
Abstract
Study Design
Systematic Review and Meta-Analysis.
Objectives
Despite a surge in the use of Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) in spine surgery candidates, evidence on their perioperative use remains unclear. This meta-analysis aimed to synthesize the evidence on the safety and efficacy of GLP-1 RA use in patients undergoing spine surgeries.
Methods
A systematic search of PubMed (MEDLINE), Embase, Scopus, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials (CENTRAL) was conducted. Studies that compared spine surgery outcomes in GLP-1 RA users and non-users were included. Two reviewers independently selected articles. (PROSPERO: CRD420251061447).
Results
Eleven retrospective studies reporting on 27,143 patients were included. Three studies focused on the cervical spine, 6 on the lumbar spine, and 2 included all spinal fusions. Risk of bias was deemed to be low in all studies. There were no significant differences in the GLP-1 RA users and non-users in pooled estimates for pseudoarthrosis (odds ratio: 1.29 [95% CI: 0.09 - 19.23]), surgical site infections (0.97 [0.74 - 1.27]), pneumonia (1.19 [0.30 - 4.68]), deep vein thrombosis (1.34 [0.86 - 2.08]), acute kidney injury (1.27 [0.93 - 1.74]), readmission rate (1.06 [0.94 - 1.18]), and emergency department visits (0.95 [0.10 - 8.99]).
Conclusions
Currently available level 4 evidence suggests that perioperative GLP-1 RA use in spine surgery candidates does not affect the risk of postoperative complications. However, these studies are based on administrative databases and may be confounded by indication. Future studies should include glycemic control and weight loss to better elucidate the impact of GLP-1 RA.
Keywords
Introduction
Over a million spine surgeries are performed in the US annually, with a further increase projected as the population ages. 1 Although generally a safe and effective surgery, complications still occur in approximately 16% of patients. 2 These complications pose a significant burden on patients and the healthcare system. Therefore, reducing them remains a key focus of research. Among the modifiable risk factors identified, diabetes and obesity are prominently associated with adverse events after spine surgery. 3 These include a higher incidence of pseudoarthrosis, medical complications, and worse patient-reported outcomes. 4 Moreover, these are prevalent comorbidities in spine surgery candidates, with almost 60% having obesity and 16% having diabetes. 5
Glucagon-like peptide-1 receptor agonists (GLP-1 RA) are approved by the U.S. Food and Drug Administration (FDA) for both diabetic control and weight loss. 6 Over the past decade, there has been a significant surge in the use of GLP-1 RA in the U.S. 7 and hence an increase in spine surgery candidates using GLP-1 RA. However, the safety of perioperative use of GLP-1 RA in spine surgery has not been well-established. Some animal studies have linked GLP-1 RA use to boost bone health. 8 GLP-1 RA is also demonstrated to improve glycemic control, blood pressure, lipid profiles, cardiovascular risk, and renal function.9,10 These effects should theoretically lead to improved outcomes after spine surgery. Additionally, these drugs have been reported to promote bone metabolism akin to anti-osteoporotic medicines. 11 However, GLP-1 RA are also associated with significant gastrointestinal adverse events, rapid weight loss, and decreased gastric emptying. 9 When present in the immediate preoperative period, these adverse effects may increase the risk of complications. 12 Therefore, due to these potentially paradoxical effects of GLP-1 RA, evidence is required to establish their perioperative safety.
Recently, some studies have evaluated the perioperative use of GLP-1 RA in specific spine surgeries. They often report mixed results, and hence, the overall evidence on perioperative GLP-1 RA use remains unclear. 13 To the best of our knowledge, there is no meta-analysis with pooled estimates of the effectiveness and safety of GLP-1 RA in spine surgery. Therefore, this meta-analysis aims to synthesize the evidence on the safety and efficacy of GLP-1 RA use in patients undergoing spine surgeries.
Methods
Study Design and Protocol Registration
This systematic review is conducted and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 14 The PRISMA checklist is available in Supplemental Section 1. The protocol was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) (registration ID: CRD420251061447).
Eligibility Criteria
The population of interest was defined as follows: Population: adult patients (≥18 years) undergoing spinal surgery Exposure: GLP-1 RA user Comparison: GLP-1 RA non-user Outcomes: Postoperative surgical and medical outcomes
All retrospective and prospective observational studies, as well as randomized controlled trials, were eligible for inclusion. Case reports, review articles, editorials, opinion pieces, and articles in languages other than English were excluded.
Data Sources and Search Strategy
The systematic literature search was performed on PubMed (MEDLINE), Embase, Scopus, ClinicalTrials.gov, and the Cochrane Central Register of Controlled Trials (CENTRAL). The search included all studies published from the earliest date available in each of the mentioned databases up to and including June 9, 2025. The search strategy included MeSH and free-text terms related to spine surgery and GLP-1 RA. The full search strategy is included in Supplemental Section 2.
