
Abstract
Study Design
Retrospective cohort study using a nationally representative inpatient database.
Objective
To determine the incidence, timing, and predictors of new-onset psychiatric disorders following lumbar fusion surgery, and to propose a data-driven risk stratification model for early identification and intervention.
Methods
We queried the Nationwide Readmissions Database (2016-2019) to identify adults undergoing elective inpatient lumbar fusion. Patients with preexisting psychiatric diagnoses were excluded. Outcomes included new-onset depression, anxiety, suicidal ideation, and homicidal ideation within 12 months postoperatively. Predictors were assessed using odds ratios. Timing of onset was evaluated with density plots.
Results
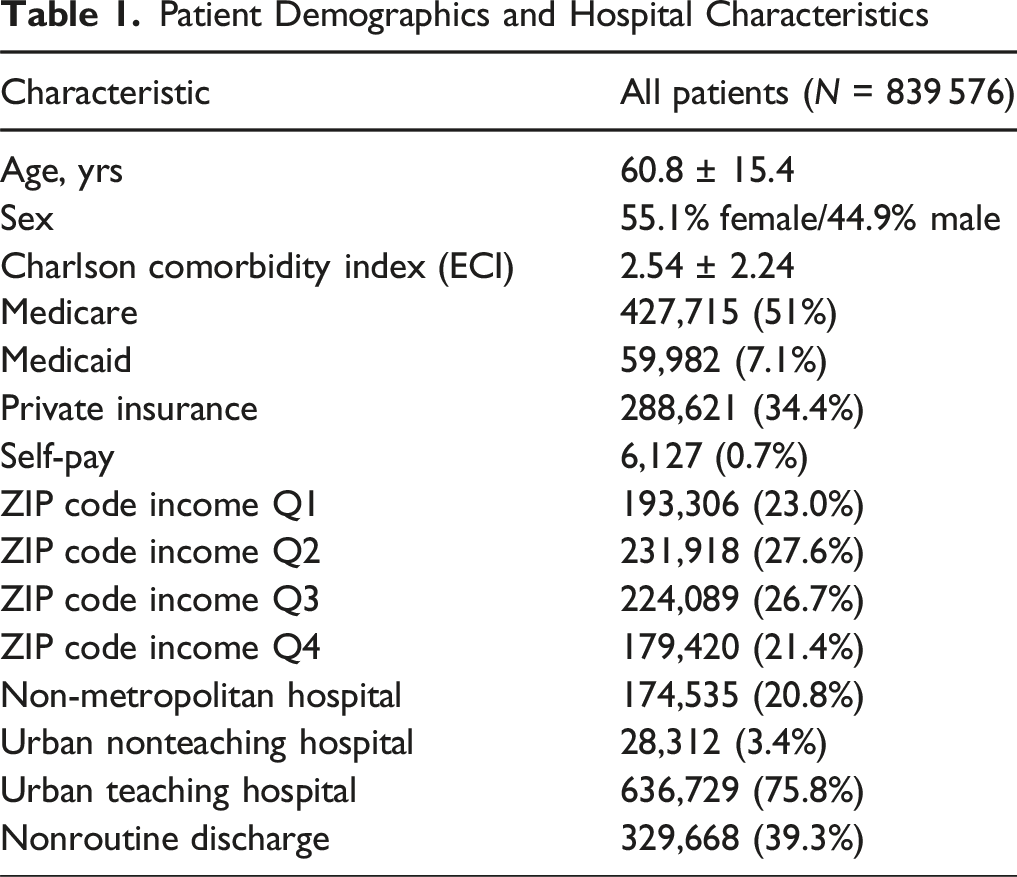
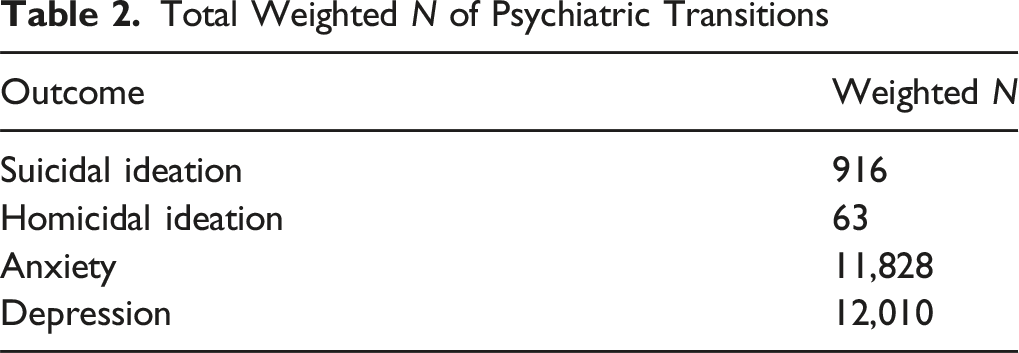
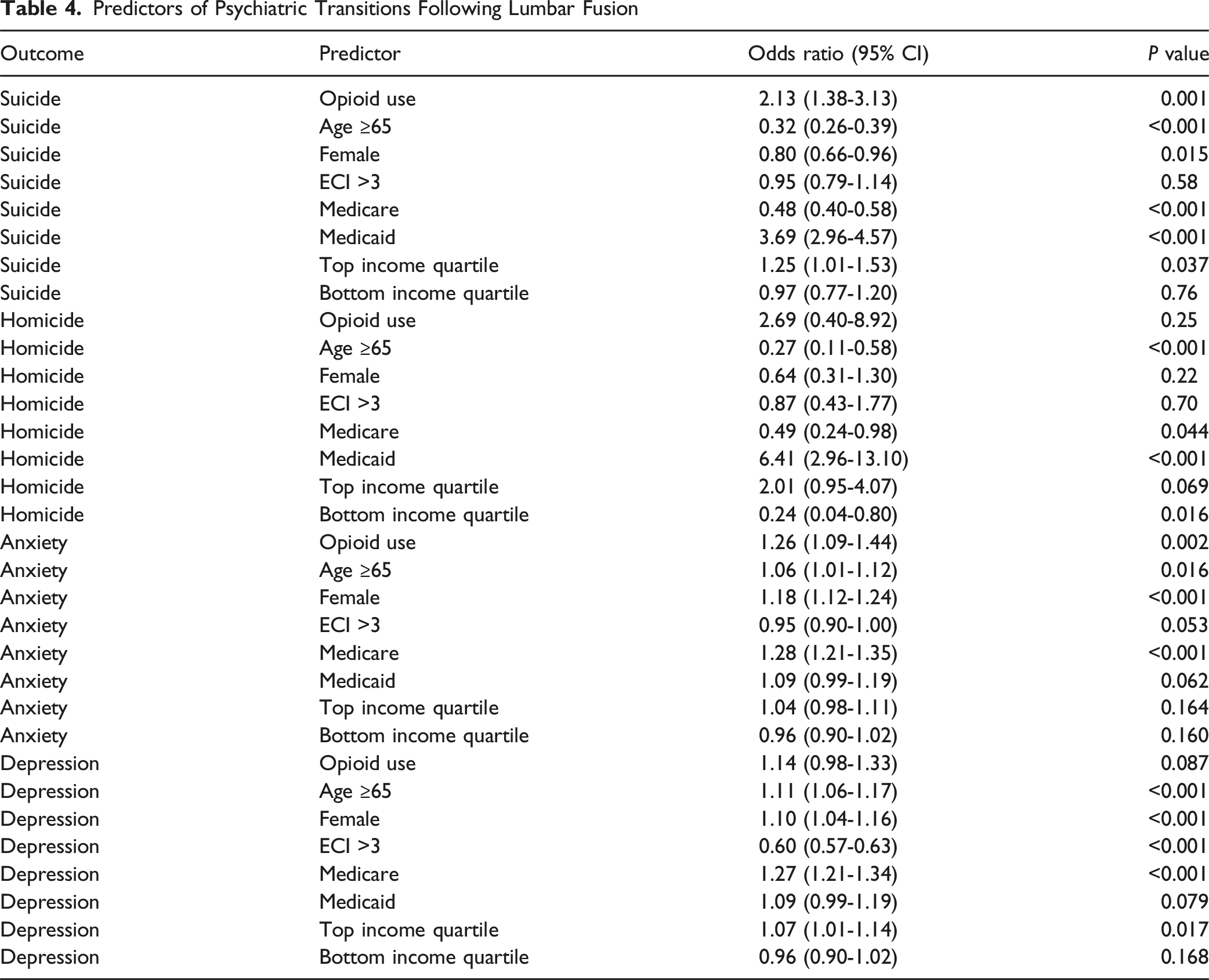
Among 839,576 patients, 12,011 developed depression, 11,828 anxiety, 916 suicidal ideation, and 63 homicidal ideation. Most diagnoses occurred within 90 days postoperatively, with peak incidence around 3 weeks. Opioid use during the index admission significantly increased odds of suicidal ideation (OR 2.13, P = 0.001), anxiety (OR 1.26, P = 0.002), and showed a trend toward depression (OR 1.14, P = 0.087). Medicaid insurance was the strongest predictor of suicidal (OR 3.69) and homicidal ideation (OR 6.41). Female sex and younger age were associated with anxiety and depression; older age was protective against ideation.
