxon Signed-Rank Tests for Ordinal Qualitative Data.
SD, standard deviation.
aEffect Size Reported as Cohen’s d for Quantitative Comparisons.
bEffect Size Reported as Rank Biserial Correlation for Qualitative Comparisons. The Negative Value for Axial Spinal Cord Reflects a Shift in Quality Ratings From “Good Contrast” to “Blurred Contrast” Between Sequences, Though Overall Visibility Remained High
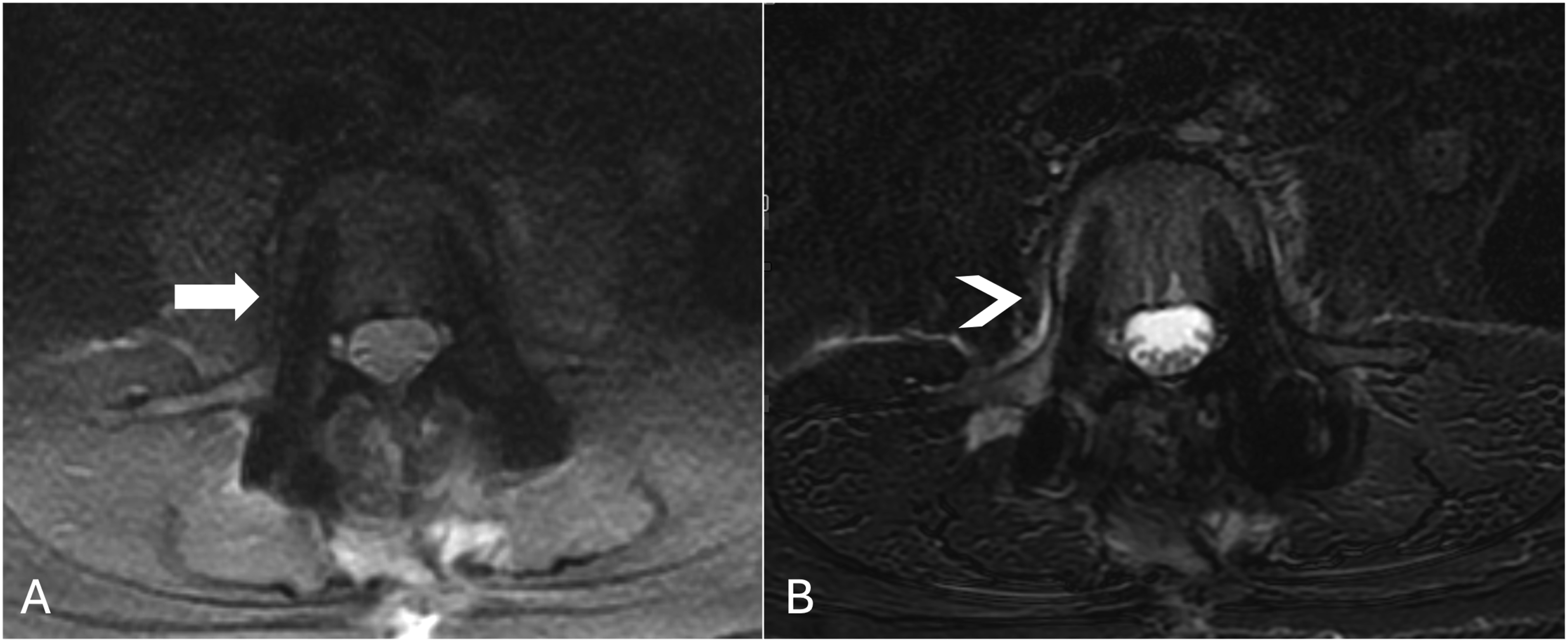
Axial MRI Images at the Same Anatomical Level Demonstrating Pedicle Screw Artifact Differences. (A) MAVRIC-SL Image Shows Clear Delineation of Titanium Pedicle Screws With Minimal Surrounding Signal Loss, Preserving Adjacent Bone Marrow and Soft Tissue Detail (Arrow). (B) STIR Image at the Identical Level Demonstrates Extensive Signal Void With Surrounding Hyperintense Artifacts that Could Mimic Pathological Findings Such as Edema or Inflammatory Changes (Arrowhead). Note the Potential for Diagnostic Misinterpretation With Conventional STIR Imaging Compared to the Accurate Tissue Representation With MAVRIC-SL
Qualitative Assessment
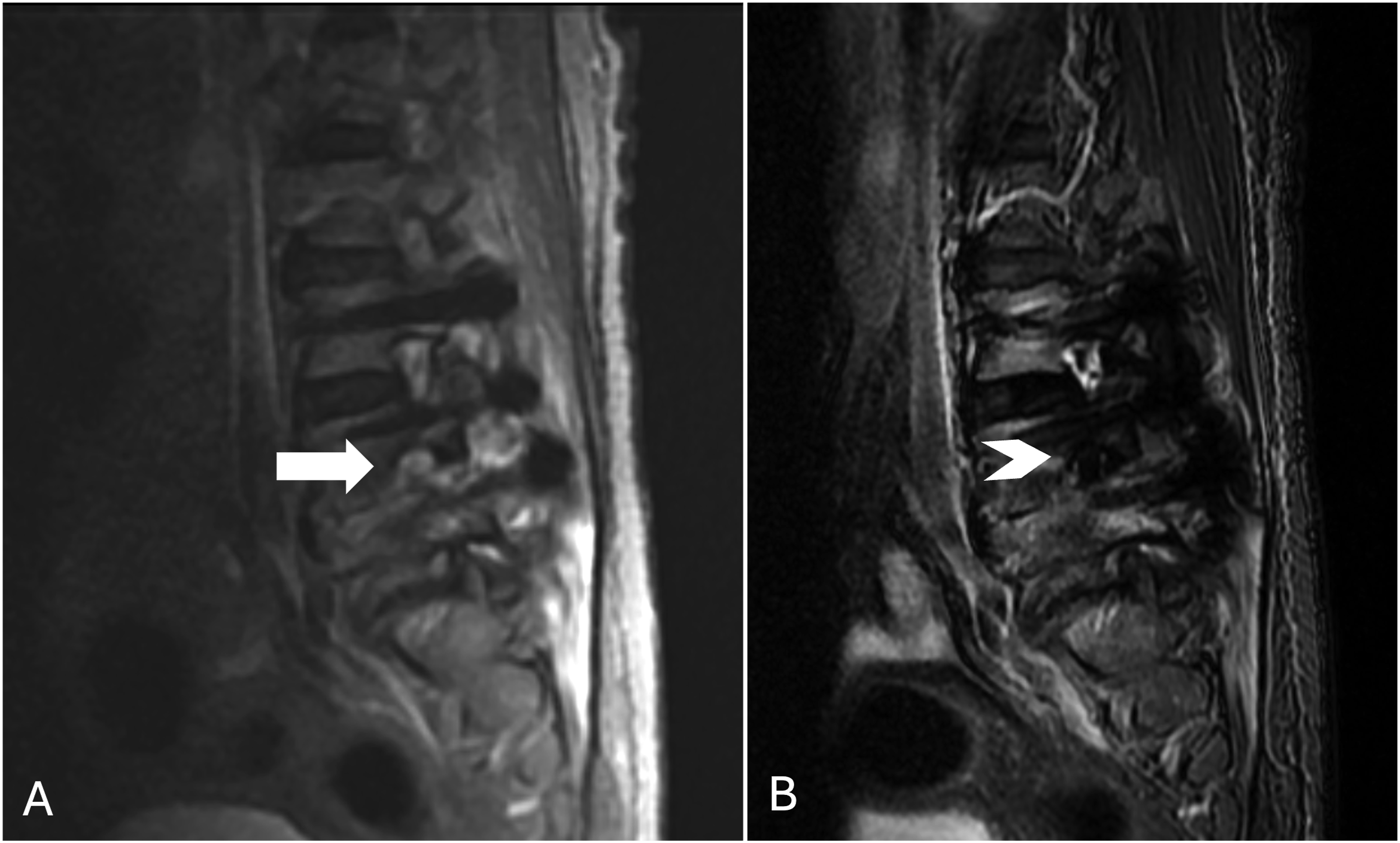
MAVRIC-SL significantly improved visualization of all assessed anatomical structures (Table 2). According to the Wilcoxon signed-rank test, all improvements were statistically significant (P < .001). Substantial improvements occurred in neural foramina visibility. Axial neural foramina visibility increased from 0% with STIR (no cases received score (1) to 96.4% with MAVRIC-SL (81 of 84 cases received score (1) (P < 0.00001), showing a very large effect size (rank biserial correlation = 1.000) (Figure 2). Similarly, sagittal neural foramina visibility improved from 7.1% to 96.4% (rank biserial