
Abstract
Study Design
Retrospective Cohort Study.
Objective
Obesity rates have risen over recent decades, with many affected individuals experiencing degenerative spine conditions. A parallel increase in spine surgeries has raised questions about how to best optimize care in obese patients. Those with extremely high BMI (>50), classified as “Super Morbidly Obese (SMO)”, may face higher risks of poor surgical outcomes. To better understand the challenges in treating this population, we compared complications, and operative characteristics between morbidly obese (MO), and SMO.
Methods
A single-institution retrospective review was conducted on patients with a BMI over 40 who underwent a neurosurgical procedure from 2017 to 2023. Inclusion criteria were (1) patient age >17 years, (2) BMI >40, and (3) surgical interventions performed by a member of the department of neurological surgery. Demographic, clinical, surgical, and post-operative follow-up were analyzed.
Results
Patients were split into SMO (BMI 50+) and MO (BMI 40-50) groups. SMO received more intra-operative imaging radiation (P = 0.0169), experienced longer hospital stays (P < 0.0005) and experienced more post-operative complications than MO patients (P = 0.008). SMO patients experienced more complications when discharged home than their MO counterparts (P = 0.0002, RR = 12.2 [2.7-53.4]).
Conclusion
Risk in SMO spine surgery can be reduced through weight loss, modified surgical approaches, and better discharge planning. Regardless of comorbidities, SMO patients discharged home face higher complication rates than MO patients and may benefit from early discussions about skilled nursing placement. Larger studies are needed to better assess surgical management and outcomes in this population.
Introduction
Obesity is a chronic condition that affects people of all ages and backgrounds. According to the National Health and Nutrition Examination Survey (NHANES), the prevalence of obesity in the United States (US) in 2017 was 41.9%, increased from 30.5% in 1999. 1 Other studies have evaluated the impact of obesity on public health trends and concluded that this is a heavy health burden.2-4 With the incidence of spine surgery increasing worldwide, it is important to evaluate outcomes in high-risk patient populations to individualize the care of these patients.5,6
It is well understood that outcomes of spine surgery are influenced by many factors including age, activity-level, and comorbid conditions. Elevated BMI is a well described risk factor in patients undergoing spine surgery. While many studies have compared surgical outcomes for patients with normal BMI to overweight (25-30 BMI) or obese (>30 BMI) patients, few studies have analyzed outcomes for morbidly obese (MO) patients (>40).7-12 Bono et al found a significant increase in infections and surgical complications for patients with BMI >35 with rates further increasing for BMI >40. 13 Additionally, Marquez-Lara et al. found that patients who were overweight and obese had increased complication rates following spine surgery. 14
There is an even greater paucity of literature evaluating the super morbidly obese (BMI >50). O’Connell et al. reported that super morbid obesity is associated with younger age and high prevalence of adverse metabolic profiles. 15 Katsevman et al described outcomes of 63 SMO patients (BMI >50) with control groups of patients of BMI <30 and 30-50. They concluded that complication rates were significantly higher for SMO patients compared to non-SMO patients, especially for those who were undergoing non-elective surgery. 16
With 1 in 4 adults projected to be BMI >35 by 2030, it is important to better understand the implications of spine surgery in this SMO population. 17 In this study, we aim to describe our institutional experience operating individuals with high class obesity. We compare individuals with MO to those with SMO with respect to demographics, procedural data, complication rates, and clinical outcome.
Methods
Study Design and Inclusion Criteria
The present study is a retrospective cohort of morbidly obese (BMI 40-49.99) and super morbidly obese (BMI >50) patients undergoing any surgical procedure by one of four board-certified, fellowship-trained neurological surgeons from 2017 to 2023 at a single institution. Among the patients operated on, the inclusion criteria for this specific study were: (1) patient age >17 years, (2) BMI over 40, and (3) surgical interventions performed by a member of the department of neurological surgery. Patients whose surgical intervention did not include primary spine surgery or were under 17 were excluded. All BMI 50+ patients were selected from a list of cases performed at our institution during the time frame of 2017-2023. The MO group was then selected from the same list of cases performed during the above time period, and were matched based on year of surgery.
