
Abstract
Study Design
Retrospective analysis using national Medicare data.
Objectives
To evaluate historical trends in single and multi-level ACDF utilization and project future procedure volumes among Medicare beneficiaries through 2060.
Methods
Publicly available data from the Centers for Medicare and Medicaid Services (CMS) Medicare Part-B National Summary were analyzed for single-level and multi-level ACDF from 2011 through 2022. Analyses were limited to Part-B claims and therefore excluded inpatient-only procedure codes that are not reported in Part-B. Volumes were adjusted for Medicare Advantage enrollment. Four forecasting models were applied, with Poisson regression selected based on model performance. Point forecasts and 95% confidence intervals were generated through 2060.
Results
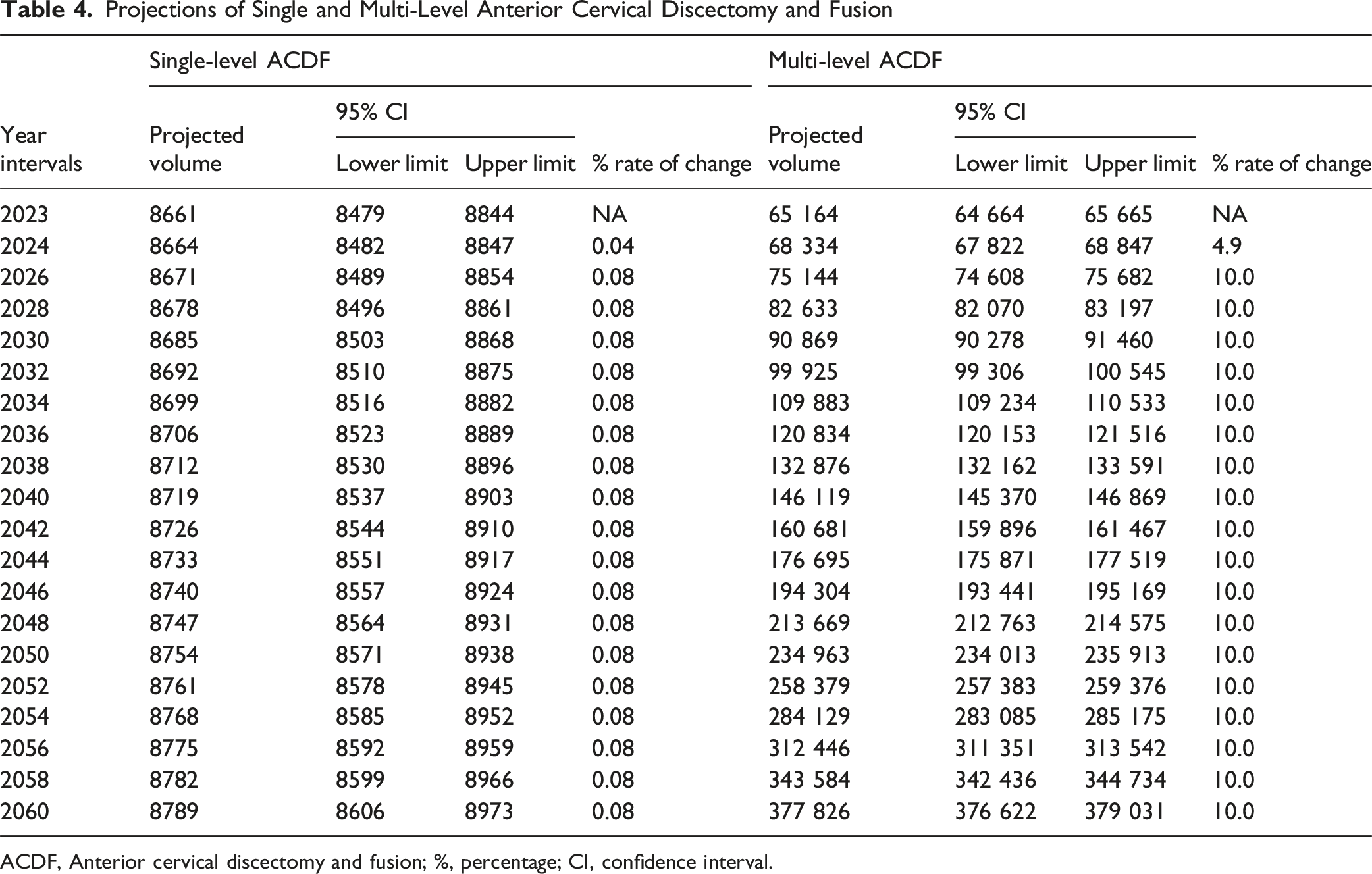
Single-level ACDF volumes decreased by 0.32% from 2011 to 2022, with the largest annual increase from 2011 to 2012 (11.3%) and 5-year growth from 2011 to 2016 (25.7%). In contrast, multi-level ACDF volumes increased by 86.9%, with a 19.5% increase between 2011 and 2012 and 69.8% growth from 2011 to 2016. The Poisson model projected stable annual growth for single-level ACDF at 0.04%, reaching 8,789 procedures (95% CI: 8,606-8,973) by 2060. Multi-level ACDF is projected to grow by approximately 4.9% annually, reaching 377,826 procedures (95% CI: 376,622-379,031) by 2060.
