
Abstract
Study Design
Retrospective cohort study.
Objectives
Anterior cervical discectomy and fusion (ACDF) provides clinical improvement for cervical radiculopathy. Recently, it was determined that foraminal decompression via uncinate process resection could lead to faster and greater improvement of arm pain. Total uncinatectomy (TU) and partial uncoforaminotomy (PU) are commonly used for direct foraminal decompression. But the advantages and pitfalls of the two techniques remain unknown.
Methods
Consecutive patients(n = 306) who underwent single-level ACDF for degenerative cervical radiculopathy and who were followed up for >2 years were retrospectively reviewed.
Results
GroupTU had a significantly higher degree of subsidence than GroupPU. The 1-year and 2-year fusion rates were higher in GroupPU than those in GroupTU. Postoperative arm pain VAS score, neck pain VAS score, and NDI scores did not demonstrate significant intergroup differences at all time points. GroupTU had a significantly longer operative time, greater EBL, higher dysphagia rate, and more severe retropharyngeal soft tissue swelling than GroupPU did. There was one case (0.7%) of cerebral infarction due to vertebral artery injury in GroupTU.
Conclusion
PU resulted in lesser complications, shorter operative time, and lesser intraoperative bleeding than did TU. Moreover, the uncinate process was partially preserved in PU as a potential stabilizer, causing lesser subsidence and higher fusion rates. However, the clinical efficacy of PU was comparable to that of TU. Thus, resection of only the posterior part of the uncinate process provides sufficient direct foraminal decompression. Therefore, PU could be an effective and safer alternative to TU for foraminal decompression during ACDF.
Keywords
Highlights
• To compare the clinical outcomes and complications of TU and PU to determine the most suitable technique for foraminal decompression during ACDF. • Group PU demonstrated lower rates of complications, shorter operative times, and reduced intraoperative blood loss, both techniques yielded comparable clinical efficacy based on patient-reported outcomes. • PU could be an effective and safer alternative to TU for foraminal decompression during ACDF.
Introduction
Cervical radiculopathy is a common degenerative disorder in aging populations, often leading to pain, disability, and reduced quality of life.1-3 Anterior cervical discectomy and fusion (ACDF) has long been the standard surgical treatment, providing stabilization and indirect neural decompression with reliable clinical outcomes.4-7 In recent years, direct foraminal decompression by resection of the uncinate process has been proposed to achieve more immediate and effective relief of arm pain, a hallmark symptom of cervical radiculopathy.8-11 Among the available techniques, total uncinatectomy (TU) and partial uncoforaminotomy (PU) are most widely used.12-15 However, their comparative advantages and risks remain insufficiently defined in the literature.16-18 Therefore, the purpose of this study was to compare TU and PU with respect to surgical outcomes and complications in patients undergoing single-level ACDF for degenerative cervical radiculopathy, aiming to provide evidence to guide surgical decision-making and improve patient care.
Materials & Methods
Patients
