
Abstract
Study Design
A retrospective cohort study.
Objective
Intraoperative neurophysiological monitoring (IONM) is crucial for detecting impending iatrogenic neurological injury during high-risk scoliosis surgery. However, the implication of significant IONM alarms on long-term neurological function remains unknown for complex deformity correction. This study aims to report the longitudinal neurological outcomes and identify predictors of long-term neurological survivorship for patients with severe spinal deformities.
Methods
A total of 115 patients who encountered significant intraoperative neuromonitoring alarms (excluding systematic and non-operative confounders) during high-risk surgical maneuvers were analyzed. A longitudinal clinical dataset containing baseline information, surgical details, multimodal IONM data, and follow-up neurological function was collected. Cox regression analysis was performed to identify prognostic factors that could predict long-term neurological survivorship. Kaplan-Meier curves were plotted for these predictors, and a nomogram facilitated the clinical prediction of 2-year neurological function.
Results
Immediately after surgery, 57 patients (49.6%) showed neurological deficits, which decreased to only 5 cases (4.3%) at the 2-year follow-up. Multivariate Cox regression analysis for long-term neurological survivorship identified decreased hazard ratios (HRs) for grade six osteotomy (HR, 0.311; P = 0.028), a positive wake-up test (HR, 0.216; P < 0.001), and no recovery of descending neurogenic evoked potentials (DNEPs) (HR, 0.162; P < 0.001). A nomogram based on osteotomy grade, wake-up test, and DNEP recovery status was established to predict 2-year neurological function.
Conclusions
Overall, patients with severe spinal deformities who experienced significant IONM alarms demonstrated gradual neurological improvement over the 2-year follow-up. Osteotomy grade, wake-up test results, and DNEP recovery status were identified as valuable predictors that could facilitate surgical decision-making, prognostication, and counseling.
Introduction
Corrective surgery for severe spinal deformities often requires three-column osteotomy and poses a great risk of iatrogenic spinal cord injury.1-3 Intraoperative neurophysiological monitoring (IONM) is a common method for monitoring real-time neurological status and detecting impending neurological injury during scoliosis surgery. 4 Previous studies have shown that IONM, including somatosensory-evoked potential (SSEP), motor-evoked potential (MEP), and descending neurogenic-evoked potential (DNEP), can ensure neurological safety and improve overall outcomes.5,6 SSEPs are used to monitor afferent sensory conduction in the dorsal columns, excluding motor function. 7 MEPs can be used to directly monitor the corticospinal pathways of the spinal cord, which are more sensitive to spinal cord ischemia.
However, MEP has been reported to have a high false-positive rate owing to its vulnerability to systematic confounders, such as hypotension, hypothermia, and general anesthesia, especially inhalation anesthetics.8-10 When MEP-positive events are encountered, surgeons must first rule out these non-operative factors and then reverse high-risk surgical maneuvers (such as screw insertion, osteotomy, and correction). 11 Different from SSEP and MEP, DNEPs measure peripheral nerve antidromic sensory signals resulting from spinal cord level stimulation. 12 Despite containing only afferent spinal path way information, this response has proven very sensitive to changes in spinal cord function in a variety of surgical procedures. 13 In a 23-year review of 3436 pediatric spinal surgery cases, DNEPs accurately predicted postoperative neurologic deficits, with a single failure among 74 documented deficits. 14 Thus, Sutter et al found that multimodal IONM was more effective and accurate than unimodal monitoring in assessing spinal cord and nerve root functions during complex spinal surgeries, reducing both neurological complications and false-negative findings. 15 In brief, multimodal IONM is the gold standard for avoiding permanent neurological insults during correction surgeries for severe spinal deformities.16,17
Recently, researchers have reported that SSEPs and MEPs can serve as biomarkers for predicting postoperative neurological status. 18 Gorijala et al found that intraoperative SSEP monitoring can predict the risk of perioperative neurological injury during correction surgery for idiopathic scoliosis (IS) in the pediatric age group (≤21 years). 19 Coeur et al concluded that bilateral complete loss of SSEPs and MEPs had the highest likelihood of prolonged postoperative neurological deficits in children whose correction surgery was aborted due to IONM loss. 20 Wang et al described the phenomenon of significant MEP alerts (80-95% amplitude loss) associated with high-risk maneuvers but without complete disappearance in some complicated pediatric spine deformity surgeries. 21 They found that the rate of postoperative neural complications was relatively low in this patient group. Therefore, MEP signal survival may be used to predict non-permanent paraplegia. However, these studies mainly focused on the prediction of new neurological deficits that occurred immediately postoperatively. The evolution of insulted neurological function during long-term follow-up has seldom been investigated.
In patients with severe spinal deformities, significant MEP alerts are frequently observed during high-risk surgical interventions, indicating possible disruption of normal neural function. 13 The reversibility of these IONM alerts has an impact on subsequent recovery from postoperative neurological deficits. 22 Therefore, diligent clinical follow-up is imperative to ascertain the ultimate neurological prognosis in this patient population. In this study, we report the longitudinal neurological outcomes of 115 patients who encountered significant MEP alerts during correction surgeries for severe spinal deformities and identify factors for the prognosis of long-term neurological outcomes.
Materials and Methods
Study Cohort
This single-center retrospective cohort study was approved by the Institutional Review Board of our hospital (approval no. XHEC-D-2024-102). We reviewed 2772 patients who underwent scoliosis correction surgery between May 2008 and April 2022 at our center. The inclusion criteria were as follows: (1) severe spinal deformities (Cobb’s angle of scoliosis or kyphosis >90°); (2) three-column osteotomy in the thoracic spinal region; (3) complete multimodal IONM data, including SSEP, MEP, and DNEP; (4) significant MEP alerts after ruling out systematic and non-operative factors; and (5) more than 2 years of follow-up. Patients who had preoperative neurological symptoms, prior spinal surgeries, or were lost to follow-up were excluded. A detailed flowchart of the study is shown in Figure 1. All surgeries were performed by the same team and monitored by an electrophysiologist. No notable changes in instrumentation, neuromonitoring protocols, or surgical techniques were observed in our center during the study period. This study was conducted in accordance with the principles of the Declaration of Helsinki, and all patients and their parents signed an informed consent form. Flowchart of the Patients Included in This Study
Anesthesia
To avoid interference from inhaled anesthetics in intraoperative neuromonitoring, especially MEPs, all patients in this study were treated with total intravenous anesthesia throughout the process.23,24 Routine anesthesia induction involved the use of 1.5-2 mg/kg propofol, 3-5 µg/kg fentanyl, and 0.15-0.2 mg/kg muscle relaxants (commonly used cisatracurium). Intraoperative anesthesia was maintained with remifentanil (0.2-0.5 µg/kg/min) and propofol (5-6 mg/kg/h). During anesthesia induction, muscle relaxants were used to assist tracheal intubation, and no or a small amount of muscle relaxants was used throughout the surgery to reduce the inhibitory effect of muscle relaxants on MEPs.
