
Abstract
Study Design
Retrospective cohort study.
Objective
To evaluate the impact of age ≥75 years on postoperative complications and sagittal alignment following open transforaminal lumbar interbody fusion (TLIF).
Methods
A retrospective review was performed for patients undergoing primary open TLIF from 2017 to 2021. Patients were divided into 2 cohorts: age <75 and ≥75 years. Groups were 1:1 propensity score matched based on gender, body mass index (BMI), hypertension, diabetes, and Charlson Comorbidity Index (CCI). Radiographic sagittal parameters were analyzed preoperatively and at 1 year postoperatively. Complication rates, including reoperations, adjacent segment disease, and subsidence, were compared between matched cohorts.
Results
Prior to the PSM, a total of 489 patients fit the initial exclusion criteria with 448 in the younger (18-75 years) cohort and 40 in the older (≥75 years) cohort. After matching, 80 patients were included (40 per group) with no significant differences in demographics or perioperative variables. Postoperative radiographic parameters were similar between groups. The overall complication rates were comparable (P = 0.546). However, elderly patients experienced significantly higher rates of revision surgery (27.5% vs 5.7%, P = 0.013).
Conclusion
Patients ≥75 years old achieved similar radiographic alignment and experienced comparable complication rates following open TLIF. However, they may be at greater risk for revision surgery. These findings support the safety and effectiveness of open TLIF in elderly patients, though larger and longer-term studies are needed to further define outcomes in this population.
Level of Evidence
III.
Keywords
Introduction
Open transforaminal lumbar interbody fusion (TLIF) was initially developed to refine more traditional posterior fusion techniques to reduce the need for nerve manipulation while still achieving interbody fusion.1,2 Given its vetted safety and efficacy profile, open TLIF is a commonly used technique to treat degenerative spinal conditions, such as degenerative disc disease and spinal stenosis, in patients that failed conservative management.3,4 As the population continues to age, the demand for such surgical interventions is expected to rise. The United States Census Bureau estimates that the number of Americans ages 65 and older will increase from 58 million in 2022 to over 80 millions by 2050. 5 Eventually, this will contribute to a greater prevalence of age-related degenerative spinal disease requiring surgery, given the several physiologic changes associated with aging.6-8 Unsurprisingly, models predict that there will be an increased number of spinal fusion performed in patients 75 years and older. 9 As more elderly patients present with conditions requiring surgical correction, it becomes critical to evaluate the safety and efficacy of common surgical techniques.
While TLIF has been well-studied in the current literature, many surgeons are hesitant to perform TLIF in the very elderly population (>75), due to concerns for increased surgical time, greater blood loss, and poor bone quality. Some surgeons will opt for fusion without interbody placement or decompression alone in this patient population.10,11 While the age >65 population has been well studied, 10 There is little information on the outcomes of very elderly patients (age >75). 11 Beyond clinical outcomes, radiographic sagittal parameters are largely unexplored in elderly open TLIF patients, despite the data demonstrating their impact on long-term outcomes.12-16 Preserving or restoring sagittal parameters, such as pelvis incidence-to-lumbar lordosis (PI-LL) mismatch, has been shown to correlate with improved postoperative quality of life and reduced risk adjacent segment disease (ASD).12,13,15-17 However, few studies have included sagittal parameters as studied outcomes when looking at the effect of age on outcomes following TLIF. Additionally, no studies have used matched cohorts to control for key confounders that affect elderly populations, such as comorbidity burden and body mass index (BMI).
The aim of this study was to determine the impact of age ≥75 years on complication rates and sagittal radiographic measurements following open TLIF. We suspected that older patients would present with worse preoperative alignment, but that similar postoperative correction or preservation would be achieved. By propensity-matching several potential cofounders, this study better isolates the impact of age on outcomes following open TLIF.
Methods
Ethical Approval
This study was reviewed and approved by the Lifespan Institutional Review Board 2 (#00004624). A general waiver of informed consent was granted in accordance with 45 CFR 46.116(f)(1).
Procedure Description
All TLIF procedures were open with interbody and bilateral posterolateral fusion. After exposure, pedicle screws were inserted under fluoroscopic guidance. All TLIF procedures were performed via a unilateral transforaminal approach with facetectomy and full central canal decompression. Complete laminectomy was performed. Unilateral complete facetectomy was then performed with burr and osteotome. Discectomy was performed and morcellized local autograft and allograft, made of cancellous bone matrix and chips, were placed into the disc space. Trials were introduced to size the interbody implant, and then an oblique titanium static or expandable “bullet” cage filled with autograft and demineralized bone matrix (DBM) was inserted into the disc space under fluoroscopy to the front of the disc space. Autograft and DBM were then placed over decorticated posterolateral surfaces, and rods were inserted into screw tulips and locked in place with set caps after gentle compression.