Study Selection Process
Citations identified in the literature search were imported into Covidence, and automatic de-duplication of records was performed. Next, title and abstract screening were conducted independently by 2 reviewers (AD and SI), followed by full text screening done by the same reviewers independently. Any disagreements were resolved through discussion and consensus, or in consultation with a third reviewer (MTI). Reasons for exclusion were noted for articles excluded after full-text review.
Data Extraction
Data was independently extracted by 2 reviewers using a standardized Excel Sheet (Microsoft Corporation, Redmond, WA). Variables extracted included study characteristics such as year, country, study design, sample size, and patient demographics. Outcomes included both surgical and medical outcomes, such as readmission rates, medical and surgical complications (eg, surgical site infections, pseudoarthrosis), emergency department visits, and reoperation rates.
Risk of Bias
The risk of bias in individual studies was initially assessed by a single reviewer (AD) using the Newcastle Ottawa Scale (NOS) for observational studies, 15 which was then confirmed by a second reviewer (SI). Discrepancies in assessments were resolved by consensus.
Data Synthesis and Statistical Analysis
Where appropriate, a meta-analysis was performed using RevMan software (version 7.2.0). Since most of the studies included were conducted using administrative databases, it was impossible to determine the extent of overlap in the underlying patient populations. We followed the method suggested by Lock et al to treat administrative dataset-based studies in meta-analysis. 16 If 2 studies had overlapping eligibility criteria applied to the same database, they would be considered duplicates and only 1 would be included in the meta-analysis. In this case, studies with larger sample sizes were included. Conversely, if either the eligibility criteria or the database differed, both would be included.
