
Abstract
Study Design
This study is a meta-analysis of randomized controlled trials (RCTs) and observational studies.
Objective
Lumbar disc herniation (LDH) often requires surgery, with microdiscectomy (MD) being common. This study compares Unilateral Biportal Endoscopic Discectomy (UBED) to conventional and tubular MD for LDH treatment.
Methods
PubMed, Cochrane Central, and ScienceDirect were searched up to May 2025. Mean differences (MDs) and risk ratios (RRs) were pooled with a random effects model using Review Manager. Quality was assessed using the Cochrane risk of bias tool and the Newcastle-Ottawa Scale. Publication bias was evaluated with funnel plots and Egger’s regression test.
Results
Thirteen studies (11 observational studies and 2 RCTs), pooling 1369 patients, were included. UBED was associated with decreased 1-3 days post-operative (MD: −0.81; 95% CI: [−1.48, −0.14]; P = 0.02) and 12 months post-operative (MD: −0.37; 95% CI: [−0.74, −0.01]; P = 0.04) VAS back pain scores, 12 months post-operative ODI scores (MD: −1.32; 95% CI: [−2.44, −0.19]; P = 0.02), estimated blood loss (MD: −74.42; 95% CI: [−114.11, −34.73]; P = 0.0002), and hospital stay (MD: −1.81; 95% CI: [−2.99, −0.63]; P = 0.003) compared to conventional MD although the operative time was high (MD: 9.07; 95% CI: [1.66, 16.48]; P = 0.02). Concurrently, the 12 months post-operative VAS back pain score (MD: −0.42; 95% CI: [−1.40, 0.56]; P = 0.40) and ODI score (MD: 1.39; 95% CI: [−2.80, 5.58]; P = 0.52) along with the operative time (MD: 21.80; 95% CI: [−26.31, 69.92]; P = 0.37) and hospital stay (MD: 0.02; 95% CI: [−0.30, 0.33]; P = 0.92) were comparable between the UBED and tubular MD. The VAS leg pain scores were comparable between UBED and both conventional and tubular MD.
Conclusion
UBED may be associated with reduced early and long-term back pain, disability, blood loss, and hospital stays compared to conventional MD, but has longer surgery times, with comparable outcomes to tubular MD. More large-scale RCTs are required to validate these results.
Keywords
Introduction
Lumbar disc herniation (LDH) is a common spinal disorder caused by the degeneration and rupture of the annulus fibrosus, the outer layer of the intervertebral disc, often resulting in nerve root compression and leading to lower back pain, numbness in the lower extremities, and reduced mobility, which significantly affects the patient’s quality of life.1,2
Surgery serves as the mainstay treatment for patients unresponsive to conservative therapy, those with severe disease, or neurological impairment. Although traditional open surgery involves extensive paravertebral muscle dissection, often resulting in significant trauma, spinal instability, and higher complication rates, minimally invasive techniques have emerged as effective alternatives with reduced tissue damage and recovery time.3,4
Microdiscectomy (MD) is a widely performed, minimally invasive surgery for LDH. 5 While effective, it carries potential complications, including infection, bleeding, nerve injury, scar tissue formation, and disc re-herniation, which may impact postoperative recovery and mobility.6,7 Recurrence after MD remains a significant concern, reported in 5-15% of cases. 8
Unilateral Biportal Endoscopic Discectomy (UBED), closely related to the modern Unilateral Biportal Endoscopy (UBE) technique, is an emerging minimally invasive surgical method for LDH that employs an arthroscopic system. 9 It utilizes standard spinal instruments, requiring less specialized equipment than traditional procedures. 10 A key feature of UBED is its dual-portal system, one for endoscopic visualization and another for instrumentation, providing superior maneuverability and visualization while preserving surgical familiarity.11,12 This technique has shown promising benefits, including reduced blood loss, quicker recovery, shorter hospital stays, and favourable early clinical outcomes with minimal postoperative pain 13. Moreover, UBED results in less bone and ligament resection, thereby preserving crucial posterior spinal structures and maintaining spinal stability. 12
Despite its benefits, UBED is still less widely adopted than MD. As a new method for treating LDH, there are no established guidelines for its clinical use, which emphasizes the need for an updated meta-analysis to compare UBED with MD (both standard and tubular). Consequently, this study aims to evaluate whether UBED yields better or comparable outcomes compared to the standard MD or tubular MD in LDH treatment.
Methods
This meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 14 and followed the Cochrane Handbook of Systematic Reviews. 15 The protocol of this review was registered on PROSPERO under the ID: [CRD420251104497].
Data Sources and Search Strategy
A systematic search was conducted in PubMed, Cochrane Central, and ScienceDirect databases from inception to May 2025. Additionally, we examined the reference lists of included studies and relevant systematic reviews to identify additional studies. The Medical Subject Headings (MeSH) and keywords used were: “unilateral biportal endoscopy discectomy”, “UBED”, “two portal endoscopic spinal surgery”, “biportal endoscopy”, “microscopic discectomy”, “microdiscectomy”, “tubular microdiscectomy”, “lumbar disc herniation”, and “lumbosacral”. Details of the individual search strategies used across various electronic databases were provided in Supplemental Table 1.
Eligibility Criteria and Study Selection
The inclusion criteria were: (1) Population: Patients aged 18 years or older diagnosed with LDH requiring surgery; (2) Intervention: UBED; (3) Comparison group: MD (including both conventional and tubular subtypes); (4) Outcomes: Visual Analog Scale (VAS) scores for back and leg pain, Oswestry Disability Index (ODI) scores, operation time, estimated blood loss, length of hospital stay, and MacNab score; (5) Study designs: randomized controlled trials (RCTs) and cohort studies. Studies were excluded if they had a design other than RCTs or cohort studies, or were conducted on animals, or were only available as abstracts. No language restrictions were applied.