Patient Population
This retrospective cohort study was approved by our Institutional Review Board (IRB). We reviewed a dual-institution database to identify cases of open transforaminal lumbar interbody fusion (TLIF) that occurred between 2017 and 2021. Only primary elective open TLIF procedures were included in this analysis. Patients were excluded if they were missing age data or carried a diagnosis of metastatic cancer or severe kidney disease. Also, patients were excluded if radiographic measurement data was not complete in the database, without at least 1 year follow-up. After all inclusion and exclusion criteria were applied, eligible patients were split into 2 cohorts of either age 18-74 (Younger) or age ≥75 years (Older). To mitigate baseline differences between groups, 1:1 propensity score matching was performed.
Data Collection
Retrospectively, demographic and perioperative data was extracted from the database. Demographic variables included age, gender, and BMI. Comorbidities such as hypertension and diabetes were also recorded, along with the CCI score. Perioperative data included the number of levels fused, operative time, estimated blood loss (EBL), length of hospital stay (LOS), and the rate of in-hospital complications.
Radiographic Measurements
Radiographic measurements were taken from lateral radiographs at 2 key intervals - preoperative and 1-year postoperative. Several different measurements were tracked including lumbar lordosis (L1-S1), segmental lordosis of L4-S1 (L4-S1), apex of the lumbar curvature (L1-S1 Apex). Other key parameters included pelvic tilt (S1PT), sacral slope (S1SS), and pelvic incidence – lumbar lordosis mismatch (PI-LL).18-20
Statistical Analysis
Stata version 18.5 (StataCorp, College Station, TX) was used to complete all statistical analyses in this study. The significance cutoff was set at P < 0.05. Before comparing differences in variables between the groups, a 1:1 nearest-neighbor propensity score matching (PSM) was done based on gender, BMI, CCI scores, hypertension, and diabetes status. The propensity scores were calculated using a logistic regression model with age ≥75 as the dependent variable and the aforementioned variables as independent covariates. The calculated propensity scores were then used to match each older patient (age ≥75) to a younger patient with the closest propensity score. Covariate balance was evaluated using standardized mean differences (SMDs) and variance ratios. Bias was considered acceptable if it remained below 15%, and variance ratios were deemed satisfactory within the range of 0.5-2.0. The final matched dataset demonstrated excellent balance across all covariates, confirming the success of the matching process. After successful matching, common statistical comparisons were made between the 2 refined cohorts. Differences between continuous variables, such as age, BMI, and radiographic measurements, were analyzed using Student's t-tests. Categorical variables, including gender and comorbidity status were compared using chi-square tests. Due to small observation counts and to ensure statistical validity, complications rates were compared using Fisher’s exact tests.
Results
Patient Demographics - Unmatched
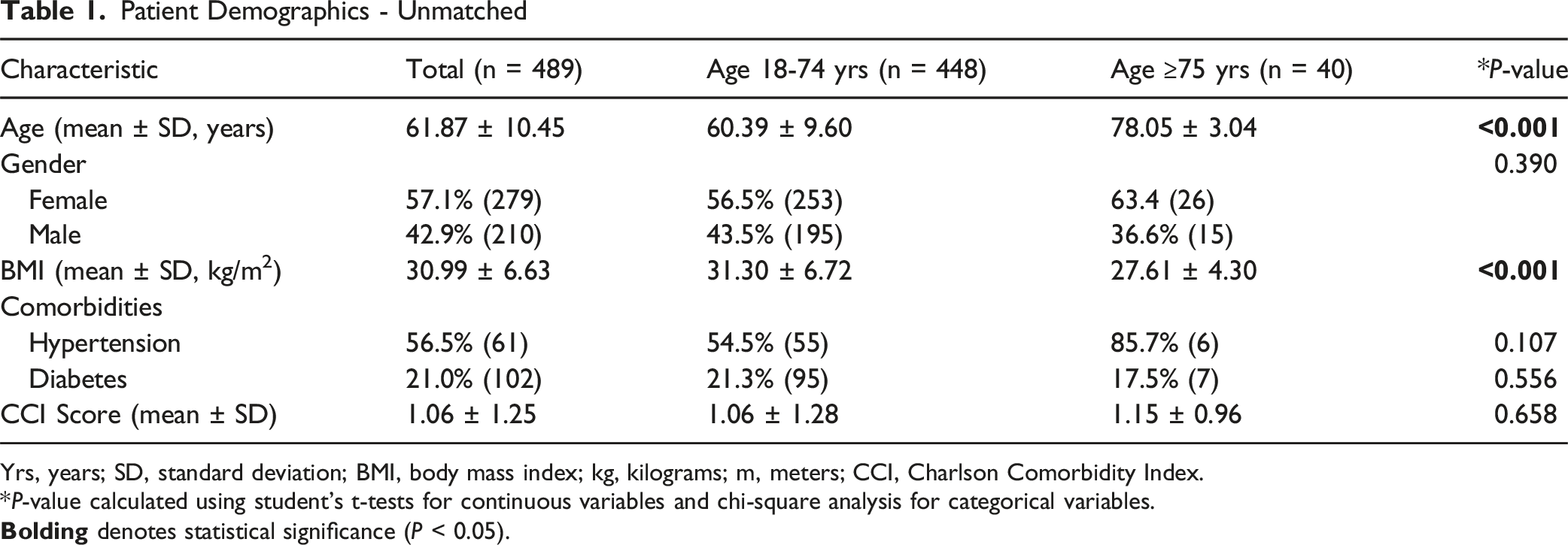
Yrs, years; SD, standard deviation; BMI, body mass index; kg, kilograms; m, meters; CCI, Charlson Comorbidity Index.
