
Abstract
Study Design
Prospective multicenter cohort study.
Objectives
To determine the incidence and risk factors for postoperative complications following cervical spine surgery and to explore their association with long-term clinical outcomes.
Methods
A total of 1482 patients with degenerative cervical disorders who underwent surgery at 10 high-volume institutions in Japan were prospectively enrolled. Perioperative complications were defined as events occurring within 30 days postoperatively. Risk factors were analyzed using univariate and logistic regression analyses. Clinical outcomes were assessed using the cervical Japanese Orthopaedic Association (JOA) score and the Physical Component Summary (PCS) of the SF-36 at baseline and 2 years postoperatively.
Results
Perioperative complications occurred in 5.5% of patients: segmental motor paralysis (2.3%), neurological deficit (0.6%), dural tear (0.5%), CSF leakage (0.3%), epidural hematoma (0.9%), and surgical site infection (0.8%). Male sex (OR 3.049; 95% CI 1.045-8.929) and posterior fusion (OR 4.016; 95% CI, 1.518-10.620) were significant risk factors for segmental motor paralysis, while respiratory disease (OR 5.500; 95% CI, 1.462-20.694) was associated with surgical site infection. At 2 years, patients with complications showed variable neurological recovery, with many failing to reach the minimum clinically important difference.
Conclusions
Male sex, posterior fusion, and respiratory disease were identified as significant risk factors for major complications. Awareness of these factors may support improved surgical planning and perioperative management. However, interpretation of long-term outcomes should be made with caution because of the limited number of cases and potential selection bias associated with incomplete follow-up.
Keywords
Introduction
Cervical degenerative diseases are progressive conditions characterized by gradual compression of the spinal cord and/or nerve roots, leading to neurological deficits. As neurological function deteriorates, patients often experience increasing difficulty with activities of daily living and a decline in quality of life (QOL).1,2 To prevent further progression of symptoms, surgical intervention is frequently chosen and has generally yielded favorable outcomes.3-5
Nevertheless, it should be acknowledged that, despite the overall efficacy of surgery, a proportion of patients experience postoperative complications. For example, segmental motor paralysis, as exemplified by C5 palsy, commonly develops in the early postoperative period and significantly contributes to reduced QOL due to its prolonged recovery.6,7 Surgical site infections can also significantly prolong hospitalization and impose both physical and financial burdens on patients.8-10 Dural tears and cerebrospinal fluid (CSF) leakage are associated with increased rates of infection and postoperative paralysis, as well as prolonged hospitalization and delayed pain relief.11,12 In addition, severe complications such as postoperative neurological deficits and epidural hematomas have been widely reported.13-15 Nevertheless, these complications are relatively rare, and the risk factors associated with their occurrence remain poorly understood.
To clarify the surgical outcomes of cervical spine disorders, we prospectively enrolled a total of 1482 patients. The large sample size provides a valuable opportunity not only to evaluate overall surgical outcomes but also to conduct a robust analysis of postoperative complications. The aim of this study was to elucidate the incidence and risk factors of complications following surgery for cervical spine disorders and to assess their impact on subsequent clinical outcomes.
Materials and Methods
Patients
This multi-institutional investigation of cervical spine surgeries was performed by 10 high-volume institutions in Japan. A total of 1482 patients with degenerative cervical disorders, including atlantoaxial instability, cervical spondylotic radiculopathy, ossification of the posterior longitudinal ligament (OPLL), cervical spondylotic amyotrophy, cervical spondylotic myelopathy, and cervical disc herniation, were prospectively enrolled between February 4, 2019, and December 27, 2022. Patients were included only if the degenerative cervical disorder was symptomatic and deemed clinically relevant for surgical intervention. Symptomatic cervical disc herniation, cervical radiculopathy, cervical spondylotic myelopathy, and atlantoaxial instability were diagnosed based on the presence of corresponding neurological symptoms together with imaging findings consistent with nerve root and/or spinal cord compression. The exclusion criteria were as follows: tumor, trauma, ankylosing spondylitis, and dialysis-associated spondyloarthropathy. The study was approved by the Ethics and Institutional Review Board of the lead institution (approval number: 20180045; date of approval: June 14, 2018), and all participants provided informed consent before undergoing surgery.
Data Collection
Demographic information, medical history, imaging findings, and surgical summary were collected through chart review. As for comorbidities, the category of “respiratory diseases” was pre-specified in the study protocol. During chart review, relevant conditions—including asthma, chronic obstructive pulmonary disease, interstitial lung disease, obstructive sleep apnea, and infectious lung diseases—were assigned to this predefined category.
All surgery-related events that occurred within 30 days of the operation were defined as perioperative complications and were verified by personnel independent of the operating surgeon. Cervical segmental motor paralysis was defined as new-onset motor weakness of at least 1 grade on the manual muscle testing (MMT) scale in any upper extremity muscle following surgery. To avoid misclassification, cases involving surgery at or above the C3 level and those treated with artificial disc replacement were pre-specified for exclusion, as these procedures are not expected to affect the anatomical or procedural factors relevant to segmental motor paralysis. Neurological deficit was defined as any new postoperative symptom, excluding segmental motor paralysis, epidural hematoma, CSF leakage, and surgical site infection, and included myelopathic signs, sensory disturbance, and bladder or bowel dysfunction. Clinical outcomes were assessed in patients who had data available at both preoperative and 2-year postoperative time points, using the cervical Japanese Orthopaedic Association (JOA) scores 16 and the Physical Component Summary (PCS) of the 36-Item Short Form Health Survey (SF-36). 17 The minimum clinically important difference (MCID) was defined as 2.5 points for the JOA score, 18 and as 4.0 points for SF-36 PCS.19,20 Radiological assessments were conducted using plain radiography. The C2–C7 Cobb angle was measured in the neutral position of the cervical spine. 21
Statistical Analyses
Continuous variables are presented as means ± standard deviations, and the categorical variables as percentages. Baseline demographics, surgical variables, and imaging characteristics were compared between patients with and without complications using unpaired t-tests for continuous variables and chi-square tests for categorical variables. Binary logistic regression analysis was performed to identify predictors of perioperative complications, with variables showing P-values <0.05 in univariate analyses included as independent variables in the model. Differences between the 2 time points for JOA scores and PCS were analyzed using paired t-tests.
A P-value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 30.0 (SPSS Inc., Chicago, IL).