Data Collection
Demographic, operative, and post-operative data was collected for all patients. Background variables included age, sex, race, previous arthroplasty, BMI, comorbidities (diabetes, atrial fibrillation, hypertension, hyperlipidemia, coronary artery disease, chronic kidney disease, osteoporosis), smoking status (current, former, never) and pack year history, presenting symptoms (back pain, fevers, neurological deficit, unknown, asymptomatic), and medical history (previous spinal surgery, spine trauma, hardware failure). Operative factors included type of approach (open vs minimally invasive), American Society of Anesthesiologists classification (ASA), surgery performed, intraoperative radiographs (time, view, and radiation amount), blood loss, operation length, length of stay, intraoperative complications, postoperative complications or hardware failure, and need for any secondary surgeries. Intra-operative complications included complications that occurred during the surgery. Post-operative complications included anything that occurred after discharge, and were collected for all patients from the progress notes at the clinic visits at 4 weeks post-op, 8 weeks post-op, and 12 weeks post-op. These were compiled as total complications and were not stratified based on timing.
Statistical Analysis
The cohorts were divided into the groups “BMI 40-50” and “BMI >50” based on BMI on the date of surgery. All statistical tests were performed with SPSS Version 29.0.1.0. For univariate analysis, continuous variables were compared with independent-sample T-test, and categorical variables compared with Chi-square analysis, and Fishers Exact test, where appropriate
Results
Demographic Data of the Two Cohorts of MO and SMO Patients
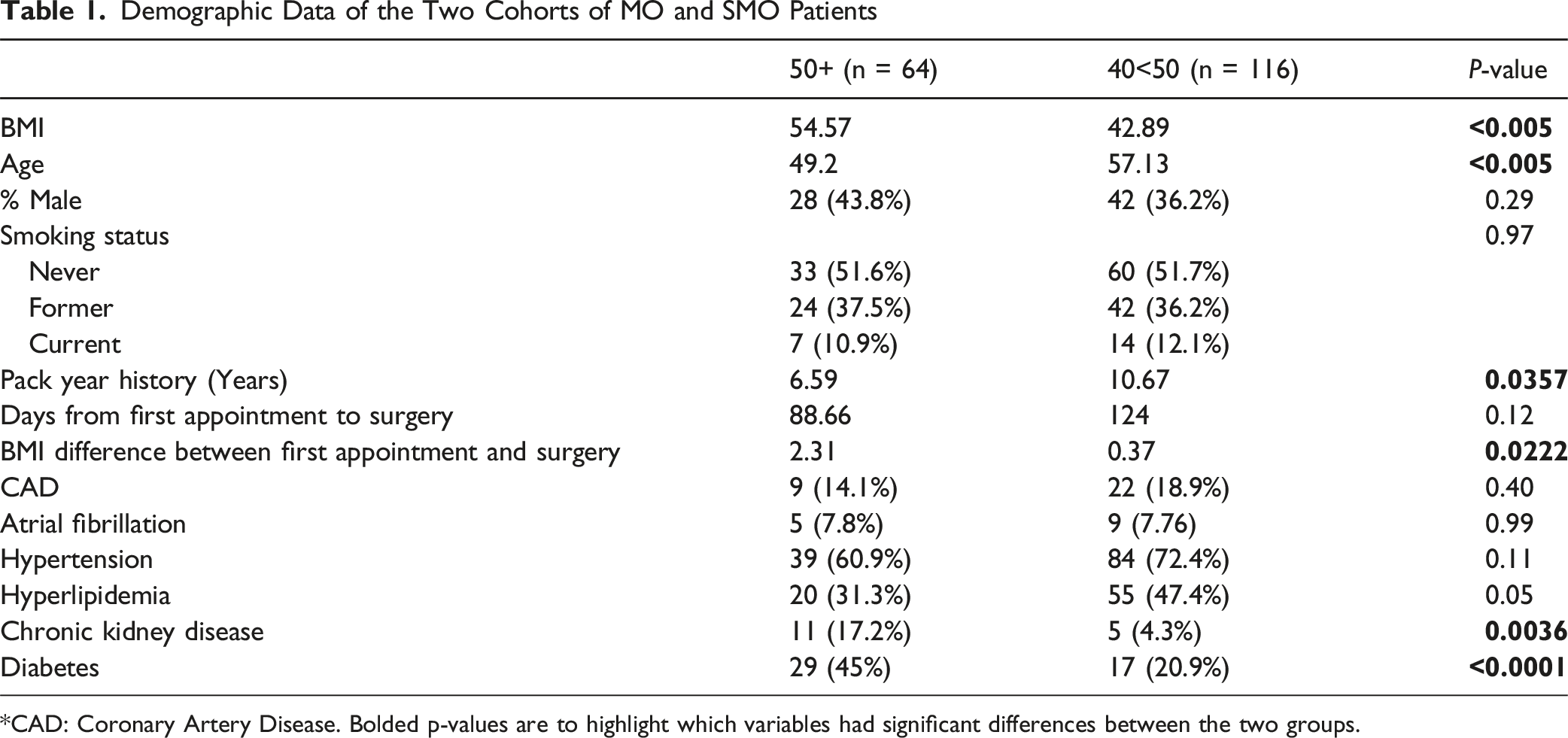
*CAD: Coronary Artery Disease. Bolded p-values are to highlight which variables had significant differences between the two groups.