*P-value calculated using student’s t-tests for continuous variables and chi-square analysis for categorical variables.
Perioperative Characteristics - Unmatched
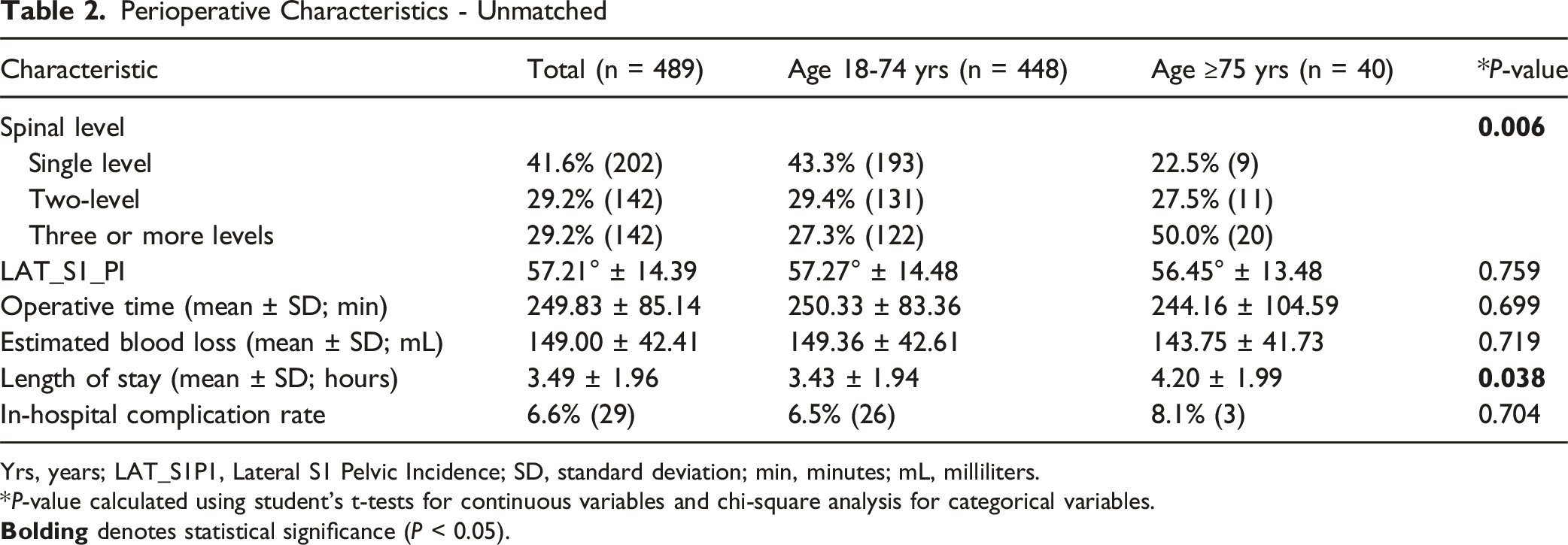
Yrs, years; LAT_S1P1, Lateral S1 Pelvic Incidence; SD, standard deviation; min, minutes; mL, milliliters.
*P-value calculated using student’s t-tests for continuous variables and chi-square analysis for categorical variables.