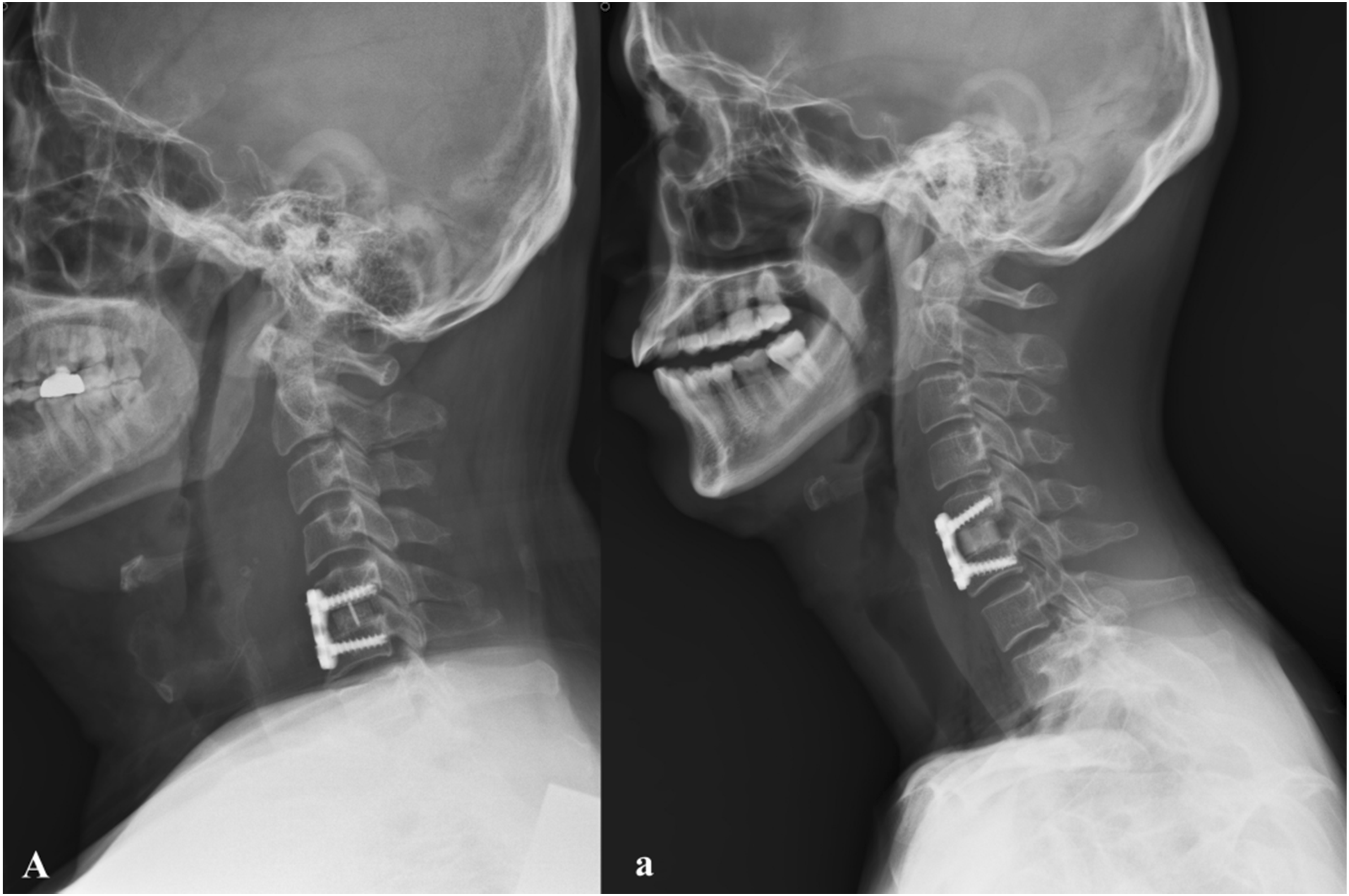
After obtaining institutional review board approval (IRB#2023-0019), this study was conducted using the details of 306 consecutive patients who underwent only single-level ACDF for degenerative cervical radiculopathy by single surgeon between January 2014 and January 2021 at a single academic institution and completed a 2-year follow-up. Patients with traumatic injury, infection, malignancy, revision procedures, loss during follow-up, incomplete study were excluded. Patient demographic features, including age, sex, smoking status, and BMI (kg/m2), were obtained via medical record review. Each patient underwent upright, lateral cervical spine plain radiography preoperatively; immediately after surgery; and 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively. CT was performed preoperatively, 1-year and 2-year post-surgery. Bony union status was measued by cervical flexion-extension lateral radiographs at 1 and 2 year postoperatively. Nonunion was defined as interspinous motion >1 mm in cervical flexion-extension lateral radiographs (Figure 1). The distance of the intervertebral disc space on cervical lateral radiographs was defined as the mean of the anterior disc height, measured as the shortest distance between the anterior edges of adjacent endplates, and the posterior disc height, measured as the shortest distance between their posterior edges (Figure 1). The degree of retro-pharyngeal soft tissue swelling was assessed by measuring the mean of the width of the retro-pharyngeal soft tissue shadow at the C2 and C7 levels on cervical lateral radiographs taken the day after surgery (Figure 2). Among the co-authors, two orthopedic surgeons specializing in the cervical spine directly analyzed the blinded plain radiography and CT images of 301 patients. All images are de-identified, arranged in random order and distributed. Each image included a uniform calibration scale. Measurements were performed in the order listed, and Petavision (Asan medical center, Seoul, Korea) software was used. Each orthopedic rater was trained on the same measurement method, and repeated the measurement three times. Patient-reported outcome measures, including neck and arm pain visual analog scale (VAS) scores, and neck disability index (NDI) scores, were obtained preoperatively and at postoperative 1 and 6 months, and at the 1- and 2-year follow-up visits. The Modified Bazaz Dysphagia Scoring System was used to assess dysphagia scores, with evaluations conducted on the day of surgery, and on the first, third and fifth post-operative days. Dysphagia was assessed using the Modified Bazaz Dysphagia Scoring System on the day of surgery and postoperative days 1, 3, and 5, with a cumulative score ≥12 defined as dysphagia. Retropharyngeal swelling was measured on lateral cervical radiographs at C2 and C7 the day after surgery. The scores are added together, with dysphagia defined as a cumulative score of ≥12. All scores were obtained via medical record review. Estimated blood loss (EBL) was calculated from suction canisters and gauze weights as documented in the operative record. Image Demonstrating the Radiograpgic measurements on Cervical Lateral Radiographs. (A+a)/2: The measurement of retropharyngeal Soft Tissue Swelling Distance; (B + b)/2: The measurement