Conclusions
Single-level ACDF utilization is projected to remain stable, while multi-level ACDF is expected to increase substantially through 2060. These trends highlight the growing reliance on ACDF for complex cervical pathology and carry implications for surgical workforce planning, hospital resource allocation, and policy in an aging population.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) remains the most commonly performed surgical intervention for cervical radiculopathy and myelopathy, with widespread use due to its effectiveness in decompressing neural elements and stabilizing the cervical spine. 1 Projections estimate a further 13.3% increase in inpatient ACDF utilization by 2040, as the population ages and the prevalence of cervical spine pathology rises. 2 While ACDF is considered the gold standard, concerns regarding postoperative complications such as dysphagia and adjacent segment degeneration have led to increased interest in cervical disc arthroplasty (CDA). 3 Despite this, ACDF continues to be the predominant surgical treatment, particularly in older patients and those with multiple comorbidities. 3
Trends in ACDF utilization are shaped by patient demographics, procedural complexity, and healthcare economics. Single-level and multi-level ACDF differ in resource use and complication rates, with multi-level procedures involving longer operative times but similar revision frequencies. 4 Cost-containment efforts have also influenced practice patterns; between 2015 and 2019, ACDF without additional anterior instrumentation increased by 91.5%, while ACDF with additional anterior instrumentation procedures declined by 18.1%, based on CMS audit data. 5 Additionally, outpatient ACDF has increased by 15.7%, while inpatient procedures have decreased by 2.2% annually, reflecting broader shifts in healthcare delivery and reimbursement models. 6
Despite outpatient growth, hospital readmissions following ACDF increased from 1.9% to 3.1% between 2011 and 2016, likely due to higher comorbidity burdens. 7 Complication rates have remained stable, yet long-term projections of ACDF utilization remain limited despite evolving demographic and policy trends. This study aims to evaluate historical trends in single and multi-level ACDF utilization among Medicare beneficiaries and to project future procedure volumes through 2060 using statistical modeling. We hypothesize that ACDF utilization will continue to rise, driven by an aging population, increasing demand for cervical spine surgery, and ongoing shifts toward outpatient care.
Methods
Database
This study utilized data from the Centers for Medicare and Medicaid Services (CMS) Medicare Part-B National Summary from 2011 to 2022. 8 This publicly available dataset provides annual procedure volumes for Medicare beneficiaries and was used to identify trends in single-level and multi-level ACDF procedures. Given the de-identified and publicly available nature of the data, this study was exempt from Institutional Review Board (IRB) approval. Informed consent was not required as the analysis used only de-identified, aggregate-level data from a public database.
Cohorts
Single-level ACDF was identified by calculating the difference between the total occurrences of CPT code 22551 and CPT code 22552, given that 22551and must be coded before 22552 in multi-level cases. Multi-level ACDF was identified by the presence of CPT code 22552.