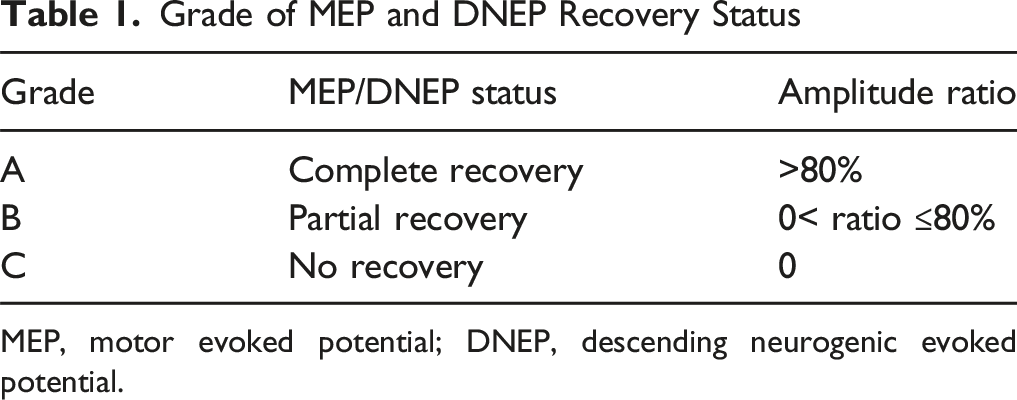
Multimodal IONM
Multimodal IONM, including SSEP, MEP, and DNEP, was performed in all patients. A significant MEP alarm was defined as the absence of MEP amplitude in the unilateral or bilateral lower extremities, despite attempts to record with increased stimulation intensity after excluding non-operative and systemic factors, and as no restoration of MEP amplitude within 10 minutes. SSEP positivity was defined as a 50% reduction in amplitude or a 10% increase in latency. DNEP positivity was defined as an 80% reduction in amplitude or a 10% increase in latency compared with baseline. IONM status was also recorded after reversible interventions to rescue the significant alarms. An amplitude exceeding 80% of the baseline value indicated complete recovery, a value less than 80% signified partial recovery, and a ratio of 0 indicated no recovery (Figure 2). Thus, the MEP and DNEP recovery status was categorized into 3 grades: A, complete recovery; B, partial recovery; and C, no recovery (Table 1). In cases of discordant bilateral MEP/DNEP recovery, the poorer outcome was recorded as the final grade. Illustration of the MEP Recovery Status. (A) Grade A: Complete Recovery; (B) Grade B: Partial Recovery; (C) Grade C: No Recovery Grade of MEP and DNEP Recovery Status MEP, motor evoked potential; DNEP, descending neurogenic evoked potential.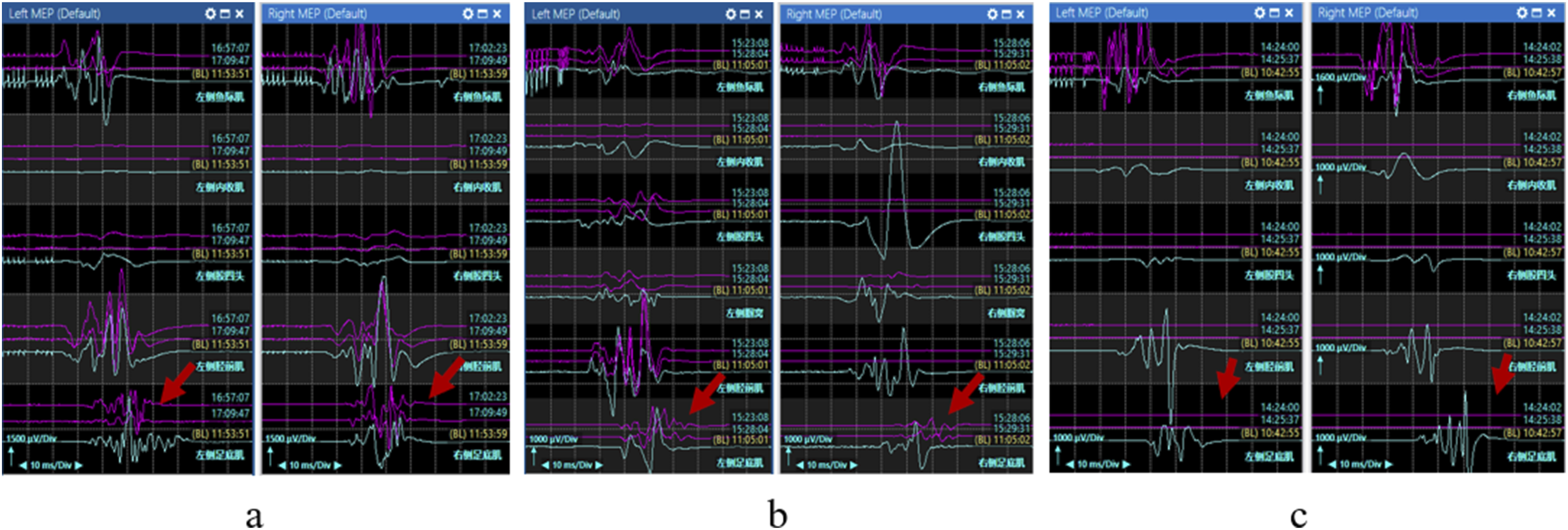
Standardized Procedures for MEPs Alarms
When MEPs alarms occur intraoperatively, we perform the standardized procedures as described below6,11: (1) stop the operation intraoperatively and examine the equipment faults; check the current anesthesia and physiological status; and appropriately increase the blood pressure and reduce the anesthesia depth; (2) inject high-dose methylprednisolone intravenously when monitoring alarms persist; (3) check the tension of spinal cord tissue and decompress the tension appropriately if necessary; (4) perform the wake-up test if monitoring alarms persist; (5) if the wake-up test is positive, loosen the regional internal fixator, and perform an O-arm examination if necessary; (6) perform laminectomy and decompression on the areas where spinal cord compression might exist; in the meantime, remove the internal fixation while maintaining the spinal stability until MEP amplitude improves; and (7) if the MEP amplitude remains unimproved, serious neurological complication might be expected and the operation should be terminated with the remaining fixation left in situ, as illustrated in representative case 2. The observation time after each check step usually took 1-2 minutes. After surgery, comprehensive management is required for these patients, including spinal MRI assessment, neurotrophic medicine, hyperbaric oxygen treatment, acupuncture therapy and physical rehabilitation. If a compressive intraspinal hematoma is detected on spinal MRI, a second surgery is performed.