Surgical Characteristics Between the Two Cohorts of MO and SMO Patients Including Intraoperative Radiation
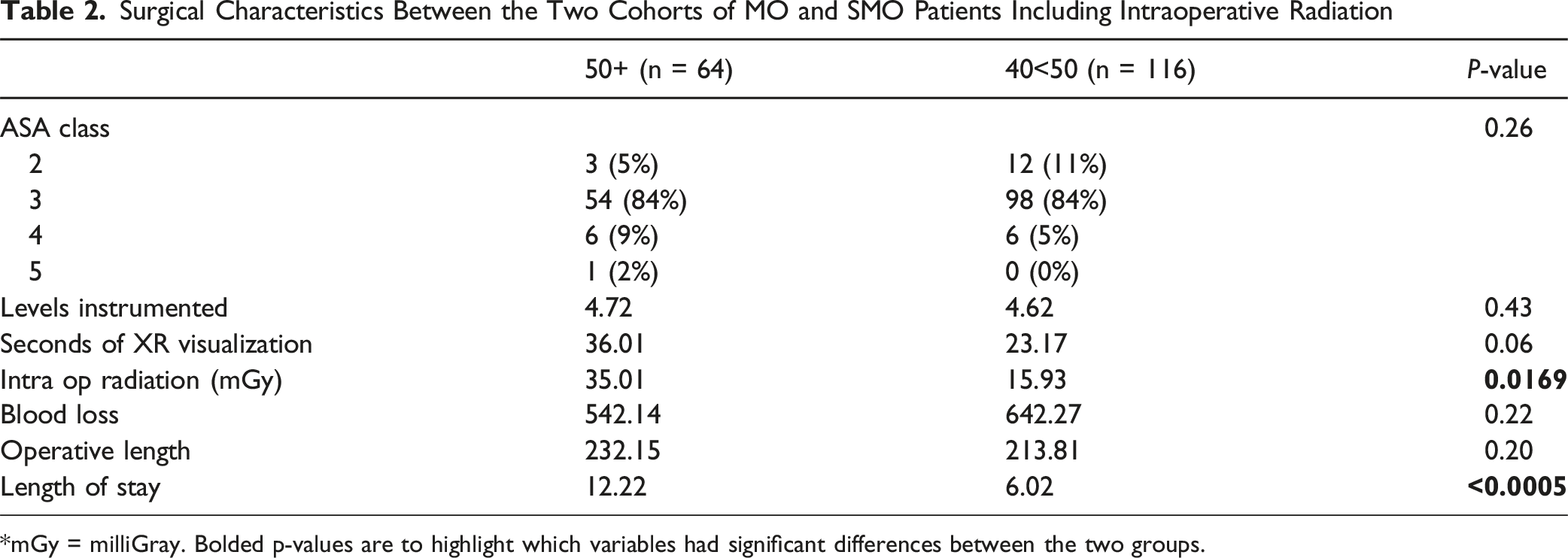
*mGy = milliGray. Bolded p-values are to highlight which variables had significant differences between the two groups.
Surgery Types of the Two Cohorts of MO and SMO Split by Spinal Location, and Whether It was Fusion or Non-fusion Surgeries

aOther is suboccipital craniectomy for BMI 50.
ACDF = Anterior Cervical Discectomy and Fusion, TLIF = Transforaminal Lumbar Interbody Fusion.