Outcomes of Interest
The primary outcomes of interest were the annual procedure volumes of single-level and multi-level ACDF. These volumes were used to model projected utilization trends through 2060, assessing growth patterns and estimating future demand for these procedures among Medicare beneficiaries. Our primary outcome is the annual number of procedures among Medicare beneficiaries. We adjusted observed counts for the rising share of Medicare Advantage to reduce undercount from beneficiaries managed outside traditional Medicare. This adjusted procedure volume using the ratio of traditional Medicare to Medicare Advantage enrollees as reported by the Kaiser Family Foundation. 9 Because our goal was to project absolute service demand in Medicare, we did not scale counts by a beneficiary denominator. Projections should be interpreted with the understanding that changes in enrollment can move absolute counts even when per-beneficiary rates are unchanged.
Statistical Analysis
All analyses were conducted using R statistical software (version 4.4.0; R Project for Statistical Computing, Vienna, Austria). We fit 4 candidate forecasting models — log-linear, Poisson regression, negative binomial regression, and auto-regressive integrated moving average (ARIMA) — and compared performance using mean absolute error (MAE) and root mean square error (RMSE). When error metrics were similar, tie-breakers prioritized interpretability with an explicit growth parameter, non-negativity of predicted counts, and availability of closed-form parametric confidence intervals. For single-level ACDF, Poisson and negative binomial achieved the lowest MAE and RMSE, with ARIMA producing nearly identical values. For multi-level ACDF, ARIMA had the lowest in-sample error, with