Patient Demographics - Matched
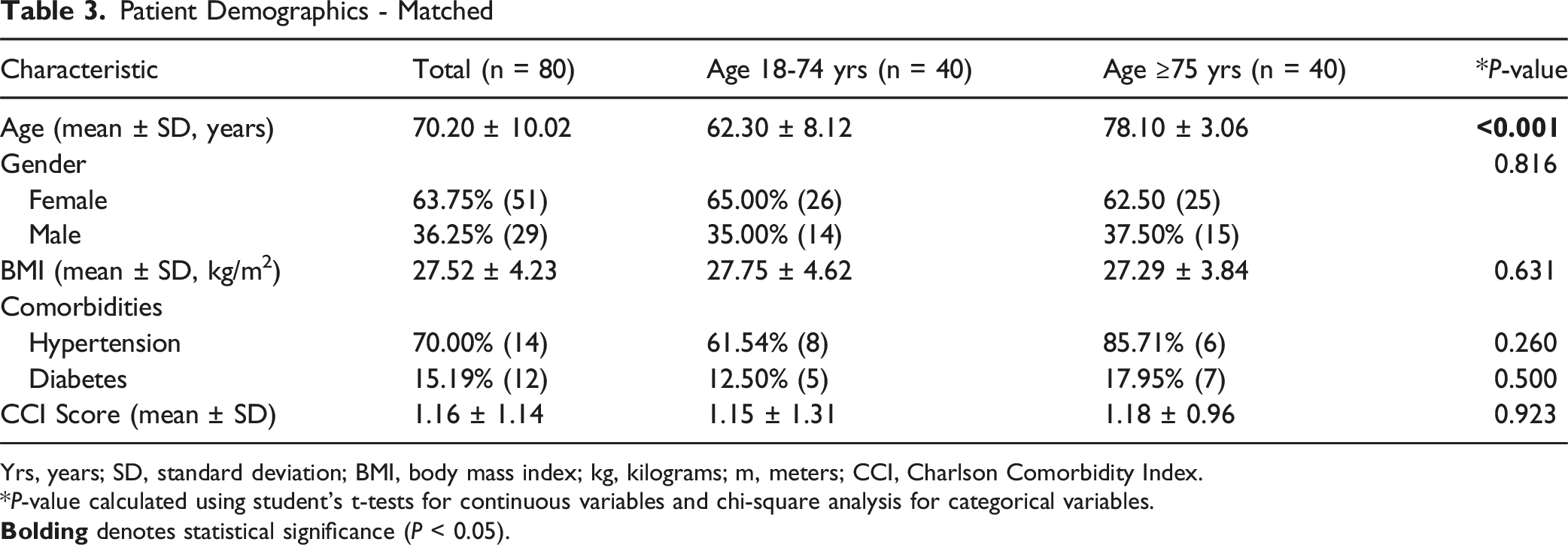
Yrs, years; SD, standard deviation; BMI, body mass index; kg, kilograms; m, meters; CCI, Charlson Comorbidity Index.
*P-value calculated using student’s t-tests for continuous variables and chi-square analysis for categorical variables.
Perioperative Characteristics - Matched
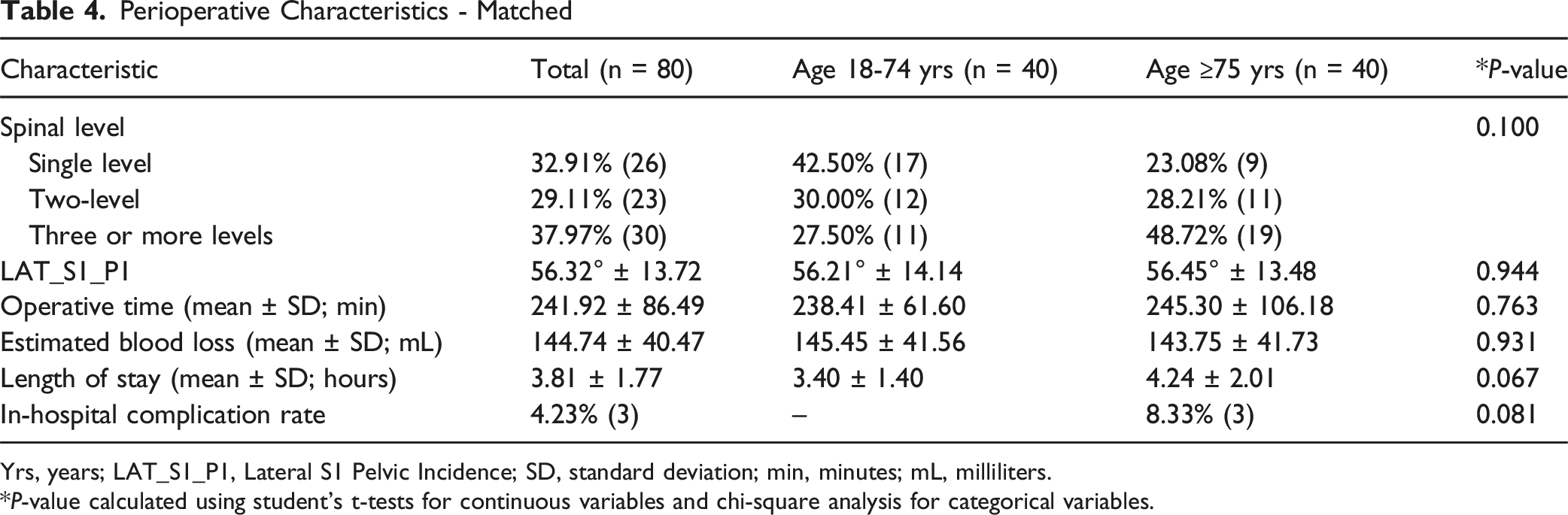
Yrs, years; LAT_S1_P1, Lateral S1 Pelvic Incidence; SD, standard deviation; min, minutes; mL, milliliters.