Conclusions
New-onset psychiatric disorders are a frequent and early complication following lumbar fusion. Several modifiable and demographic factors - including perioperative opioid use and socioeconomic status - significantly predict risk. These findings underscore the need for structured mental health screening within the first 3 months post-surgery. Implementing a predictive risk stratification tool could enable earlier psychiatric referral, reduce long-term morbidity, and improve both recovery trajectories and overall quality of life.
Introduction
Spine surgery is among the most complex and transformative interventions in modern medicine, offering significant restoration of function and quality of life for patients with degenerative, traumatic, and neoplastic spinal pathologies. While surgical advancements have refined techniques and improved physical outcomes, the psychological aftermath of these procedures remains underrecognized and underexplored. Emerging evidence indicates that psychiatric complications, such as depression, anxiety, and suicidal ideation, are prevalent following spine surgery and significantly influence recovery trajectories, functional outcomes, and overall patient satisfaction.1,2 Notably, up to 60% of spine surgery patients present with active psychological disorders, which are strongly associated with worse pain perception, increased disability, and higher healthcare utilization post-surgery.1,3 Despite these risks, perioperative psychiatric screening and management strategies are inconsistently applied, creating a critical gap in comprehensive surgical care.
Psychiatric comorbidities are among the strongest predictors of postoperative complications in spine surgery patients. Preoperative mental health disorders, particularly depression and anxiety, have been consistently linked to worse surgical outcomes, including prolonged hospital stays, higher rates of complications, and delayed functional recovery.1,4,5 Chronic postoperative pain is another significant concern, as it exacerbates psychiatric symptoms and contributes to the development of mood disorders.3,6 The cyclical nature of pain and psychiatric distress creates a substantial barrier to optimal recovery, as unmanaged pain can lead to increased psychological stress, which in turn can worsen pain perception and reduce adherence to rehabilitation protocols. 7 Addressing these risk factors early in the perioperative process may enhance outcomes and reduce the burden of postoperative complications.
Opioid use, both preoperative and postoperative, is a well-documented risk factor for psychiatric complications following spine surgery. Patients with pre-existing psychological disorders are more likely to develop postoperative opioid dependence, contributing to worse subjective pain perception and poorer functional outcomes.8,9 Prolonged opioid use has been linked to higher rates of depression, anxiety, and substance use disorders, complicating recovery and impairing long-term functional outcomes. 10 This bidirectional relationship between opioid use and psychiatric distress suggests that addressing opioid consumption as a modifiable risk factor is essential for developing effective perioperative care strategies. Furthermore, unmanaged psychological disorders are associated with greater postoperative opioid consumption and poorer pain outcomes, reinforcing the need for integrated mental health care. 11 Additionally, patients with unmanaged psychological disorders often have unrealistic expectations of surgical outcomes, further complicating their recovery journey. 12
Despite the established connection between psychiatric health and surgical outcomes, mental health assessments are not standardized within spine surgery practices. Enhanced Recovery After Surgery (ERAS) protocols have begun integrating mental health screenings, acknowledging that psychological well-being is critical for optimizing surgical outcomes and minimizing complications. However, the timing of psychiatric evaluations and their integration into routine clinical workflows remain undefined. The reviewed literature strongly advocates for routine psychological screening using validated tools such as the Distress and Risk Assessment Method (DRAM), Hospital Anxiety and Depression Scale (HADS), and Beck Depression Inventory (BDI).1,3 Recent studies have also demonstrated that preoperative neuroscience education and cognitive behavioral therapy (CBT) can reduce catastrophizing behaviors, enhance coping mechanisms, and improve postoperative pain management and functional outcomes.11-13 Yet, these interventions are rarely incorporated into standard perioperative pathways.