(a) Post-operative Complications Between the Two Cohorts Stratified by Type of Surgery in the Cervical Region
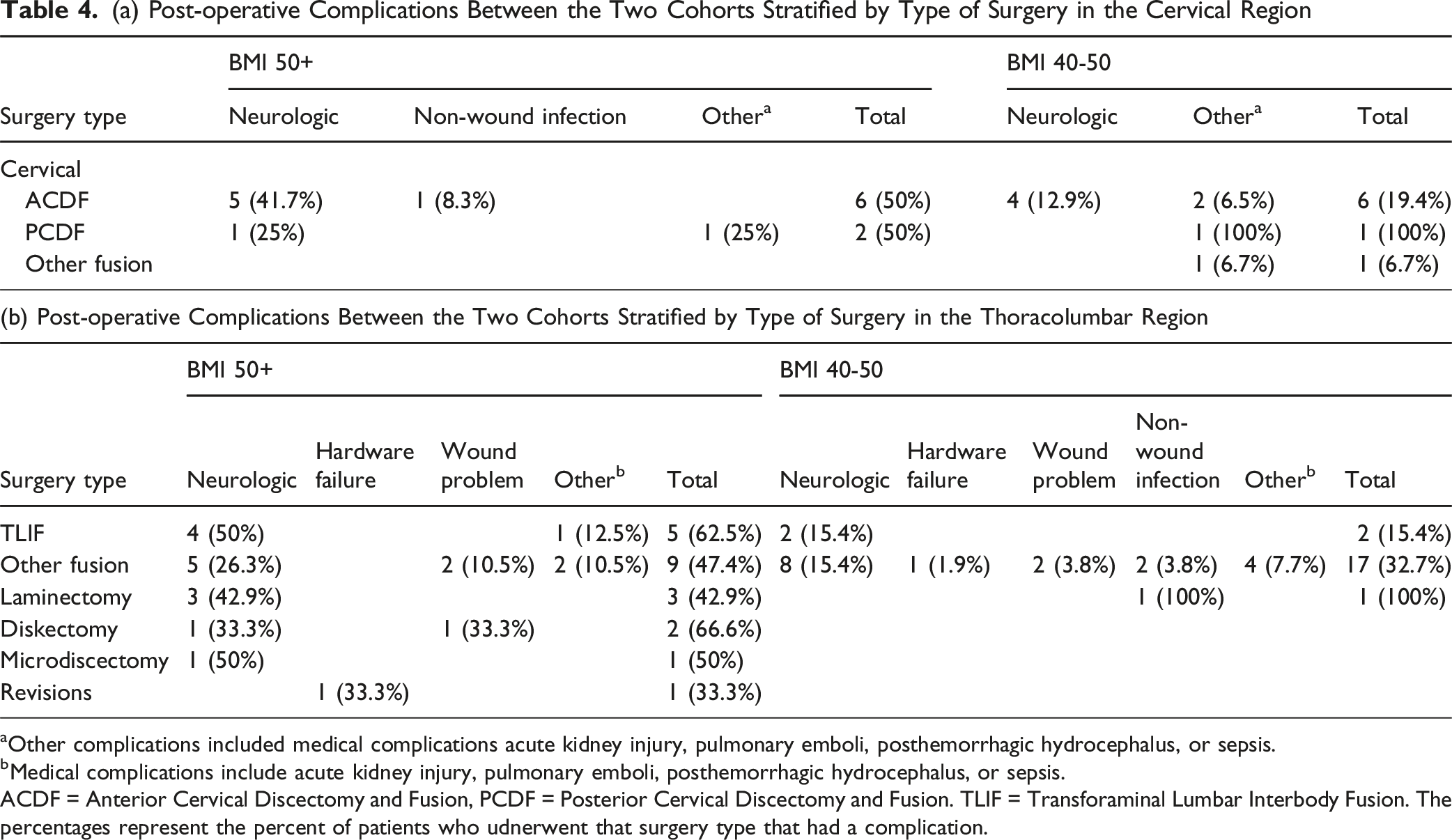
aOther complications included medical complications acute kidney injury, pulmonary emboli, posthemorrhagic hydrocephalus, or sepsis.
bMedical complications include acute kidney injury, pulmonary emboli, posthemorrhagic hydrocephalus, or sepsis.
ACDF = Anterior Cervical Discectomy and Fusion, PCDF = Posterior Cervical Discectomy and Fusion. TLIF = Transforaminal Lumbar Interbody Fusion. The percentages represent the percent of patients who udnerwent that surgery type that had a complication.