*P-value calculated using student’s t-tests for continuous variables and chi-square analysis for categorical variables.
Complication Rates - Matched
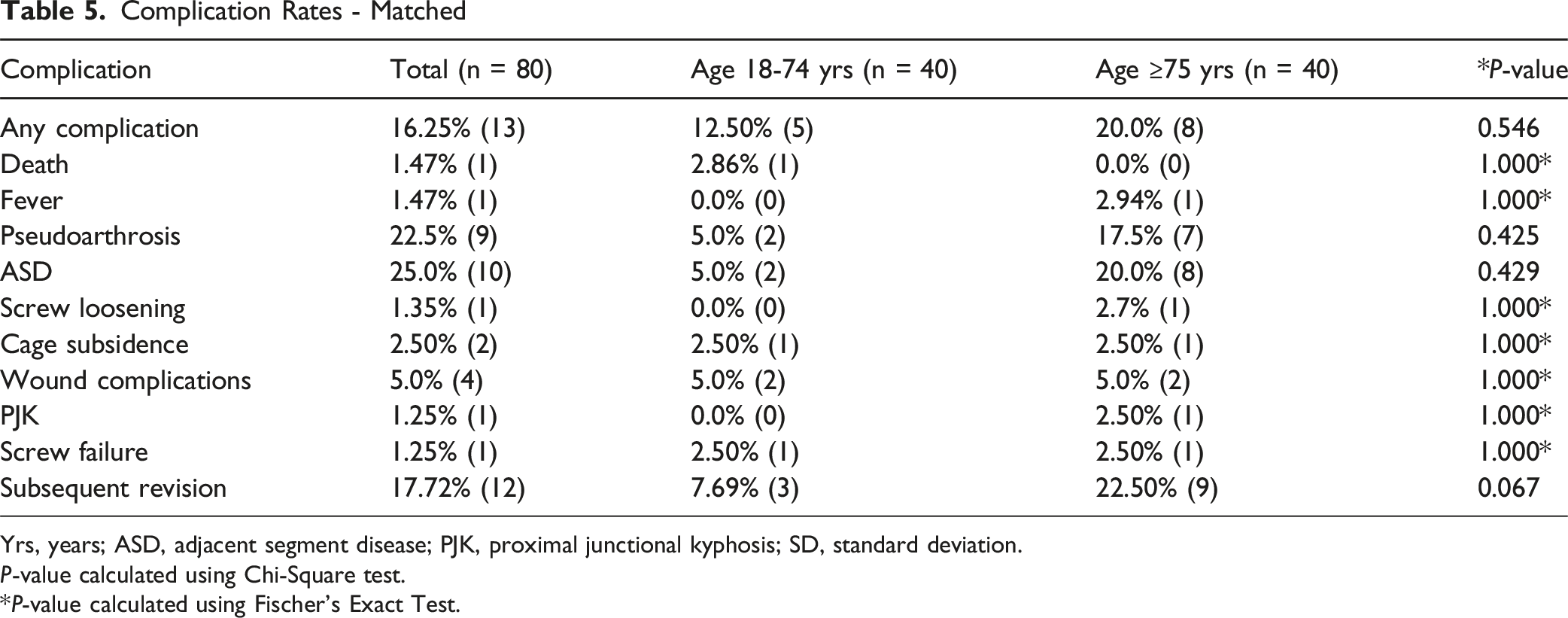
Yrs, years; ASD, adjacent segment disease; PJK, proximal junctional kyphosis; SD, standard deviation.
P-value calculated using Chi-Square test.
*P-value calculated using Fischer’s Exact Test.
