
Abstract
Study Design
Systematic review and meta-analysis.
Objective
To establish and validate region-specific MRI-derived vertebral bone quality (VBQ) thresholds predictive of mechanical complications following cervical and lumbar spinal fusion.
Methods
PubMed, EMBASE, MEDLINE, and the Cochrane Library were searched to September 2025 for observational studies reporting VBQ in patients with and without postoperative mechanical complications. Data were pooled using random-effects models with Hartung–Knapp adjustment. Diagnostic accuracy was evaluated using a bivariate random-effects meta-analysis to estimate pooled sensitivity, specificity, diagnostic odds ratio (DOR), and area under the curve (AUC).
Results
Twenty-four studies comprising 3122 patients were included. Patients who developed complications had significantly higher VBQ scores (SMD = 1.13, 95% CI 0.91-1.35). Pooled diagnostic performance demonstrated strong discrimination (sensitivity = 0.79, specificity = 0.79, DOR = 14.6, AUC = 0.83). Accuracy was higher in cervical than lumbar cohorts (AUC = 0.89 vs 0.83). Region-specific thresholds of 2.75 for cervical and 3.22 for lumbar fusion optimally balanced sensitivity and specificity. Validation analyses confirmed progressively increasing complication risk above these cut-offs.
Conclusions
MRI-derived VBQ scores provide reliable, radiation-free predictors of mechanical complications after spinal fusion. Region-specific thresholds (2.75 cervical, 3.22 lumbar) offer clinically applicable tools for preoperative risk stratification and bone health optimisation.
Introduction
Vertebral bone quality (VBQ) is a major determinant of surgical success in both cervical and lumbar fusion, influencing construct stability, endplate integrity and susceptibility to mechanical failure. Reduced trabecular density and increased marrow fat weaken endplate strength, limit screw purchase, and impair load transfer thereby predisposing patients to subsidence, loosening, and fixation failure.1,2 Traditional assessment relies on dual-energy X-ray absorptiometry (DEXA) however, DEXA demonstrates global bone mineral density, with variable sensitivity in degenerative spines, and cannot assess local trabecular strength. 3 In contemporary spine practice, computed tomography (CT)–derived Hounsfield units (HU) have therefore emerged as a more practical and widely used proxy for local bone density and are increasingly viewed as reliable predictors of mechanical complications in spinal fusion. 4 However, CT assessment exposes patients to ionising radiation, and many patients undergoing cervical or lumbar fusion already receive multiple radiographic studies throughout their care. Concerns about cumulative radiation exposure, including elevated lifetime cancer risk in patients with repeated imaging highlight the clinical need for a reliable, radiation-free method of assessing bone quality. 5
Magnetic resonance imaging (MRI)–based assessment of VBQ offers a radiation-free alternative that captures marrow composition and trabecular integrity using routinely acquired preoperative scans. VBQ score, calculated from routine preoperative T1-weighted MRI, reflects marrow fat content and correlates strongly with DEXA-derived BMD.6,7 Elevated VBQ values have been associated with higher rates of cage subsidence, pedicle screw loosening, pseudarthrosis, and adjacent segment disease in spinal fusion cohorts.1,8-10 Despite its promise, adoption of VBQ in clinical practice has been limited by marked heterogeneity in measurement techniques, imaging protocols, patient populations, and reported thresholds.11-14 Proposed cut-off values vary widely, and unlike HU, no standardised or clinically validated VBQ threshold exists for predicting mechanical failure. 4 This variability has created uncertainty regarding how VBQ should be interpreted and applied in preoperative decision-making.
This systematic review and meta-analysis therefore aims to synthesise the available evidence to establish clinically meaningful and region-specific VBQ thresholds capable of predicting mechanical complications after cervical and lumbar spinal fusion. By identifying unified cut-off values and validating their diagnostic performance, this study seeks to provide a practical, radiation-free tool for preoperative risk stratification and optimisation of bone health in patients undergoing fusion surgery.
Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Literature Search
A comprehensive search of PubMed, EMBASE, MEDLINE, and the Cochrane Library was performed for published studies until September 2025 to identify studies evaluating VBQ in relation to mechanical complications following spinal fusion. The search strategy combined Medical Subject Headings (MeSH) and free-text terms including “vertebral bone quality,” “VBQ,” “magnetic resonance imaging,” “cage subsidence,” “junctional kyphosis,” “adjacent segment disease,” “mechanical failure,” and “spinal fusion”. Boolean operators were applied to refine results, and reference lists of included articles were screened manually to capture additional studies. Two independent reviewers conducted all searches, screenings, and eligibility assessments, resolving disagreements by consensus.