Clinical Evaluations
Clinical information, including age, sex, diagnosis, Cobb’s angles of scoliosis and kyphosis, osteotomy grade, surgical time, estimated blood loss, and IONM data, was collected. The osteotomy grade was determined using the classical Schwab classification. 25 Before surgery, all patients underwent a thorough assessment of the neurological system, including sensory perception, limb strength, abdominal reflexes, and tendon reflexes, to detect potential neurological deficits. 26 Postoperative spinal cord function was evaluated according to the American Spinal Injury Association (ASIA) classification. 27 Grade E indicated intact neurological function, whereas grades A-D indicated different degrees of neurological deficits. Neurological function status was assessed immediately after surgery and at 3 days, 7 days, 15 days, 1 month, 3 months, 6 months, 1 year, and 2 years postoperatively.
Statistical Analysis
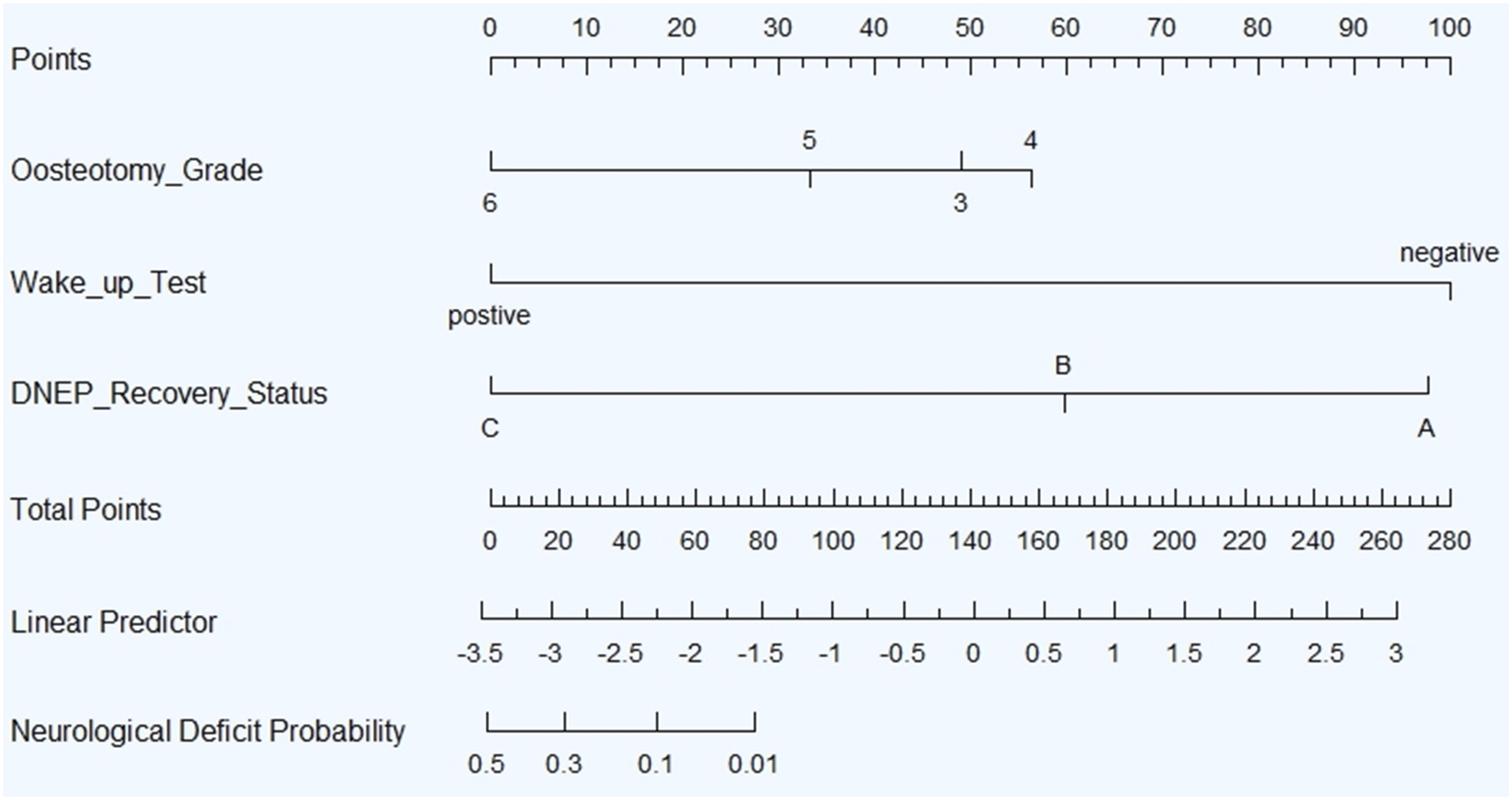
The distribution of variables is presented as mean ± standard deviation. Two-tailed Student’s t-tests were used to compare continuous data, and Pearson’s chi-square or Fisher’s exact tests were used for dichotomous data analyses. Cox regression analysis was performed to identify prognostic variables that could predict long-term neurological survival. All tests were performed using SPSS (version 22, Chicago, Illinois, USA), and P < 0.05 was considered statistically significant. A nomogram interpreting the Cox regression model findings was generated to predict the 2-year neurological function.