Reasons for Revision
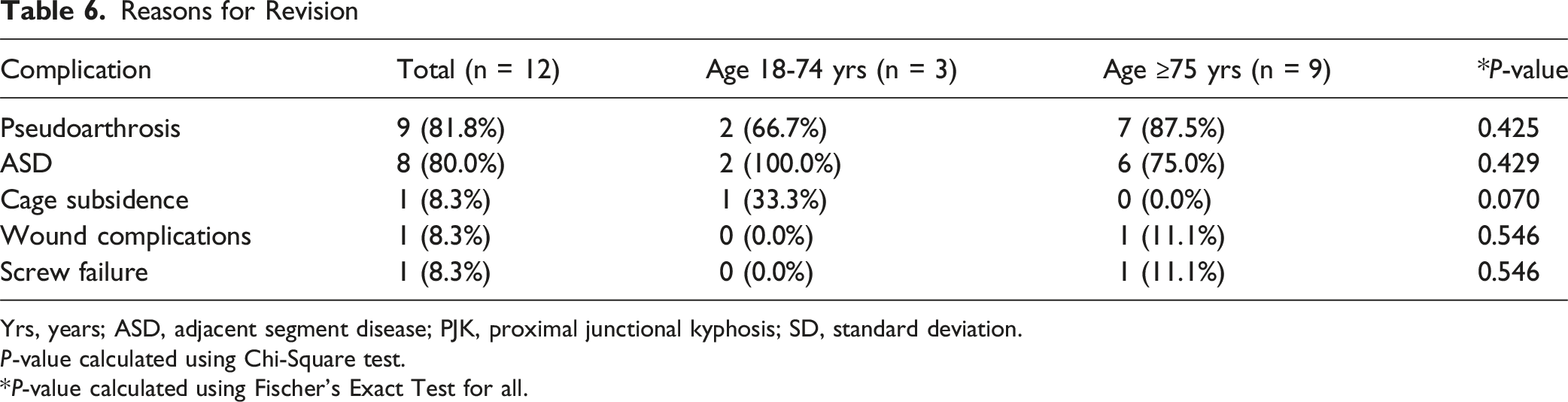
Yrs, years; ASD, adjacent segment disease; PJK, proximal junctional kyphosis; SD, standard deviation.
P-value calculated using Chi-Square test.
*P-value calculated using Fischer’s Exact Test for all.
Radiographic Measures - Matched
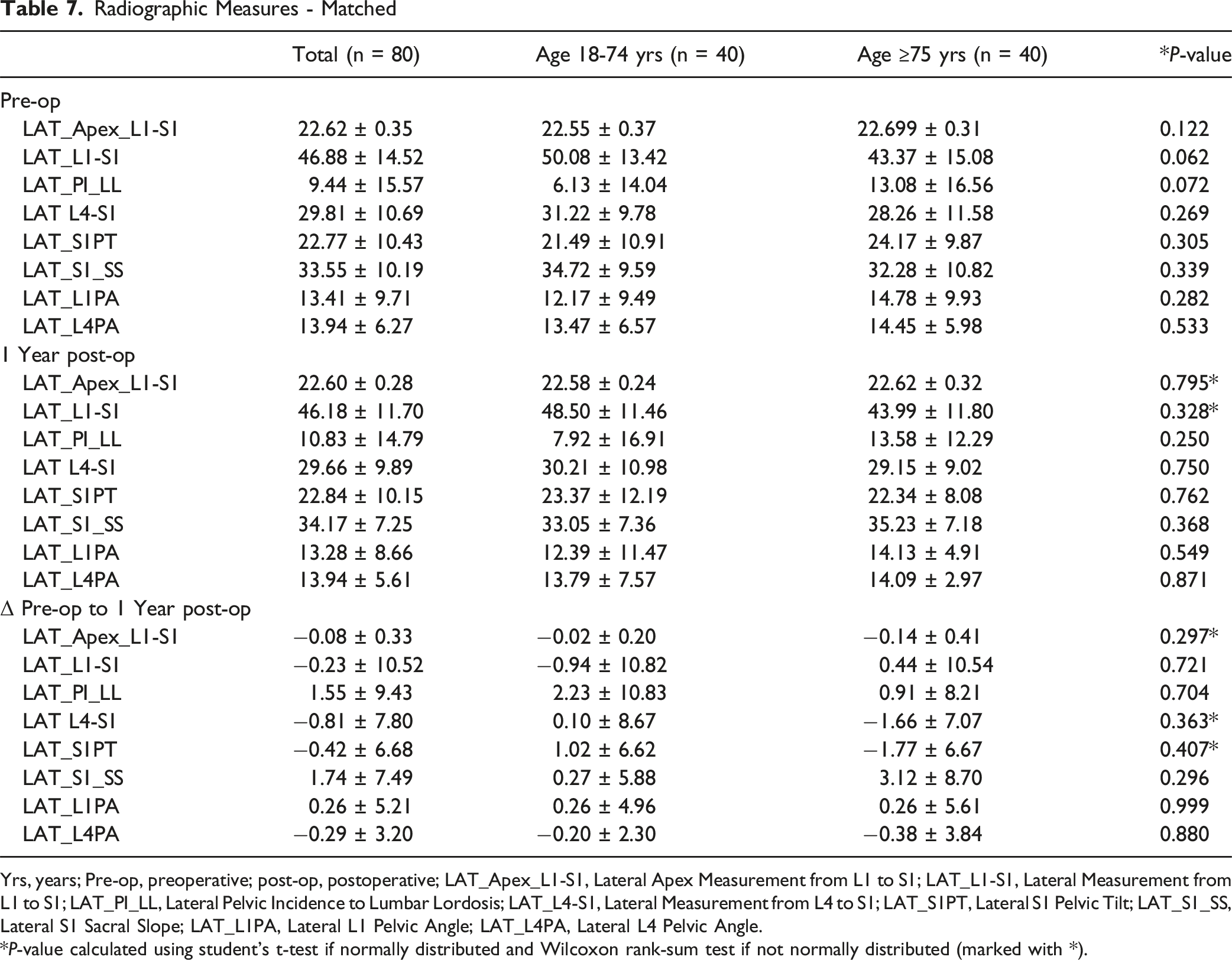
Yrs, years; Pre-op, preoperative; post-op, postoperative; LAT_Apex_L1-S1, Lateral Apex Measurement from L1 to S1; LAT_L1-S1, Lateral Measurement from L1 to S1; LAT_PI_LL, Lateral Pelvic Incidence to Lumbar Lordosis; LAT_L4-S1, Lateral Measurement from L4 to S1; LAT_S1PT, Lateral S1 Pelvic Tilt; LAT_S1_SS, Lateral S1 Sacral Slope; LAT_L1PA, Lateral L1 Pelvic Angle; LAT_L4PA, Lateral L4 Pelvic Angle.
*P-value calculated using student’s t-test if normally distributed and Wilcoxon rank-sum test if not normally distributed (marked with *).
Discussion
Continued advancements in surgical technique and instrument design have made open TLIF a safe approach for a diverse patient population.2,4,21 However, the impact of older age (>75 years) remains an area of concern when considering a surgical approach for patients undergoing lumbar fusion surgery. In the present study, we assessed if patients ≥75 years old experienced different radiographic sagittal and complication outcomes following open TLIF compared to younger individuals (18-74 years old). Preoperatively, we found that older patients had a trend towards worse preoperative sagittal alignment, particularly in terms of PI-LL mismatch (13.1° vs 6.1°, P = 0.072). This suggests that more elderly patients may present with greater sagittal imbalance prior to surgery. Postoperatively, at 1 year follow-up, there were