correlation = 1.000) (Figure 3). Axial MRI Demonstrating Metal Artifact Reduction With MAVRIC-SL Versus STIR Sequences at Same Anatomical Level (C). (A) Axial MAVRIC-SL Image Showing Clear Bilateral Nerve Root Visualization (Arrows) With Minimal Artifacts Around Pedicle Screws. (B) Axial STIR Image at the Same Vertebral Level Demonstrates Extensive Signal Void Artifacts (Arrowheads) Completely Obscuring Bilateral Neural Foramina Sagittal MRI Comparison at an Instrumented Lumbar Level Adjacent to Pedicle Screw Fixation. (A) MAVRIC-SL Sequence Demonstrates Well-Defined Foraminal Boundaries With Minimal Metallic Artifact (Arrow). (B) STIR Sequence Shows Marked Artifact From Pedicle Screws, Obscuring the Foramen (Arrowhead). Note: Image Quality With STIR Varies by Distance From Hardware. This Image Demonstrates the Critical Zone Immediately Adjacent to Instrumentation where Diagnostic Decisions are Made and where STIR Artifacts are Most Problematic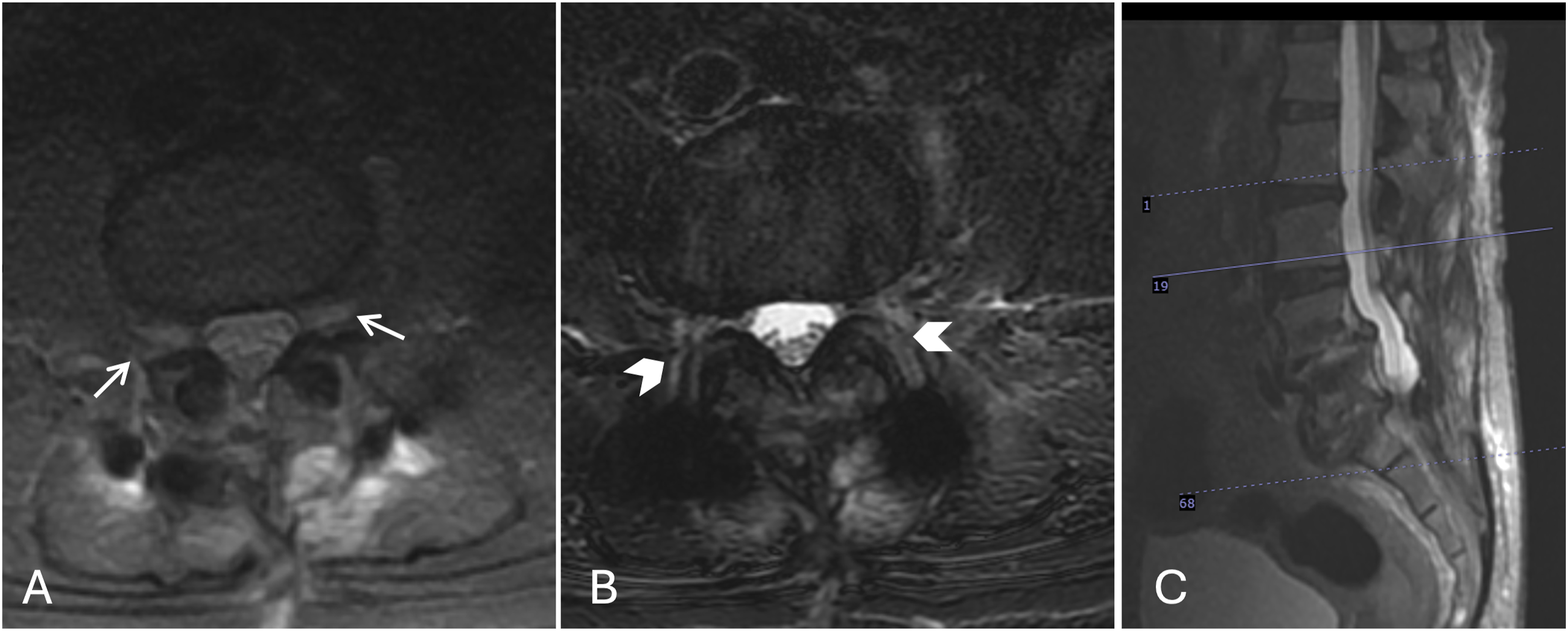
Spinal cord visualization also showed significant enhancement. In sagittal views, visibility increased from 14.3% with STIR to 98.8% with MAVRIC-SL (rank biserial correlation = 1.000). While axial spinal cord visibility was better preserved with STIR, the shift in quality was statistically significant (rank biserial correlation = −0.972). Finally, clarity of the posterior vertebral border improved from 33.3% with STIR to 94.0% with MAVRIC-SL, with a very large effect size (rank biserial correlation = 0.980).