of Intervertebral Disc Space Distance; and C-c:Interspinous Motion < 1 mm on Cervical Lateral Flexion-extension Radiographs to Assess bony Union Image Demonstrating the measurement of retropharyngeal Soft Tissue Swelling on Cervical Lateral Radiographs Taken on the first postoperative day. A. Lateral Radiographs Demonstrating the measurement of retropharyngeal Soft Tissue Swelling on the 1 day after ACDF With TU. a. Lateral Radiographs Demonstrating the measurement of retropharyngeal Soft Tissue Swelling on the 1 day after ACDF With PU. TU, total Uncinatectomy; PU, partial Uncoforaminotomy; ACDF, anterior Cervical Discectomy and Fusion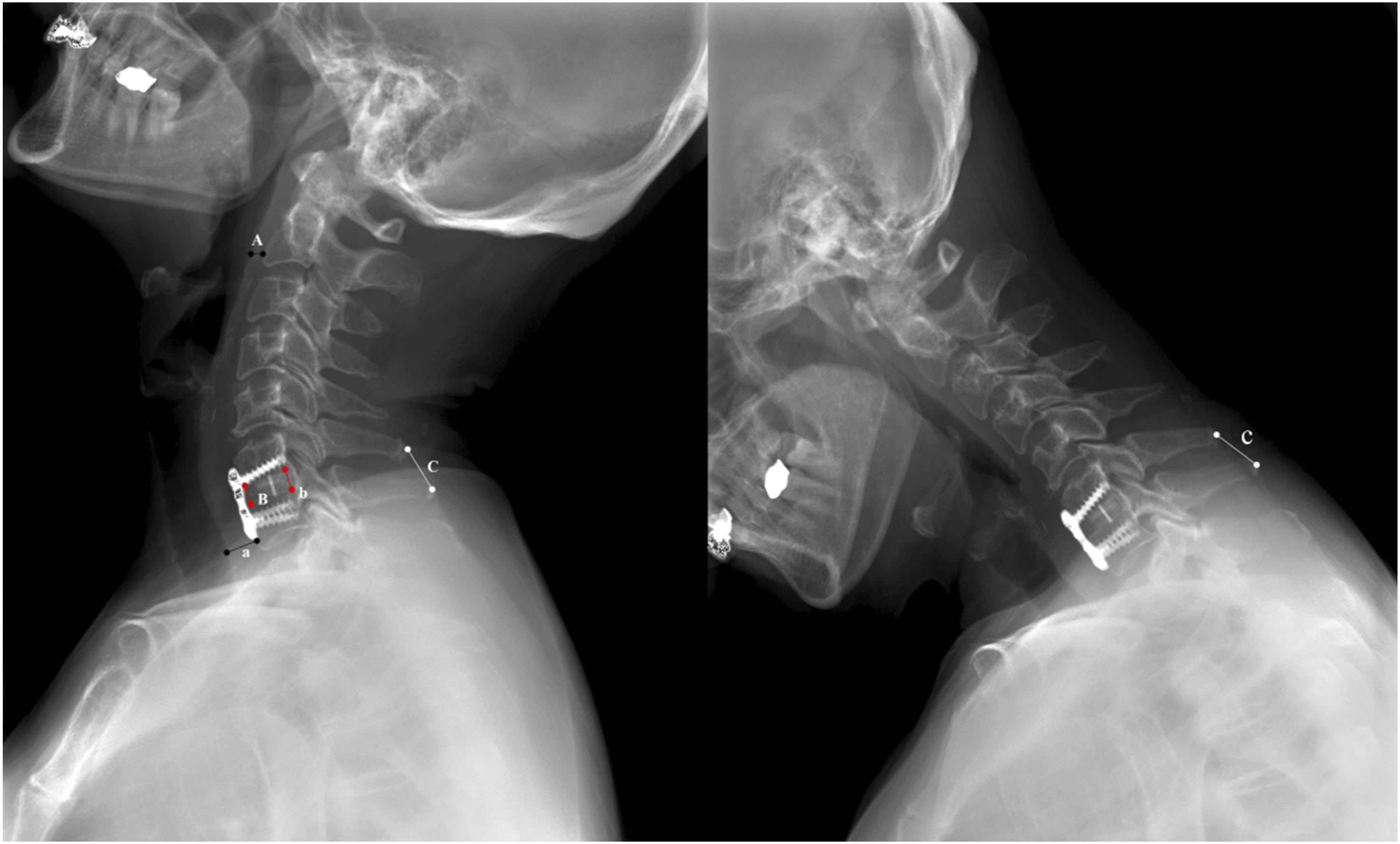
Surgical Methods
All procedures were performed by a single surgeon using a standard Smith–Robinson anterior cervical approach, most commonly through a left transverse skin incision. After discectomy, the disc space was distracted by approximately 2-3 mm using a Casper retractor. Cartilaginous endplates, residual disc, the posterior longitudinal ligament, and osteophytes were removed as indicated. A structural cortical allograft (Cornerstone L-ASR; Medtronic, Minneapolis, USA) packed with local bone was inserted, followed by anterior plate fixation (VENTURE™, Medtronic, Memphis, TN) with variable-angle screws. Patients wore a Philadelphia collar for 6 weeks. No cervical traction or growth factors were used.
For consistency across cases, the true intervertebral foramen was defined as the osseous corridor bounded cranially and caudally by the inferior cortex of the superior pedicle and the superior cortex of the inferior pedicle, and medially and laterally by the pedicle walls. The lateral safety margin corresponded to the periosteal plane overlying the transverse foramen, representing the vertebral artery (VA). The endpoint of decompression was defined as circumferential clearance of this pedicle-to-pedicle corridor, confirmed by visualization and mobilization of the exiting nerve root, without violating the facet joint or transverse foramen.
In the total uncinatectomy (TU) technique, the longus colli muscle was dissected laterally until the uncinate process (UP) was exposed. A Penfield dissector was then inserted lateral to the UP to develop the subperiosteal plane and protect the VA and nerve root. The UP was completely excised using a high-speed burr, backward micro-curette, and micro-pituitary forcept including anterior, posterior, and lateral cortical components. The goal of resection is the complete removal of all bony structures of the hypertrophied uncinate process. Decompression was considered adequate when epidural fat within the foramen and the full circumference of the exiting root canal were clearly visible (Figure 3, Supplementary video). Schematic Illustration of two foraminotomy methods During ACDF. (A) Right Neural Foraminal Stenosis due to Hypertrophied Uncinate Process (UP). 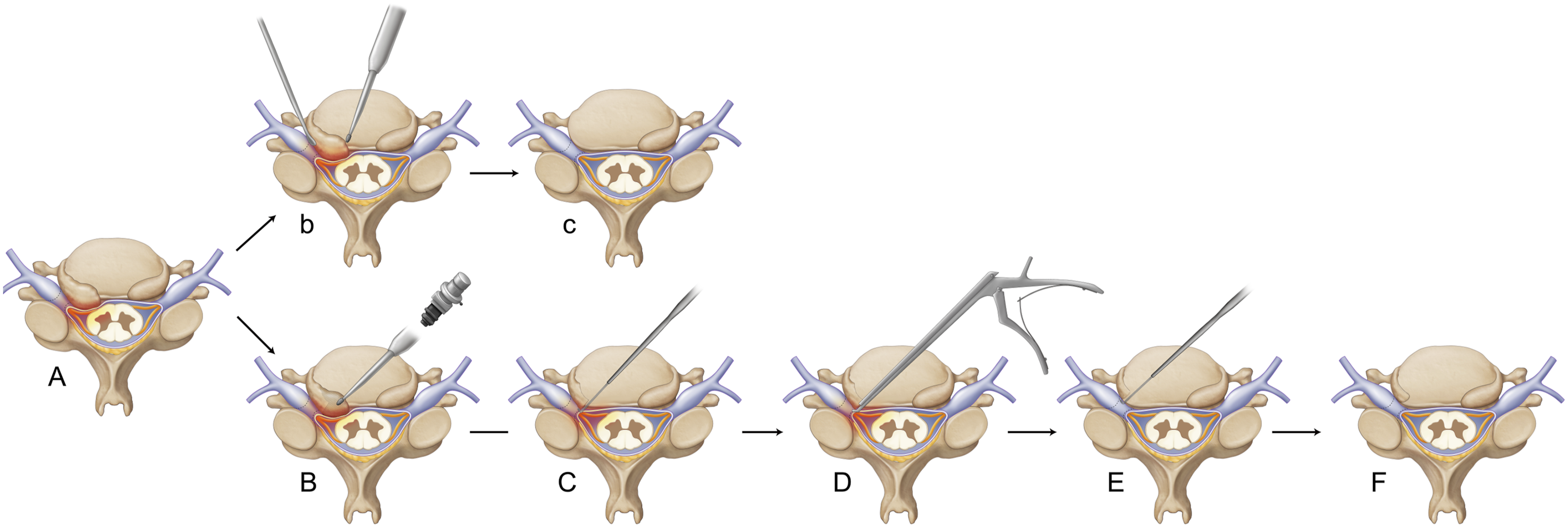