Poisson close in magnitude. Although ARIMA achieved slightly lower in-sample error in places, its reliability for long-term forecasting was limited, so we selected Poisson to generate point forecasts and 95% confidence intervals for 2023 to 2060. Poisson regression models non-negative counts and estimates a smooth year-over-year growth rate, yielding expected annual procedure counts with interval estimates. Compared with negative binomial, log-linear, and ARIMA models, Poisson provided transparent growth parameters, non-negative predictions, and stable long-horizon behavior. Forecasts should be read as the expected number of Medicare ACDF procedures if recent patterns continue without major structural change. This modeling approach has been validated in prior studies examining long-term procedural volume trends.10,11
Results
From 2011 to 2022, the uplifted annual volumes of single-level ACDF procedures declined slightly from 7,584 to 7,560, reflecting a net decrease of 0.32%. The most significant annual increase occurred between 2011 and 2012, with an 11.3% rise. The steepest annual decline was between 2021 and 2022, decreasing by 13.6%. The highest 5-year growth for single-level procedures was observed between 2011 and 2016, with a 25.7% increase in volume.
Adjusted Historical Procedure Volume of Single and Multi-Level Anterior Cervical Discectomy and Fusion
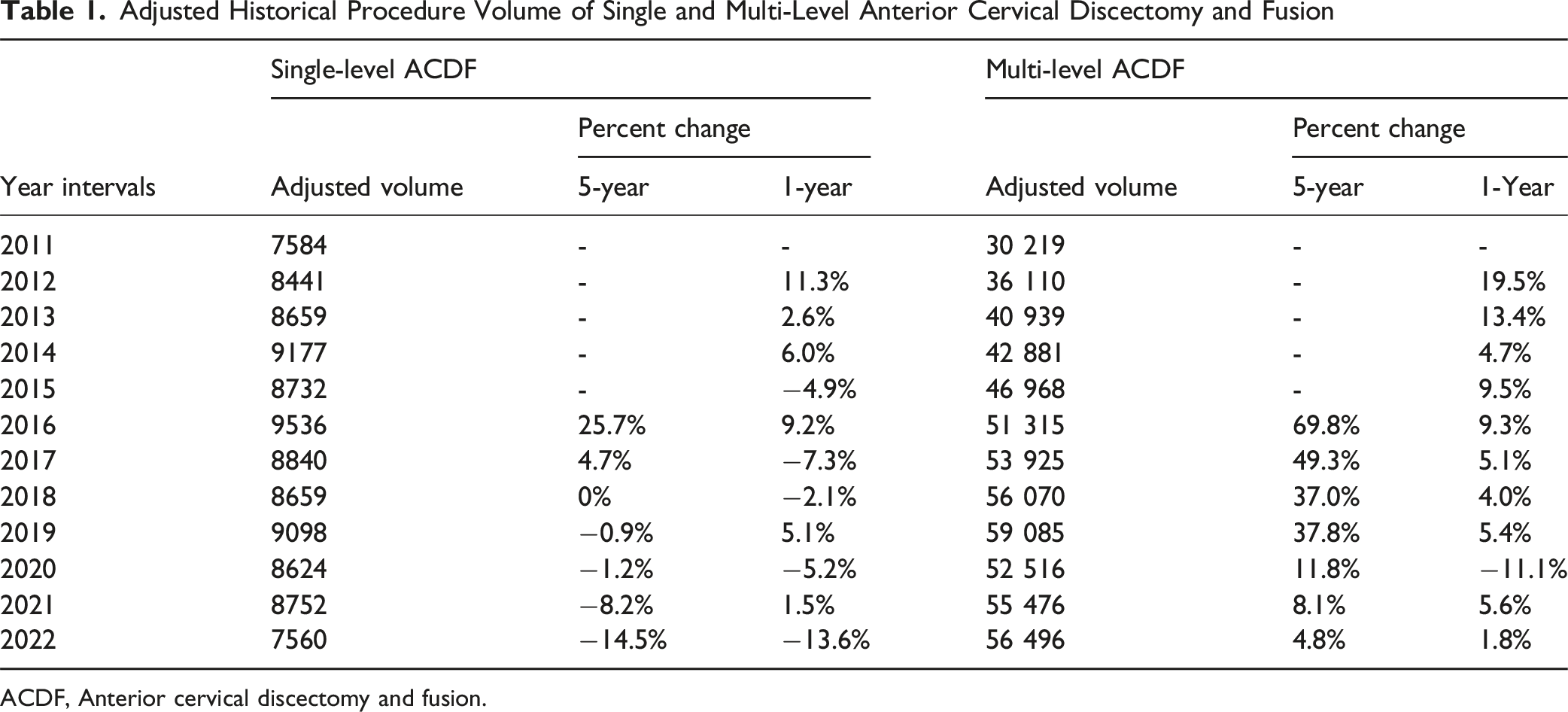
ACDF, Anterior cervical discectomy and fusion.
Forecast Model Outputs for Single-Level Anterior Cervical Discectomy and Fusion
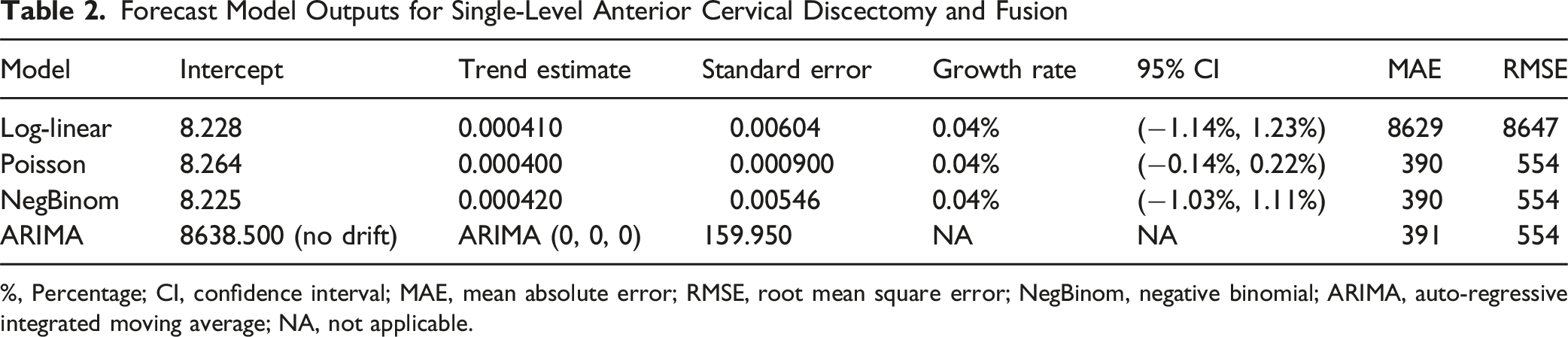
%, Percentage; CI, confidence interval; MAE, mean absolute error; RMSE, root mean square error; NegBinom, negative binomial; ARIMA, auto-regressive integrated moving average; NA, not applicable.