Interobserver reliability was good to excellent across all measurements, with weighted kappa values ranging from 0.61 to 0.79 for qualitative assessments. The highest agreement occurred for axial spinal cord assessment (κ = 0.79) and the lowest for sagittal neural foramen evaluation (κ = 0.61). These reliability values are consistent with published spine imaging studies and indicate reproducible assessments. The slightly lower agreement for sagittal neural foramen evaluation likely reflects the challenging nature of this assessment in the presence of metal artifacts, highlighting the clinical importance of MAVRIC-SL’s significant improvement in this parameter (7.1% to 96.4% visibility).
Discussion
Principal Findings and Clinical Significance
This focused analysis of lumbar spine instrumentation revealed that MAVRIC-SL provides substantial improvements in metal artifact reduction and neural structure visualization, with a large effect size for signal loss reduction (Cohen’s d = 2.04) and strong associations for improved structure visibility (rank biserial correlations >0.95), among the largest reported in medical imaging studies. The restriction to lumbar spine patients, implemented to address anatomical heterogeneity concerns, unexpectedly strengthened our findings compared to mixed population studies, highlighting the importance of anatomical specificity in metal artifact research.
The most clinically significant finding is the significant improvement in neural foramina visualization. The complete inability to visualize axial neural foramina with STIR (0%) vs near-universal visibility with MAVRIC-SL (96.4%) represents a fundamental shift in diagnostic capability. This improvement directly addresses a critical limitation in postoperative spine imaging, where foraminal stenosis and nerve root compression are primary causes of persistent symptoms requiring surgical intervention.