All the articles identified in our search were imported into EndNote version 20, and any duplicates were eliminated. Two independent reviewers (A.H. and M.K.) screened the titles and abstracts, excluding irrelevant studies. Full-text screening was then performed in accordance with the eligibility criteria. A third reviewer (M.H.W.) resolved disagreements. The detailed study selection process is illustrated in the PRISMA flowchart (Figure 1). PRISMA flowchart of the study selection process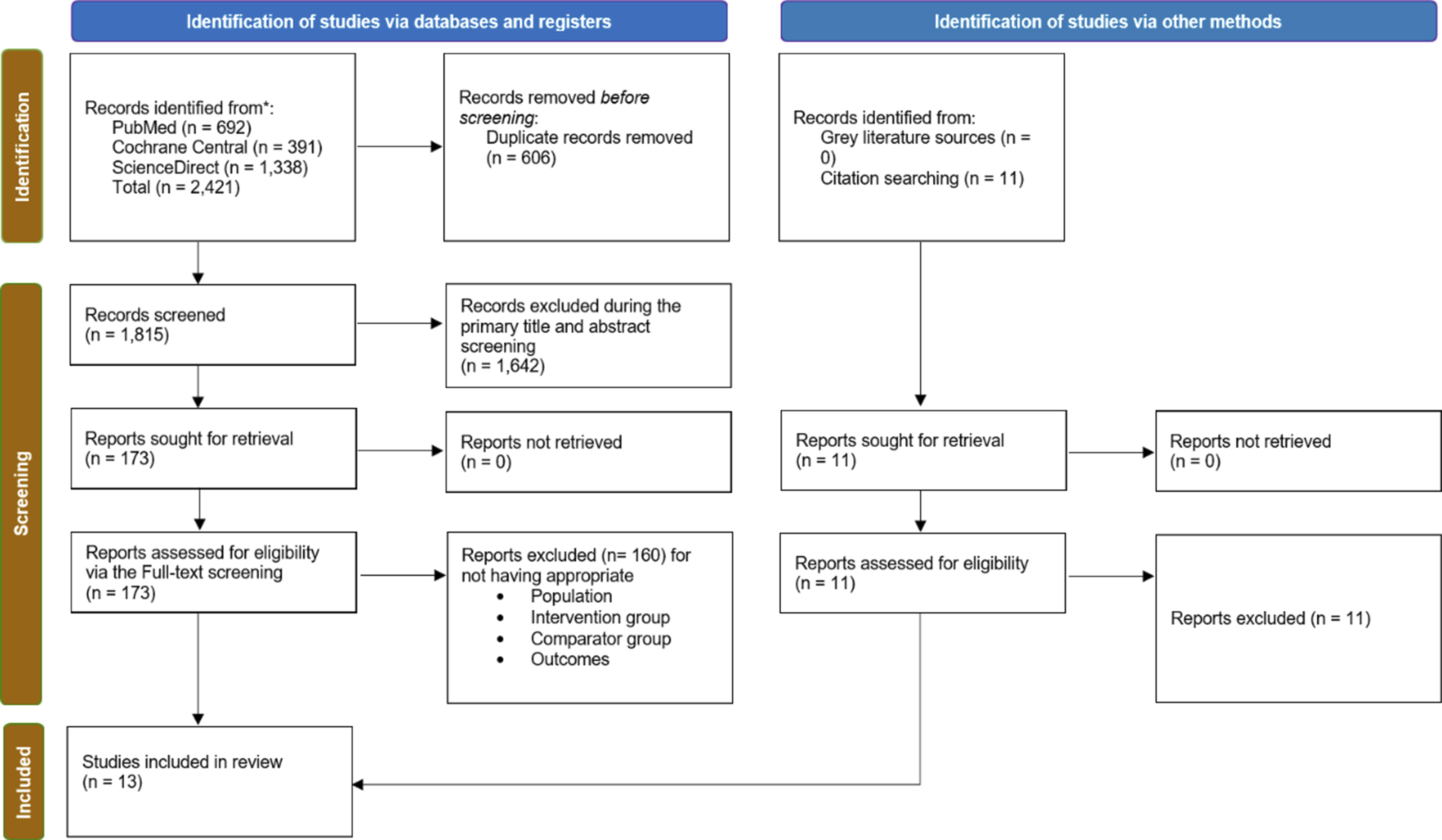
Data Extraction
Data were extracted on an Excel sheet by two authors independently (Z.U.A. and Z.A.). The baseline characteristics extracted included study ID, location, study design, sample size, age, sex, preoperative VAS Back scores, preoperative VAS Leg scores, preoperative ODI scores, and operation levels. Outcomes extracted were VAS for back and leg pain, ODI, operative time, estimated blood loss, length of hospital stay, and MacNab score. These measures collectively evaluate pain relief, functional improvement, surgical efficiency, perioperative safety, recovery speed, and overall patient satisfaction in the management of LDH.
Quality Assessment
Two authors (R.A. and M.A.) independently assessed the quality of the included studies using established tools. Randomized controlled trials (RCTs) were evaluated using the Cochrane Collaboration tool for risk of bias (RoB 2.0), 16 which examines factors such as random sequence generation, allocation concealment, and blinding. Observational studies were assessed using the Newcastle-Ottawa Scale (NOS), 17 with scores of 7 or higher indicating high quality. Any discrepancies in the assessment process were resolved through consensus or by consultation with a senior author (M.H.W.).
Statistical Analysis
Statistical analyses were performed using the Review Manager software (RevMan 5.4.1) under the random-effects model. Continuous outcomes were pooled and reported as mean differences (MDs) with 95% confidence intervals (CIs). Dichotomous outcomes were analyzed using risk ratios (RRs). A P-value of <0.05 was deemed statistically significant. Heterogeneity across studies was assessed using the Higgins I2 statistics 18 and Cochrane Q statistics. For outcomes with heterogeneity exceeding 50%, we investigated potential causes through leave-one-out sensitivity analysis. For publication bias, the Egger’s test was performed using the Comprehensive Meta Analysis software, version 3, with a P-value <0.05 indicating statistically significant publication bias. GRADE assessment was performed using GRADEpro GDT software to assess the certainty of the evidence. 19 The endpoints were assessed at specific postoperative intervals, namely 1-3 days, 1-3 months, and 12 months. Additionally, subgroup analyses were carried out by study design (observational studies or RCTs) and MD type (standard or tubular).