For the meta-analysis, a random-effects model was used to calculate the pooled effect size for quantitative outcomes such as pseudoarthrosis, 90-day readmission rate, and 90-day emergency department visits. 17 We deemed the random-effects model appropriate, given the underlying variability in the studies included, such as the inclusion of a wide variety of spinal surgeries, heterogeneity in patient samples, body weight, diabetic control, variable follow-up times, as well as variable use of causal inference techniques. A leave-one-out sensitivity analysis was conducted by iteratively excluding 1 study at a time from the meta-analysis to evaluate its impact on the pooled estimate. Heterogeneity was assessed using the I2 statistic, with values greater than 50% indicating substantial heterogeneity.
Publication Bias and Ethical Approval
Since all meta-analyses included fewer than ten studies, publication bias was not assessed, as recommended by the Cochrane Handbook for Systematic Reviews. 18 Ethical approval was not required because this systematic review only used already published data with no interaction with human subjects.
Results
A total of 3263 records were identified in the initial systematic search of the databases. After de-duplication and screening based on eligibility criteria described above, 11 studies were included for the final review.19-29 Figure 1 displays the PRISMA flowchart for study selection. Prisma flowchart for study selection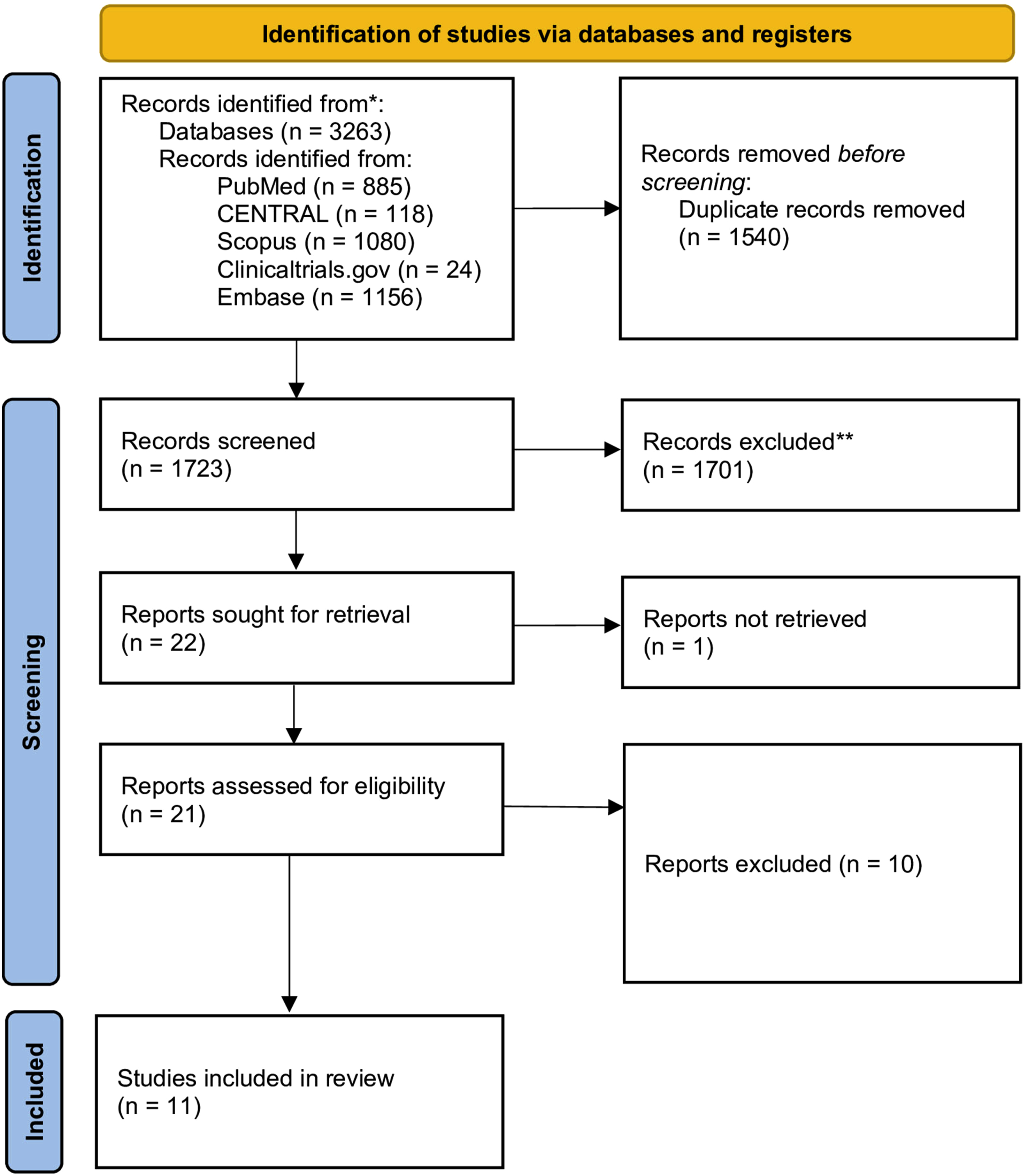
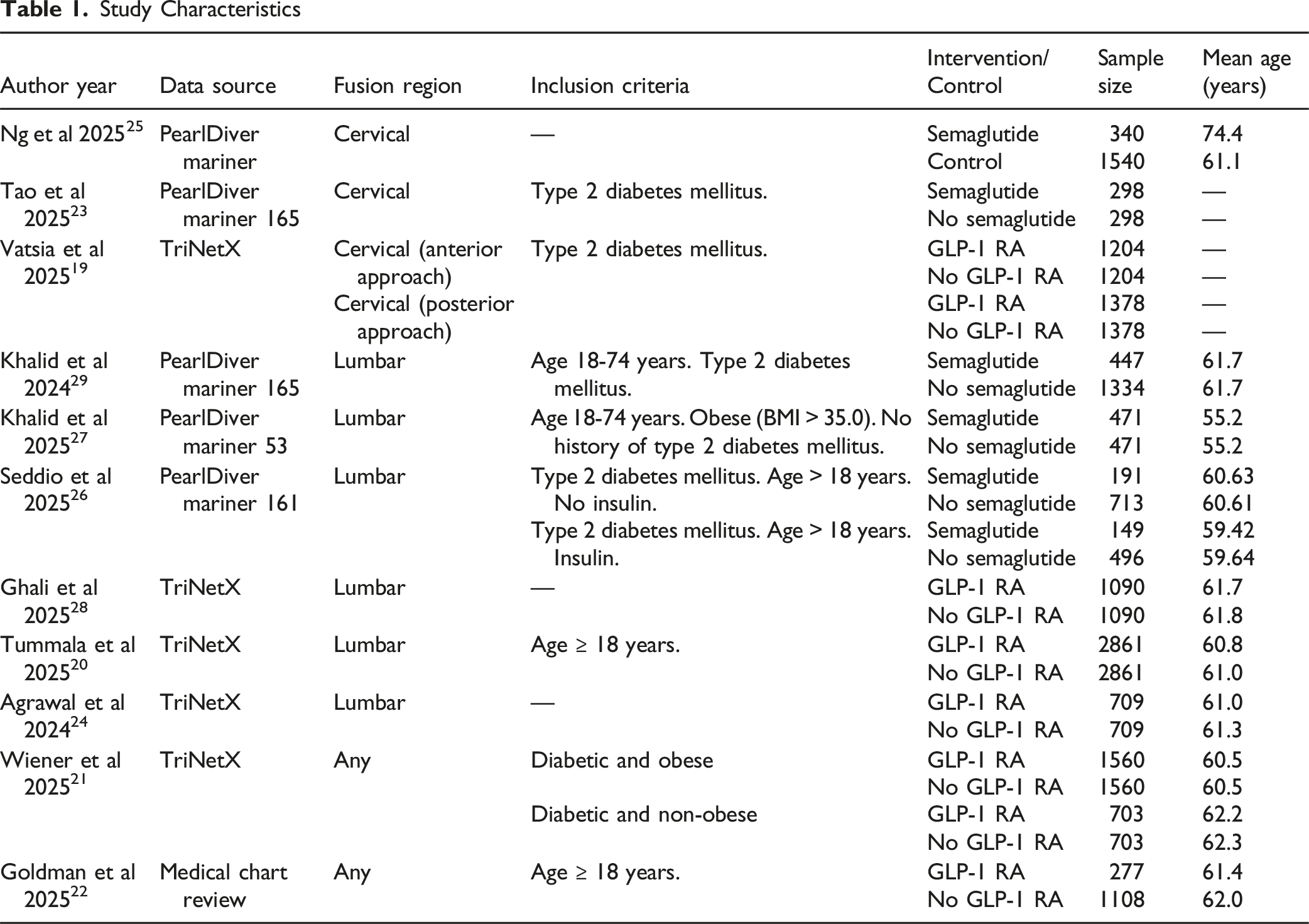
Study Characteristics
Study Characteristics
Risk of Bias
All 11 cohort studies were assessed as low risk of bias on the Newcastle-Ottawa Scale. Each study demonstrated appropriate cohort selection, comparability, and outcome ascertainment, supporting confidence in the overall findings (Supplemental Section 4).