In partial uncoforaminotomy (PU), the microscope was tilted obliquely toward the symptomatic foramen, and when necessary the operating table was adjusted contralaterally or ipsilaterally to optimize the trajectory. The posteromedial portion of the hypertrophied UP was selectively resected with a burr, while the anterior cortical shell was preserved as a stabilizing buttress. A nerve hook is used to palpate and confirm the medial border of the pedicle, ensuring orientation and safety during decompression. The posterolateral half of the UP was undercut using a burr and then further removed with a Kerrison punch or backward micro-curette, with the extent of resection limited to the lateral border of the pedicle but not beyond the VA safety plane. A nerve hook is used to palpate the lateral border of the pedicle, confirming that decompression extends fully to the true lateral margin of the neural foramen with safety. The superior and inferior margins were restricted between the pedicles, ensuring preservation of the facet. Adequate decompression was confirmed by direct visualization of epidural fat and the shoulder and axillary portions of the exiting nerve root. For the distal portion of the root not directly visible, decompression was confirmed by blunt probing with a micro-hook advanced along the root trajectory. The posterior longitudinal ligament was also removed to expose the dura, and final decompression was reconfirmed by palpating the medial and lateral pedicle borders with a nerve hook. This technique provided full clearance of the pedicle-to-pedicle corridor of the foramen while maintaining the anterior UP cortex as a stabilizing element (Figure 3).
Across both TU and PU, resection was never extended beyond the lateral pedicle wall or the periosteal plane over the VA, and cranial and caudal cuts were carefully confined between the pedicles to prevent facet violation. Continuous microscopic visualization, subperiosteal dissection with a Penfield dissector, and repeated palpation of the pedicle margins with a nerve hook were used to maintain orientation and minimize the risk of VA or nerve root injury.
The choice between TU and PU was not based on patient-specific anatomical or clinical criteria but was primarily influenced by evolving institutional practice patterns and increasing surgeon experience. TU was predominantly performed in the earlier years of the study (2014-2017), while PU was more frequently adopted in the later years (2018-2021). The selection of surgical approach (TU vs PU) during the study period was influenced primarily by the evolving institutional practice patterns and growing clinical experience rather than strict predefined criteria. In the earlier years of the study (2014-2017), TU was more commonly employed due to its established surgical familiarity and outcomes. As clinical experience with PU accumulated and favorable short-term outcomes were observed, there was a gradual shift in preference toward PU in the latter years (2018-2021). Thus, the choice of surgical technique in this cohort reflects a natural progression of surgical strategy based on accumulating evidence, surgeon familiarity, and evolving institutional protocols, rather than patient-specific anatomical or clinical selection criteria.
Statistical Methods
Differences in proportions between the groups were analyzed using the chi-square test. Continuous variables were compared using both parametric (Student’s t-test) and non-parametric tests (Mann–Whitney U test for independent samples and Wilcoxon’s signed-rank test for dependent samples), as appropriate. Statistical analysis was performed using SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < 0.05.