Results
Incidence of Perioperative Complications
Surgical Information of 1482 Patients
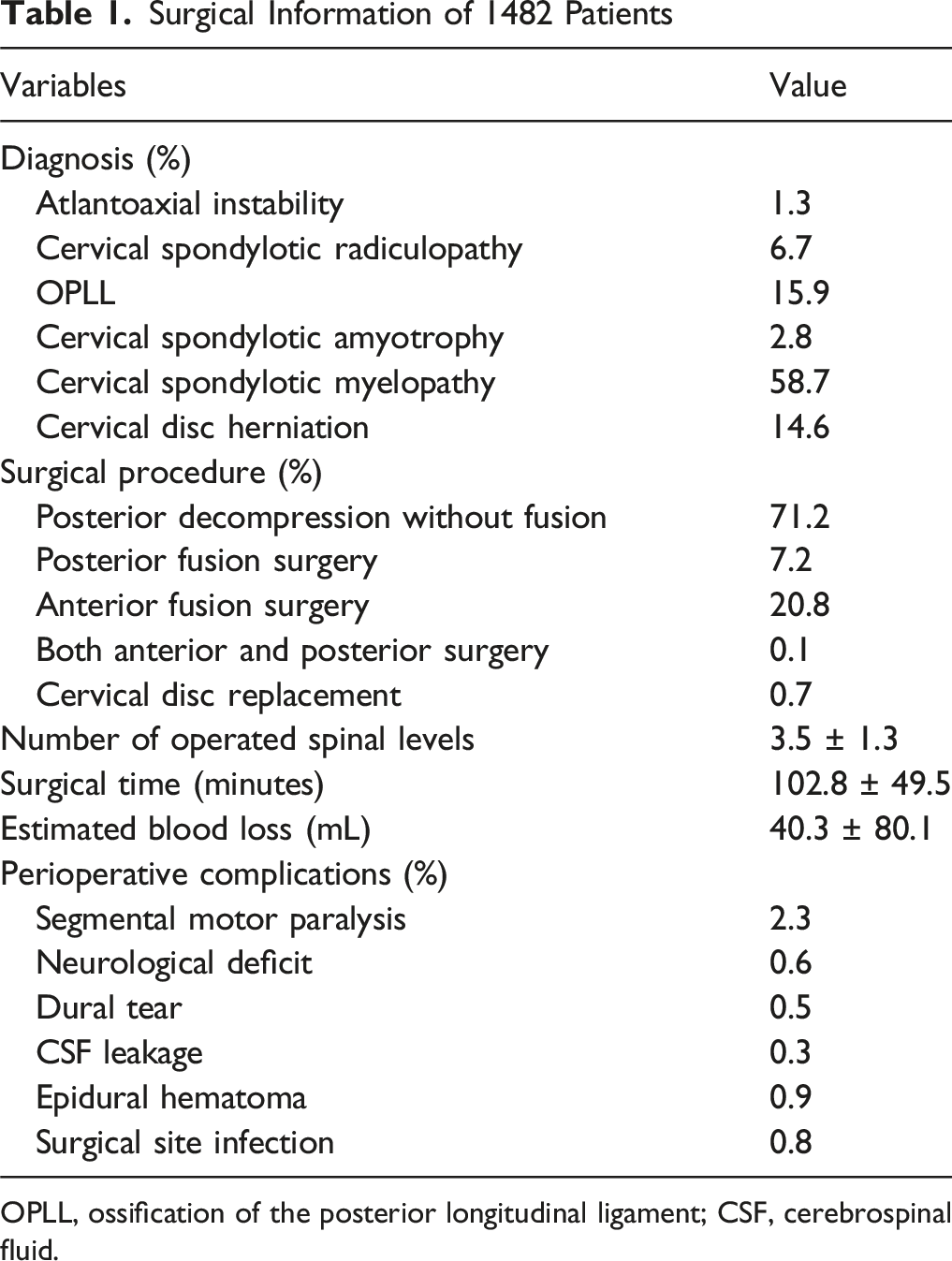
OPLL, ossification of the posterior longitudinal ligament; CSF, cerebrospinal fluid.
Perioperative complications occurred in 5.5% of the cohort (n = 82), with cervical segmental motor paralysis in 2.3% (n = 34), neurological deficits in 0.6% (n = 9), dural tear in 0.5% (n = 8), CSF leakage in 0.3% (n = 5), epidural hematoma in 0.9% (n = 14), and surgical site infection in 0.8% (n = 12).
Clinical Characteristic and Course of Each Complication
Among the 34 patients who developed segmental motor paralysis, the majority of cases involved the C5 segment (n = 31), while only 1 case each involved the C6, C7, and C8 segments. Three underwent reoperation for foraminal decompression, whereas the remaining 31 received only conservative management with rehabilitation. During hospitalization, improvement was observed in 20 patients, while 14 showed no change.
Of the 9 patients who developed neurological deficits, 7 presented with myelopathic signs, and 2 exhibited unilateral sensory disturbance. Symptoms were present immediately after surgery in 6 cases, including 4 with myelopathic signs and 2 with sensory disturbance. In 5 of these, the cause remained unidentified, and in the remaining case, malposition of a screw was identified, necessitating reoperation. In contrast, 3 patients developed neurological deficits after a delay. In 1 patient, symptoms appeared on postoperative day 2 without an identifiable cause and were managed conservatively. The other 2 developed symptoms on postoperative day 6: in 1 case, postoperative disc herniation was observed and managed conservatively; in the other, changes in spinal alignment were identified, and reoperation was performed. All patients experienced improvement during hospitalization.
All 8 cases of dural tear underwent intraoperative repair, such as dural suturing or duraplasty, and none experienced postoperative neurological deterioration.
Of the 5 cases of CSF leakage, 3 were managed conservatively, 1 underwent spinal drainage, and 1 underwent reoperation with duraplasty. Symptoms resolved in all cases.
All patients who developed postoperative epidural hematoma underwent reoperation for hematoma evacuation. Symptoms improved in 12 of 14 patients, while 2 remained unchanged.
Regarding postoperative surgical site infections, 9 patients underwent reoperation with debridement and irrigation, while 3 received only conservative treatment with medication. All patients showed improvement.
Factors Associated with Cervical Segmental Motor Paralysis
Prior to the risk factor analysis, cases deemed unlikely to be associated with segmental motor paralysis were excluded, including those who underwent artificial disc replacement (n = 11) and those in whom the surgical level did not involve C4 or more caudal segments (n = 42). As a result, 1429 patients were included in the analysis.