Meta-Analysis Results
Pseudoarthrosis
Pseudoarthrosis rates were pooled from 3 studies, and the meta-analysis revealed comparable rates of pseudoarthrosis in GLP-1 RA users and non-users (Odds Ratio: 1.29 (95% CI: 0.09 - 19.23, P = .73). High heterogeneity was observed (I2 99%) (Figure 2). Forest plot showing the effects of GLP-1 RA use on pseudoarthrosis (follow-up of 2-3 years)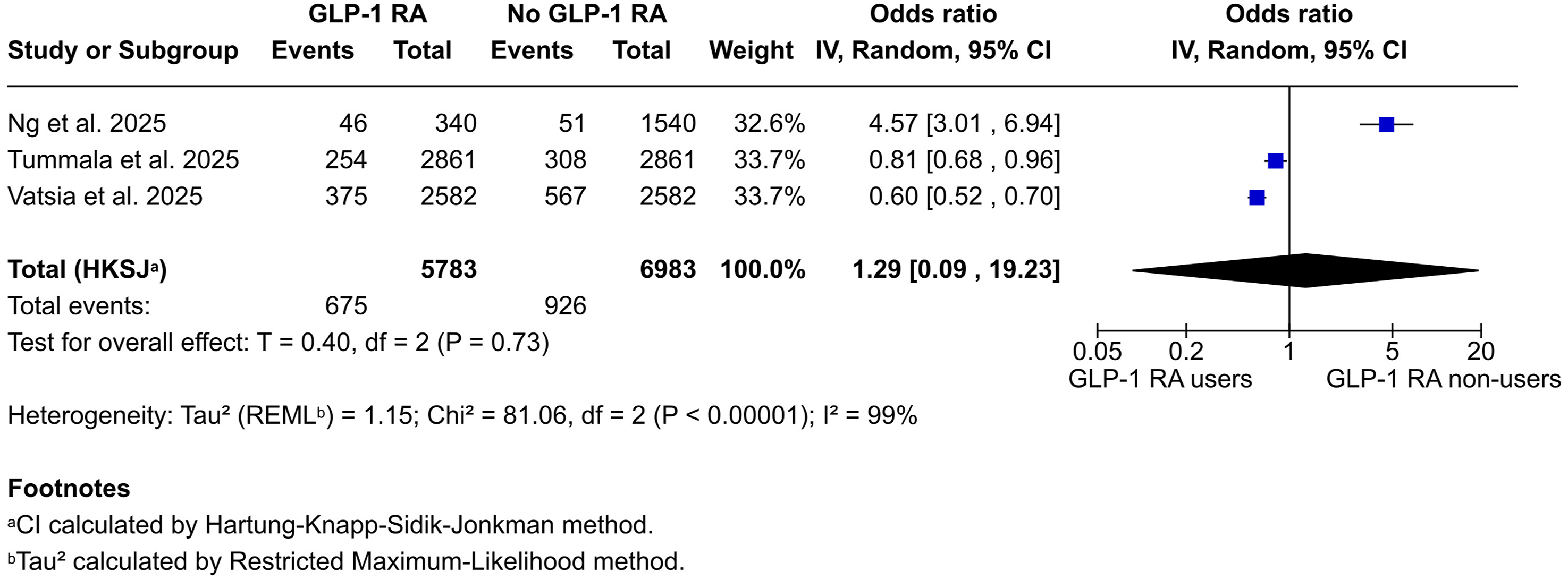
Surgical Site Infections
Surgical site infections were pooled from 4 studies, and the meta-analysis revealed comparable rates of surgical site infections between the 2 groups, with a statistically insignificant odds ratio of 0.97 (95% CI, 0.74 to 1.27; P = .72). No heterogeneity was observed (I2 0%) (Figure 3). Forest plot showing the effects of GLP-1 RA use on surgical site infections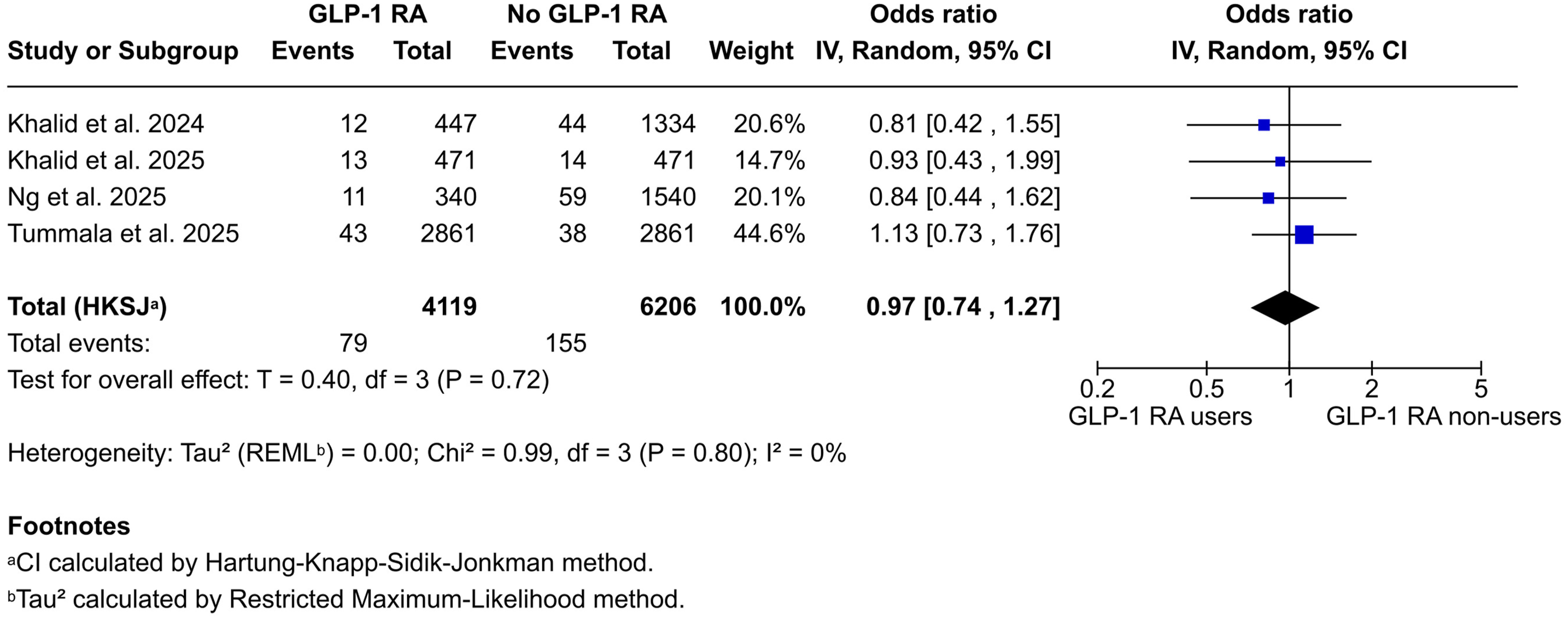
Pneumonia
Pneumonia was pooled from 4 studies, and the meta-analysis revealed comparable rates of pneumonia between the 2 groups with a statistically insignificant odds ratio of 1.19 (95% CI 0.30 to 4.68, P = .71). Moderate heterogeneity was observed (I2 71%) (Figure 4). Forest plot showing the effects of GLP-1 RA use on pneumonia
Deep Vein Thrombosis
Deep vein thrombosis was pooled from 4 studies and the meta-analysis revealed comparable rates of deep vein thrombosis between the 2 groups with a statistically insignificant odds ratio of 1.34 (95% CI 0.86 to 2.08, P = .13). No heterogeneity was observed (I2 0%) (Figure 5). Forest plot showing the effects of GLP-1 RA use on deep vein thrombosis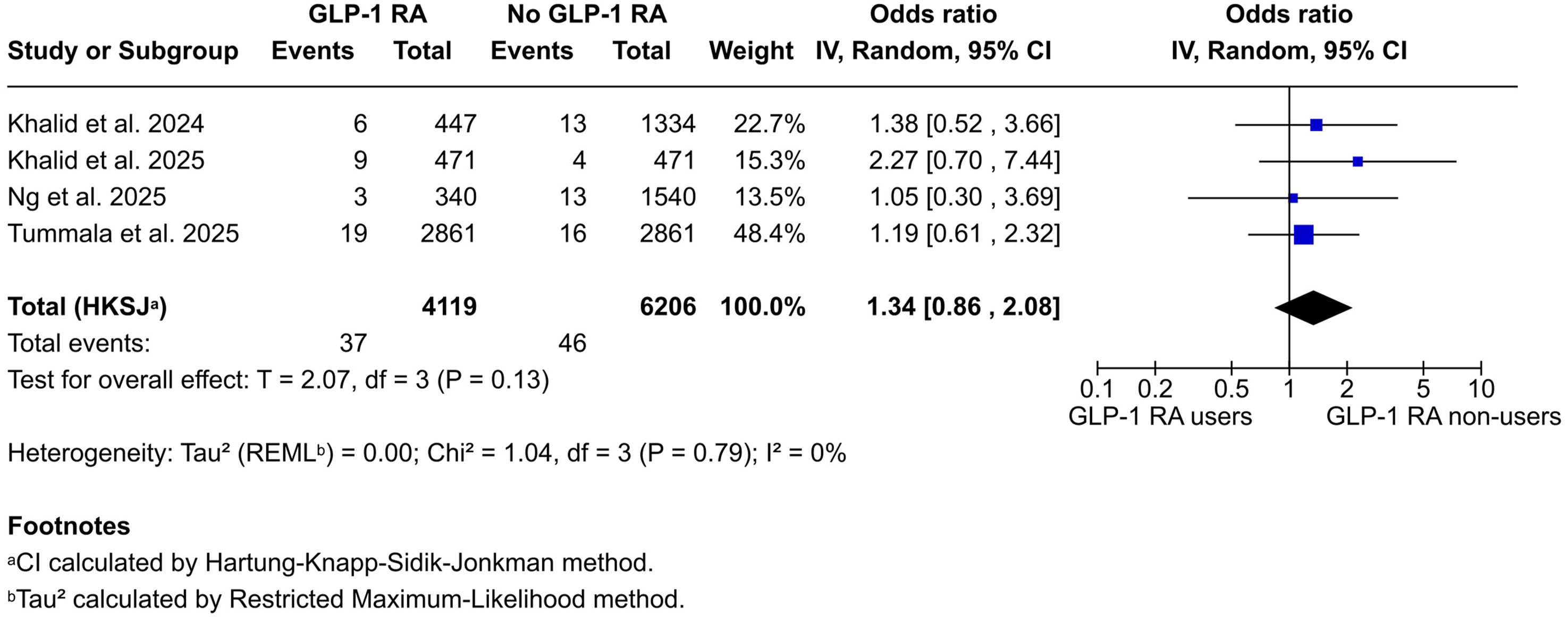
Acute Kidney Injury