Results
Study Selection
An initial electronic database search identified 2421 studies. After removing duplicates (n = 606), 1815 unique records remained and were screened based on their titles and abstracts. This led to the exclusion of 1642 studies. The remaining 173 articles were then evaluated through full-text review. Of these, 160 studies were excluded, and ultimately, 13 studies20-32 fulfilled the predefined eligibility criteria and were included in the final meta-analysis. The excluded studies and reasons for their exclusion are provided in Supplemental Table 2. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
Study Characteristics
Baseline Characteristics of Included Studies
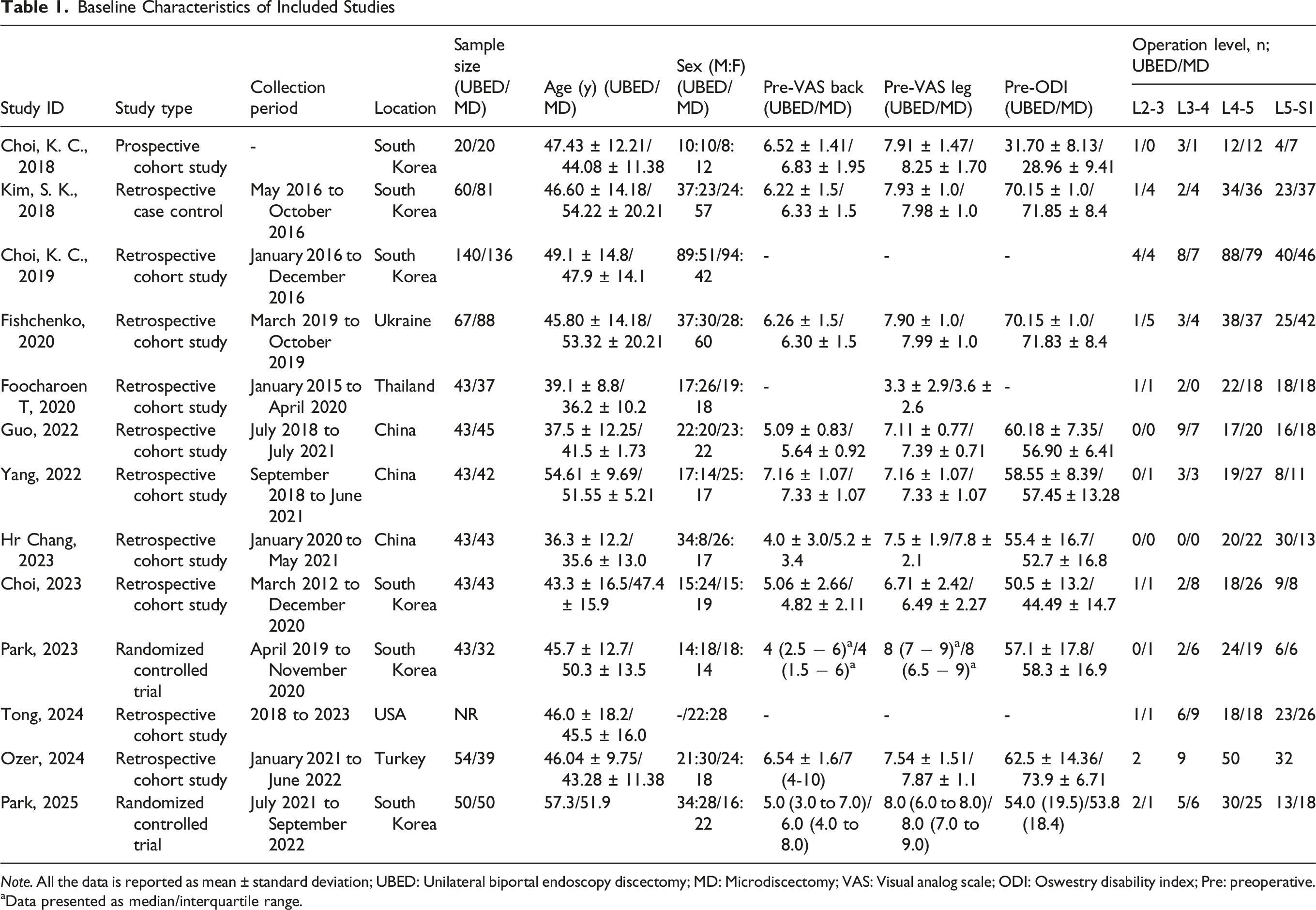
Note. All the data is reported as mean ± standard deviation; UBED: Unilateral biportal endoscopy discectomy; MD: Microdiscectomy; VAS: Visual analog scale; ODI: Oswestry disability index; Pre: preoperative.
aData presented as median/interquartile range.
Outcomes
Summary of Meta-Analysis

Note. VAS: Visual analog scale; ODI: Oswestry disability index; MD: Mean difference; df: Degree of freedom.
aRisk ratio.
VAS Back Pain
A total of six observational studies, encompassing 581 patients (UBED: 262; MD: 319), evaluated VAS back pain at 1-3 days postoperatively as an outcome. Our pooled analysis revealed that UBED was associated with a significant reduction in VAS back pain score (MD: −0.81; 95% CI: [−1.48, −0.14]; P = 0.02). High heterogeneity(I2 = 95%) was observed among the studies (Figure 2A). Forest plot for visual analog scale (VAS) back pain score (A) 1-3 days post-operative, (B) 1-3 months post-operative, (C) 12 months post-operative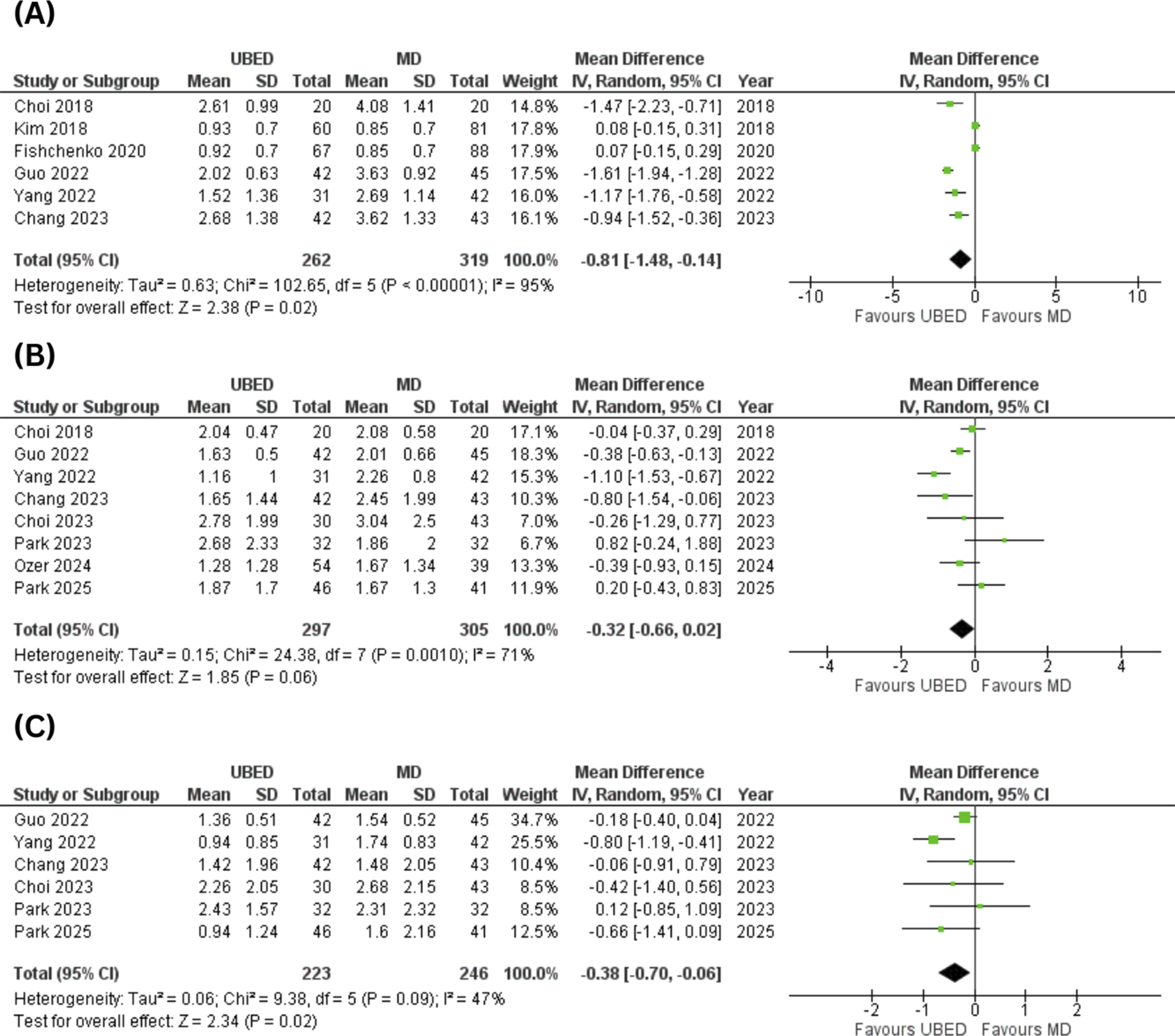
A total of eight studies (six observational studies and two RCTs), including 602 patients (UBED: 297; MD: 305), assessed VAS back pain at 1-3 months. Our analysis showed that this outcome was comparable between the two groups (MD: −0.32; 95% CI: [-0.66, 0.02]; P = 0.06; I2 = 71%) (Figure 2B).