MAVRIC-SL reduced signal loss area by 39.1 ± 15.2% (1.356 ± 0.266 cm2 vs 0.809 ± 0.205 cm2, P < 0.001) with a large effect size (Cohen’s d = 2.04). Beyond quantitative improvements, the qualitative enhancements fundamentally change diagnostic capability, all showing large effect sizes: sagittal neural foramina visibility improved from 7.1% to 96.4% (rank biserial correlation = 1.000), sagittal spinal cord visibility from 14.3% to 98.8% (rank biserial correlation = 1.000), and posterior vertebral border clarity from 33.3% to 94.0% (rank biserial correlation = 0.980).
Comparator Sequence Selection
The choice of STIR as the comparator sequence requires clarification. STIR is widely used for fat-suppressed imaging near metallic implants because conventional fat saturation techniques fail due to magnetic field inhomogeneity.1,3 While newer specialized sequences like SEMAC-VAT have been developed,10,11 STIR remains commonly employed in clinical practice due to its availability and established protocols. Our goal was to demonstrate improvement over current clinical practice rather than comparing with specialized sequences that may have limited availability. Furthermore, postoperative complications such as bone marrow edema, infection, inflammation, and adjacent segment disease require fluid-sensitive sequences for detection. T1-weighted sequences, while less affected by metal artifacts, cannot adequately detect these fluid-sensitive pathologies. STIR’s clinical utility in detecting pathology, despite its artifacts, makes it the appropriate comparator for evaluating MAVRIC-SL’s clinical impact. The improvements observed with MAVRIC-SL vs STIR demonstrate clear clinical value for institutions considering MAVRIC-SL implementation.