Study Selection
Observational studies comparing quantitative MRI-derived bone quality metrics from preoperative MRI between patients who developed mechanical complications and those who did not following cervical or lumbar fusion were included. As no randomised controlled trials were available, both retrospective and prospective cohort designs were eligible. One study measured VBQ at the S1 level. Given that S1 demonstrates comparable threshold values and diagnostic accuracy to L1–L4, this was classified under the lumbar subgroup for consistency. Related MRI-based indices, such as modified VBQ and endplate bone quality scores, were excluded to avoid heterogeneity. Exclusion criteria were non-fusion spinal procedures, studies involving corpectomy, and reports lacking extractable quantitative results.
Data Extraction and Quality Assessment
Two reviewers independently extracted data using a predefined form recording study characteristics, spinal region, sample size, number of events, VBQ means and standard deviations, diagnostic thresholds, sensitivity, specificity, and AUC. Extracted data were cross-checked for accuracy, and discrepancies were resolved by consensus. Methodological quality was appraised using the Newcastle–Ottawa Scale (NOS) for observational studies.
Statistical Analysis
All analyses were conducted using R (version 4.4.1) with the meta (v8.2) and mada packages. Continuous outcomes were synthesised as standardised mean differences (Hedges g) between event and non-event groups using a random-effects model with the restricted maximum-likelihood estimator and Hartung–Knapp adjustment. Heterogeneity was assessed using the I2 and τ2 statistics, and 95% prediction intervals were calculated to estimate the expected range of effects across future populations.
