
Abstract
Study design
A retrospective cohort study.
Objective
Severe rigid spine deformity presents major challenges in surgical correction. Although three-column osteotomies (3-CO) provide powerful correction, they are associated with prolonged operative time, increased blood loss, and high neurological risk. This study aimed to compare the radiographic correction, surgical parameters, and complication profiles between staged halo-pelvic traction combined with posterior spinal fusion (HPT+PSF) and one-stage posterior spinal fusion (PSF) in patients with severe rigid spine deformity requiring 3-CO.
Methods
This retrospective cohort study included 110 patients (mean age, 25.7 ± 8.5 years) with severe rigid deformity (Cobb angle or maximal kyphosis >90°, flexibility <30%) who underwent either staged HPT+PSF (n = 60) or single-stage PSF (n = 50) between 2016 and 2023. Radiographic parameters, including the main curve Cobb angle and maximal kyphosis (MK), were measured preoperatively, post-traction, postoperatively, and at the latest follow-up. Operative time (ORT), estimated blood loss (EBL), osteotomy grade, intraoperative neuromonitoring (IONM) alerts, and complications were compared between groups. Pulmonary function tests (PFTs) were evaluated longitudinally.
Results
Following traction, the main curve Cobb angle and MK in the HPT+PSF group improved from 132.4° ± 23.3° to 65.1° ± 20.7° and from 122.3° ± 29.7° to 53.3° ± 24.1°, respectively. At the last follow-up, the correction rate of the main curve and MK were significantly higher in the HPT+PSF group than in the PSF group (62.9% vs 55.2%, P = 0.004; 67.7% vs 54.5%, P < 0.001). The HPT+PSF group demonstrated significantly reduced ORT (298.3 ± 64.7 vs 361.9 ± 76.3 min, P < 0.001) and EBL (490.5 ± 183.3 vs 1010.6 ± 252.1 mL, P < 0.001). The rate of IONM alerts (3.3% vs 20.0%, P = 0.005) and neurological deficits (3.3% vs 14.0%, P = 0.042) were markedly lower in the HPT+PSF group. Although traction-related complications occurred in 16.7% of patients, all were transient and resolved after adjustment of HPT devices.
Conclusion
Staged HPT followed by PSF provides a safe and effective strategy for the management of severe rigid spine deformities. In terms of radiographic correction and perioperative safety profile, this staged approach demonstrated significant advantages over one-stage 3-CO, notably reducing operative time, blood loss, and neurological risks. Preoperative traction effectively decreases deformity stiffness and magnitude, facilitating safer and less invasive surgical correction.
Keywords
Introduction
Severe rigid spine deformity remains one of the most demanding conditions in spinal surgery, characterized by large angular curvature, minimal flexibility, and frequent cardiopulmonary compromise.1,2 The primary goal of surgical management is to restore global spinal balance, achieve adequate deformity correction, and relieve cardiopulmonary restriction while minimizing neurological complications. However, due to the rigidity of the deformity and the proximity of neural elements, conventional posterior instrumentation or low-grade osteotomies often fail to provide sufficient correction.
Spine instrumentation and three-column osteotomies (3-CO), including pedicle subtraction osteotomy (PSO), bone–disc–bone osteotomy (BDBO), and vertebral column resection (VCR), have become standard techniques for such cases.3-5 These procedures enable powerful correction but are associated with extensive operative time, increased blood loss, and a high risk of neurological complications, with reported rates of neurological deficits up to 30%. Thus, strategies that reduce surgical aggressiveness while maintaining correction efficacy are clinically desirable.
Halo–pelvic traction (HPT) provides gradual deformity correction and soft-tissue adaptation before definitive fusion, potentially improving cardiopulmonary function and reducing deformity stiffness.6-8 Although its use has declined with modern instrumentation, recent evidence suggests that staged HPT followed by posterior spinal fusion (PSF) may achieve satisfactory correction with improved safety profiles compared to one-stage high-grade osteotomy procedures.9,10 However, direct comparative data between these 2 approaches remain scarce.
The present study aimed to compare the radiographic correction, surgical parameters, and complication profiles between staged HPT combined with PSF and one-stage PSF in patients with severe rigid spine deformities requiring 3-CO. We hypothesized that preoperative HPT could achieve comparable or superior correction while reducing operative time, blood loss, and neurological complications.
Methods
Patient Cohort
This is a single-center retrospective cohort study conducted from January 2016 to January 2023. Patients with severe rigid spine deformity who underwent either staged halo-pelvic traction combined with posterior spinal fusion (HPT+PSF) or single-stage PSF were retrospectively included. All surgical procedures were performed by the same senior spine surgeon. The inclusion criteria were as follows: 1. The coronal Cobb angle of the main curve or the maximal kyphosis greater than 90°; 2. Flexibility less than 30%; 3. Requiring three-column osteotomy (3-CO) based on surgical decision-making; 4. Minimum 2-year postoperative follow-up. Exclusion criteria included a history of active spinal infection, previous spine surgery and intolerance to HPT or PSF. The indications for 3-CO in our center were as follows: (1) fixed coronal and/or sagittal imbalance; (2) flatback deformity; (3) angular spine deformities with deformity angular ratio (DAR) > 20°11,12; (4) congenital spine deformity with circumferential fusion; (5) accompanied spinal cord compression or myelopathy. 13 Patients admitted before 2019 primarily underwent one-stage PSF. From January 2020 onwards, the staged HPT+PSF protocol was recommended for all patients meeting the inclusion criteria. However, to respect patient autonomy and ensure safety, patients in the post-2020 period were assigned to the one-stage PSF group if they: (1) presented with contraindications to HPT (e.g., severe osteoporosis, cervical instability, or skull/skin infections); (2) demonstrated intolerance to the traction device during the initial trial (in the first week); or (3) expressed a strong preference for a single-stage procedure after a detailed explanation of both options. Therefore, this cohort was divided into the HPT+PSF group and the PSF group. Ethical approval was obtained from the institutional review board at Beijing Chao-Yang Hospital (Approval No. 2025-HU-505), and all participants provided informed consent prior to enrollment.