Acute kidney injury (AKI) was pooled from 4 studies, and the meta-analysis revealed comparable rates of AKI between the 2 groups with a statistically insignificant odds ratio of 1.27 (95% CI 0.93 to 1.74, P = .09). No heterogeneity was observed (I2 0%) (Supplemental Section 5).
90-Day Readmission Rates
90-Day readmission rate was pooled from 4 studies, and the meta-analysis revealed comparable readmission rates between the 2 groups with a statistically insignificant odds ratio of 1.06 (95% CI 0.94 to 1.18, P = .22). No heterogeneity was observed (I2 0%) (Figure 6). Forest plot showing the effects of GLP-1 RA use on 90-day readmission rate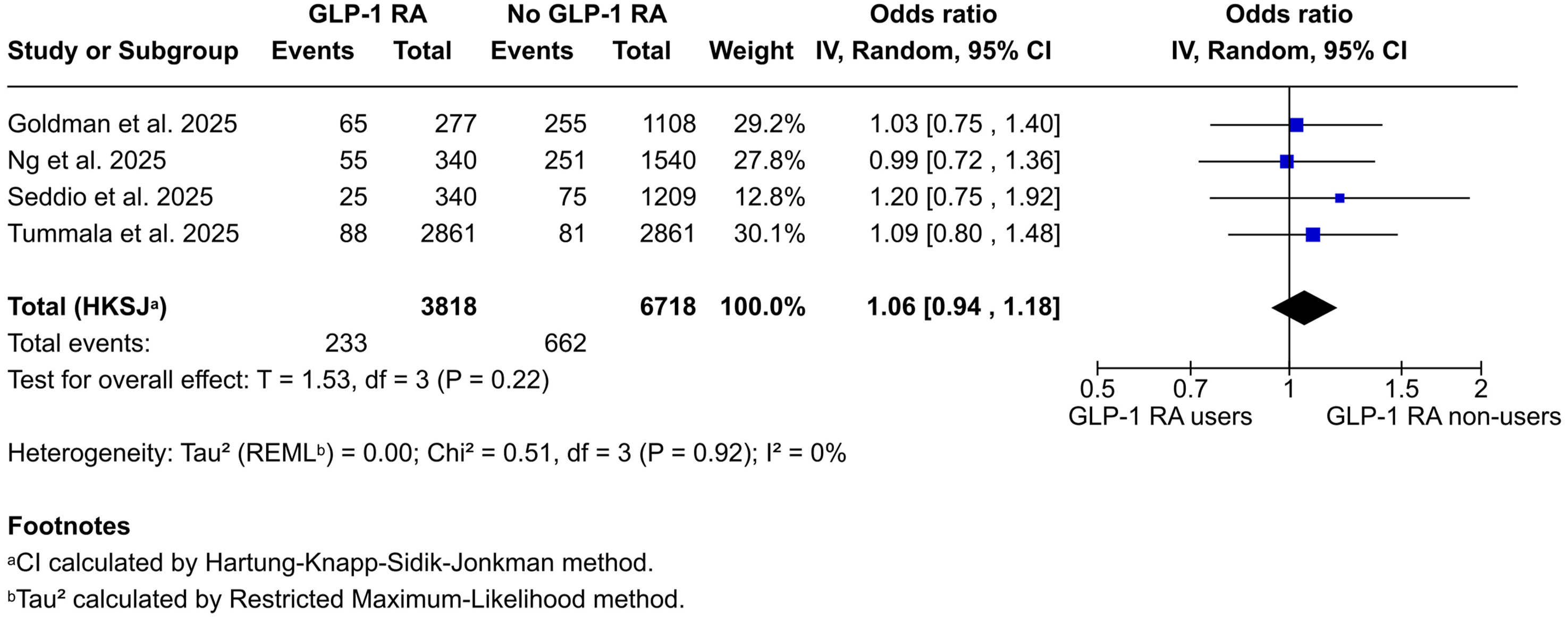
Emergency Department Visits at 90 days
Emergency department visits at 90 days were pooled from 4 studies and the meta-analysis revealed comparable visits to the emergency department between the 2 groups with a statistically insignificant odds ratio of 0.95 (95% CI 0.10 to 8.99, P = .93). High heterogeneity was observed (I2 96%) (Figure 7). Forest plot showing the effects of GLP-1 RA use on emergency department visits within 90 days
Sensitivity Analysis
Pooled estimates remained robust in leave-one-out sensitivity analysis for all outcomes except AKI. In AKI, the overall pooled estimate was not statistically significant (OR: 1.27 [0.93-1.74]). With the removal of Khalid et al 2024, 29 the pooled estimate demonstrated higher odds of AKI in GLP-1 RA users (1.14 [1.09-1.19]). Detailed results from the sensitivity analysis are provided in Supplemental Section 6. Of note, Khalid et al (2025) was the only study to include a subgroup analysis by prescription duration. Apart from higher odds of AKI and UTI with GLP-1 RA for greater than 9 months, they did not find differences in any other outcomes.
Qualitative Synthesis