Forecast Model Outputs for Multi-Level Anterior Cervical Discectomy and Fusion

%, Percentage; CI, confidence interval; MAE, mean absolute error; RMSE, root mean square error; NegBinom, negative binomial; ARIMA, auto-regressive integrated moving average; NA, not applicable.
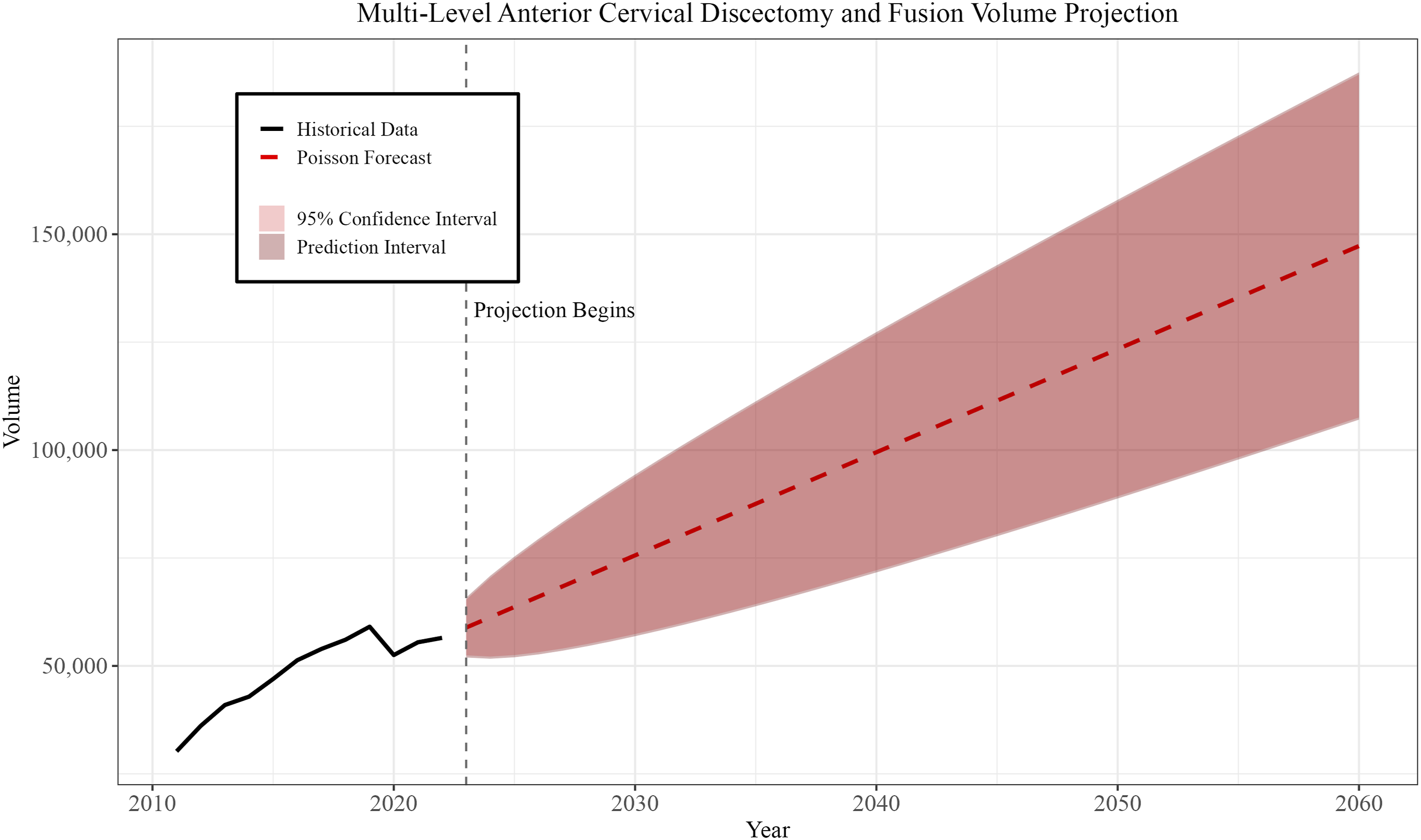
Using the Poisson model, point forecasts and 95% confidence intervals were generated for annual procedure volumes through 2060. For single-level ACDF, the annual growth rate is projected to remain steady at 0.04%, resulting in a projected volume of 8,789 (95% CI: 8,606-8,973) by 2060. In contrast, multi-level ACDF volumes are expected to grow at a more substantial rate, averaging approximately 4.9% annually, reaching 377,826 procedures (95% CI: 376,622-379,031) by 2060. Figures 1 and 2 illustrate historical trends and future projections for both single-level and multi-level ACDF (Table 4). Historical trends and projected volumes for single-level anterior cervical discectomy and fusion (2011-2060) Historical