Results
Baseline Characteristics
Baseline Information of Enrolled Patients

IONM Data
Neurophysiological Monitoring Data
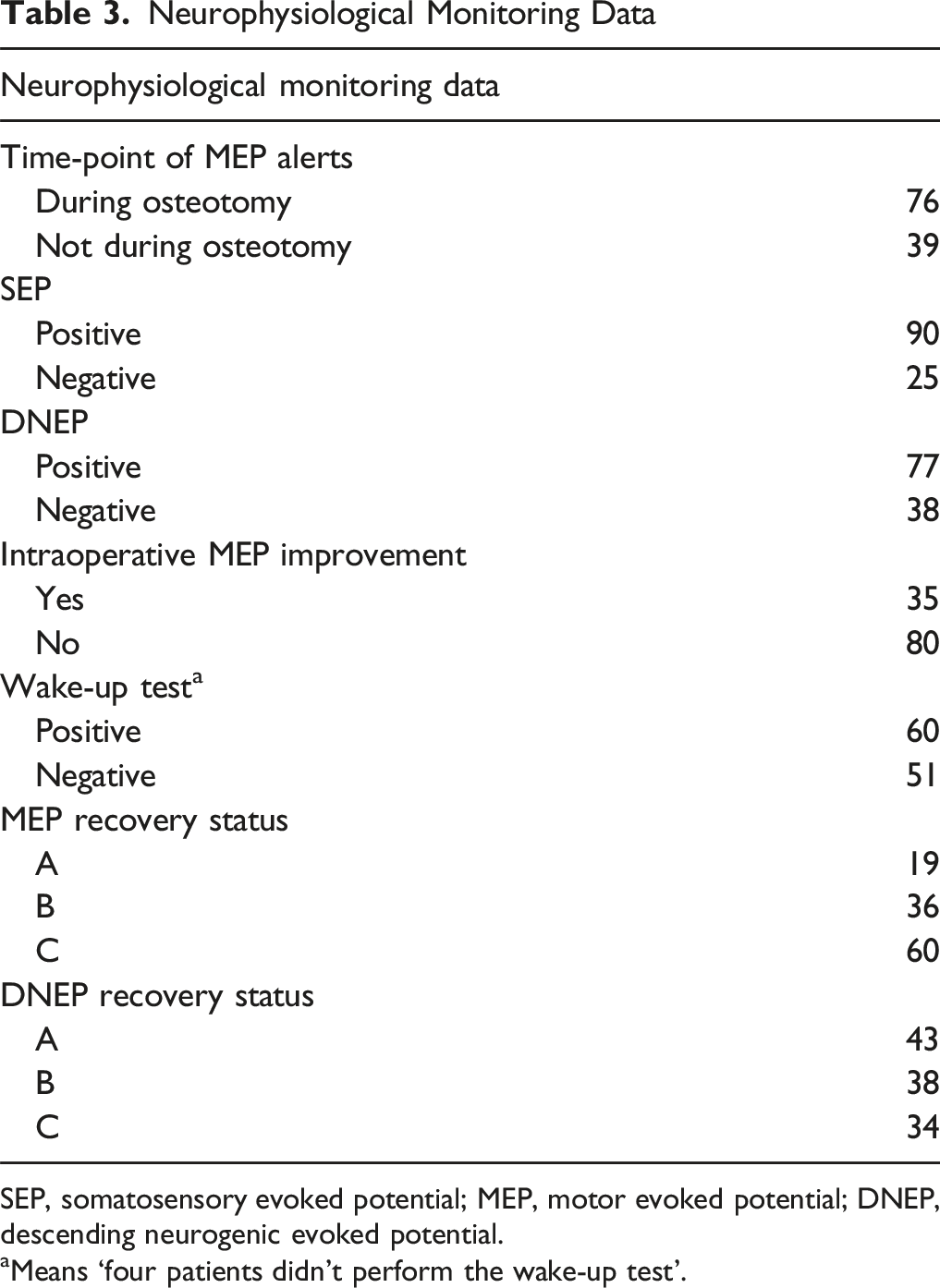
SEP, somatosensory evoked potential; MEP, motor evoked potential; DNEP, descending neurogenic evoked potential.
aMeans ‘four patients didn’t perform the wake-up test’.