Clinical Characteristics of Patients Who Developed Cervical Segmental Motor Paralysis Among the 1429 Patients
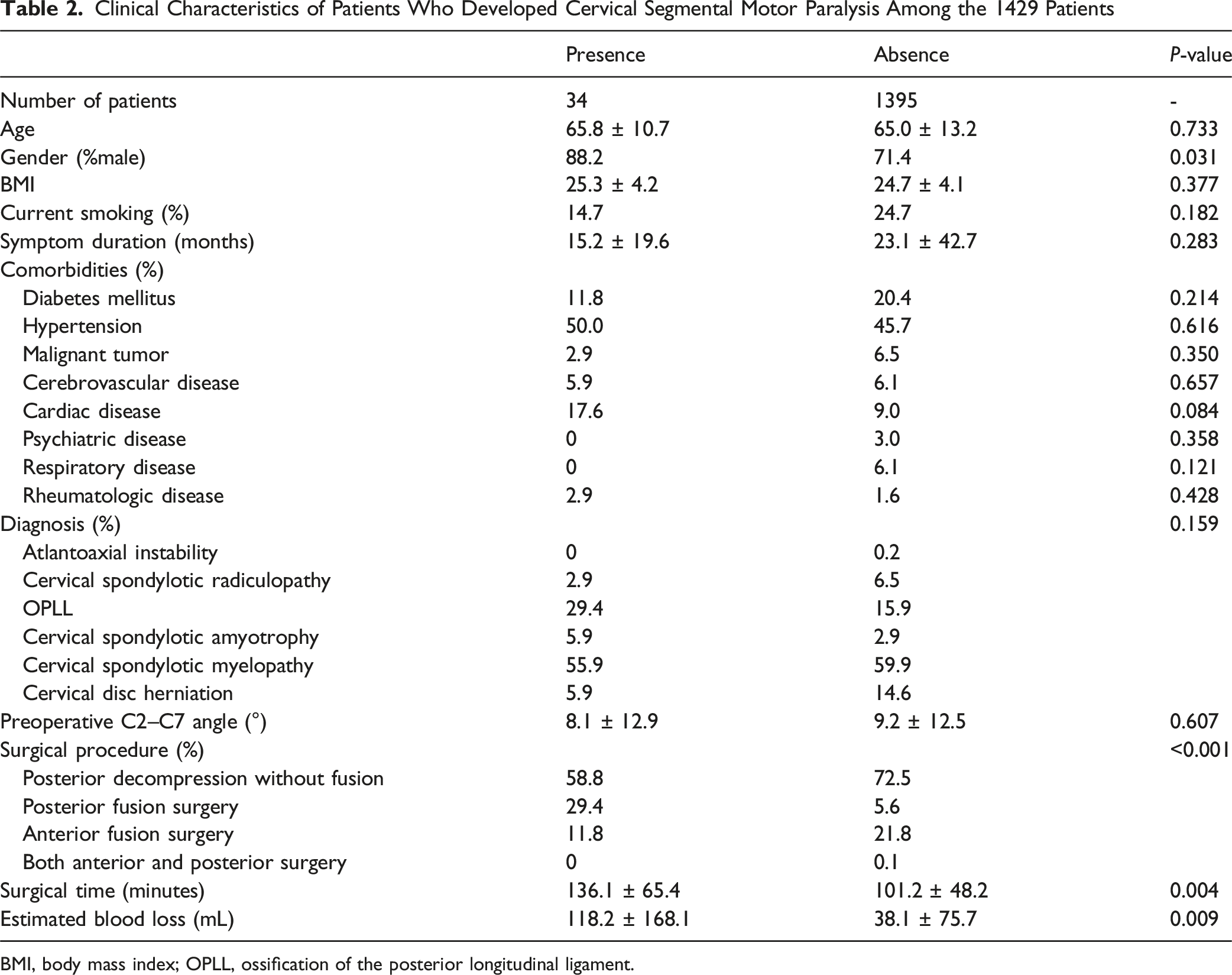
BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament.
Analysis of Factors Associated with Other Complications
Clinical Characteristics of Patients Who Developed Each Complication Among the 1482 Patients
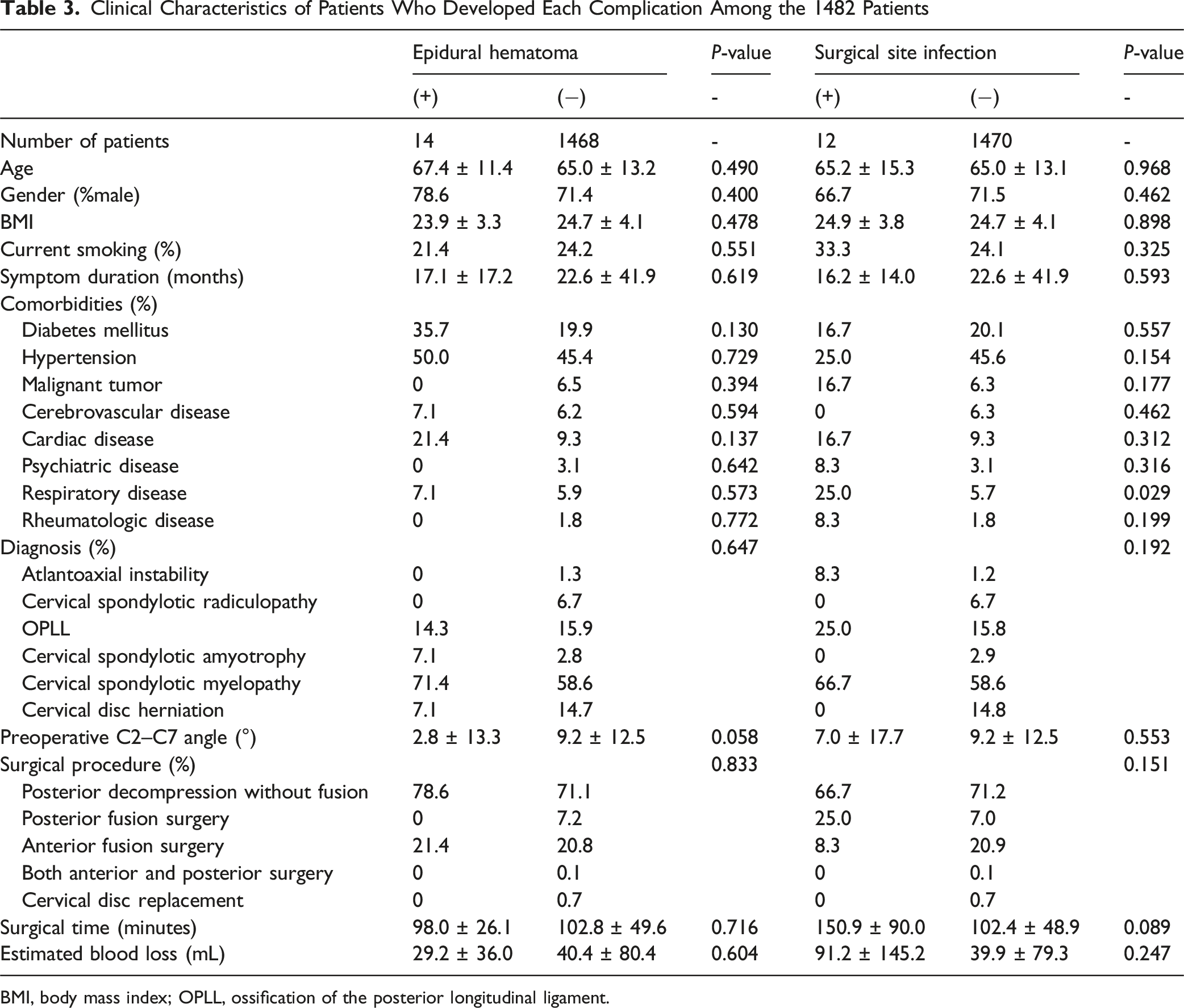
BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament.