trends and projected volumes for multi-level anterior cervical discectomy and fusion (2011-2060) Projections of Single and Multi-Level Anterior Cervical Discectomy and Fusion ACDF, Anterior cervical discectomy and fusion; %, percentage; CI, confidence interval.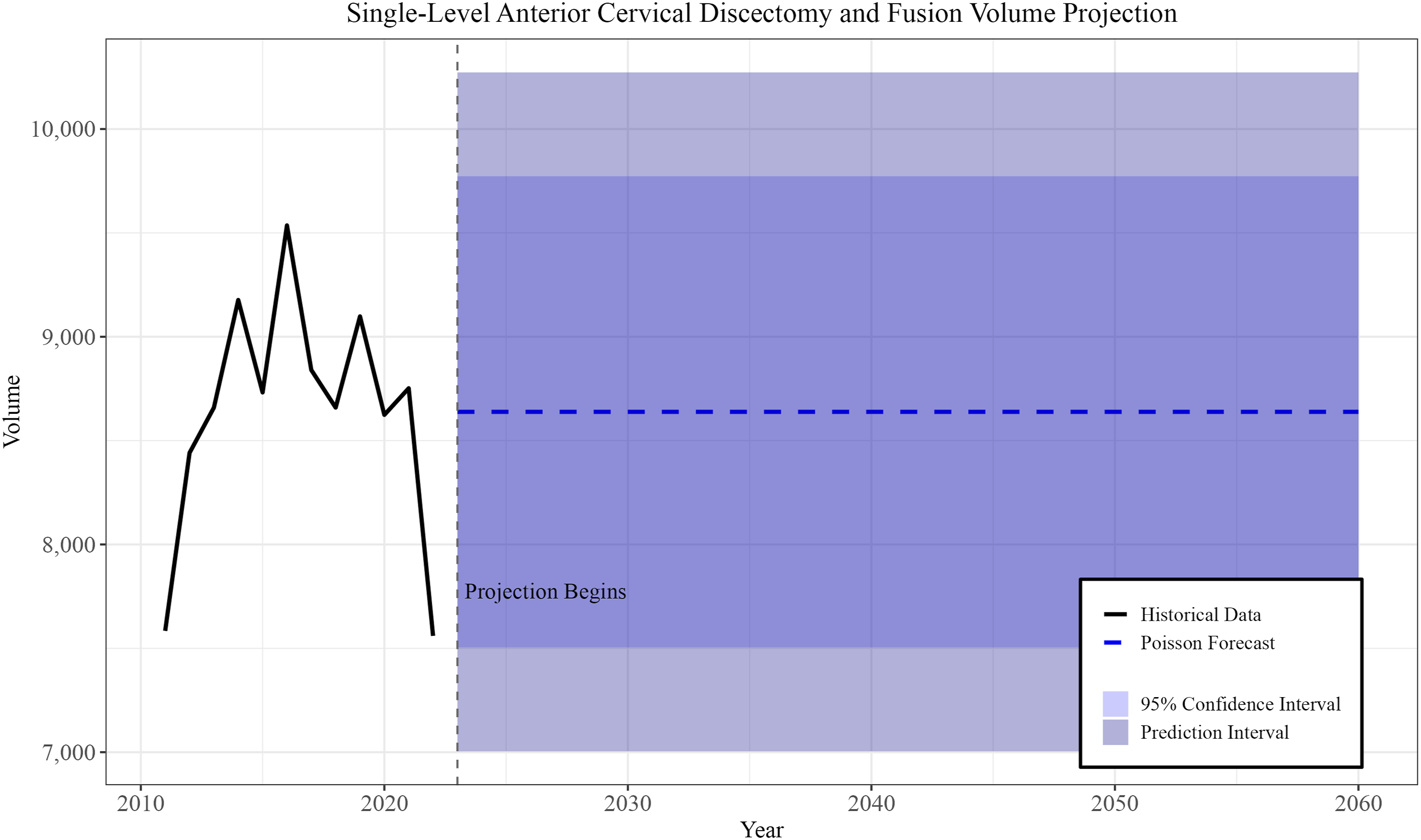
Discussion
ACDF remains a critical procedure in the surgical management of cervical radiculopathy and myelopathy, with increasing utilization among Medicare beneficiaries. Our analysis demonstrated that while single-level ACDF volumes have remained relatively stable, multi-level ACDF procedures are projected to rise substantially through 2060. These findings align with previous projections of increased cervical spine surgeries but offer additional granularity by distinguishing between single and multi-level trends — an area previously underexplored in the literature. 2 The growing demand for multi-level ACDF underscores evolving clinical practice patterns and demographic shifts in the Medicare population.