It is important to note that STIR performance varies by proximity to metal hardware. At levels distant from instrumentation, STIR may provide adequate visualization. However, our study specifically evaluated neural structures at and immediately adjacent to instrumented segments, where artifacts are most problematic and where clinical decision-making occurs. The substantial improvements with MAVRIC-SL are most critical in these zones where conventional sequences fail to provide diagnostic information. Any single image slice may show variable performance depending on distance from hardware, but our quantitative results (Table 2) represent averaged measurements across instrumented levels where metal artifacts directly impact clinical assessment.
Comparison with Literature and Technical Context
Our 39.1% reduction in signal loss aligns closely with Yang et al's (2021) 12 48% reduction in cervical spine PEEK implants, validating the consistency of MAVRIC-SL performance across different spine regions when analysed separately. However, our effect sizes exceed those typically reported in metal artifact reduction studies, likely reflecting both our focused anatomical approach and the severity of baseline artifacts with titanium instrumentation.
For comparison, Choi et al (2015) 8 reported artifact reductions of 59.9% at the hip level with effect sizes of approximately 1.2, while our lumbar spine analysis found a large effect size for signal loss reduction (Cohen’s d = 2.04). The large effect size for axial neural foramina visibility (rank biserial correlation = 1.000) likely reflects the complete absence of visualization with STIR (0%) combined with near-universal visibility with MAVRIC-SL (96.4%), creating a transformational rather than incremental improvement.
Comparative Studies on Metal Artifact Reduction Techniques
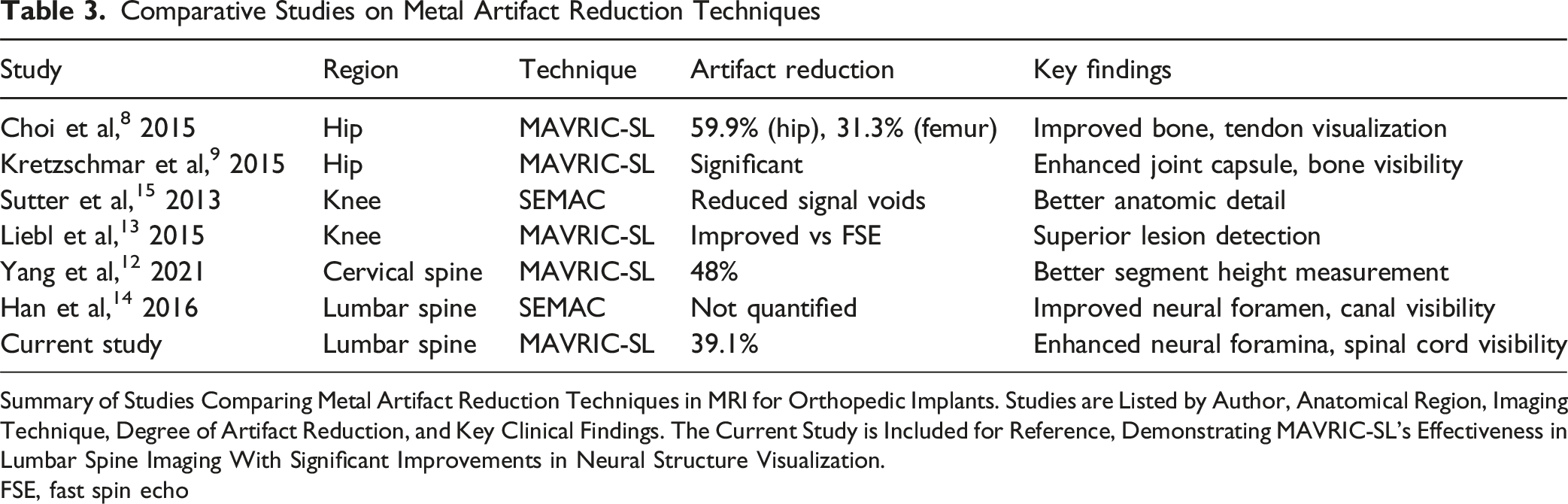
Summary of Studies Comparing Metal Artifact Reduction Techniques in MRI for Orthopedic Implants. Studies are Listed by Author, Anatomical Region, Imaging Technique, Degree of Artifact Reduction, and Key Clinical Findings. The Current Study is Included for Reference, Demonstrating MAVRIC-SL’s Effectiveness in Lumbar Spine Imaging With Significant Improvements in Neural Structure Visualization.