no significant radiographic differences observed between the 2 groups. Additionally, we saw that the overall magnitude of change in sagittal measurements was similar between the cohorts, suggesting that older individuals are equally capable of maintaining surgical correction. Looking at complications, we see that overall, complications rates were similar between the 2 groups. However, patients ≥75 years old required higher rates of revision surgery (22.5% vs 7.69%, P = 0.013). This indicates that while surgery is similarly safe for more elderly patients, they may have an increased risk of subsequent revision surgery. On closer analysis of reasons for revision, older patients were revised more often for Pseudoarthrosis (87.5% vs 66.7%), adjacent segment disease (75.0% vs 100.0%), and screw failure (11.1% vs 0.0%), though none of these were statistically significant (all P > 0.425). This data suggests that, while the overall safety record of surgery does not vary with age, elderly patients may be more likely to experience biologic and mechanical modes of failure requiring revision. Our findings are supported by Patel et al, who reported comparable revision rates between elderly (>65 years) and younger patients undergoing single-level open TLIF (7.8% vs 7.0%), but noted that older individuals more frequently required revision for screw loosening, pseudoarthrosis, and cage migration, whereas younger patients were revised for pseudoarthrosis and adjacent segment disease. 10 Patel et al also found no differences in fusion rates at 24 months postoperatively. 10 Notably, the literature exploring the reasons for revision TLIF along the dependent variable of age is significantly lacking.