Discharge Characteristics Between the Two Cohorts of MO and SMO Patients
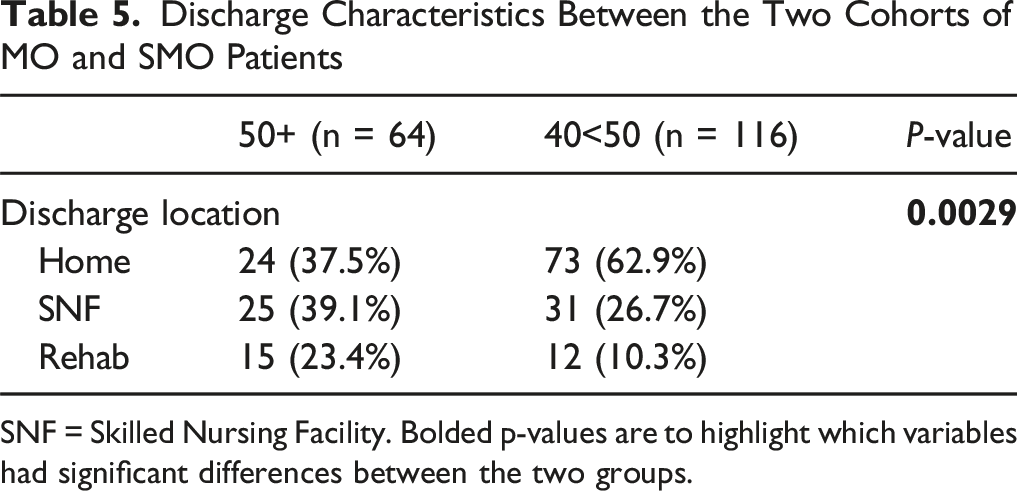
SNF = Skilled Nursing Facility. Bolded p-values are to highlight which variables had significant differences between the two groups.
Complication Profiles of the Two Cohorts of MO and SMO Patients
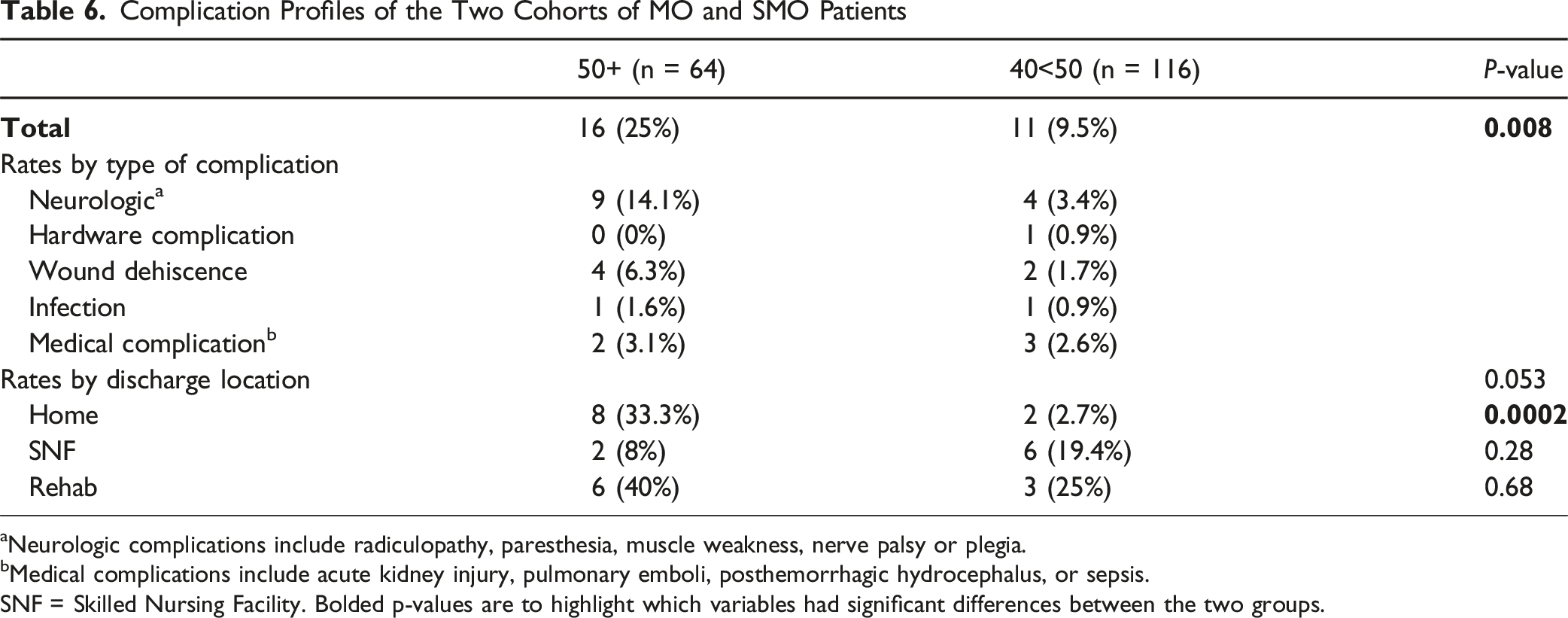
aNeurologic complications include radiculopathy, paresthesia, muscle weakness, nerve palsy or plegia.
bMedical complications include acute kidney injury, pulmonary emboli, posthemorrhagic hydrocephalus, or sepsis.