In patients who developed epidural hematomas, the preoperative C2–C7 angle tended to be smaller than in those without hematomas (2.8 ± 13.3° vs 9.2 ± 12.5°), although there was no significant difference (P = 0.058). For the remaining variables, no significant differences were observed between the groups.
As for surgical site infections, respiratory disease was significantly more prevalent in the infection group (25.0% vs 5.7%, P = 0.029). Regarding the breakdown of respiratory diseases, the infectious group included asthma (n = 2) and infectious lung disease (tuberculosis; n = 1), while the non-infectious group comprised asthma (n = 44), chronic obstructive pulmonary disease (n = 13), interstitial lung disease (n = 4), obstructive sleep apnea (n = 12), and infectious lung disease (n = 11). Other variables showed no significant differences.
Risk Factors Identified by Logistic Regression
Risk Factors for Each Complication Identified by Binary Logistic Regression Analysis
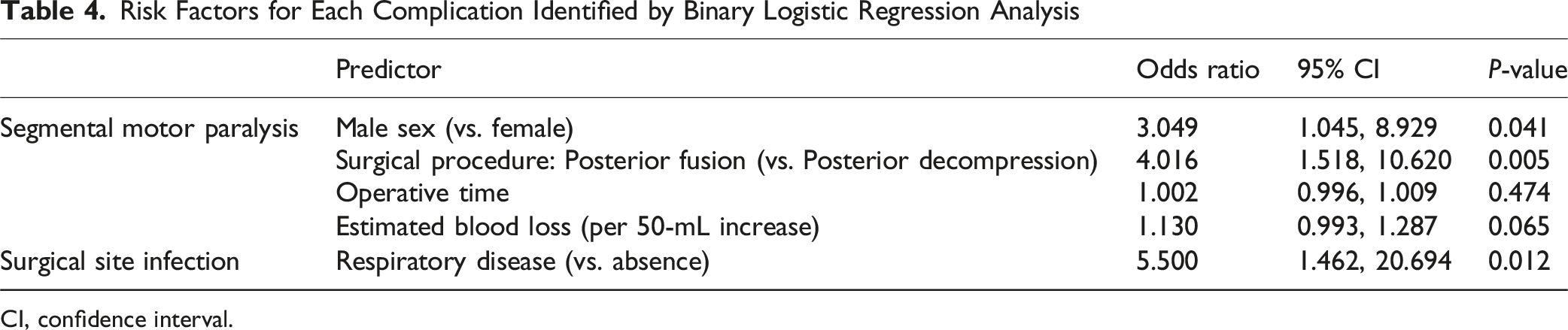
CI, confidence interval.
For segmental motor paralysis, gender, surgical procedure, operative time, and estimated blood loss met the pre-specified threshold for inclusion (P < 0.05) and were entered into the logistic regression model. In the final analysis, male sex (odds ratio [OR], 3.049; 95% confidence interval [CI], 1.045-8.929; P = 0.041) and posterior fusion surgery (OR, 4.016; 95% CI, 1.518-10.620; P = 0.005) were significantly associated with the development of segmental motor paralysis.
For surgical site infection, the presence of respiratory disease was the only variable that met the pre-specified threshold for inclusion in the logistic regression model based on the univariate analysis. Consequently, respiratory disease was entered as the sole predictor in the model, and the final analysis demonstrated that its presence significantly increased the risk of surgical site infection (OR, 5.500; 95% CI, 1.462-20.694; P = 0.012).
Subgroup Analysis of Risk Factors for Complications in Each Surgical Procedure
The incidence of perioperative complications was summarized for each surgical approach. Among the 1055 patients who underwent posterior decompression without fusion, 20 developed segmental motor paralysis, 7 had neurological deficits, 6 experienced dural tears, 3 had CSF leakage, 11 developed epidural hematomas, and 8 had surgical site infections. In the posterior decompression with fusion group (n = 106), segmental motor paralysis occurred in 10 patients, while dural tear, CSF leakage, and surgical site infection were observed in 1, 1, and 3 patients, respectively. In the anterior decompression with fusion group (n = 308), segmental motor paralysis occurred in 4 patients, neurological deficit in 2, dural tear, CSF leakage, and surgical site infection in 1 each, and epidural hematoma in 3 patients.
To identify risk factors for complications within each surgical procedure, only complications with a frequency of ≥10 were analyzed: segmental motor paralysis (n = 20) and epidural hematoma (n = 11) in the posterior decompression without fusion group, and segmental motor paralysis (n = 10) in the posterior decompression with fusion group. Within each surgical approach, patients with and without each complication were compared, and variables with P < 0.05 in univariate analysis were entered into a binary logistic regression model.