A qualitative synthesis across 11 included cohort studies found a predominantly neutral to positive effect of GLP-1 RA compared to no GLP-1 RA in spinal surgery patients. Most results were not statistically significant. Regarding neurological outcomes, the 3- and 1-year foot drop rates showed small, non-statistically significant differences, with some studies reporting a marginally higher incidence in the GLP-1 group.20,28 Infection rates, sepsis, and composite surgical site outcomes were also similar between the groups.23,28 Although some studies showed decreased pseudoarthrosis rates at 3 years, this was not reflected in the pooled synthesis of the data. GLP-1 RA use had no effect on reoperation rates at 90-day or 1-year follow-up.20,22
Discussion
Over the past decade, GLP-1 RA use has grown substantially, with a reported monthly prescription growth rate of up to 254% for some drugs in this class. 30 Along with this rise, spine surgery candidates are increasingly using or asking about these drugs to attain appropriate preoperative diabetic and weight control. This systematic review is a comprehensive synthesis of current evidence on the perioperative use of GLP-1 RA in spine surgery. Pooled results from all studies demonstrated a neutral effect of GLP-1 RA use in spine surgery, with no significant increase or decrease in complications or fusion rates.
Existing guidelines and consensus statements on perioperative use of GLP-1 RA are “highly contradictory”. 31 Theoretically, GLP-1 RA raises the risk of certain immediate postoperative complications, such as increased gastric volume leading to aspiration pneumonia. 