SNF = Skilled Nursing Facility. Bolded p-values are to highlight which variables had significant differences between the two groups.
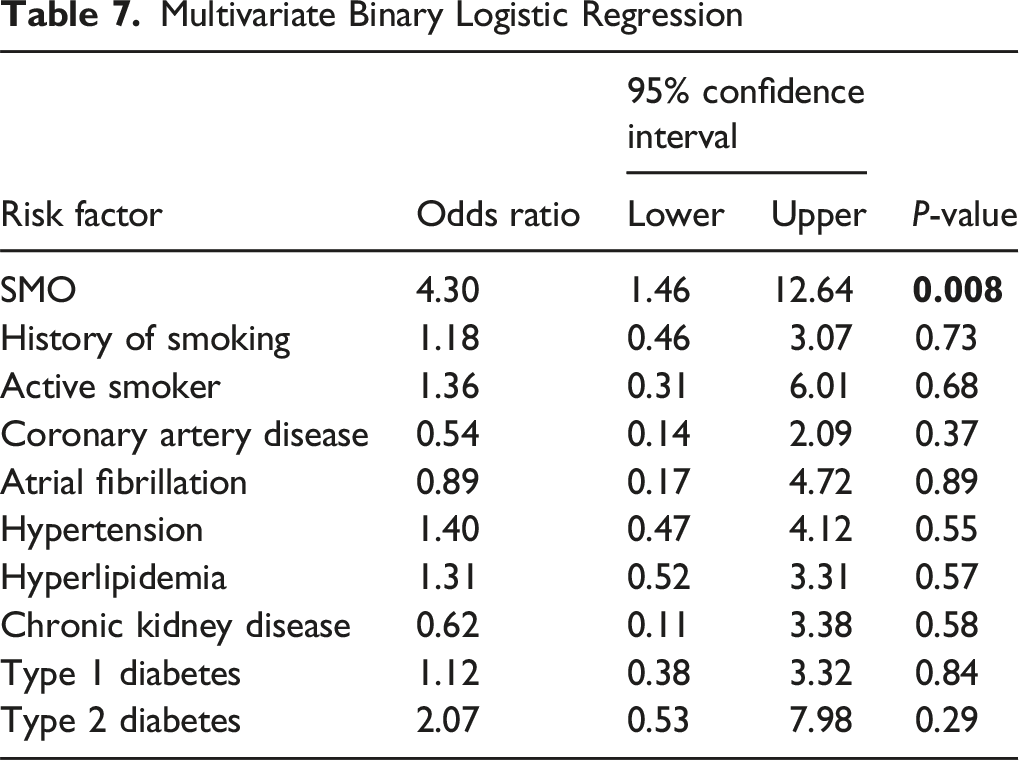
Multivariate Binary Logistic Regression
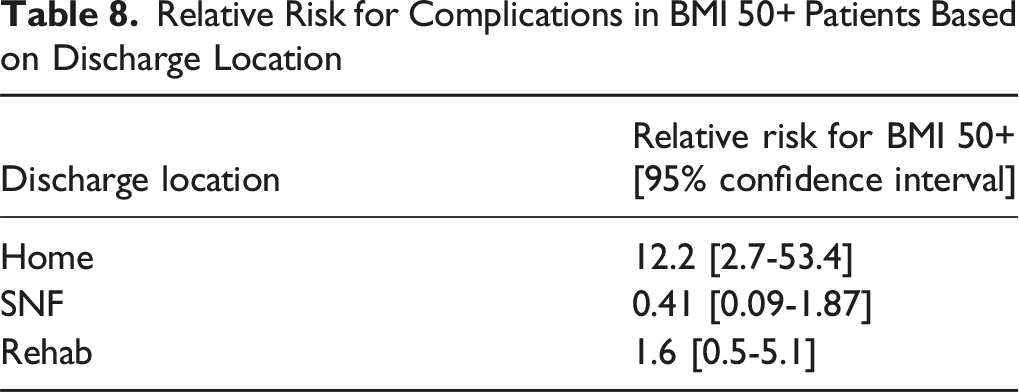
Relative Risk for Complications in BMI 50+ Patients Based on Discharge Location
Institutional Surgical Management of SMO Patients
The care of patients with elevated BMI offers unique challenges in terms of healthcare associated logistics and can affect the surgical management of these patients. Of these, the main challenges with this patient population are proper surgical positioning, difficult visualization with the use of intra-operative imaging, higher risks of both intraoperative and post-operative complications, and the effect of volume distribution on surgical technique and instrument selection. These operative challenges vary based on surgery type, spinal location, and complexity of the case. Within our institution, there has been a shift to use different methods for some of these cases with the hope of reducing barriers to care in this patient population.