Prognosis of Long-Term Neurological Outcomes
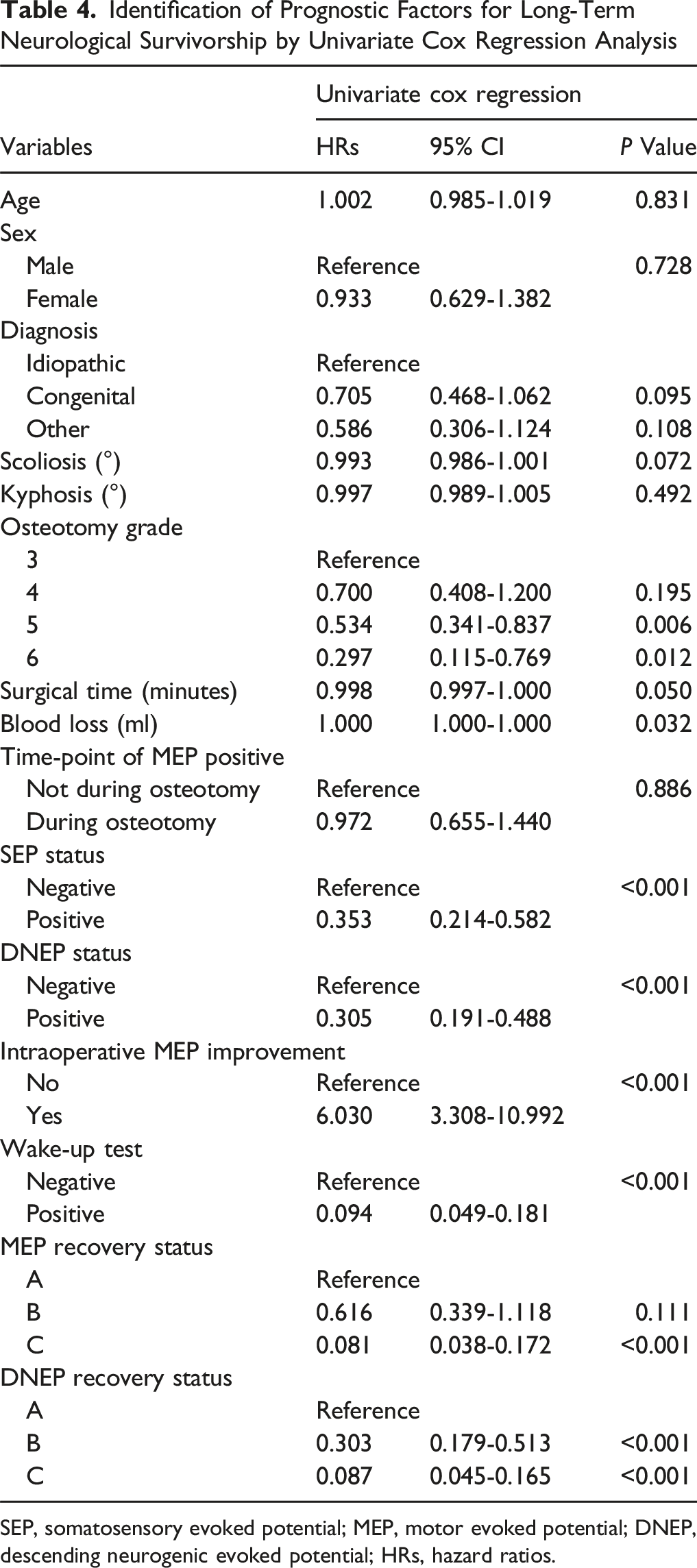
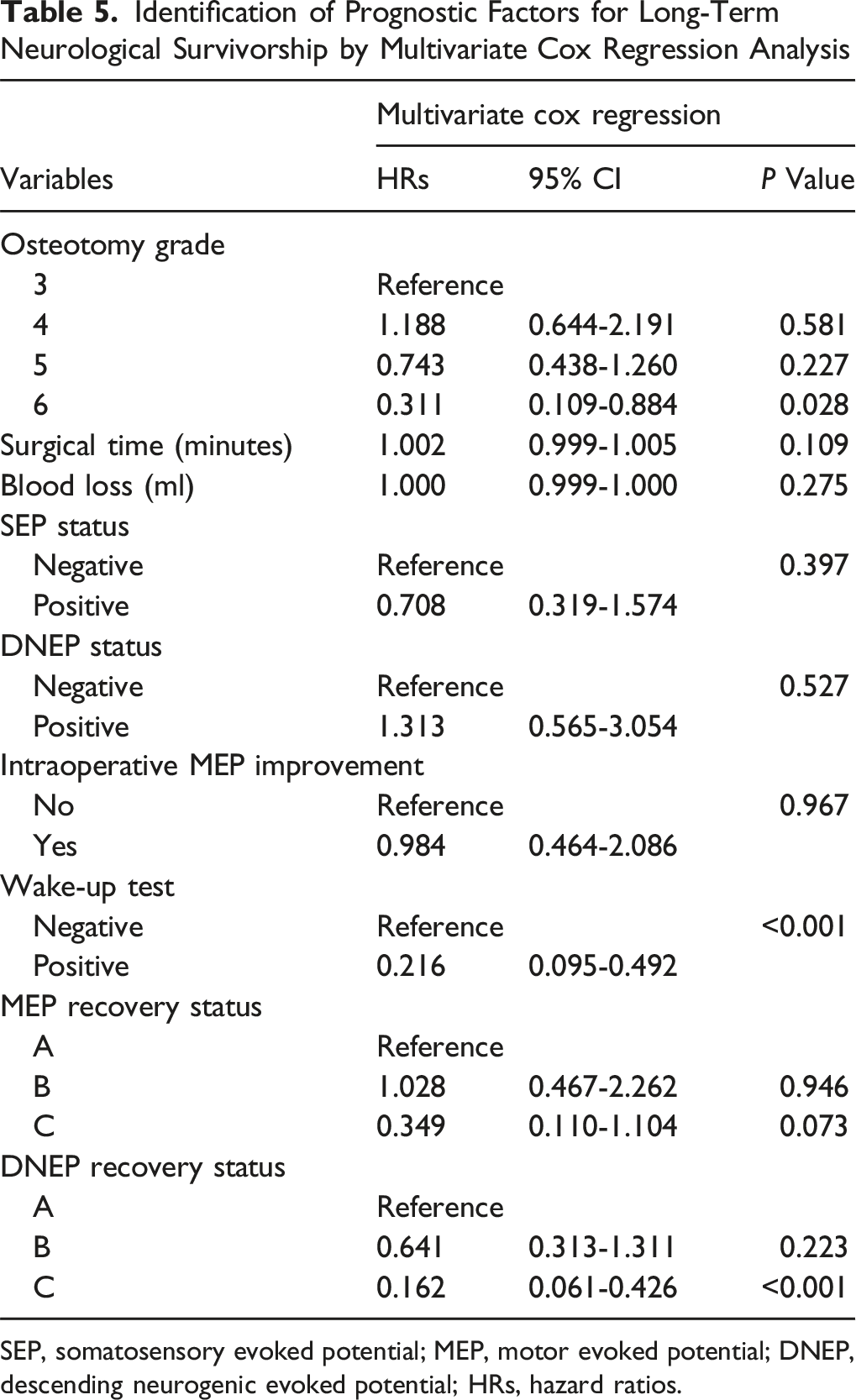
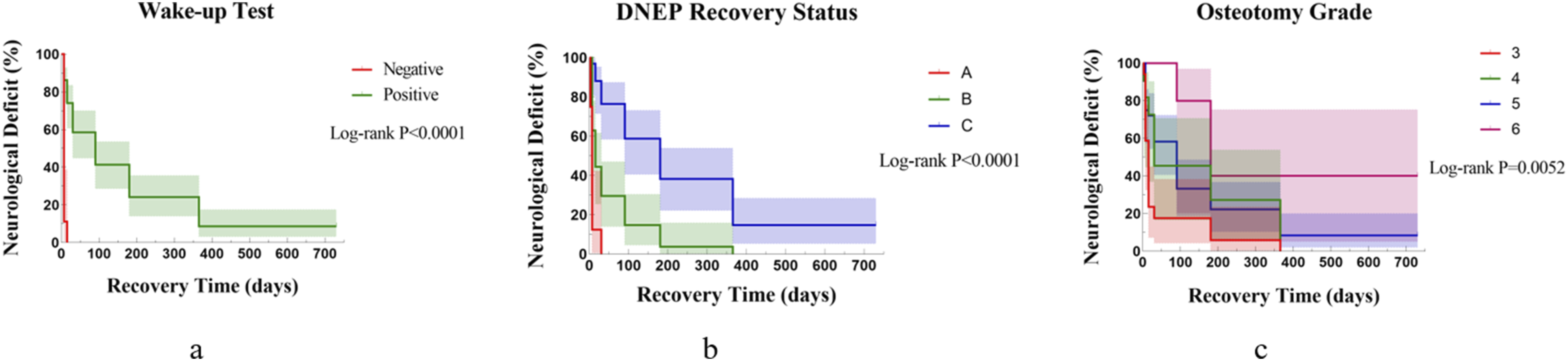
Immediately after surgery, 49.6% (57 patients) displayed neurological deficits, which decreased to 47.0% (54 patients) at 3 days, 44.3% (51 patients) at 7 days, 29.6% (34 patients) at 1 month, 20.9% (24 patients) at 3 months, and 12.2% (14 patients) at 6 months. By the 1-year follow-up, only 5 patients (4.3%) had not recovered, and this finding remained stable at the 2-year follow-up (Figure 3). To investigate the predictors of long-term neurological survivorship, Cox regression analysis was performed considering both neurological status and recovery time over a 2-year follow-up. Univariate Cox regression analysis revealed nine factors that were significantly associated (P < 0.05): osteotomy grade, surgical time, blood loss, SEP status, DNEP status, intraoperative MEP improvement, wake-up test, and MEP and DNEP recovery status (Table 4). Subsequently, multivariate Cox regression analysis incorporating these factors identified osteotomy grade, wake-up test results, and DNEP recovery status as independent prognostic factors (Table 5). Specifically, patients with grade six osteotomy exhibited a 68.9% reduction in the likelihood of long-term intact neurological function (HR, 0.311; P = 0.028). Similarly, a positive wake-up test (HR, 0.216; P < 0.001) and absence of DNEP recovery (HR, 0.162; P < 0.001) were associated with 78.4% and 83.8% reductions in the probability of long-term intact neurological function, respectively. The Kaplan-Meier curves for these variables highlighted their significant impact on long-term neurological survival prognosis (Figure 4). A nomogram based on the Cox regression model findings facilitated the prediction of 2-year neurological function (Figure 5). The Evolution of Postoperative Neurological Outcomes Identification of Prognostic Factors for Long-Term Neurological Survivorship by Univariate Cox Regression Analysis SEP, somatosensory evoked potential; MEP, motor evoked potential; DNEP, descending neurogenic evoked potential; HRs, hazard ratios. Identification of Prognostic Factors for Long-Term Neurological