For diagnostic accuracy data, a bivariate random-effects meta-analysis was used to derive pooled sensitivity, specificity, diagnostic odds ratios, and summary receiver operating characteristic (SROC) curves. Reported VBQ thresholds were synthesised to identify convergent cutoff values, and pooled mean thresholds were used to define low, balanced, and high cutoffs (±1 standard deviation). Study-level distributions were reconstructed to generate dichotomised 2 × 2 tables, which were meta-analysed using random-effects models (Mantel–Haenszel method, Hartung–Knapp correction) to obtain pooled odds ratios. Diagnostic performance was summarised using sensitivity, specificity, Youden’s J, and area under the curve (AUC). Publication bias was assessed visually with funnel plots and statistically using Egger’s regression test.
Results
The primary database search led to one hundred and twenty-seven studies, of which one hundred and three were excluded. The final review included twenty-four studies (Figure 1). PRISMA flow chart detailing study selection
Characteristics and Demographics of Included Studies
Characteristics of Included Studies
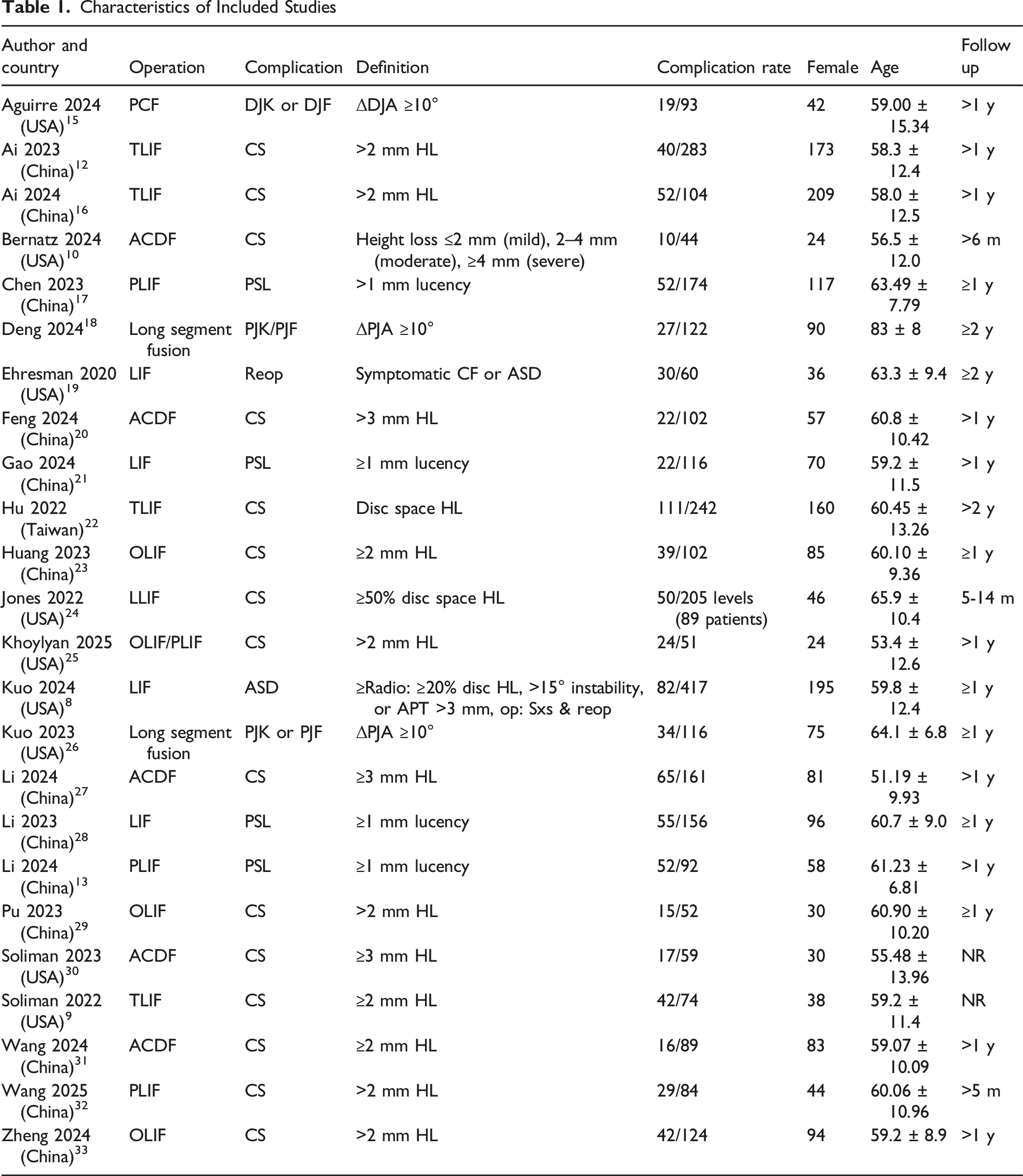
Methodological Quality of Included Studies