For most spine surgeries, patients are in the prone position, but there are a few instances, such as the anterior cervical discectomy and fusion (ACDF), which requires the patient to be in a supine position. Regardless of position, one of the main challenges is to achieve proper pressure free positioning around adipose folds and pannus. In prone patients, the intra-operative challenges involve exposure of the index levels due to excess dorsal fat pads and length restrictions of instruments. A few solutions used to reduce the burden of exposure are to minimally invasive platforms such as tubular retractors or endoscopy to navigate through long operative corridors.
Challenges that arise in patients, regardless of surgery type or positioning, involve difficulty with visualization using intra-operative imaging. This increases the risk of wrong level procedures. Some solutions that our surgeons implement are to use anterior-posterior x-rays in combination with oblique lateral views, along with the use of intraoperative CT. In both cases, the radiation exposure to patients is higher due to the need for higher penetrance dosing as well as additional views of imaging.
Current literature surrounding post-operative complications in super morbidly obese patients shows that they have a higher rate of complications like wound dehiscence and surgical site infections. 16 To decrease the risk of developing these types of complications, our institutional practice is to use multiple surgical drains post-operatively for aggressive drainage of the surgical site as well as the use of incisional wound vacuums to mitigate seroma formation.
Obesity is an ever-growing epidemic that provides unique challenges and complications to spine surgery; however, many of these patients can still benefit from surgery in certain circumstances assuming the surgeons provide a detailed discussion of the risks and benefits of the procedure. Minimally invasive techniques can be helpful in certain patients in this population although the decrease in visualization can further complicate these techniques. Careful indications and surgical planning are paramount in reducing the morbidity and mortality of spine surgery in this population.
Discussion
Obesity has nearly tripled worldwide since 1975 with more than 1.9 billion adults now classified as overweight and, of these, nearly 650 million are considered obese. Along with this rise in the obese population, there has been an upward trend in the total number of spinal fusion procedures performed worldwide, with some literature showing that the highest incidence of spine surgeries was in the United States.18,19 Complication profiles from spine surgery within the obese population has been studied extensively in the past and is an ever-growing area of work as physicians attempt to decrease morbidity and mortality of these potentially life-altering surgeries.9,16 Morbidity, as well as the post-operative mortality, associated with spine surgeries has been shown to vary based on BMI as well as other comorbidities related to metabolic dysfunction including hypertension or hyperlipidemia.20,21 A systematic review of the effects of bariatric surgery showed that complication rates in spine surgery are lower in obese patients who lost weight via bariatric surgery compared to those who did not lose weight. 22
A significant limitation in treating these patients stems from the facility where the surgery is performed. Despite modifications to surgical approaches, many centers lack the necessary equipment to accommodate SMO patients. Operating tables, CT scanners, and MRIs all have weight limits that cannot be easily bypassed at every institution. Additionally, intraoperative imaging with an O-arm can be challenging in patients with broad shoulders or larger body frames, and minimally invasive equipment is limited by a maximum 10-centimeter tube length. This highlights that, despite surgical modifications, healthcare teams still face significant challenges when managing SMO patients.
With SMO patients being younger, ensuring the longevity of surgical instrumentation presents a unique challenge. Additionally, SMO patients gained more weight between their initial appointment and surgery compared to MO patients, adding complexity to operative planning. SMO patients also had higher rates of chronic kidney disease (CKD) and diabetes mellitus (DM), which could act as confounders for complications. However, subgroup analysis revealed no significant differences. Although none of the comorbidities had a P-value that showed significance, this is likely due to the high that our analysis was underpowered to detect their independent effects, a type 2 error. SMO patients had more than double the rates of diabetes, and nearly four times the rate of CKD compared to MO patients, and identifying BMI as an independent risk factor for complications is unjust based on our small sample size. There instead is likely a causal pathway that links SMO status to adverse outcomes, as SMO serves as a powerful composite proxy for a high-risk metabolic state. This metabolic state increases the risk for confounding comorbidities, which all leads to an increased complication risk, rather than BMI being an isolated risk factor.