Survivorship by Multivariate Cox Regression Analysis SEP, somatosensory evoked potential; MEP, motor evoked potential; DNEP, descending neurogenic evoked potential; HRs, hazard ratios. Kaplan-Meier Curves of Three Prognostic Factors Predicting Long-Term Neurological Outcomes in Patients With Severe Spinal Deformities A Nomogram Predicting Two-Year Neurological Function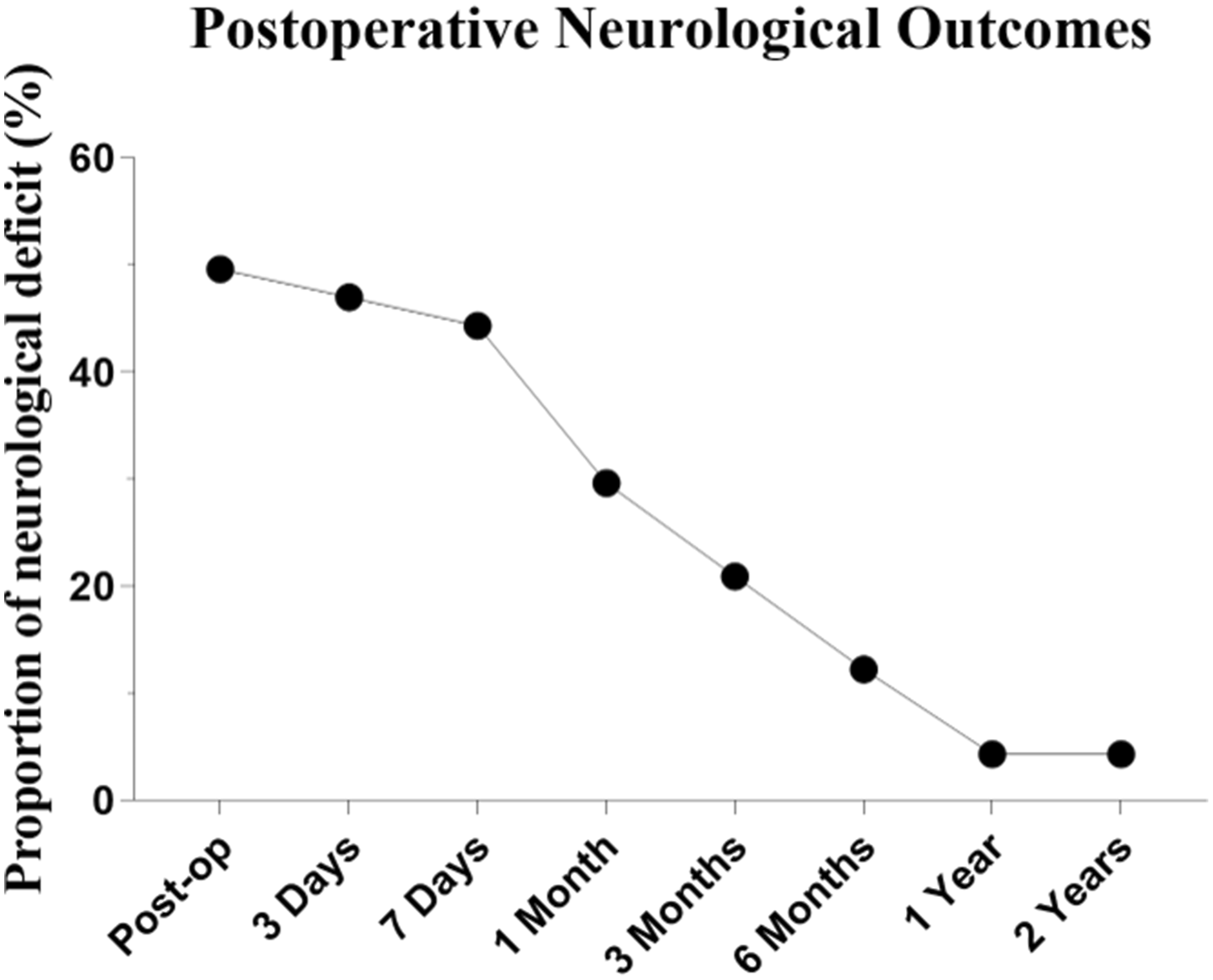
Discussion
Maintaining the integrity of the neurological system is of paramount importance during surgery for severe spinal deformities. 28 Complex surgical interventions, such as osteotomy and correction aimed at restoring normal spinal alignment, require meticulous planning and execution to mitigate the risk of potential neurological complications. Thus, careful IONM is essential to safeguard neurological function, minimize the likelihood of adverse outcomes, and optimize overall surgical success. 29 Risk factors for IONM data loss include patient factors such as larger curves with greater angular deformity and surgical factors such as longer operative time, greater blood loss, and 3-column osteotomies. 30 Besides, baseline spinal cord shape and function are also found to influence the IONM, and could help surgeons anticipate problems and guide management strategies.26,31 Despite multiple preventive strategies, patients with complex deformity still experience IONM loss and postoperative neurological deficits.
In this study, the incidence of neurological deficits immediately after surgery (49.6%) was higher than that reported in the literature. 32 This can be attributed to the fact that only patients with significant MEP alarms were included in this study. This study population presented with severe spinal deformities that posed extensive challenges during surgical intervention, and significant MEP alerts further led to the risk of neurological complications. Despite the high rate of immediate neurological deficits, most patients demonstrated remarkable recovery of neurological function during the postoperative follow-up period. At the 2-year follow-up, only 5 patients (4.3%) demonstrated permanent neurological deficits. This observation underscores the remarkable capacity of the nervous system to