All included studies demonstrated generally high methodological quality according to the NOS. Total scores ranged from 6 to 9 out of a possible 9 points. Twenty studies (83%) achieved a score of 9, indicating low risk of bias, while three studies scored 7 and one study scored 6, reflecting moderate quality due to limited comparability or incomplete outcome reporting. Most studies achieved full marks for selection and outcome domains, whereas comparability was the main area of variability, often reflecting lack of adjustment for potential confounders. Overall, the evidence base was considered methodologically robust with predominantly low risk of bias across included studies (Supplemental table 1).
VBQ Scores Across Complications
Across 24 studies (6 cervical and 18 lumbar), patients who experienced mechanical complications demonstrated significantly higher mean VBQ scores compared with those without complications. Pooled analysis yielded a standardised mean difference (SMD) of 1.13 (95% CI: 0.91-1.35, P < 0.001), indicating consistently poorer vertebral bone quality among the complication group. Between-study heterogeneity was significant overall and in subgroups, reflecting variability across spinal regions and measurement protocols. Subgroup analysis by spinal region showed a substantially larger association in the cervical cohort than in the lumbar cohort. In cervical studies, patients with complications had markedly higher VBQ scores (SMD = 1.65, 95% CI 0.98-2.33), whereas the lumbar subgroup showed a more modest difference (SMD = 0.99, 95% CI 0.79-1.19). The between-subgroup difference was statistically significant (P = 0.0181), indicating effect modification by region (Figure 2). VBQ scores across complications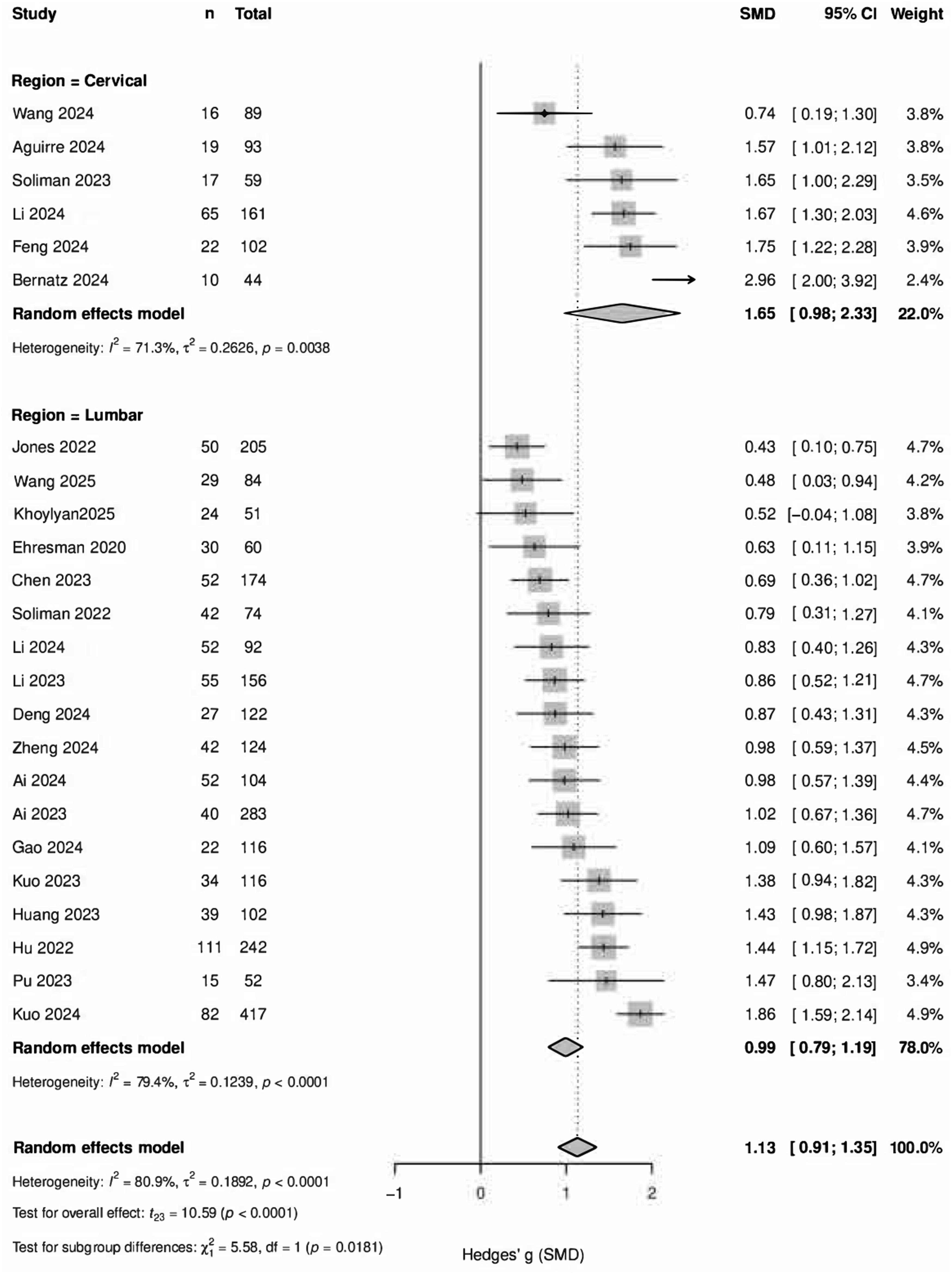
Pooled Diagnostic Metrics Across Regions
Predictive Performance