Psychological traits such as catastrophizing and fear-avoidance behaviors have been shown to negatively influence postoperative recovery. Patients who perceive themselves as unhealthy, have negative pain beliefs, or possess poor coping mechanisms are more likely to experience worse outcomes following surgery.3,12 Additionally, psychological inflexibility, defined as the inability to adapt to changing situations, has been associated with heightened stress responses, persistent somatic symptoms, and chronic disability post-surgery.14,15 These findings suggest that incorporating assessments of psychological flexibility into preoperative evaluations could offer another avenue for identifying at-risk patients and tailoring postoperative interventions.
Our previous research on traumatic brain injury (TBI) further supports the value of early psychiatric assessment. Using the Nationwide Readmissions Database (NRD), we identified key demographic and clinical factors predictive of psychiatric outcomes post-TBI.16,17 Importantly, we found that psychiatric symptoms frequently emerged within the first 3 months post-injury, highlighting the importance of early intervention. These insights from our prior NRD analyses provide a valuable framework for understanding psychiatric vulnerabilities in lumbar spine surgery using similar methodology.
Despite these insights, analogous research in the context of lumbar fusion surgery is limited. This gap is concerning given the high rates of opioid use, chronic pain, and physical impairment frequently observed in lumbar fusion patients - factors that are independently associated with psychiatric morbidity. 18 Understanding which patient populations are most susceptible to postoperative psychiatric disorders, as well as the timing of symptom onset, which may cluster in the early postoperative period, is crucial for optimizing perioperative care and improving long-term outcomes.
The primary aim of this study is to determine the incidence, timing, and predictors of new-onset psychiatric disorders following lumbar fusion surgery using a nationally representative dataset. By assessing factors such as procedure type, demographic characteristics, and opioid use, we seek to develop a predictive model and risk stratification tool to help spine surgeons and healthcare providers identify high-risk patients. This approach will inform tailored screening and intervention strategies, contributing to the development of comprehensive, multidisciplinary care pathways that optimize perioperative management and improve long-term psychiatric and surgical outcomes.
Methods
Data Source
This study utilized data from the Nationwide Readmissions Database (NRD), a publicly available resource developed as part of the Healthcare Cost and Utilization Project (HCUP) by the Agency for Healthcare Research and Quality (AHRQ). The NRD is a nationally representative inpatient dataset designed to support comprehensive analyses of hospital readmissions and patient outcomes. It includes millions of de-identified patient encounters, with detailed information on demographics, diagnoses, procedures, and hospital characteristics. Through the use of anonymized patient linkage numbers, the NRD enables tracking of readmissions within a calendar year. To ensure national representation, discharge weights provided within the database were applied during analysis. The study focused on data from 2016 to 2019, using International Classification of Diseases, 10th Revision (ICD-10) codes to extract relevant cases. This period encompasses more than 70 million hospital discharges, offering a large and diverse dataset for predictive modeling. As the NRD contains only de-identified information and is publicly accessible, Institutional Review Board (IRB) approval and informed consent were not required.
Patient Selection
Patients were included if they underwent elective, inpatient lumbar fusion and were followed for readmission events within the same calendar year. We excluded patients with multiple lumbar fusions in the same year, as well as those with prior diagnoses of depression, anxiety, suicidal ideation (SI), or homicidal ideation (HI), in order to identify incident psychiatric transitions. Diagnoses were captured through ICD-10-CM codes assigned by healthcare professionals during inpatient encounters. Self-reported data were not included. Psychiatric diagnoses were captured exclusively through ICD-10-CM codes assigned by healthcare providers during inpatient encounters. The NRD does not specify whether these diagnoses were identified through systematic screening protocols, validated instruments, or ad hoc clinical assessments, and this variability may influence diagnostic consistency.