Data on VAS back pain 12 months postoperatively were reported in six studies (four observational studies and 2 RCTs), including 469 patients (UBED: 223; MD: 246). Our analysis revealed that patients with UBED had significantly lower VAS back pain scores I2 months postoperatively compared to patients with MD (MD: −0.38; 95% CI: [−0.70, −0.06]; P = 0.02; I2 = 47%) (Figure 2C).
VAS Leg Pain
A total of six observational studies, comprising 581 patients (UBED: 262; MD: 319), assessed VAS leg pain 1-3 days postoperatively as an outcome. Our analysis showed that this outcome was comparable between the two groups (MD: −0.19; 95% CI: [−0.49, 0.12]; P = 0.24; I2 = 68%) (Figure 3A). Forest plot for visual analog scale (VAS) leg pain score (A) 1-3 days post-operative, (B) 1-3 months post-operative, (C) 12 months post-operative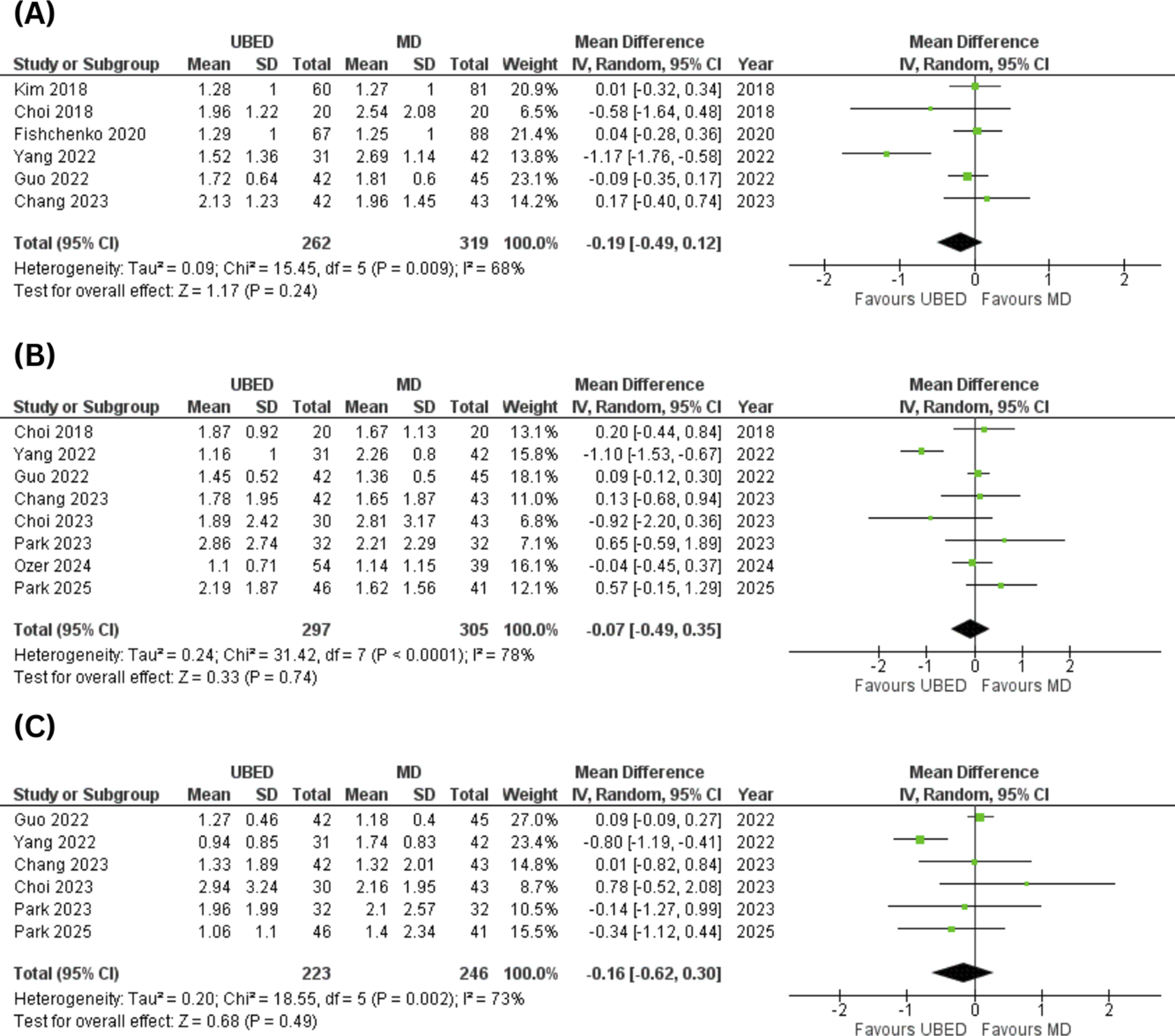
Eight studies (six observational studies and two RCTs), including a total of 602 patients (UBED: 297; MD: 305), assessed the VAS leg pain score at 1-3 months. Pooled analysis revealed that VAS leg pain-1-3 months postoperative was comparable between the two groups (MD: −0.07; 95% CI: [−0.49, 0.35]; P = 0.74; I2 = 78%) (Figure 3B).
Six studies (four observational studies and two RCTs), including 469 patients (UBED: 223; MD: 246), assessed the VAS leg pain score at 12 months postoperatively as an outcome. No significant difference was observed between the two groups (MD: −0.16; 95% CI:[-0.62, 0.30]; P = 0.49; I2 = 73%) (Figure 3C).