Clinical Characteristics of Patients With Postoperative Cervical Segmental Motor Paralysis After Posterior Decompression Without Fusion (n = 1,031
a
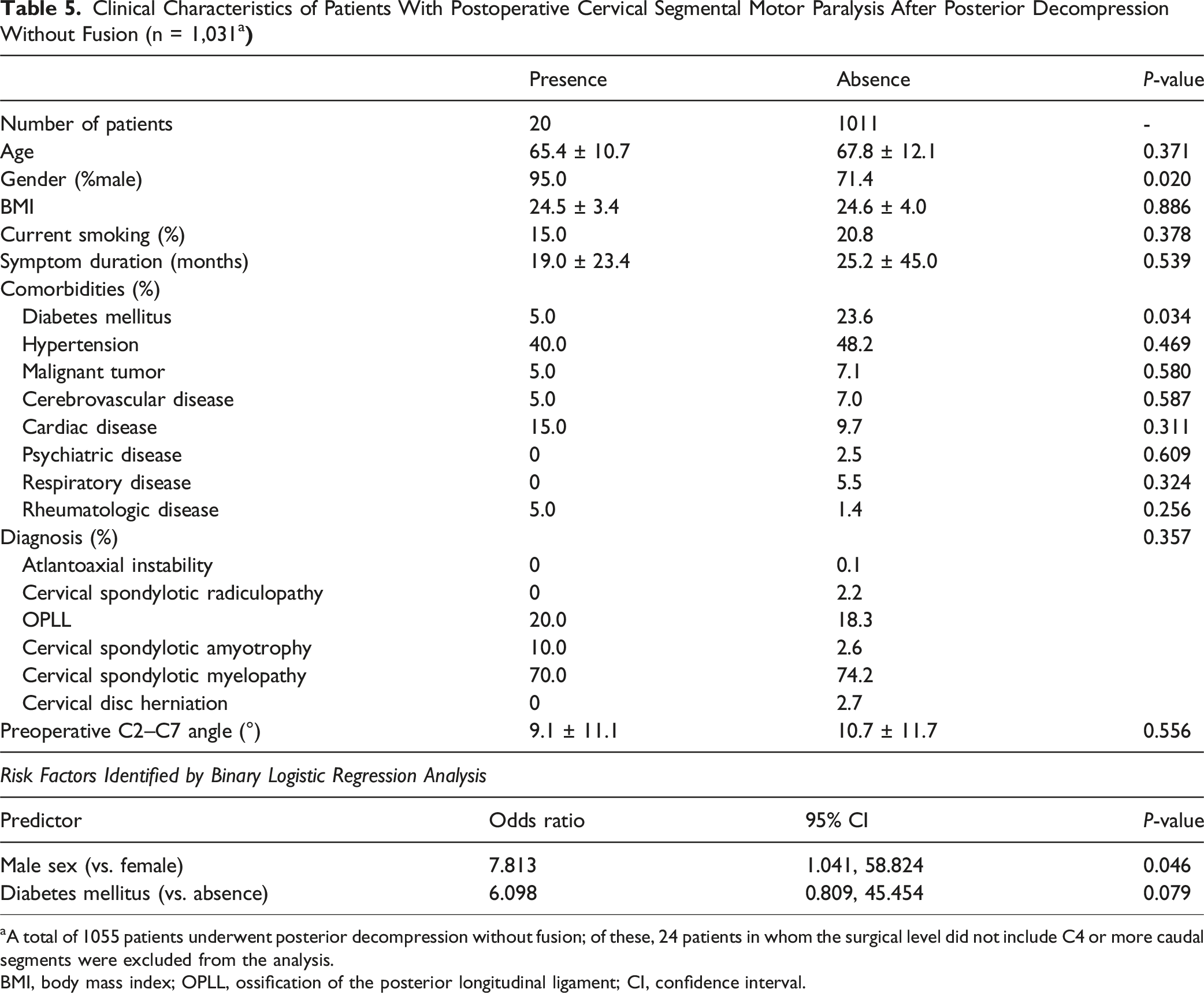
aA total of 1055 patients underwent posterior decompression without fusion; of these, 24 patients in whom the surgical level did not include C4 or more caudal segments were excluded from the analysis.
BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament; CI, confidence interval.
Clinical Characteristics of Patients With Postoperative Epidural Hematoma After Posterior Decompression Without Fusion (n = 1055)
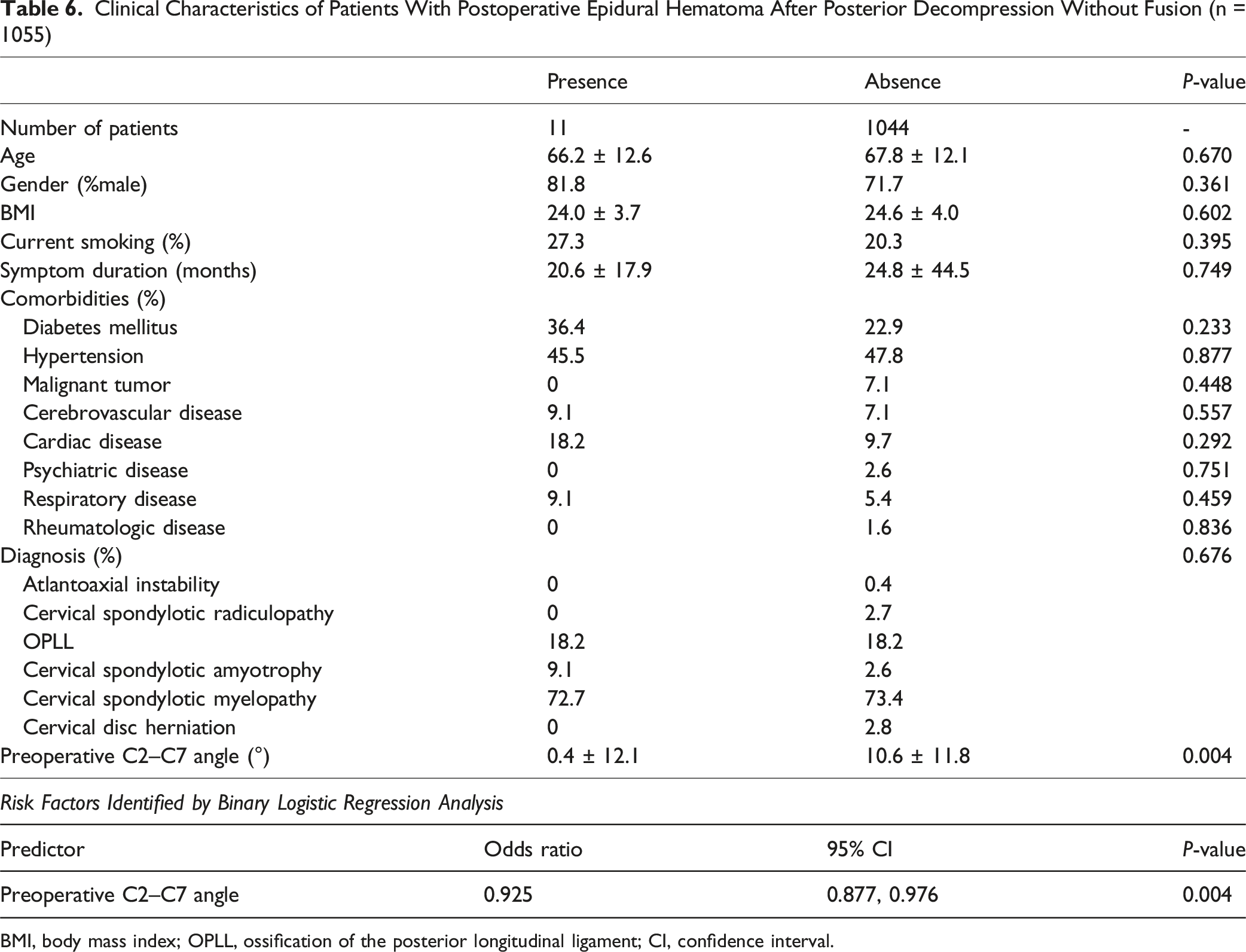
BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament; CI, confidence interval.