Outcomes included new-onset SI, HI, anxiety, and depression. Transition time was calculated as the number of days from the index lumbar fusion to the first recorded psychiatric diagnosis. We also assessed whether patients were screened for psychiatric conditions within 21 and 90 days of surgery.
Similarly, the NRD does not provide information on whether diagnostic criteria such as the DSM-5, PHQ-9, or Hospital Anxiety and Depression Scale were used. All diagnoses reflect provider-coded entries, which may or may not have been based on validated tools. As such, there is a possibility of overestimation or misclassification.
Covariates included age, sex, Elixhauser Comorbidity Index (ECI), primary insurance type, ZIP code income quartile, hospital type, discharge disposition, and the presence of opioid use during the index admission. Opioid use was defined by ICD-10-CM codes indicating dependence, abuse, or documented use. The NRD does not contain granular prescribing data such as type of opioid, dose, frequency, morphine milligram equivalents (MME), or duration of use. Discharge weights were applied to generate nationally representative estimates using HCUP recommendations.
Odds ratios were derived from bivariate analysis to examine associations between each psychiatric outcome—suicidal ideation, homicidal ideation, anxiety, and depression—and key clinical and demographic factors. Independent variables included age ≥65 years, sex, Elixhauser Comorbidity Index, primary insurance type, ZIP code income quartile, and perioperative opioid use. National estimates were weighted using discharge-level sampling weights provided by the Healthcare Cost and Utilization Project (HCUP) to ensure representativeness. Odds ratios with corresponding 95% confidence intervals were calculated using the epitools package, with statistical significance defined as two-sided P < .05. All analyses were conducted using R (version 4.1.2; RStudio 2021.09.2.382).
Results
Patient Demographics and Hospital Characteristics
Total Weighted N of Psychiatric Transitions
Psychiatric Screening Timelines Post-Surgery

Predictors of Psychiatric Transitions Following Lumbar Fusion
Discussion
This study provides a comprehensive assessment of new-onset psychiatric disorders following lumbar fusion, utilizing a nationally representative cohort of over 800,000 patients. These findings underscore a frequently overlooked yet clinically significant aspect of spine surgery: the emergence of psychiatric morbidity during the early postoperative period.19,20 By quantifying incidence, delineating timing, and identifying modifiable risk factors, this work contributes critical evidence to support proactive screening and targeted mental health integration into surgical care pathways. 21
The observed 12-month incidence of new-onset depression and anxiety closely aligns with prior studies highlighting the psychological burden among patients undergoing spine surgery, particularly those with chronic pain and limited functional recovery.1,3,22,23 Notably, most psychiatric diagnoses clustered within the first 90 days postoperatively, with a peak incidence at approximately 3 weeks—emphasizing this early phase as a critical window for intervention.20,24,25
A particularly salient finding was the association between opioid exposure during index hospitalization and subsequent psychiatric complications. Opioid use more than doubled the risk of suicidal ideation and significantly increased the likelihood of anxiety, with a trend toward increased depression. These results mirror a growing body of research demonstrating a bidirectional relationship between opioid use and psychiatric distress - whereby psychological symptoms fuel opioid reliance, which in turn worsens affective states.26-28 This maladaptive cycle can impair recovery, elevate pain sensitivity, and prolong functional disability, underscoring the need for integrated perioperative strategies that prioritize both mental health support and opioid stewardship.13,29
Socioeconomic disparities further influenced psychiatric outcomes. Patients with Medicaid insurance demonstrated the highest odds of both suicidal and homicidal ideation, consistent with existing literature showing that insurance type often serves as a stronger predictor of mental health risk than income level alone.9,30 These findings underscore the need for equitable mental health screening strategies, particularly among socially vulnerable populations.
The observed disparities by insurance type and demographic characteristics likely reflect a complex interplay of factors. Prior studies suggest that Medicaid beneficiaries face reduced access to timely mental-health services, higher comorbidity burden, and greater socioeconomic vulnerability, all of which may contribute to elevated risk of SI/HI. Similarly, younger patients and females may experience greater psychiatric morbidity due to higher baseline prevalence of anxiety and depression, differential pain perception, and psychosocial stressors. Conversely, older age may confer protective effects through more established coping mechanisms and different patterns of healthcare utilization.