A key driver of the projected rise in multi-level ACDF is the aging U.S. population, which is more susceptible to multi-level cervical degenerative disease. Prior projections indicate substantial increases in ACDF volume among older adults, particularly in the 75-84 and >85-year-old cohorts, reflecting the growing burden of age-related spinal pathology. 2 Beyond demographics, evolving anterior techniques and perioperative pathways have improved the safety and reproducibility of multilevel constructs, and patient selection has broadened to favor comprehensive, single-stage correction of multilevel pathology. Additionally, advances in imaging modalities such as MRI and CT have enhanced the early detection of multi-level cervical spine degeneration, thereby facilitating timely surgical intervention. Concurrently, site-of-service shifts toward outpatient care, driven by more surgeons performing ACDF/CDA as outpatient procedures, together with coding/documentation changes, may facilitate single-episode multilevel treatment in appropriately selected patients. 12 Evolving surgical guidelines also increasingly support addressing multiple symptomatic levels during a single operation to improve long-term outcomes and reduce the risk of future reoperations. 13 For instance, ACDF has demonstrated more rapid and sustained relief of radicular symptoms compared to conservative management, supporting its use in appropriately selected patients. 13 Furthermore, adjacent segment disease (ASD), a known complication following ACDF, is more prevalent among older patients and those with congenital stenosis, underscoring the importance of comprehensive surgical treatment at the time of initial presentation. 14 Collectively, these factors — aging demographics, refined surgical and perioperative practices, broadened selection criteria, improved diagnostic capabilities, and site-of-service and coding shifts — help explain the disproportionate growth in multi-level ACDF. Pandemic-era access constraints in 2020 and 2021 reduced availability for lower-acuity single-level cases and prioritized patients with more severe multilevel disease. Concurrent shifts toward outpatient care may also have concentrated higher-yield episodes. 15 These dynamics align with the observed decrease in single-level procedures and the relative increase in multilevel procedures during that period. Although our models use the full historical record, future changes in access or policy could move realized volumes away from the predicted ranges.