FSE, fast spin echo
Han et al (2016) 14 and Song et al (2013) 11 demonstrated SEMAC’s effectiveness in spine imaging, but their studies did not provide quantitative effect size calculations for direct comparison. Our comprehensive quantitative analysis, combined with clinically relevant qualitative assessments, provides the most detailed evaluation of metal artifact reduction effectiveness in lumbar spine instrumentation to date. 15
Clinical Implications
With spinal fusions rising 137% from 1998 to 2008 and long construct fusions increasing 141% from 2004 to 2014,4,5 accurate postoperative imaging is increasingly important. Our cohort’s 38.1% revision surgery rate underscores the importance of precise diagnostic imaging for identifying complications and guiding treatment decisions. 16
Adjacent segment disease, identified in 29.8% of our patients, exemplifies the diagnostic challenges MAVRIC-SL addresses. This condition requires visualization of disc spaces, neural foramina, and facet joints adjacent to instrumentation - precisely the structures most affected by metal artifacts with conventional imaging. MAVRIC-SL’s ability to restore neural foramina visibility from 0% to 96.4% in axial views directly impacts the ability to diagnose foraminal stenosis, nerve root compression, and adjacent segment pathology.
The improved spinal cord visualization in sagittal views (14.3% to 98.8%) enables detection of rare but serious complications such as epidural hematomas, infections, or cord compression. Similarly, the enhanced posterior vertebral border visualization (33.3% to 94.0%) facilitates assessment of hardware position, fusion status, and potential loosening - critical factors in determining the need for revision surgery.
The longer acquisition time (6:23 vs 1:43 minutes) represents MAVRIC-SL’s primary limitation but must be weighed against the diagnostic gains. For symptomatic patients where surgical decision-making depends on accurate imaging, this time investment is clinically justified. Recent acceleration techniques using compressed sensing and parallel imaging show promise for reducing acquisition times while maintaining diagnostic quality, potentially addressing this limitation in future implementations.17,18
Strengths & Limitations
Several limitations warrant acknowledgment while maintaining perspective on the study’s contributions. The retrospective design, while appropriate for this comparative effectiveness research, may introduce selection bias. However, the consecutive patient enrolment and comprehensive inclusion criteria minimize this concern.
The study was performed on a single 1.5 T GE scanner model, which ensures methodological consistency but may limit generalizability to other vendors and field strengths. However, 1.5 T remains the most widely available clinical MRI platform globally, and the choice over 3T was deliberate, as 1.5 T produces fewer artifacts with titanium implants while providing adequate resolution for clinical decision-making.
Detailed implant specifications (specific screw diameters, rod materials, number of instrumented levels, presence of interbody cages) were not systematically recorded, limiting our ability to correlate hardware characteristics with artifact reduction effectiveness. This information was not consistently available in retrospective surgical records but should be collected prospectively in future studies to optimize protocol selection for specific implant configurations.
The interobserver reliability, while good to excellent (weighted κ = 0.61-0.79), showed the lowest agreement for sagittal neural foramen assessment. This finding, rather than representing a study weakness, highlights the clinical significance of MAVRIC-SL’s improvement in this challenging assessment area. The difficulty in reliably assessing sagittal neural foramina with STIR (κ = 0.61) emphasizes why this structure was visible in only 7.1% of cases, making MAVRIC-SL’s 96.4% visibility rate particularly valuable.