Overall, cervical, and lumbar SROC curves
Cervical Threshold Generation and Validation
Utility of Cervical Thresholds


Forest plot representing increasing complication odds from low, balanced, and high cervical VBQ thresholds
Lumbar Threshold Generation and Validation
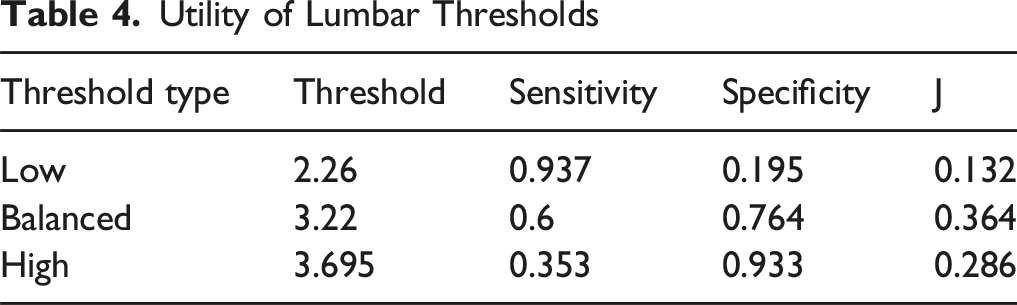
Utility of Lumbar Thresholds
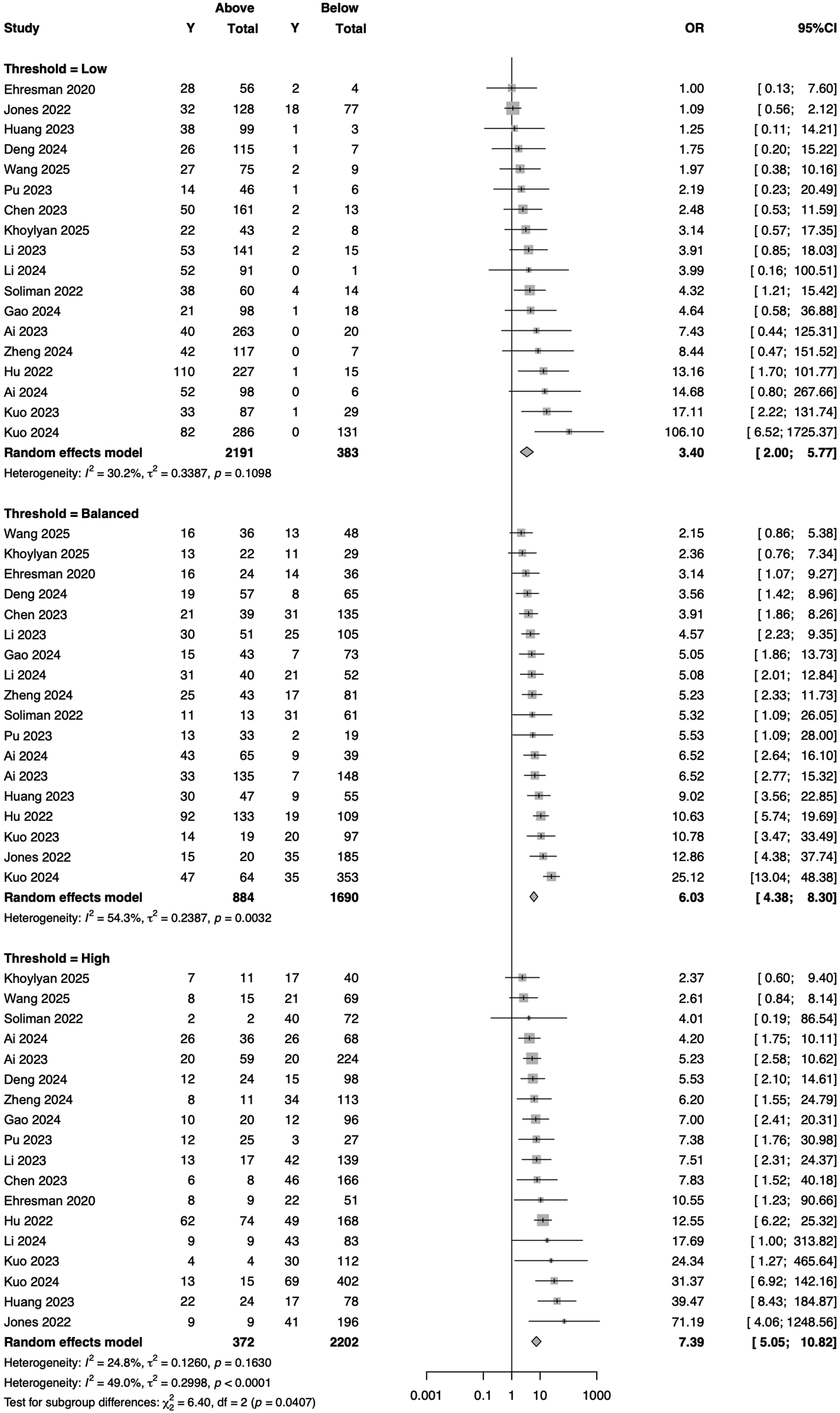
Forest plot representing increasing complication odds from low, balanced, and high lumbar VBQ thresholds
Publication Bias
Egger’s Regression Test for Publication Bias

Funnel plot for assessing publication bias
Discussion
This systematic review and meta-analysis provides the most comprehensive synthesis to date of MRI-derived VBQ as a predictor of mechanical complications following spinal fusion. Across 24 studies and 3172 patients, higher VBQ was consistently associated with postoperative mechanical failure, and diagnostic threshold analyses yielded clinically usable cut-offs for both the cervical and lumbar spine. The pooled continuous-effect estimate showed that patients who developed complications had significantly higher VBQ values than those who did not. This association remained consistent across spinal regions, although the effect size differed significantly, with a substantially stronger relationship observed in the cervical subgroup compared with the lumbar subgroup. Diagnostic meta-analysis further showed good overall discrimination, with slightly superior accuracy in the cervical spine (AUC 0.894) compared with the lumbar spine (AUC 0.831). Between-study heterogeneity was modest, and no evidence of publication bias was identified.