32 However, they also mitigate well-established surgical risks associated with poor glycemic control and obesity. Current evidence in spine surgery suggests that the theoretical risks and benefits balance out in the clinical setting, resulting in no appreciable impact on complication rates. Most studies employed propensity score matching and adjusted for covariates, thereby reducing confounding bias. In the final pool estimate, there was no significant risk or benefit associated with GLP-1 RA use in spine surgery. This aligns with the results of a meta-analysis evaluating the use of GLP-1 RA in patients undergoing arthroplasties. 33 Except for reduced risk of periprosthetic joint infection, GLP-1 RA did not affect any other surgical or medical outcomes.
GLP-1 RAs have been associated with improved bone health, which raises the possibility of enhanced fusion rates in spine surgery. A recent meta-analysis by Tan et al demonstrated that GLP-1 RAs lead to a statistically significant increase in bone mineral density (mean difference = 0.06 g/cm2, 95% CI: 0.04-0.07, P < .001) and certain bone turnover markers. 34 However, they did not find a corresponding decrease in fracture risk in GLP-1 RA users. In our meta-analysis, although some studies reported a reduction in the incidence of pseudoarthrosis in the GLP-1 RA group, the pooled estimate showed no statistically significant difference (OR: 1.29 [95% CI: 0.09-19.23]; P-value = 0.73). This aligns with the growing doubts about the use of bone mineral density or Dual-Energy X-ray Absorptiometry (DEXA) as a surrogate for fracture risk and spinal fusion rates.35,36 However, since most studies in our meta-analysis did not adjust for osteoporosis, relied on billing codes to assess fusion, and had a relatively short follow-up duration (2-3 years), further evidence is needed to conclusively determine the impact of GLP-1 RA use on spinal fusion rates.