Motion artifact susceptibility, theoretically increased with longer MAVRIC-SL acquisitions, was not systematically analysed. However, no patients were excluded due to motion artifacts, suggesting good clinical feasibility. Future studies should include formal motion assessment and patient tolerance evaluations.
Future Directions
The results warrant several research directions that could further optimize MAVRIC-SL’s clinical implementation. Prospective studies correlating MAVRIC-SL findings with surgical outcomes would establish sensitivity and specificity for specific pathologies, potentially demonstrating improved diagnostic accuracy over conventional imaging. Cost-effectiveness analyses weighing increased acquisition time against improved diagnostic yield would inform implementation decisions.
Development of accelerated MAVRIC-SL protocols represents a critical area for technical advancement. Early work has shown promise for reducing acquisition times while maintaining image quality,17,18 and further development of compressed sensing and parallel imaging techniques could address the current time limitation.
Systematic evaluation across different implant materials (titanium vs PEEK vs stainless steel) and configurations would optimize protocol selection for specific clinical scenarios. Previous work has shown material-dependent artifact patterns, 10 suggesting that tailored approaches could maximize clinical benefit relative to acquisition time.
Integration of quantitative imaging biomarkers derived from MAVRIC-SL, such as automated measurements of neural foraminal dimensions or signal intensity metrics, could provide objective measures for monitoring postoperative changes. Automated analysis approaches could potentially standardize interpretation and reduce observer variability.
Multicentred validation studies across different scanner vendors and field strengths would establish the generalizability of our findings and inform broader clinical implementation strategies. Such studies should include standardized training protocols to optimize measurement reproducibility across institutions.
Conclusion
MAVRIC-SL demonstrates superiority over conventional STIR imaging for lumbar spine instrumentation, with effect sizes that are large and clinically meaningful. This focused analysis of anatomically homogeneous lumbar cases revealed even stronger improvements than initially observed in mixed populations, validating the importance of region-specific evaluation in metal artifact studies.
The improvement in neural structure visualization, particularly the near-complete restoration of neural foramina visibility (0% to 96.4% for axial views, 7.1% to 96.4% for sagittal views), fundamentally changes the diagnostic capability for evaluating symptomatic patients with lumbar instrumentation. These improvements directly address critical clinical needs as spinal fusion procedures continue to increase.4,5
While the longer acquisition time (6:23 vs 1:43 minutes) represents a practical consideration, the transformational diagnostic improvements strongly support implementing MAVRIC-SL as the preferred protocol for postoperative lumbar spine imaging when detailed neural structure evaluation is clinically necessary. The large effect sizes, including a Cohen’s d of 2.04 for artifact reduction and rank biserial correlations approaching 1.0 for structure visibility, demonstrate not merely statistical significance but clinically meaningful improvements that can impact patient care and surgical decision-making.
These findings establish MAVRIC-SL as an important advancement in postoperative spine imaging, providing clinicians with improved visualization of critical anatomical structures previously obscured by metal artifacts. As spinal instrumentation continues to increase, 4 MAVRIC-SL’s superior diagnostic capability becomes increasingly valuable for optimizing patient outcomes through more informed clinical decision-making.
Footnotes
ORCID iDs
Ethical Considerations
This retrospective study was approved by the Institutional Ethics Committee of Manipal Hospital, Bangalore (ECR/34/Inst/KA/2013/RR-19). Informed consent was waived due to the use of anonymized clinical data, in accordance with ethical guidelines.
Author Contributions
All authors meet the ICMJE criteria for authorship and have approved the final manuscript. Contributions were: Conceptualization: Vidyadhara S, Methodology: Vidyadhara S, Abhishek Soni, Data Collection: Prashant Janorkar, Data Curation & Analysis: Abhishek Soni, Balamurugan T, Ullas V Acharya, Surgical Procedures: Vidyadhara S, Writing – Original Draft: Abhishek Soni, Writing – Review & Editing: Vidyadhara S, Madhava Pai Kanhangad, Supervision: Vidyadhara S, Ullas V Acharya
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request, subject to approval by the Institutional Ethics Committee of Manipal Hospital, Bangalore.