Results
The Preoperative Demographic Features of patients
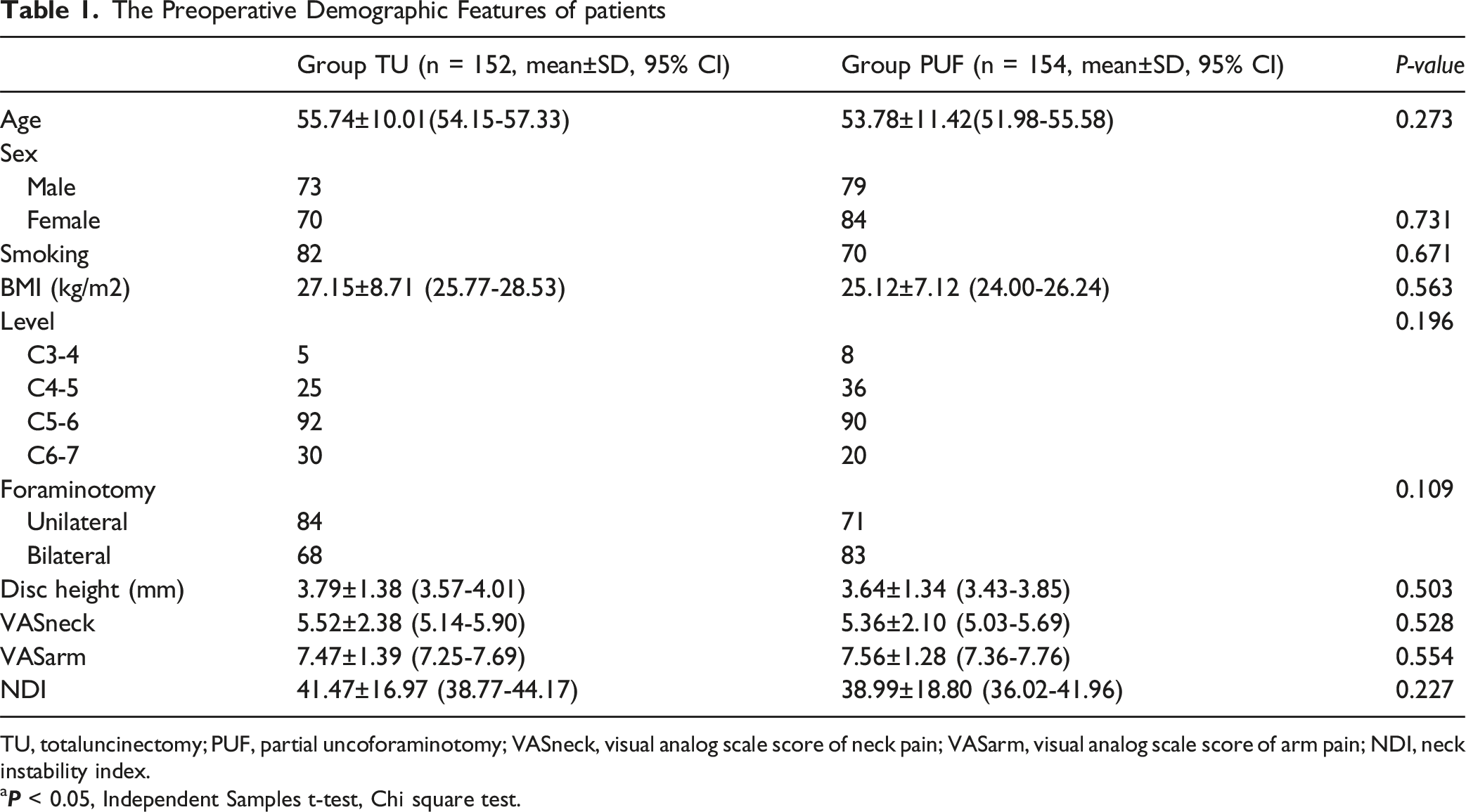
TU, totaluncinectomy; PUF, partial uncoforaminotomy; VASneck, visual analog scale score of neck pain; VASarm, visual analog scale score of arm pain; NDI, neck instability index.
a
Comparison of Clinical Outcomes Between Groups TU and PUF

TU, totaluncinectomy; PUF, partial uncoforaminotomy; OP time, operative time; EBL, estimated blood loss; Retro-swelling, retropharyngeal soft tissue swelling; VA, vertebral artery; POD, postoperative day; VASneck, visual analog scale score of neck pain; VASarm, visual analog scale score of arm pain; NDI, neck instability index.
b
aModified Bazaz dysphagia scoring system was used.
cAssessment is undertaken on the day of operation and on the first, third and fifth post-operative days; the scores are added together, with dysphagia defined as a cumulative score of ≥12.
Discussion
Severe degeneration or disc herniation of the cervical spine is a common cause of arm radiating pain. In many cervical radiculopathic patients, neural foramen stenosis is caused by accumulation of osteophytes or severe hypertrophy of the uncovertebral joint.19-21 Surgical intervention may be considered when conservative treatment fails for a sufficient period of time. The standard surgical technique is ACDF, a discectomy with fusion of two adjacent vertebral bodies. ACDF is a well-established surgical technique, recognized for its excellent clinical outcomes and relatively low complication rates. 22 It has also been reported that performing direct foraminal decompression during ACDF can lead to more rapid and superior relief of arm pain, a process that requires uncinate process resection. 14
Foraminotomy, the surgical procedure aimed at enlarging the intervertebral foramen to alleviate nerve root compression, has gained prominence in the context of ACDF. 14 Over the years, various techniques have emerged, including total uncinatectomy. 9 These methods allow for direct decompression of the neural structures, thereby enhancing patient outcomes.9,13 However, various spinal movements such as flexion, extension, lateral bending, and rotation are influenced by the articulating structure between the uncinate process and the vertebra above.23,24 Fundamentally, the uncinate process plays a role in limiting lateral bending and posterior translation. Additionally, it helps support the load from the superior vertebra, providing stability between the upper and lower vertebrae under greater loading conditions. 24 Therefore, complete resection of the uncinate process during ACDF may lead to segmental instability, potentially complicating the fusion process or contributing to various complications.24,25 As a result, the technique of partial uncoforaminotomy has emerged, where only the posterolateral portion of the uncinate process is resected, decompressing the foraminal area defined by the medial and lateral margins of the pedicle, rather than performing a total uncinatectomy.12,16 While several studies have examined the effectiveness of partial uncoforaminotomy, no direct comparative studies have been conducted to evaluate its outcomes and complications in relation to traditional total uncinatectomy.