Similarly, we found no differences in these long-term radiographic outcomes. In their study looking specifically at open TLIF, Takahashi et al reported that elderly patients (70-86 years old) exhibited less improvement in patient-reported outcomes (PROs) compared to younger patients following TLIF. However, their study also found no significant differences in fusion rates (94% vs 98%) or L1-L5 sagittal alignment correction, further supporting the idea that radiographic outcomes may not be significantly influenced by age greater than 70 years. 11
Our results did not detect a significant difference in fusion or ASD rates. Given that the more elderly patients achieved comparable sagittal alignment, the significant difference in revision surgery may stem from other factors such as the lesser bone mineral density and poorer wound healing that develop as part of aging, rather than inadequate intraoperative sagittal alignment. 6 The relationship between lower preoperative bone mineral density and outcomes following lumbar fusion has been well explored in the literature. Numerous studies have demonstrated that lower preoperative CT Hounsfield values are associated with higher rates of pseudoarthrosis, pedicle screw loosening or failure, cage subsidence, and the development of adjacent segment disease following lumbar fusion surgery.22-26 Nguyen et al conducted a retrospective age-matched study comparing 10 patients with symptomatic pseudoarthrosis and 10 patients without following L4-S1 posterolateral fusion. The preoperative CT Hounsfield Unit (HU) values, measured at L1-L5, were compared, wherein they found patients with pseudoarthrosis had significantly lower HU values at the fused levels (P = 0.01), suggesting reduced bone quality at the operative site may predict nonunion risk. 26 In their study of 70 patients, Schreiber et al similarly found that lower preoperative vertebral body was correlated with an increased risk of radiographic nonunion following lateral lumbar fusion. 25
With the well-understood association between increased age and decreased bone mineral density, researchers have examined these long-term outcomes in patients undergoing lumbar fusion along the dependent variable of age. Several studies have shown non-significant differences in fusion and revision surgery rates when comparing older and younger patients.10,27,28 For example, in their retrospective cohort study of 120 patients who underwent minimally invasive TLIF (MIS-TLIF), Goh et al found no significant difference in fusion or revision. 29 Notably, many other papers comparing outcomes between younger and older individuals often lack a direct comparison of revision rates or simply do no report on long-term revisions or the reasons for revision.30-32 Together, although sagittal alignment in the 2 age cohorts was similar, the increased revision rates in the elderly might best be ascribed to biological considerations of reduced bone mineral density and healing potential in this population. With the proven relationship of reduced preoperative bone quality, most commonly determined in the form of hounsfield units or DEXA scans, and pseudoarthrosis, ASD, and instrumentation failure, these factors are most likely to explain most of the observed revisions.
While spine surgeons continue to adopt minimally invasive surgery (MIS) techniques, open TLIF still is very commonly performed, particularly in the elderly population. Often, elderly patients have more diffuse and/or severe spinal pathology than younger patients, which makes indirect decompression or MIS TLIF more challenging. Open TLIF remains a commonly used approach, particularly for cases requiring extensive spinal decompression, multi-level fusions, or complicated revision surgeries.33,34 Future studies could compare sagittal alignment parameters between MIS and open TLIF to determine if there is any difference in long-term outcomes.
Additionally, further studies are needed to determine whether specific sagittal alignment goals (eg, PI-LL ≤10°) should be prioritized to optimize long-term outcomes and minimize the risk of longer term complications such as ASD or the need for revision surgery. Longer term studies evaluating the connection between age >75 years, sagittal alignment, and complications will be critical in optimizing surgical decision-making for this growing population.
This study is not without a few limitations. Firstly, the sample size was relatively small, which may limit the generalizability of our findings. Our propensity matching was useful in balancing key confounders, nonetheless future studies with a larger cohort would improve the statistical power and allow for a deeper subgroup analysis. Secondly, the follow-up period of 1 year is limited and does not capture the full picture of potential long-term outcomes or complications. Studies with longer follow-up periods are needed to determine if observed sagittal parameters persist over time and if ASD or other degenerative changes may manifest. Thirdly, this study did not incorporate patient-reported outcomes (PROMs), such as the visual analog scale (VAS) for back and leg pain or the Oswestry Disability Index (ODI) for disability. The inclusion of these outcome measures would have provided a more comprehensive evaluation of the clinical picture and allowed us to correlate key radiographic findings with the patient experience. Future studies should include both radiographic and PROM outcomes to fully describe the effects of open TLIF in this population. Lastly, Radiographic factors such as the degree of olisthesis, dynamic instability, and bone mineral density were not consistently documented across patients and were therefore not included in the analysis. Future studies incorporating these parameters may provide a more comprehensive understanding of their influence on fusion and clinical outcomes.
Conclusion
Our results suggest that an age ≥75 years does not have a significant impact on radiographic outcomes following open TLIF. Additionally, perioperative complication rates were similar between groups, although more elderly patients demonstrated a higher rate of revision surgery. As the number of elderly individuals undergoing lumbar fusion surgery continues to rise, further research will be required to determine if optimizing sagittal alignment, along specific parameters, can improve long-term outcomes in this population.
Footnotes
Ethical Considerations
This study was approved by Lifespan IRB.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GS, AP, MJ, CF, IS, and TJ have nothing to declare. BGD reports the following: receives consulting fees from Medtronic and Spineart; CEO and shareholder at Spinal Alignment Solutions. AHD discloses the following: receives royalties from Spineart, Stryker, and Medicrea, consulting fees from Medtronic, research support from Alphatec, Medtronic, and Orthofix, grant from Medtronic, and fellowship support from Medtronic. BB is a consultant for Stryker, Globus, and Medtronic. For the remaining authors, none were declared.
Data Availability Statement
Data will be made available upon reasonable request.