ODI
A total of three observational studies, involving 369 patients (UBED: 158; MD: 211), examined ODI 1 week postoperatively. The pooled MD was −1.09 (95% CI: [−4.08, 1.90]; P = 0.47; I2 = 60%), indicating no significant difference in ODI at 1 week postoperatively between the two groups (Figure 4A). Forest plot for oswestry disability index (ODI) score (A) 1-week post-operative, (B) 1-3 months post-operative, (C) 12 months post-operative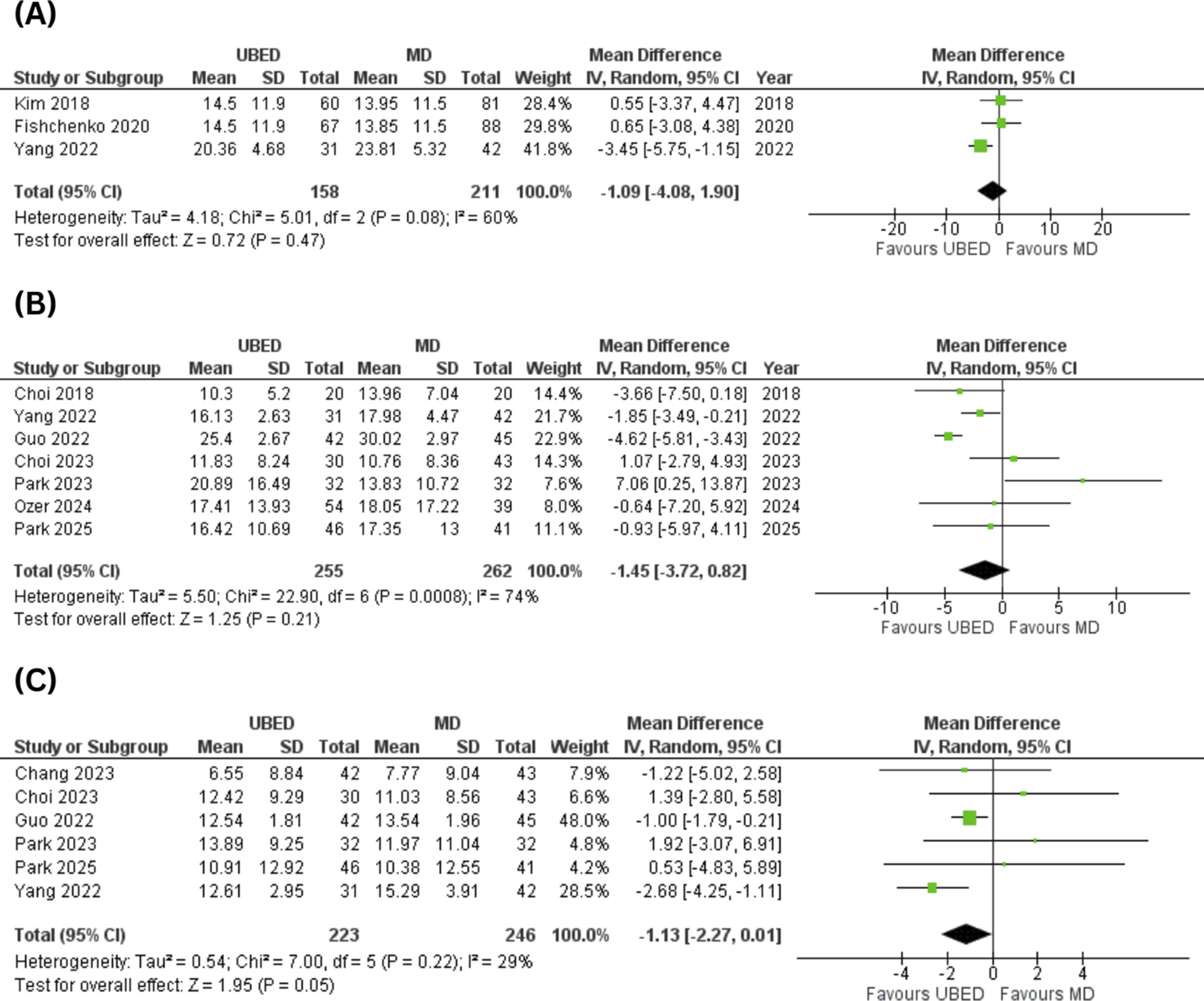
ODI 1-3 months postoperatively was reported in seven studies (five observational studies and two RCTs), involving a total of 517 patients (UBED: 255; MD: 262). No significant difference was observed in ODI 1-3 months postoperative between the two groups (MD: −1.45; 95% CI:[-3.72, 0.82]; P = 0.21; I2 = 74%) (Figure 4B).
Six studies (four observational studies and two RCTs), including 469 patients (UBED: 223; MD: 246), evaluated ODI at 12 months as an outcome. The pooled analysis revealed no significant difference between the two groups (MD: −1.13; 95% CI: [−2.27, 0.01]; P = 0.05; I2 = 29%) (Figure 4C).
Operation Time
Thirteen studies (11 observational studies and 2 RCTs), including 1356 patients (UBED: 655; MD: 701), assessed operation time as an outcome. Pooled analysis revealed that UBED is associated with a significant increase in operation time (MD: 11.12; 95% CI: [3.45, 18.79]; P = 0.005). High heterogeneity (I2 = 93%) was observed among the studies (Figure 5). Forest plot for operative time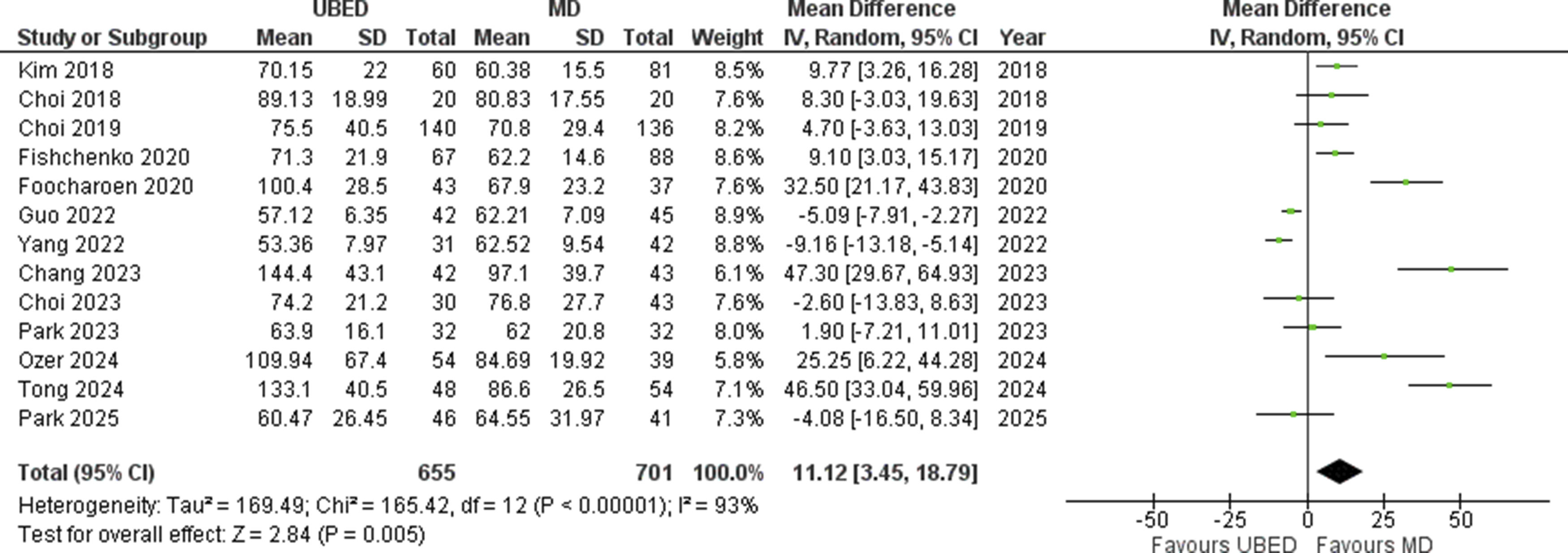
Estimated Blood Loss