Demographic characteristics also shaped psychiatric risk. Female patients were more likely to experience anxiety and depression, consistent with broader psychiatric epidemiology.28,31,32 Conversely, female sex was protective against suicidal ideation, though not significantly so for homicidal ideation. Older age (≥65 years) conferred a protective effect against ideation-related outcomes, yet was paradoxically associated with a slight increase in anxiety and depression. This divergence may reflect differences in coping mechanisms, pain perception, or patterns of healthcare utilization across age groups.
In light of these findings, we propose a three-phase psychiatric screening protocol following lumbar fusion: at 3 weeks, 3 months, and 12 months postoperatively. This approach aligns with the temporal clustering of psychiatric transitions observed in our cohort and reflects emerging trends in Enhanced Recovery After Surgery (ERAS) protocols that advocate for early mental health assessment. 10 Incorporating validated screening instruments—such as the Hospital Anxiety and Depression Scale (HADS), Beck Depression Inventory (BDI), and Distress and Risk Assessment Method (DRAM)—during these intervals may facilitate timely detection and appropriate referrals.1,3
Our results also support the broader application of preventive psychological interventions. Cognitive behavioral therapy (CBT), preoperative neuroscience education, and structured expectation management have demonstrated efficacy in reducing catastrophic thinking, enhancing coping, and improving functional recovery.11-13 Tailoring these interventions to high-risk groups—including opioid-exposed patients, Medicaid beneficiaries, and younger females—offers a targeted, equitable model of care delivery.
Strengths and Limitations
Strengths of this study include its unprecedented sample size, national generalizability, and robust methodology, including multivariable modeling and survival analysis. However, several limitations merit discussion. The use of administrative data introduces the possibility of diagnostic misclassification, particularly for psychiatric conditions that may be managed in outpatient settings and not captured in the database. Reliance on ICD-10-CM coding introduces the potential for diagnostic misclassification or under-coding, particularly for outpatient psychiatric conditions not captured in the database. Additionally, key psychosocial variables—such as employment status, social support, trauma history, and prior outpatient psychiatric treatment—were not available in the NRD. These unmeasured factors