Clinical outcomes between single and multi-level ACDF are comparable in terms of ASD, but multi-level surgeries offer superior correction of cervical lordosis. 16 This enhanced correction can be particularly beneficial in patients with kyphotic deformities or advanced multi-level spondylosis, where restoration of sagittal alignment is crucial for functional recovery. However, multi-level ACDF is associated with higher implant-related complication rates, reflecting increased procedural complexity. 4 These risks must be carefully weighed against potential benefits, especially as the volume of multi-level procedures continues to rise. Despite the increasing adoption of CDA — which grew by 654% between 2011 and 2019 — ACDF remains the preferred approach for patients with severe degeneration, instability, or multi-level involvement. 3 Furthermore, CDA is often contraindicated in older patients or those with significant facet arthropathy, limiting its applicability across the broader patient population. Notably, cost-effectiveness analyses over a 5-year horizon have shown no clear economic advantage between ACDF and CDA, suggesting that clinical indications continue to drive procedural choice. 17
Surgeons frequently default to ACDF when anatomical or degenerative changes render motion-preserving implants unsuitable. Older patients with advanced spondylosis, osteophyte formation, or severe facet arthropathy often require ACDF to achieve adequate spinal stability and ensure surgical safety. 18 In these populations, CDA is often contraindicated due to concerns over implant subsidence, limited facet preservation, and reduced motion benefit in the context of advanced degeneration.3,14 This reliance on ACDF, especially in complex or multi-level cases, accounts for its sustained and growing utilization despite the availability of alternatives. The increasing prevalence of multi-level cervical pathology among older adults further drives the need for fusion-based approaches, as evidenced by the substantial projected rise in multi-level ACDF volumes through 2060. These trends carry significant implications for healthcare systems, including the need for expanded surgical capacity, targeted workforce training, and optimized postoperative care pathways to manage growing patient demand.6,7 Policy adjustments in reimbursement models and the development of clear procedural guidelines may also be necessary to support equitable and appropriate utilization across diverse hospital settings. 5
While our projections adjust for the rising share of Medicare Advantage beneficiaries, Medicare Advantage and traditional Medicare populations may differ in ways that can shift absolute volumes. First, unit prices for common physician services in Medicare Advantage are generally similar to traditional Medicare, suggesting price levels alone are unlikely to drive divergence. 19 However, episode payments and site-of-service patterns in spine care vary meaningfully, whereby 90-day payments and facility costs differ between inpatient and outpatient settings in datasets that include Medicare Advantage beneficiaries, and substantial preoperative spending on nonoperative modalities prior to ACDF is concentrated in imaging and injections.20,21 Regional practice variation relevant to perioperative management, such as opioid use, is also documented in claims that include Medicare Advantage populations, indicating geography may mediate utilization patterns. 22 Finally, patient-perceived integrated care appears similar across Medicare Advantage and traditional Medicare, implying that differences in coordination alone may not explain large utilization gaps. 23 These factors could alter absolute projected counts even if the contrasting trajectories we report for single vs multi-level ACDF remain directionally consistent. Accordingly, the long-range projections are conditional on historical patterns. Accelerated technology adoption, faster outpatient migration, or reimbursement changes could shift levels or growth rates relative to these projections. To avoid overinterpretation, we emphasize directionality and relative differences between single and multilevel trajectories, which were consistent across model specifications.
This study has several limitations. Our analysis used Medicare Part B data, which primarily represents older adults and excludes trends among younger or privately insured populations. As a result, these findings primarily reflect Medicare beneficiaries and should not be directly generalized to younger populations or privately insured cohorts. Aggregate national files may also be subject to reporting lags or suppression rules that limit completeness and granularity in some years. The dataset reports aggregate CPT-level counts rather than patient-level records, which prevents stratification by demographics, clinical severity, or hospital characteristics. Changes in coding practices, edits to CPT descriptors, and documentation behavior over time may alter how single vs multilevel procedures are recorded. Migration of cases across sites of service, including hospital outpatient departments and ambulatory surgery centers, may also affect completeness and comparability across years. Forecasting models, while based on historical trends, cannot fully anticipate future policy changes, technological advances, or shifts in clinical practice. Confidence intervals reflect statistical uncertainty from the model only and do not capture potential impacts of policy, coding, technology, or access changes. Our forecasts are based on count models and represent absolute Medicare volumes. They do not adjust for future changes in the size or age mix of the beneficiary population beyond our Medicare Advantage correction. Projections should be interpreted alongside evolving enrollment trends. CPT code edits, documentation and audit initiatives, and reimbursement changes have previously produced discontinuities in observed volumes. 5 Accordingly, our confidence intervals capture only statistical model uncertainty and likely understate true uncertainty, and structural breaks over a 38-year horizon may shift utilization outside model-derived bounds. Despite these limitations, our projections provide valuable insights into future ACDF demand, informing resource allocation and strategic planning for an aging surgical population.
Conclusions
This study demonstrates a projected stability in single-level ACDF volume with a minimal annual growth rate of 0.04%, reaching approximately 8,789 procedures by 2060. In contrast, multi-level ACDF is projected to grow substantially, with an average annual increase of 4.9%, culminating in an estimated 377,826 procedures by 2060. These trends underscore the increasing reliance on ACDF for the treatment of complex multi-level cervical pathology, with important implications for surgical capacity, resource allocation, and long-term healthcare planning.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Disclosures
IRB Approval
No IRB approval was required for performance of this review.