Four observational studies, including 456 patients (UBED: 200; MD: 256), assessed estimated blood loss. The pooled MD was −74.42 (95% CI: [−114.11, −34.73]; P = 0.0002), indicating that UBED is associated with a significant decrease in estimated blood loss as compared to MD. High heterogeneity (I2 = 99%) was noted among the studies (Figure 6). Forest plot for estimated blood loss
Hospital Stay
Data on hospital stay were reported by twelve studies (10 observational studies and 2 RCTs), including a total of 1269 patients (UBED: 613; MD: 656). Analysis revealed that UBED is associated with a significant decrease in hospital stay compared to MD (MD: −1.47; 95% CI: [−2.50, −0.44]; P = 0.005). High heterogeneity (I2 = 98%) was observed among the studies (Figure 7). Forest plot for hospital stay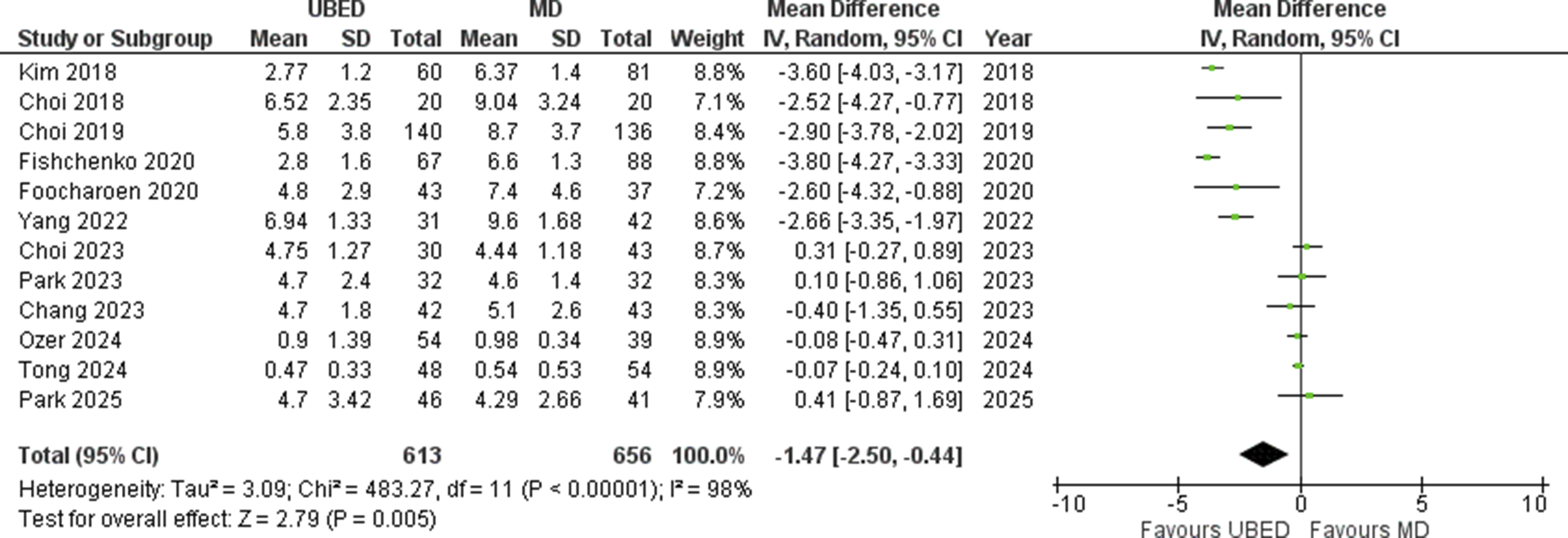
MacNab Score
Six observational studies, including 641 participants (UBED: 308; MD: 333), evaluated the MacNab score as an outcome. No significant difference was observed in MacNab scores between the two groups (RR: 1.05; 95% CI:[0.99, 1.12]; P = 0.10; I2 = 0%) (Figure 8). Forest plot for MacNab score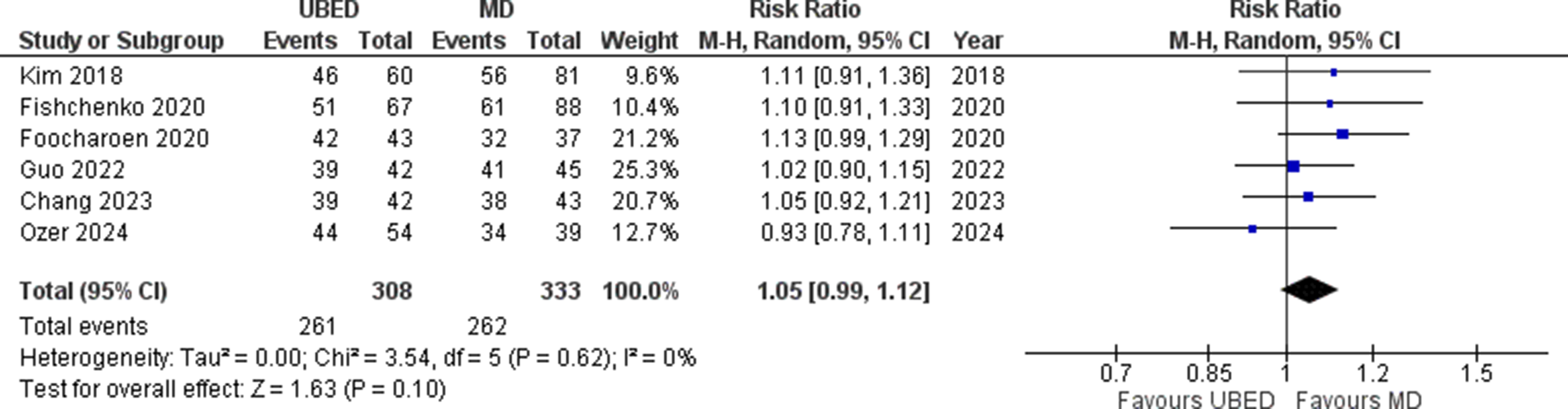
Quality Assessment
We performed the quality assessment for 2 RCTs28,31 using the Rob 2 tool, which demonstrated a high risk of bias. The quality of 11 observational studies was assessed using the NOS, 17 with scores ranging from 7 to 9, indicating good quality. The details regarding quality assessment were given in Supplemental Figure 1 and Supplemental Table 3.
Subgroup Analysis
The subgroup analysis of the included endpoints was conducted by MD type (conventional or tubular) and study design (observational studies or RCTs).