One of the more important findings from this cohort relates to complication rates and discharge location. SMO patients had significantly more complications than MO patients when discharged home (P = 0.0002). There was no statistically significant difference in complication rates between the 2 groups when discharged to SNFs/rehab. However, MO patients discharged home had a significantly lower risk of post-operative complications compared to those discharged to SNFs or rehab (P < 0.005). In the SMO group, 33.3% of home dischargers experienced complications compared to 40% of those discharged to a rehabilitation center, or 8% discharged to a SNF. While this did not reach statistical significance due to the relatively small sample size, it may carry important clinical implications and warrants further study. Additionally, there may be patient-specific factors that influence both discharge disposition and complication risk. Our data showed a more than 12-fold increased risk of complications (RR = 12.2) when SMO patients were discharged home compared to MO patients, though the precision of this estimate is limited (95% CI 2.7-53.4). Although this suggests a real and large effect with the lower bound being 2.7, the exact magnitude is hard to determine without further studies with larger patient populations.
BMI is not the only factor that goes into determining the discharge location of patients undergoing spine surgery. There is an inherent selection bias in these cohorts for discharge location from clinicians that considers factors such as patient stability, functional status, and social support. This bias likely influences the results of the post-operative complication data, as the bias favors selection of healthier patients for home discharges. However, these “healthier patients” in the SMO group still had an overwhelmingly high rate (33% of the patients) of complications. This inherent selection bias makes the observed high complication rates in the SMO group even more clinically alarming.
From our institutional experience and the data presented, 2 potential strategies to mitigate complication risk in obese patients undergoing spine surgery include discharging to SNFs and encouraging preoperative weight loss, either through natural means or bariatric surgery. Other patient-specific considerations must also be considered when determining discharge location. Although not formally analyzed, SMO patients are also likely at greater risk for intraoperative pressure injuries due to positioning challenges.
Anecdotally, SMO patients have higher rates of discharge to skilled nursing facilities, longer recovery times and higher risks of wound complications. This all amounts to longer time away from home and could potentially lead to poorer functional outcomes and poorer perceived outcomes. To help appropriately set expectations, surgeons need to properly counsel patients preoperatively about the abovementioned risks including wound complications, longer hospital stays, discharge locations, and recovery times. This thorough preoperative counseling should be performed with both MO and SMO patients, and focus on the unique risks they face, and surgery should only proceed if patients fully understand and accept these risks.
Limitations
To date, this represents the largest institutional experience comparing spinal surgery outcomes in super morbidly obese (SMO) patients to those with morbid obesity (MO). However, the study is limited by its retrospective design and potential patient selection bias, which may affect the generalizability of the results. Follow-up time is short, and although our SMO cohort is relatively small, it remains one of the largest reported in the literature. Having longer follow-up of these patients could better stratify the long term complication profiles in this patient population and be better suited for determining clinical utility for pre- and post-operative treatments. A normal BMI comparison group was not included, though the complication profile for this subset is well documented elsewhere. Including institutional data from this group could better show associations between complication rates and BMI in this certain population and could potentially make it more generalizable to other institutions who serve similar patient populations. Additionally, the level of care at secondary facilities is unknown and may introduce confounding factors in the assessment of postoperative complications. Further studies are needed to expand the cohort, identify barriers to care in this population, and assess long-term outcomes with extended follow-up.
Conclusion
There is a high risk of post-operative complications in both MO and SMO patients who undergo spinal surgery although SMO are at an even greater risk of surgical complications. Despite the elevated risk of complications, these surgeries can be performed safely if appropriate risk mitigation strategies are undertaken, and thorough pre-operative counseling is provided to the patient. SMO patients have significantly more complications than their MO counterparts when discharged home. With a population that is increasing in size and number, and with advancements in surgical techniques, it is of utmost importance to modify our surgical and peri-operative approach to ensure the highest quality of care for SMO patients.
Footnotes
Ethical Considerations
This was a retrospective study approved by the universities Institutional Review Board. No ethical approval is required.
Consent to Participate
This was a retrospective cohort study approved by the universities IRB and no informed consent was required.
Author Contributions
Study design, conception, preparation, data collection, and analysis were performed by Jacob Ward, Seth Wilson, and David Xu. The original manuscript was written by Jacob Ward, Seth Wilson, Katelyn Sette, Matthieu Weber, and Ryan Eaton. All authors commented on previous versions, and approved the final version for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
Institutional Review Board number: #2023H0100.