Clinical Characteristics of Patients With Postoperative Cervical Segmental Motor Paralysis After Posterior Decompression With Fusion (n = 88
a
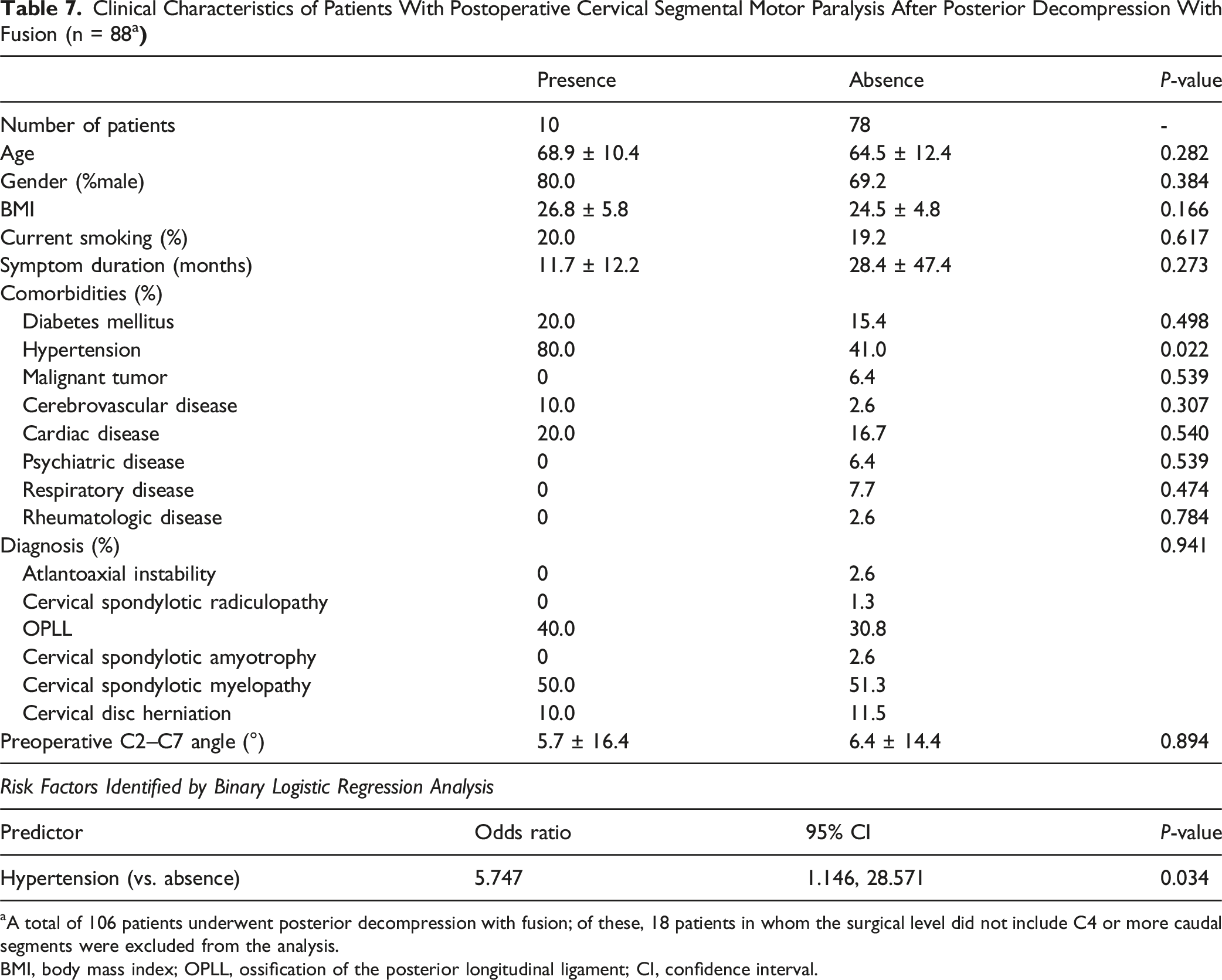
aA total of 106 patients underwent posterior decompression with fusion; of these, 18 patients in whom the surgical level did not include C4 or more caudal segments were excluded from the analysis.
BMI, body mass index; OPLL, ossification of the posterior longitudinal ligament; CI, confidence interval.