adapt and reorganize, even in the face of potential intraoperative insults, highlighting the importance of comprehensive rehabilitation and long-term management in optimizing outcomes. This study provides an important reference for researchers to guide neurological rehabilitation in this complex patient population with temporary deficits after corrective surgery. Understanding the potential outcomes and trajectories of neurological conditions can help to inform treatment strategies, set realistic expectations, and enable patients and their families to make informed decisions.
The clinical prognosis of long-term neurological function is crucial for both patients and healthcare providers. Neurological complications have a profound effect on patients’ quality of life, limiting mobility, independence, and overall well-being. Therefore, the primary goal of correction surgery is not only to improve normal spinal alignment but also to preserve and, ideally, enhance the patient’s neurological function. However, there is a dearth of research exploring the predictors of long-term neurological survival. This study demonstrated for the first time that osteotomy grade, wake-up test, and DNEP status were significant prognostic factors for long-term neurological survivorship. From the Kaplan-Meier curves, it could be seen that grade 6 osteotomy, positive wake-up test, and no DNEP recovery significantly correlated with a poorer neurological recovery.
According to previous literature, MEPs are vulnerable to anesthetics, hypotension, and other systematic factors during neurological monitoring, leading to a relatively high false-positive rate of MEPs.
33
To decrease the rates of false-positive MEPs, we routinely monitor DNEPs as supplements to MEPs in patients with severe spinal deformities. Previous studies concluded that DNEP could be regarded as an important auxiliary tool to assist MEP in monitoring intraoperative neurological injury and could serve as a temporary substitution monitoring technique after MEP is lost during surgery for severe spinal deformity.14,34,35 Chen et al demonstrated that patients in the DNEP-negative group showed greater MEP improvement than those in the DNEP-positive group (81.5% vs 53.2%).