On subgrouping based on the MD subtype, most results remain unchanged. However, the pooled VAS back pain score at 12 months post-op was no longer significant in the tubular MD subgroup (Supplemental Figure 2). The ODI score at 12 months post-op became significantly lower (MD = −1.32; P = 0.02) in the conventional MD group (Supplemental Figure 3). The pooled results for operating time lost significance (P = 0.37) in the tubular MD subgroup (Supplemental Figure 4), and the hospital stay also became insignificant (P = 0.92) in this subgroup (Supplemental Figure 5).
On subgroup analysis based on study design, most results remained consistent, with some exceptions: the VAS back pain score at 1-3 months post-op became significant (P = 0.005) in the observational studies subgroup (Supplemental Figure 6); the VAS back pain score at 12 months post-op was no longer significant in both observational and RCTs subgroups (Supplemental Figure 7); the ODI score at 1-3 months (Supplemental Figure 8) and 12 months post-op (Supplemental Figure 9) showed significant decreases in the observational studies subgroup (P values 0.02 and 0.03 respectively); the pooled operating time results lost significance (P = 0.96) in the RCTs subgroup (Supplemental Figure 10); and the hospital stay results also became insignificant (P = 0.59) in the RCTs subgroup (Supplemental Figure 11).
Sensitivity Analysis
For outcomes reporting heterogeneity above 50% a leave-one-out sensitivity analysis was performed to investigate the cause of heterogeneity. On removing the study by Yang et al. 26 the heterogeneity dropped from 71% to 45% in VAS back pain 1-3 months post-op endpoint (Supplemental Figure 12). Removing the same study 26 caused a reduction of heterogeneity to 0% in the VAS leg pain at 1-3 days, 1-3 months, and 12 months post-op outcomes (Supplemental Figures 13–15). Likewise, the removal of Yang et al. 26 reduced the heterogeneity to 0% in the outcome of ODI 1-week post-op (Supplemental Figure 16). Removal of the study by Guo et al. 25 reduced the heterogeneity from 74% to 45% in the ODI outcome at 1-3 months postoperatively (Supplemental Figure 17).
Publication Bias
The publication bias was assessed visually through funnel plots and statistically via Egger’s regression test. No visual asymmetry on the funnel plots was observed, which was further proved via Egger’s regression testing, except for the ODI score 1-3 months post-op (P = 0.04), operating time (P = 0.004), and estimated blood loss (P = 0.01) endpoints, which showed significant publication bias. The funnel plots and Egger’s regression testing details are provided in Supplemental Figures 18-43.
GRADE Assessment
GRADE Summary of Findings Table

UBED compared to MD for LDH.
Patient or population: LDH.
Intervention: UBED.
Comparison: MD.
Note. CI: confidence interval; MD: mean difference; RR: risk ratio
aHeterogeneity value is above 60%.
bHigh risk of bias is detected.
cThe 95% confidence interval crosses 0.
dThe 95% confidence interval crosses 1.
Discussion
This updated meta-analysis, comprising 1369 participants (659 UBED and 710 MD), provides a comparative evaluation of clinical and perioperative outcomes between UBED and MD techniques. UBED was associated with significantly reduced back pain in both the early postoperative period (1-3 days) and at 12 months. It also resulted in reduced estimated blood loss and shorter hospital stay, but required longer operative time. No significant differences were found in leg pain or overall patient satisfaction measured by the MacNab score.
Minimally invasive spinal surgery has progressed significantly due to improvements in surgical techniques and a growing demand for procedures with less tissue disruption. Techniques such as PELD, PTED, and PEID have been widely adopted since the 1980s, offering outcomes comparable to those of open surgery while minimizing incision size, blood loss, and recovery time.33,34 Though PELD is considered the least invasive, the newer UBED technique combines elements of both open and endoscopic methods, aiming to optimize surgical access and patient recovery.20,35
In our study, the lack of significant differences in VAS leg pain scores between UBED and MD across multiple postoperative time points highlights the comparable efficacy of these techniques in relieving leg pain associated with LDH. Feng et al. reported no significant difference in leg pain VAS scores between UBED and MD at various postoperative intervals, corroborating our findings. 36 This consistency across time reinforces the notion of comparable efficacy between the two techniques. 37 Leg pain in LDH primarily results from compression of the nerve root by herniated disc material. UBED and MD aim to decompress the affected nerve root, thereby relieving pain. The effectiveness of both techniques in achieving adequate decompression likely contributes to the similar improvements in leg pain observed postoperatively.38-40 Both MD and UBED effectively relieve radicular leg pain by decompressing the nerve root. MD uses a small, open, or microscopic approach and remains the traditional gold standard, while UBED uses dual portals with endoscopic visualization to reduce tissue trauma. When performed correctly, both methods offer comparable pain relief. 29 By preserving the integrity of the nerve root and surrounding tissues, UBED and MD facilitate recovery and reduce the likelihood of postoperative complications that could affect leg pain outcomes. 21
Our meta-analysis compared VAS scores for back pain after UBED and MD at specific postoperative times, showing that UBED was associated with a significant reduction in VAS back pain scores in the early (1-3 days) postoperative period and in the long-term (12 months) period. Feng et al. reported a significant reduction in VAS scores for back pain in the UBED arm during the early period only, while the two techniques showed comparable results in the long term. 36 Tong et al. 30 reported less opioid medication use in UBED patients early on, attributed to its less-invasive approach using small portals with endoscopic visualization, minimizing tissue damage, and reducing post-operative back pain compared to more invasive MD procedures. 20 Post-surgery, tissues undergo inflammation, then regeneration, which restores function. By the 1-3-month point, inflammation typically subsides, and soft tissues heal, leading to reduced pain regardless of the surgical technique used 41 ; also shown by the results of our meta-analysis, which found that the reduction in VAS back pain score was comparable at 1-3 months post-operatively.
Postoperative pain experiences are also greatly influenced by individual differences in pain perception and rehabilitation outcomes. Patients’ perceptions and reporting of pain can be influenced by a variety of factors, including social circumstances, psychological states, and genetic predispositions. The unique benefits of one surgical approach over another during the intermediate recovery phase may be overshadowed by these individual variances. Studies have shown that the degree of tissue damage is not the only element influencing how pain is felt; a complex interaction of biological, psychological, and social factors also plays a role.42,43 Furthermore, UBED’s muscle-sparing and less invasive technique is probably why patients who had it reported far less back pain 12 months after surgery than those who had MD. This long-lasting advantage is due to less disturbance of the paraspinal muscles and a decreased risk of epidural fibrosis, which is a primary cause of chronic postoperative back pain brought on by the creation of scar tissue around nerve roots. 44 However, on subgroup analysis according to the MD subtypes (standard and tubular), the long-term (12 months) postoperative VAS back score becomes comparable between the UBED and tubular MD, showing that both techniques offer similar long-term advantage, which may be due to the less invasive nature of tubular MD compared to that of the standard MD. However, this finding is supported by a limited number of studies, so a definitive conclusion cannot be made.