Clinical Outcomes Following the Occurrence of Complications
Clinical Outcomes Following the Occurrence of Complications
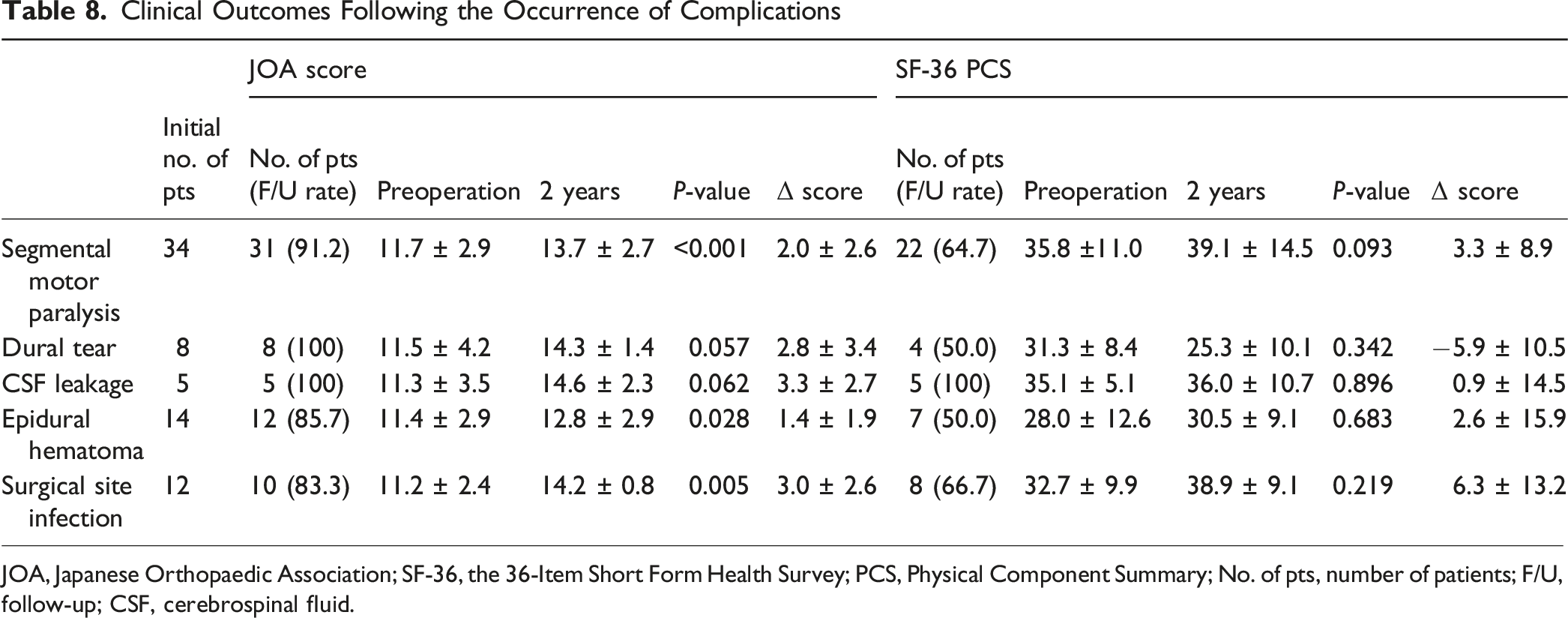
JOA, Japanese Orthopaedic Association; SF-36, the 36-Item Short Form Health Survey; PCS, Physical Component Summary; No. of pts, number of patients; F/U, follow-up; CSF, cerebrospinal fluid.
Significant neurological improvement was observed in patients with segmental motor paralysis and surgical site infection, while those with epidural hematoma showed modest but statistically significant recovery. In contrast, patients with dural tear or CSF leakage demonstrated only nonsignificant trends toward improvement. Changes in the SF-36 physical component summary PCS were not statistically significant in any group.
Assessment of whether each outcome reached the MCID revealed that, for the JOA score, dural tear, CSF leakage, and surgical site infection achieved improvements greater than the threshold of 2.5 points. Regarding the SF-36 PCS, only the surgical site infection group reached the MCID threshold of 4.0 points.
Discussion
This study is a large-scale, multicenter investigation that comprehensively evaluated postoperative complications following cervical spine surgery. To our knowledge, few prospective studies of this scale have examined rare postoperative complications in this context. Although the number of patients who developed complications was limited even in our study, the findings highlight the importance of heightened awareness regarding their management and prevention.
Our findings identified male sex as a significant risk factor for cervical segmental motor paralysis, a result that remained consistent both in the overall cohort and when the analysis was limited to patients who underwent posterior decompression without fusion. The association between sex and the incidence of this complication has been reported in previous studies, most of which consistently showed a higher incidence in males.22-24 Although the underlying mechanisms remain uncertain, 1 possible explanation may involve differences in cervical alignment between males and females. Males generally exhibit a greater degree of cervical lordosis compared to females, 25 which could contribute to a more pronounced posterior shift of the spinal cord following posterior decompression. This posterior migration has been hypothesized in previous studies to increase nerve root tension and thereby elevate the risk of segmental motor paralysis in males,26,27 although this relationship was not directly evaluated in the present study. Another possible explanation may relate to the higher prevalence of OPLL in males.28,29 In cases of OPLL, where the ossified lesions often extend across multiple levels, surgeons may be inclined to perform wider decompression to prevent postoperative neurological deterioration. 30 As a result, the posterior shift of the spinal cord may increase, potentially leading to traction or impingement of the C5 nerve root. In our cohort, although the diagnosis distribution did not differ significantly between groups, the incidence of OPLL was nearly twice as high in patients who developed segmental motor paralysis (Table 2). Indeed, previous studies have reported a higher incidence of C5 palsy in patients with cervical OPLL.22,31-33 Collectively, these observations may suggest that anatomical and pathological factors specific to male patients could increase the susceptibility to this complication, warranting careful attention during surgical planning.
The increased incidence of segmental motor paralysis following posterior fusion procedure, another identified risk factor, has also been described in previous studies.23,34,35 It has been proposed that realignment procedures during posterior fixation might inadvertently exacerbate foraminal stenosis, leading to nerve root compression and subsequent paralysis. Miller et al. evaluated treatment outcomes in patients who developed segmental motor paralysis using patient-reported outcome measures, and reported that, 1 year after surgery, these patients experienced significant difficulties with personal care and activities of daily living, leading to an increased need for rehabilitation and a corresponding rise in medical expenditures. 6 Based on these findings, when posterior fixation is performed, excessive correction should be carefully avoided, and prophylactic foraminotomy may be considered in cases with preoperative evidence of narrowed intervertebral foramina. 36 Interestingly, in the present study, when the analysis was limited to patients who underwent posterior fusion surgery, the incidence of motor paralysis was significantly higher among those with hypertension. A previous study reported that the prevalence of hypertension was significantly higher among patients who developed C5 palsy in univariate analysis, although this association was not retained in multivariate analysis. 37 Given that ischemia-reperfusion injury occurring after decompression has been proposed as a potential mechanism underlying this complication, 38 it is conceivable that patients with hypertension may be more vulnerable to microcirculatory disturbances associated with such reperfusion. Taken together, when determining the surgical strategy for posterior fusion, the potential risk of this complication should be carefully considered to facilitate individualized decision-making.