36
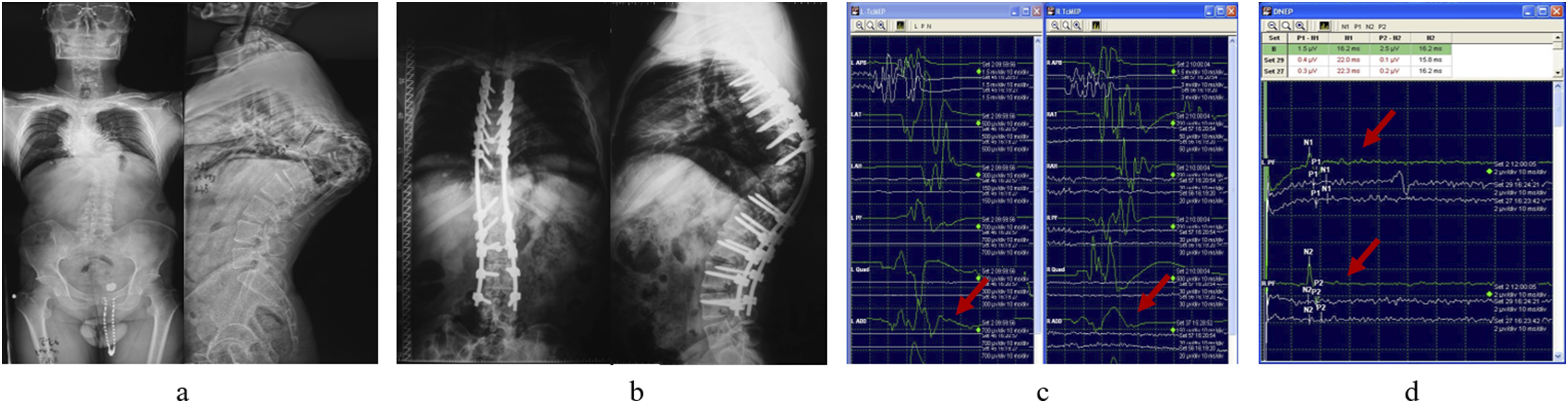
Therefore, MEP-positive cases with negative DNEP results might have a better prognosis for neurological outcomes. Our study showed that postoperative DNEP statuses indicated distinctive neurological recovery conditions. For example, when a patient underwent a positive wake-up test and had no recovery of postoperative MEP status, neurological recovery was still possible if the postoperative DNEP status was good (Figure 6). However, if all three factors were positive, serious neurological sequelae seemed inevitable (Figure 7). With these prognostic factors in mind, surgeons can better predict neurological outcomes and guide rehabilitation more effectively. Representative Case 1. (A) A 20-Year-old Girl With Idiopathic Scoliosis. The Preoperative Scoliosis and Kyphosis Were 155 and 165 Degrees, Respectively. (B) She Received T9-10 VCRs. The Postoperative Scoliosis and Kyphosis Were 52 and 64 Degrees, Respectively. (C) At the End of Surgery, MEPs Showed Complete Loss in the Left Lower Limb (Grade C) and Obvious Weakness in the Right Lower Limb (Grade B). (D) Immediately after Surgery, However, DNEP was Nearly Normal (Grade A). This Patient Developed Neurological Deficits after Surgery, With Muscle Strength of the Left Lower Limb Ranking Grade 0 and Right Lower Limb Ranking Grade 4. Seven Days after Surgery, the Muscle Strength of the Right Lower Limb Recovered to Grade 5. One Month after Surgery, the Left Lower Limb Also Returned to a Normal Level. The Neurological Function Remained Stable at the Two-Year Follow-Up Representative Case 2. (A) A 44-Year-old Man was Diagnosed With Tuberculosis-Associated Kyphosis. The Preoperative Kyphosis was 130 Degrees. (B) He Received T9-11 VCRs. The Postoperative Kyphosis was 78 Degrees. (C) At the End of the Surgery, MEPs Showed Complete Disappearance in Both Lower Limbs (Grade C). (D) DNEP Also Showed Complete Disappearance at the End of Surgery (Grade C). This Patient had Catastrophic Neurological Complications. The Muscle Strength of Both Lower Limbs was Grade 0 after Surgery and did Not Recover after the Two-Year Follow-Up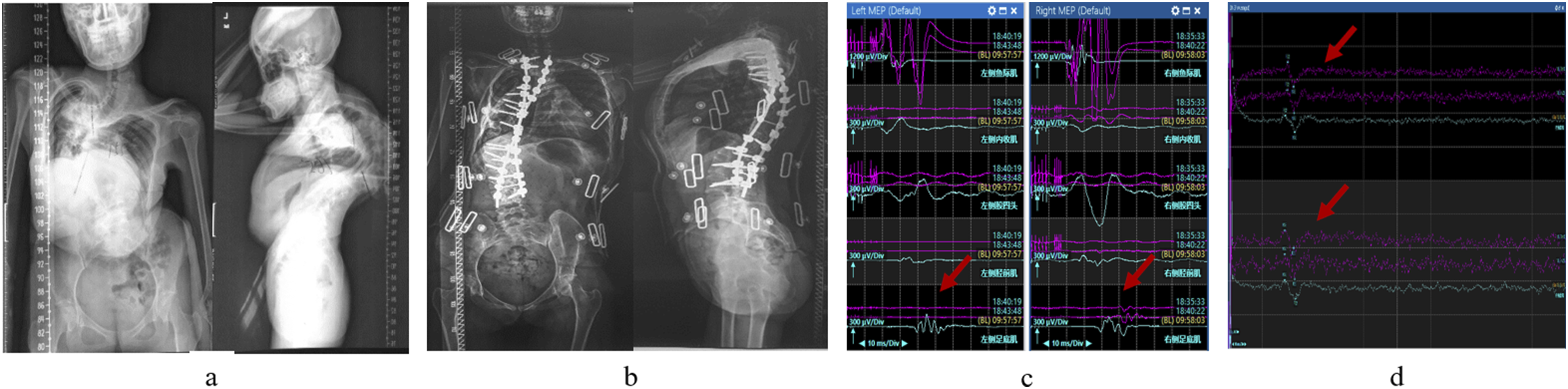
This study had several limitations. First, this was a retrospective analysis with an inherent possibility of data inaccuracy, and potential selection and information biases might exist due to the single-center design. Second, owing to the low incidence of severe spinal deformities, the sample size was relatively small. More cases are required to compare patients with different etiologies and eliminate underlying confounders. Third, although this study found the relationship between DNEP monitoring and long-term neurological outcomes, but it failed to explain the underlying mechanism. Lastly, multi-center research is required to validate its clinical utility.
Conclusions
This is the first study to report the longitudinal neurological outcomes in patients with severe spinal deformities who have significant intraoperative neuromonitoring alerts. Overall, neurological function gradually improves during the 2-year follow-up. Osteotomy grade, wake-up test results, and DNEP recovery status serve as critical predictors for prognosticating long-term neurological outcomes in clinical practice. Therefore, the appropriate osteotomy grade should be determined preoperatively, and prompt surgical maneuvers should be implemented intraoperatively to restore positive wake-up test results or DNEP signals. Together, these parameters provide clinicians with a basis for evidence-based counseling of patients and their families regarding recovery expectations and the necessity of subsequent rehabilitation.
Footnotes
Ethical Considerations
This study was conducted in accordance with the principles of the Declaration of Helsinki, and all patients and their parents signed an informed consent form.
Funding
This work was supported by the National Key Research and Development Program of China (Research on prevention and treatment of common frequently-occurring diseases / 2023YFC2507702), the National Nature Science Foundation of China (82472789) and Yunnan Province Science/Technology Talent and Platform Plan Project (No. 202205AF150062).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.