Thirdly, the ODI scores for patients undergoing MD and UBED showed no significant difference during the post-operative periods assessed (1 week, 1-3 months, and 12 months). These results align with those of Feng et al, who also found similar ODI scores between UBED and MD throughout most postoperative periods, except at 12 months, when the UBED group experienced a significant decrease in ODI scores. 36 This implies that both surgical methods yield similar initial gains in functional mobility and pain relief, most likely due to efficient decompression of neural structures in both procedures. Niu et al. (2022) reported that ODI scores were not significantly different between the two groups at the preoperative baseline, at 1 week postoperatively, and at 1-3 months postoperatively, confirming that early functional recovery is similar regardless of the surgical approach. 45 Also, patients who underwent UBED showed comparable improvement in the ODI score at 12 months after surgery compared with those who underwent conventional MD. This long-term functional advantage is attributed to the minimally invasive, muscle-sparing technique of UBED, which preserves paraspinal musculature and stabilizes spinal structures, thereby supporting improved biomechanical function over time. 46 Studies have shown that UBED results in less postoperative paraspinal muscle atrophy and fatty infiltration, as assessed by magnetic resonance imaging, leading to improved spinal stability and reduced chronic back pain. Furthermore, UBED has been associated with reduced epidural fibrosis and less iatrogenic damage to facet joints and ligaments, both of which are critical for maintaining spinal mobility and alignment.47,48 Altogether, these factors support improved long-term functional outcomes, including increased physical activity tolerance, more efficient rehabilitation, a faster return to work, and an overall higher standard of living. 37 However, compared to the tubular MD, UBED showed a comparable reduction in 12-month postoperative ODI scores, which might be due to the less invasive nature of the tubular MD compared to the standard or conventional MD.
Following the evaluation of pain and functional outcomes, it is also essential to consider key perioperative parameters that impact surgical efficiency and patient safety. In our study, UBED procedures often have longer operative times compared to conventional MD, a finding supported by the previous meta-analysis by Feng et al.. 36 This is primarily due to the steep learning curve required to master endoscopic techniques, which require proficiency in two-dimensional visualization and precise instrument handling.49,50 The study by Wu et al. also highlighted that with increased surgical experience, the operation time for UBED approaches that of MD. 51 Despite the initially longer learning curve associated with UBED, its benefits, including reduced tissue trauma, lower complication rates, and favorable clinical outcomes, make it a valuable surgical option in the long term.52,53 However, operative time was comparable between UBED and tubular MD, possibly due to the greater expertise required to perform a tubular MD.
UBED is also linked to reduced estimated blood loss compared to MD, primarily because of its minimally invasive approach. This finding is also supported by Feng et al. 36 Despite these findings, most studies agree that the observed blood loss in UBED is minimal, and if any blood loss occurs, it’s not clinically significant and rarely necessitates transfusion. Since UBED is a minimally invasive procedure, patients who have it generally experience shorter hospital stays than those who undergo conventional MD. This finding aligns with Feng et al's results. 36 This method facilitates earlier mobilization by causing less disruption to the paraspinal muscles and a decrease in postoperative discomfort. 54 Duong et al. reported that patients were discharged from the hospital on average after 4.7 days (range: 2-10 days) and were ambulatory by the second postoperative day. 55 Reduced tissue damage with UBED also results in fewer problems and decreased inflammatory reactions, which speeds up recovery. Together, these elements not only improve patient outcomes but also lower healthcare expenses and resource usage. 56 However, hospital stay was comparable between the UBED and tubular MD, which may be due to the tubular MD’s less invasive nature compared to the conventional MD.
Beyond objective clinical measures, evaluating patient-reported satisfaction offers essential insights into the overall effectiveness and acceptability of surgical treatments. The comparable patient satisfaction observed in the analysis between UBED and MD, as measured by the modified MacNab criteria, a finding also supported by the meta-analysis by Feng et al. 36 can be attributed to both procedures effectively alleviating symptoms of LDH. Despite differences in surgical techniques and invasiveness, both UBED and MD result in significant improvements in pain relief and functional recovery, leading to similar patient-reported outcomes.54,57 This suggests that the overall patient perception of surgical success is influenced more by symptom relief and functional restoration than by the specific surgical approach used. Therefore, while clinical and functional scores may vary, subjective outcome perceptions, as captured by the MacNab score, remain similar across different surgical techniques. 58
This meta-analysis highlights important clinical implications for the treatment of LDH. UBED’s minimally invasive, muscle-preserving technique offers benefits such as reduced postoperative back pain, less blood loss, and improved long-term function, making it a promising option for patients seeking lasting spinal stability and a faster recovery. The shorter hospital stays and quicker patient mobilization with UBED also indicate potential cost savings and better use of healthcare resources, benefiting both patients and medical facilities. Overall, these findings may support UBED as an alternative to MD, but further confirmation through high-quality, large-sample-size RCTs is necessary.
Limitations
This review and meta-analysis have several limitations. The limited number of comparative studies between UBED and MD, combined with the inclusion of mostly observational studies, reduces the strength of the evidence. Significant variability in study design, patient characteristics, and surgical skill, as well as high heterogeneity in the pooled outcomes and short follow-up periods, further limit the reliability of the results. Similarly, the limited number of studies in the tubular MD subgroup and RCTs subgroup reduced the overall power of the subgroup analyses. The learning curve for UBED, reliance on subjective measures such as pain scores, and imprecise estimates of blood loss may introduce bias. Additionally, the lack of blinding, as well as potential publication and selection biases, hinders a thorough assessment of safety and generalizability. Due to the limited data, calculations of minimal clinically important differences were not performed. Therefore, future studies should evaluate these to determine the clinical significance of the statistically significant results. Additionally, the health economics of the two surgical techniques, particularly regarding cost-effectiveness and operation time, could not be evaluated due to insufficient data. Future studies should address this aspect. More robust randomized controlled trials with larger samples are needed to confirm these findings.
Conclusion
UBED may offer decreased early and long-term back pain, reduced functional disability, decreased estimated blood loss, and shorter hospital stays compared to conventional MD, though it involves longer surgery times. Conversely, UBED’s effects on long-term back pain, functional disability, hospital stay length, and operative time are comparable to those of tubular MD. Large well-designed RCTs are needed to validate these findings.
Supplemental Material
Supplemental Material - Comparing Unilateral Biportal Endoscopic Discectomy Versus Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis
Supplemental Material for Comparing Unilateral Biportal Endoscopic Discectomy Versus Microdiscectomy for Lumbar Disc Herniation: A Systematic Review and Meta-Analysis by Muhammad Hassan Waseem, Zain ul Abideen, Muneeba Ahsan, Rimsha Adnan, Arusha Hasan, Zoya Aamir, Mahrosh Kasbati, Pawan Kumar Thada, Brandon Lucke-Wold in Global Spine Journal.
Footnotes
Author Contributions
Study concept and design: MHW and ZUA; acquisition of data: ZUA and MA; analysis and interpretation of data: RA, and AH; drafting of the manuscript: ZA, MK, PKT, and BLW; critical revision of the manuscript: MHW and BLW.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.