In the present study, preexisting respiratory disease was identified as an independent risk factor for postoperative surgical site infection. Among these conditions, 2 patients with concomitant asthma developed infections. To our knowledge, no studies have examined the association between asthma and postoperative infections after cervical spine surgery, although evidence from other surgical fields supports this potential relationship. Yamaguchi et al. reported, in a cohort of patients undergoing gastrectomy for gastric cancer, that those with asthma had a significantly higher incidence of surgical site infection compared with non-asthmatic patients, with the risk being further elevated in individuals with marked obstructive impairment. 39 Similarly, Lupo et al. demonstrated that chronic obstructive pulmonary disease was an independent risk factor for infection following spine surgery. 40 Although the underlying mechanisms remain to be fully elucidated, impaired oxygenation and host immune dysfunction associated with compromised pulmonary function have been suggested to delay wound healing and increase susceptibility to infection.41-43 Furthermore, in our study, 1 case of surgical site infection occurred in a patient with tuberculosis. Ke et al. analyzed a nationwide database of patients undergoing non-chest surgeries, including musculoskeletal procedures, and suggested that both active and previously treated tuberculosis were independently associated with a significantly increased risk of postoperative deep infections. 44 Despite the limited number of surgical site infection cases in our cohort and the inability to assess pulmonary function severity, it is important to recognize the potential risk of postoperative infections in patients with respiratory diseases and associated functional impairment.
The reported incidence of postoperative epidural hematoma following cervical spine surgery varies across studies, ranging from 0.09% to 0.24%.15,45 In the present study, although the incidence was relatively higher at 0.9%, it still represents a rare complication. Previous literature has indicated that delayed diagnosis or treatment of this condition can result in permanent neurological impairment, highlighting the importance of early recognition and prompt intervention.45,46 Several studies have suggested that preoperative spinal alignment abnormalities, such as thoracic kyphosis and lumbar hypolordosis, may be associated with an increased risk of postoperative hematoma.47,48 In the present study, although the trend did not reach statistical significance in the overall cohort in the univariate analysis (Table 3; P = 0.058), preoperative cervical hypolordosis was identified as a significant risk factor when the analysis was limited to patients who underwent posterior decompression without fusion (Table 6; P = 0.004). While further studies with a larger sample size are warranted, these findings suggest that preoperative spinal alignment should be carefully considered when developing strategies to minimize the risk of this complication.
When interpreting postoperative clinical outcomes, it is important to distinguish between statistical significance (P < 0.05) and clinical importance (exceeding the MCID threshold). Although several complication groups demonstrated mean improvements exceeding the MCID for the JOA score (2.5 points) or SF-36 PCS (4.0 points), these changes did not always reach statistical significance, likely due to the small sample size and variability. Conversely, some statistically significant improvements did not meet the MCID threshold, indicating that while they may be mathematically significant, their clinical relevance is limited. Specifically, patients with segmental motor paralysis demonstrated a statistically significant improvement in JOA scores; however, the mean change did not reach the MCID threshold. In contrast, patients with dural tears exceeded the MCID despite the absence of statistical significance, likely due to the small sample size and greater variability in this group. Only the surgical site infection group achieved both statistical significance and an improvement exceeding the MCID for the JOA score. Nevertheless, these findings should be interpreted with caution because the analysis included only patients with complete data at both preoperative and postoperative time points. The exclusion of patients lost to follow-up or with missing data may have introduced selection bias. Specifically, while more than 80% of patients completed follow-up for the JOA score, the 2-year follow-up rate for the SF-36 was notably lower. This discrepancy likely reflects the inherent challenges of collecting patient-reported outcome measures in the postoperative period and may also indicate the difficulty of obtaining such data when the patient–physician relationship becomes strained after postoperative complications.
This study has several limitations. First, the overall number of complication cases was small, and risk factor analysis was not feasible for complications with fewer than 10 cases. Even among complications with 10 or more cases, variables with P-values close to but not reaching 0.05 may have been affected by insufficient statistical power. Second, beyond sample size considerations, the logistic regression models used univariate screening with a threshold of P < 0.05 for variable selection. Although this approach is commonly applied in clinical research, it has methodological limitations that should be acknowledged. Third, this study was conducted within the framework of Japan’s single national health insurance system and included a large proportion of patients with OPLL, which is more prevalent among East Asian populations. These epidemiological and healthcare system characteristics may have influenced both surgical strategies and the incidence of complications. Therefore, the generalizability of our findings to other regions or ethnic groups remains uncertain. Finally, surgical indications and postoperative management were determined at the discretion of each participating institution, without a standardized protocol. Such variability may have influenced the incidence of complications and subsequent clinical outcomes. Despite these limitations, this study provides valuable evidence through a large-scale, prospective evaluation of perioperative and postoperative outcomes in patients undergoing cervical spine surgery. Recognizing the risk factors for complications is essential for refining treatment strategies and ensuring thorough preoperative counseling regarding prognosis.
In conclusion, this study investigated postoperative complications following cervical spine surgery. In particular, for segmental motor paralysis, attention should be paid to patient sex and surgical procedure, while for surgical site infections, the presence of concomitant respiratory disease warrants careful consideration.
Footnotes
Acknowledgments
We would like to express our deepest gratitude to all the institutions that have cooperated with us. In preparing this manuscript, ChatGPT (OpenAI) and Grammarly (Grammarly Inc.) were used for grammar refinement and typographical error correction. These tools were employed exclusively to improve clarity and readability without modifying the scientific content or interpretation of the findings.
Consent to Participate
We confirmed that all methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all subjects.
Author Contributions
NN contributed to data provision, analysis, and manuscript writing. JY, MM, MN, and KW supervised the study. NN and TO managed the data. YH, YKa, NI, HK, YKo, RS, TI, KT, MO, and SS contributed to data provision and guidance on the manuscript content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and the use of all data in this study was approved by the ethics committee of the institution of the current study.