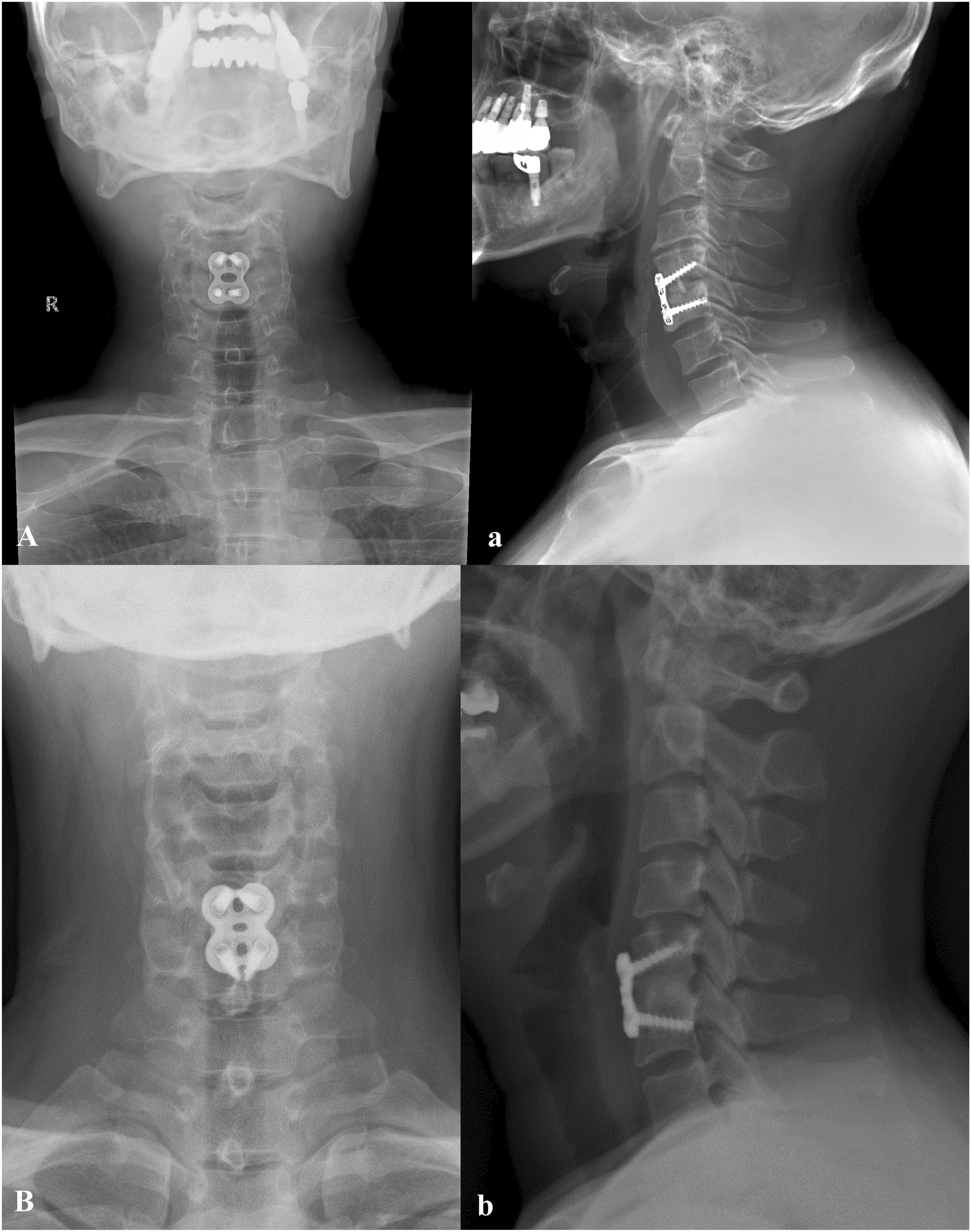
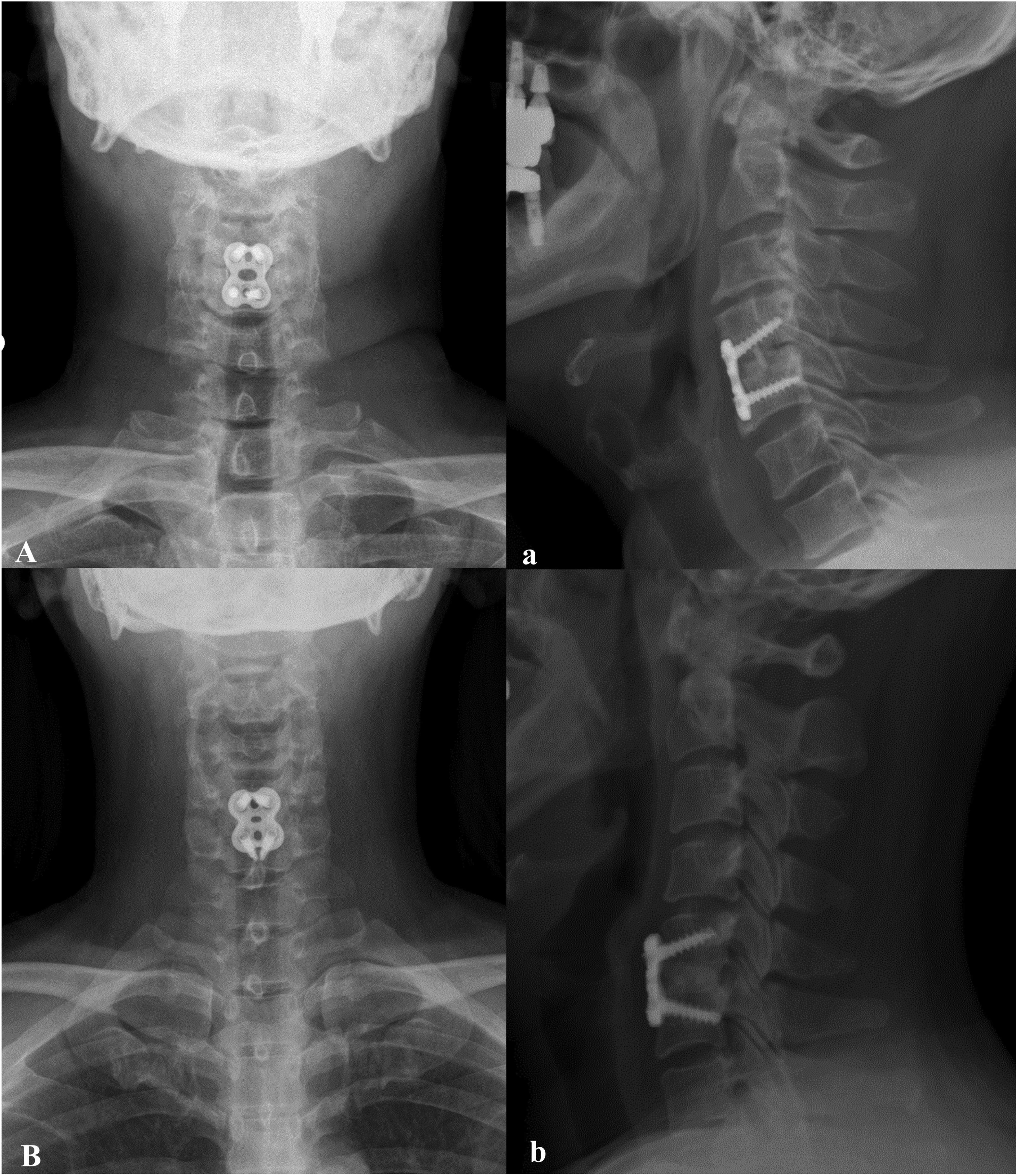
The comparison of TU and PU in the context of ACDF for cervical radiculopathy reveals significant differences in clinical outcomes, operative parameters, and complications. While both techniques aim to achieve foraminal decompression, our findings suggest that PU may offer superior results in terms of safety and efficiency. Firstly, the analysis demonstrated a significantly higher degree of subsidence in Group TU compared to Group PU at multiple postoperative intervals. The higher subsidence rate in the TU group may also be partly related to the use of larger cages, which were required after complete uncinate removal. This difference is crucial, as subsidence can lead to compromised stability of the construct and potential long-term failure of the fusion. Additionally, the lower rates of nonunion observed in Group PU at both one and two years postoperatively indicate that preserving the uncinate process contributes positively to spinal stability and enhances fusion rates. Despite higher subsidence in TU, global cervical lordosis and sagittal alignment at 2 years were not significantly different between groups. This suggests that moderate subsidence did not lead to clinically relevant sagittal imbalance within the follow-up period. The preservation of the uncinate process during PU likely provides a critical stabilizing effect that reduces the likelihood of subsidence, thus supporting the argument that less invasive techniques can yield favorable long-term outcomes (Figures 4 and 5). Operative time and estimated blood loss were notably higher in Group TU, aligning with the expectation that more extensive surgical procedures entail increased morbidity. The longer operative times associated with TU may also correlate with greater postoperative dysphagia and retropharyngeal swelling. Specifically, the dysphagia rates were significantly higher in Group TU, along with higher dysphagia scores based on the modified Bazaz dysphagia scoring system. This highlights the trade-off between achieving complete foraminal decompression and the potential for increased postoperative complications, such as swallowing difficulties, which can severely impact the patient’s quality of life. Despite the differences in surgical technique, patient-reported outcomes, including VAS scores for arm and neck pain and the NDI scores, did not reveal significant intergroup