may confound observed relationships. Furthermore, the NRD lacks detailed information on opioid prescribing patterns, including type of medication, dosage, frequency, and duration of use, which limits the ability to assess dose-dependent or temporal relationships between opioid exposure and psychiatric outcomes. This study was limited to lumbar fusion patients; comparative analyses across other surgical cohorts (eg, arthroplasty, cardiac surgery) would further contextualize these findings but were beyond the scope of this analysis.
Conclusion
New-onset psychiatric disorders are a significant and early complication of lumbar fusion surgery. This study provides compelling evidence for structured perioperative mental health screening and intervention, particularly within the critical first 90 days postoperatively. By identifying high-risk populations and aligning screening efforts with temporal patterns of symptom emergence, these findings offer a framework for developing risk-stratified care models. The integration of psychiatric assessment, opioid stewardship, and behavioral support has the potential to improve recovery, reduce healthcare utilization, and advance a more holistic standard of care in spine surgery (Figure 1). Transition Time to Psychiatric Outcomes Following Lumbar Fusion. Histogram and Density Plots Show Days to New Onset of Psychiatric Outcomes Following Lumbar Fusion. Panel A: Suicidal Ideation. Panel B: Homicidal Ideation. Panel C: Depression. Panel D: Anxiety. All Outcomes Demonstrate a Right-Skewed Distribution, With Most Transitions Occurring Within 90 Days Postoperatively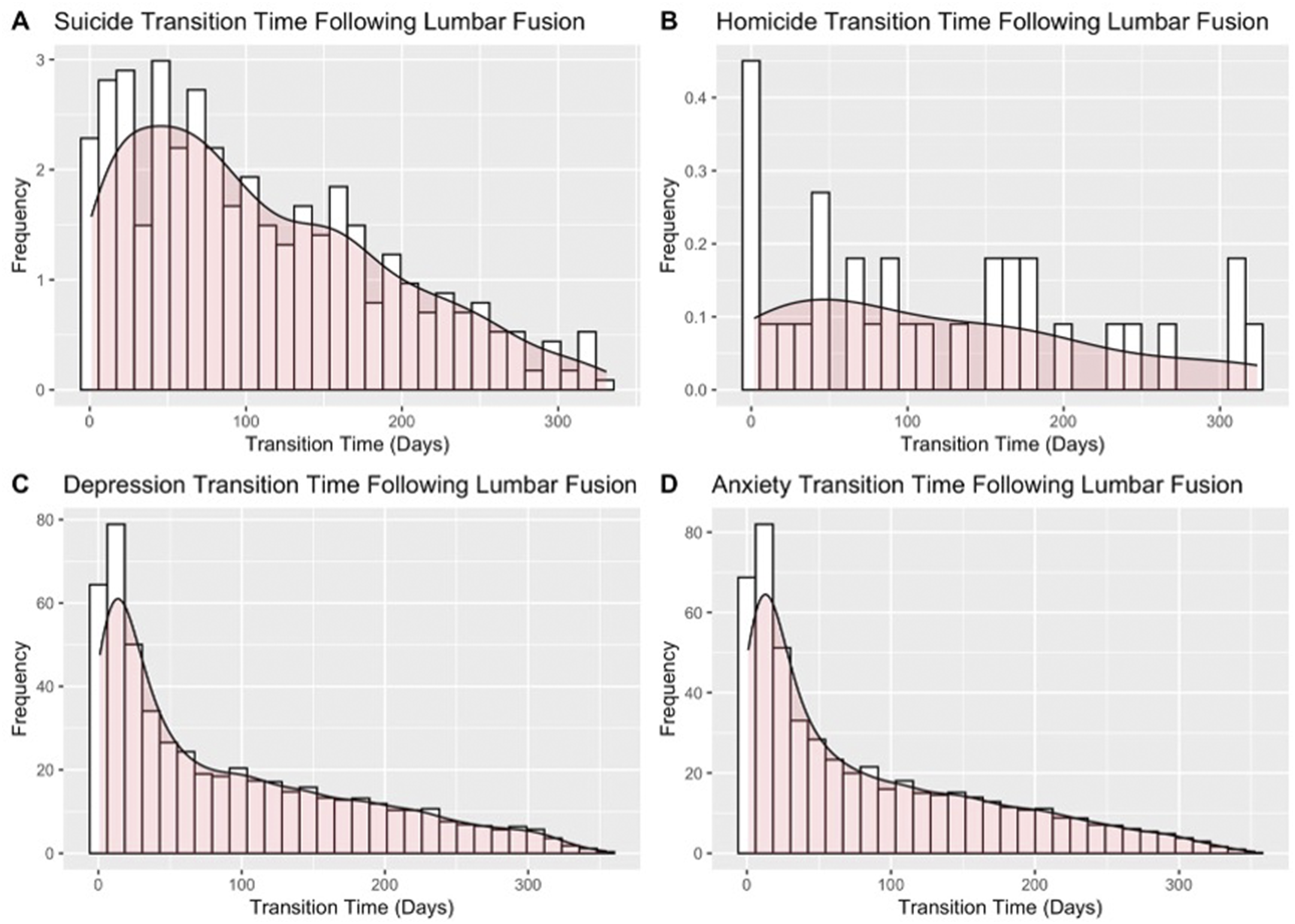
Footnotes
Author Note
ZB is an employee of Cerapedics, Global Head, Medical Strategy (as of 03/01/2025). Cerapedics had no role in the study. JW is a consultant for Angitia, Bioretec, Epidutech, and Precision OS; receives royalties from Biomet, Novapproach, Seaspine, and Synthes; holds stock or stock options in PearlDiver and Surgitech; and serves on the Editorial Board of Global Spine Journal and the Board of the AO Foundation. None of these affiliations had any role in the current study.
Ethical Considerations
This study utilized a deidentified national dataset.
Author Contributions
AMB led the conception and design of the study; SS performed statistical analysis and contributed to study methodology; AT conducted data extraction and supported data interpretation; XTC led the literature review and assisted with results synthesis; ZB and JW provided critical revisions and overall supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.