Threshold synthesis produced clinically meaningful cut-offs for both spinal regions. In the cervical spine, the balanced threshold of 2.75 provided the best compromise between sensitivity and specificity, while sensitivity- and specificity-optimised points were 1.87 and 3.21, respectively. In the lumbar spine, a balanced threshold of 3.22 achieved optimal overall discrimination, with 2.26 and 3.70 marking the sensitivity- and specificity-optimised bounds. Validation analyses confirmed a stepwise rise in complication risk with increasing VBQ, with odds ratios escalating from 5.46 at the low threshold to 21.23 at the high threshold in the cervical spine, and from 3.4 to 7.39 in the lumbar spine. These findings indicate a clear graded relationship, whereby increasing VBQ reflects greater fatty marrow conversion and reduced trabecular density, which are associated with a progressively higher likelihood of mechanical failure (Figure 7). Risk stratification across cervical and lumbar thresholds
The stronger association observed in the cervical spine is both biologically and biomechanically plausible. The cervical vertebral endplates, particularly their central regions, are thin and exhibit reduced load-bearing capacity. 34 Because interbody cages engage a smaller contact area in the cervical spine, even minor reductions in bone quality can lead to disproportionately higher localised stress at the cage–endplate interface.34,35 Moreover, cervical fusion constructs, particularly single-level ACDFs, rely predominantly on the cage–endplate interface to maintain height and alignment, whereas lumbar constructs typically benefit from the stabilising influence of bilateral pedicle-screw fixation, which distributes axial loads more evenly across the construct. 36 Consequently, even subtle losses in cervical endplate integrity can precipitate focal collapse or segmental kyphosis. Because the cervical spine has limited compensatory mechanisms, small height reductions at a single level can propagate into loss of global lordosis, altered sagittal balance, and increased strain at adjacent levels.37,38 Collectively, these factors magnify the clinical and radiographic consequences of diminished trabecular strength in the cervical region, explaining the stronger relationship between VBQ and mechanical failure compared with the lumbar spine.
The CT-based HU literature provides a strong external comparator for interpreting the diagnostic performance and clinical applicability of our VBQ thresholds. Multiple pooled analyses have consistently demonstrated that patients who experience mechanical or junctional complications following spinal fusion possess significantly lower vertebral HU values than those without complications, averaging around 120 HU compared with 150 HU in controls. 14 A global HU threshold of approximately 118 HU has been shown to predict complications with a sensitivity of 73%, specificity of 64%, and an almost threefold increase in mechanical or junctional failure below this level. Our findings parallel these results closely, as VBQ thresholds demonstrated similar diagnostic accuracy, with balanced sensitivity and specificity near 0.8 and a pooled AUC of 0.83, indicating that MRI-derived bone quality offers predictive capability comparable to CT-based assessments. While HU possesses a slightly higher AUC as demonstrated in a recent meta-analysis, this difference is unlikely to hold clinical significance and is offset by VBQ’s radiation-free nature, opportunistic acquisition, and integration into standard preoperative MRI protocols, particularly when CT is not routinely obtained. 39
The present results justify integrating VBQ into routine preoperative interpretation, particularly in cervical fusion candidates. Region-specific thresholds can be translated into simple clinical bands that trigger actionable steps. Patients above the cervical balanced or high thresholds are plausible candidates for larger-footprint cages to maximise endplate coverage, meticulous endplate preparation that preserves the subchondral plate, and alignment-restorative strategies that avoid over-distraction.39-42 In lumbar constructs, elevated VBQ should prompt consideration of load-sharing strategies, supplemental fixation, or cement augmentation in severe compromise. 43 In both regions, high VBQ should trigger systematic bone-health optimisation, including assessment for secondary causes, correction of calcium and vitamin D deficiency, and initiation of antiresorptive or anabolic therapy where indicated. Because VBQ and HU capture complementary aspects of skeletal competence, marrow composition and mineral density, respectively, centres with access to both modalities can combine them to refine risk stratification. Discordant patterns, such as normal HU with elevated VBQ, may flag early marrow fat infiltration preceding mineral loss; concordant impairment across both modalities identifies a red-flag phenotype warranting augmented fixation and closer postoperative surveillance.