differences at any follow-up time points. Although PU demonstrated lower subsidence and higher fusion rates, these radiographic advantages did not translate into significant differences in VAS or NDI scores during the 2-year follow-up. The long-term functional significance remains uncertain and warrants further investigation. This suggests that while TU may ensure complete decompression, PU still achieves comparable clinical efficacy, allowing for a more favorable balance between efficacy and safety. The finding that patients undergoing PU experienced similar pain relief and functional improvement supports the notion that partial decompression is adequate for addressing cervical radiculopathy without necessitating extensive surgical intervention. These results achieved using only the PU technique suggest the possibility that adequate neural decompression can be attained by targeting the actual intervertebral foramen area surrounded by the pedicle, accomplished by palpating the medial and lateral margins of the pedicle using a probe during the surgical procedure. The technical nuances of each approach also warrant discussion. Total uncinatectomy, while effective, requires excessive lateral exposure and retraction, which may exacerbate postoperative complications, particularly dysphagia and soft tissue swelling. These factors should be carefully considered when selecting the appropriate surgical technique for individual patients, particularly in a population where minimizing morbidity is paramount. Vertebral artery injury is a rare but serious complication of TU. Preventive strategies include careful identification of the lateral margin using a Penfield dissector, controlled burring under constant visualization, and limiting lateral resection. In cases where total uncinatectomy is performed and subsidence risk is high, supplemental posterior fixation may be considered to enhance construct stability and promote solid fusion (Figure 6). Total Uncinatectomy and partial Uncoforaminotomy Cases During ACDF: Antero-Posterior (AP) and Lateral Radiographs Taken first day after Surgery. A-a. AP and Lateral Radiographs on the first day after ACDF With TU. B-b. AP and Lateral Radiographs on the first day after ACDF With PU. TU, total Uncinatectomy; PU, partial Uncoforaminotomy; ACDF, anterior Cervical Discectomy and Fusion Total Uncinatectomy and partial Uncoforaminotomy Cases During ACDF: Antero-Posterior (AP) and Lateral Radiographs Taken