Generalizability of current evidence may be limited due to confounding by indication. GLP-1 RA are not first-line drugs for either diabetes or obesity. Most patients are prescribed GLP-1 RA when they either fail first-line treatment or have clinical complications due to obesity. 37 However, most studies in our review queried administrative databases to construct 2 groups: GLP-1 RA users and non-users. While some studies reported subgroup analyses based on diabetes or obesity status, none explicitly ensured that the control group was truly comparable to the exposure group in terms of body mass index (BMI) thresholds, failure of first-line diabetic therapies, or complications of obesity or diabetes. Therefore, it is likely that GLP-1 RA users have a greater metabolic risk than non-users. Matching on administrative billing codes does not account for disease severity or treatment failure, so this matching does not represent accurate causal inference. Despite this, if this ‘higher-risk’ GLP-1 RA cohort achieved comparable complication rates to the control group in these observational studies, we hypothesize that the true protective effect of GLP-1 RA therapy is likely underestimated. A randomized controlled trial with balanced baseline metabolic risk may reveal the true magnitude of GLP-1 RA benefits. Nonetheless, from a surgical standpoint, achieving adequate glycemic control and appropriate BMI remain key objectives, irrespective of the medical treatments used to achieve them.
Strengths and Relevance
This is the first systematic review and meta-analysis to collate the studies on the safety and efficacy of GLP-1 RA use in spine surgery. We identified that currently, there is no established risk or benefit associated with GLP-1 RA use; however, the quality of evidence is limited and needs further research for definitive conclusions. Future research on the topic should report the comparability of the cohorts in terms of specific indications of GLP-1 RA, quantify glycemic control, baseline metabolic laboratory values, and weight loss achieved preoperatively and in the follow-up period, and include information on the concurrent use of other anti-diabetic and weight loss medications. Moreover, it is critical to include details on dosing, frequency, and duration of GLP-1 RA use to enable mechanistic interpretation and generalizability of results. Lastly, to assess the impact on fusion rates in GLP-1 RA users, ideally, prospective studies should be designed adjusting for baseline bone mineral density, and include radiological assessment of fusion.
Limitations
Findings of this review must be considered in light of its limitations. First, most studies used 2 administrative databases, making it difficult to prevent the inclusion of duplicates in the pooled analysis. Since this is a relatively new issue, there is no established guidance on this matter. However, we used the algorithm published by Lock et al to mitigate the inclusion of duplicate patients to the maximum extent possible. 16 Studies from the same timeframe and databases with an overlapping eligibility criterion were deemed duplicates and only 1 of those studies was included in the pooled estimates. Nevertheless, it cannot be guaranteed that there were no duplicates in the final analysis. Second, most of the data was retrospective, which risks biased results and cannot establish causality. However, all the studies included in the review employed causal inference techniques for observational studies, such as propensity score matching, thereby minimizing confounding to the maximum reasonable extent. Third, studies included heterogeneous patient samples, such as different anatomical regions and variable eligibility criteria. However, except for AKI, none of the results changed in the sensitivity analysis, indicating robustness of the pooled estimates reported. Moreover, we believe that heterogeneity improves the external validity of the findings. Despite these limitations, this study has several strengths. To our knowledge, it is the first meta-analysis to provide pooled estimates of GLP-1 RA use in spine surgery. Moreover, since the underlying studies utilized nationally representative data, the findings are generalizable to the US population.
Conclusion
Currently available level 4 evidence suggests that perioperative GLP-1 RA use in spine surgery candidates does not affect the risk of postoperative complications. However, these studies are based on administrative databases and may be confounded by indication. Future studies should include glycemic control and weight loss in their analysis to better elucidate the impact of GLP-1 RA on spine surgery outcomes.
Supplemental Material
Supplemental Material - Glucagon-Like Peptide-1 Receptor Agonist Does Not Impact Spine Surgery Outcomes: A Systematic Review and Meta-Analysis
Supplemental Material Glucagon-Like Peptide-1 Receptor Agonist Does Not Impact Spine Surgery Outcomes: A Systematic Review and Meta-Analysis by Syed Ibrahim, Abrahim Durrani, Muhammad Talal Ibrahim, Nicolas Kuttner, Phillip Glivar, Varun Kumar Singh, Elizabeth Yu in Global Spine Journal
Footnotes
Author Contributions
Conception and design (SI, MTI, VKS, EY); article screening and selection (SI, AD, MTI); data extraction and quality assessment (SI, AD, MTI); pooling of results (MTI, NK, PG); first draft of the manuscript (SI, AD, MTI); critical review of the manuscript (all authors); supervision (EY); read and approved the final version of the manuscript (all authors); take responsibility for all sections of the manuscript (all authors).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data are publicly available.
Supplemental Material
Supplemental Material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.