A major limitation to the widespread clinical application of VBQ has been its dependence on MRI scanner characteristics and magnetic field strength, particularly the discrepancy between 1.5 T and 3.0 T systems. The recently proposed calibrated-VBQ technique addresses this limitation by normalising vertebral marrow signal intensity to cerebrospinal fluid and subcutaneous fat on T1-weighted images, thereby producing a field-independent and unitless measure. 44 Comparative analyses have shown that calibrated-VBQ remains consistent across magnetic field strengths, exhibits stronger correlations with QCT-derived bone mineral density, and offers improved diagnostic accuracy for osteoporosis relative to conventional VBQ. 44 Within the context of our meta-analysis, such standardisation has direct relevance for threshold generation and validation; by minimising scanner-related variability, calibrated-VBQ could reduce between-study dispersion and yield more reproducible cervical and lumbar thresholds. This approach therefore represents an important methodological advance toward establishing unified, transferable VBQ reference values across centres and imaging platforms.
This study has several limitations that warrant consideration. All included studies were observational, which introduces potential confounding from demographic, surgical, and implant-related variables. There was also variation in MRI acquisition parameters, region of interest placement, and signal normalisation methods, which may have contributed to between-study heterogeneity. Moreover, although the aim was to provide general thresholds for various complications, the included literature encompassed a wide range of mechanical outcomes such as subsidence, screw loosening and junctional failure, each defined using different radiographic or clinical criteria, which limits direct comparability across studies. These outcomes are also influenced by factors such as implant design, cage footprint, surgical technique, and alignment targets, which could not be standardised or adjusted for in the available evidence. Due to the paucity of studies, subgroup analyses per complication were not feasible. Additionally, cervical fusion data were particularly limited, with relatively few studies and smaller sample sizes compared to lumbar cohorts, which may have influenced the precision of region-specific estimates. Finally, reconstructing diagnostic data from reported means and standard deviations assumes normal distributions and may not fully account for study-level variability. Future research should focus on prospective, multicentre validation of these VBQ thresholds using standardised measurement protocols, uniform complication definitions, and direct comparisons with CT-based bone quality metrics.
Conclusion
In conclusion, MRI-derived VBQ may potentially provide a reliable, radiation-free biomarker of vertebral bone quality that demonstrates strong predictive accuracy for mechanical complications after spinal fusion. The region-specific thresholds identified in this meta-analysis offer clinically actionable values for preoperative risk stratification, supporting the incorporation of VBQ into surgical planning and perioperative bone health optimisation.
Supplemental Material
Supplemental material - Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis
Supplemental material for Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis by Omar Lubbad, Akram Hagos, Yahya El-Tahlawy, Laila Lubbad, Giuseppe L Morassi and Nektarios K Mazarakis in Global Spine Journal
Supplemental Material
Supplemental material - Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis
Supplemental material for Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis by Omar Lubbad, Akram Hagos, Yahya El-Tahlawy, Laila Lubbad, Giuseppe L Morassi and Nektarios K Mazarakis in Global Spine Journal
Supplemental Material
Supplemental material - Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis
Supplemental material for Establishing and Validating Cervical and Lumbar Vertebral Bone Quality Thresholds for Predicting Mechanical Complications in Patients Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis by Omar Lubbad, Akram Hagos, Yahya El-Tahlawy, Laila Lubbad, Giuseppe L Morassi and Nektarios K Mazarakis in Global Spine Journal
Footnotes
Author Contributions
OL: Inception, data collection, analysis and manuscript writing, AH, YE: Data collection, LL: Manuscript writing, GM and NM: Manuscript proofreading and supervision
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data collected and generated is within the manuscript or its supplementary data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.