at 1 Year after Surgery. The Foramen Shown is Located on the Left Side. A-a. AP and Lateral Radiographs on the 1 year after ACDF With TU. B-b. AP and Lateral Radiographs on the 1 year after ACDF With PU. TU, total Uncinatectomy; PU, partial Uncoforaminotomy; ACDF, anterior Cervical Discectomy and Fusion Total Uncinatectomy and partial Uncoforaminotomy Cases During ACDF: Antero-Posterior (AP) and Lateral Radiographs Taken at 2 Year after Surgery. The Foramen Shown is Located on the Left Side. A-a. AP and Lateral Radiographs on the 2 year after ACDF With TU. B-b. AP and Lateral Radiographs on the 2 year after ACDF With PU. TU, total Uncinatectomy; PU, partial Uncoforaminotomy; ACDF, anterior Cervical Discectomy and Fusion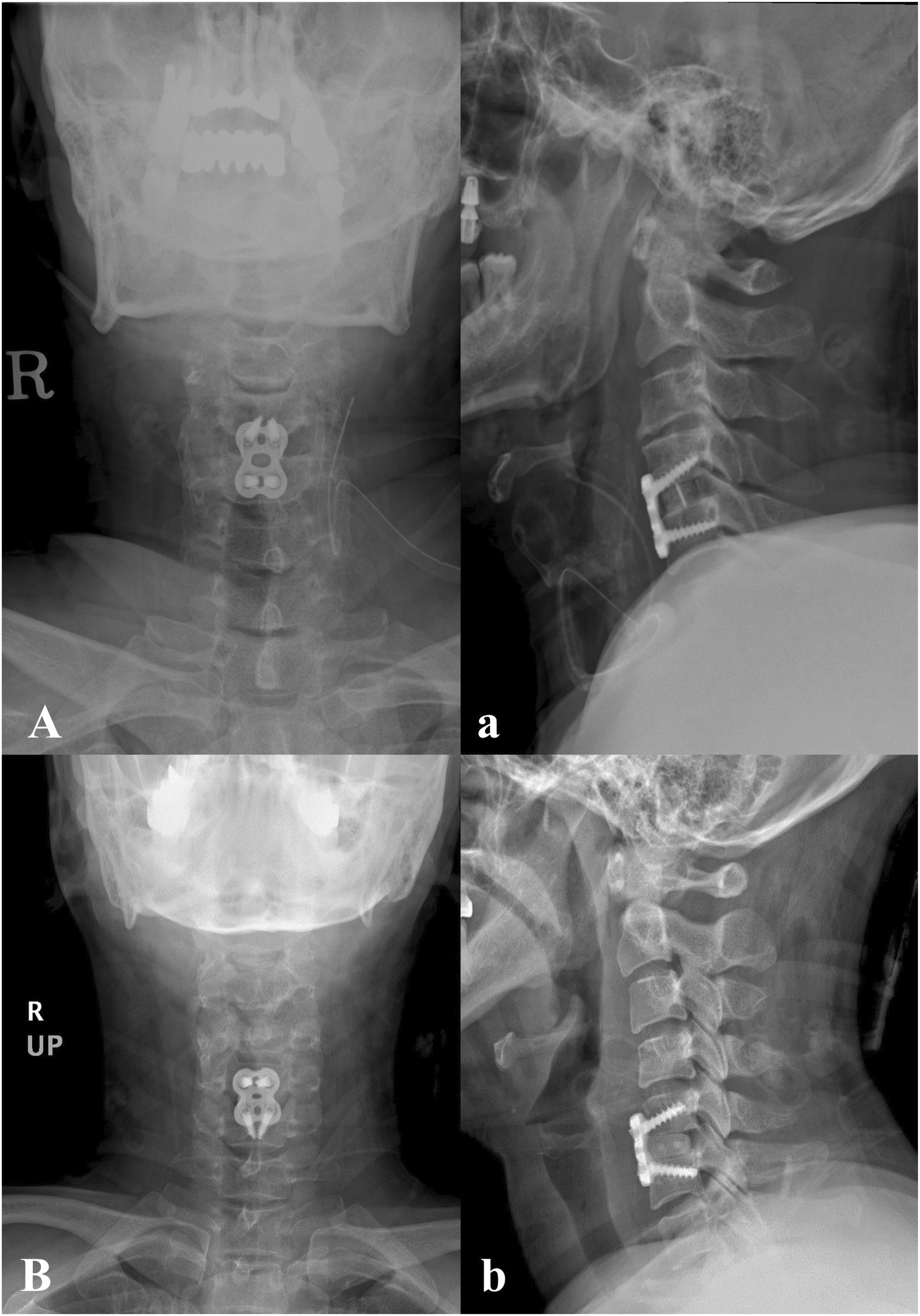
This study has several limitations. First, its retrospective design inherently limits the ability to establish causality. Second, a chronological bias may exist because TU was performed earlier in the study period, followed by a gradual transition to PU as the surgeon’s preference evolved, which may have influenced outcomes. Third, due to incomplete availability of key covariates across the entire cohort, a reliable multivariate adjustment could not be performed, which limits control for potential confounding factors. Lastly, long-term follow-up radiographs were not available for all patients, which restricted our ability to systematically evaluate sagittal alignment outcomes. Therefore, the results should be interpreted with caution, and future well-designed prospective comparative studies are warranted to validate our findings.
In conclusion, while TU provides complete foraminal decompression, the results of this study favor PU as the preferred technique during ACDF for cervical radiculopathy. PU not only reduces operative time and blood loss but also minimizes the incidence of complications such as dysphagia, all while achieving similar clinical outcomes. Based on our findings, PU appears to be a safer and equally effective alternative to TU for foraminal decompression during ACDF, although prospective randomized studies are needed to validate these results. Future studies should aim to further elucidate the long-term effects of these techniques on patient quality of life and surgical outcomes.
Supplemental Material
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.
IRB Approval
This study was approved by IRB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.