Surgical Technique
Halo-Pelvic Traction
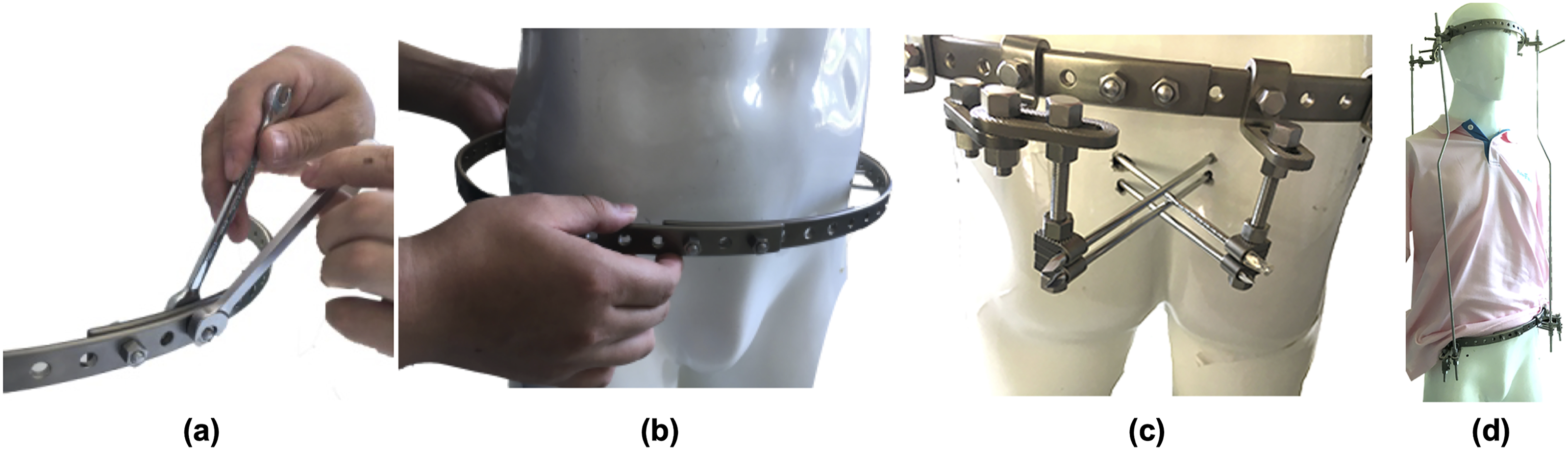
All patients underwent a standardized HPT protocol. Under general anesthesia, the pelvic fixation component was installed by placing 2 pins bilaterally into the iliac crest and the posterior superior iliac spine, waiting for the subsequent connection to a circular pelvic ring (Figure 1A-E). A standard halo ring was fixed to the skull with ten sharp-tipped pins, ensuring correct placement in safe zones around the skull (Figure 1F-G). Four threaded rods connected the halo ring to the pelvic ring, providing the foundation for gradual traction (Figure 2). Traction was initiated at a rate of 3-5 mm/day in the first week and reduced to 0.5-1 mm/day in the following weeks based on patient tolerance. Patients were closely monitored for neurological deterioration, pin-site infection, and mechanical complications. Daily neurological assessments and weekly radiographs were performed to evaluate the traction’s effects and detect potential complications. Neurological symptoms were treated by immediately reducing the traction distance by 10 mm and simultaneously administered methylprednisolone as well as mannitol via intravenous infusion. Gradual resumption could be tried if symptoms resolved. Once maximum safe correction was achieved via HPT, PSF surgery was performed with the HPT device sustained. The decision to terminate traction and proceed with definitive PSF was based on the following criteria: (1) achievement of the targeted radiographic correction (approximately 50% for the main curve or kyphosis); (2) observation of a correction plateau, indicated by no further significant improvement on sequential weekly radiographs; and (3) optimization of the patient’s nutritional status and pulmonary function. Illustration of the operating room phase of halo-pelvic traction devices setup. (a) patient positioning; (b-c) pelvic pin insertion in one side; (d) patient repositioning to the opposite side; (e) pelvic pin insertion in the opposite side; (f-g) halo ring installation Illustration of the non-operating room phase of halo-pelvic traction devices setup. (a-b) Pelvic ring assembly by combining the 2 semi-circular rings; (c) fixing pelvic pins to the pelvic ring; (d) installing vertical threaded rods to connect pelvic ring and halo ring
Posterior Spinal Fusion
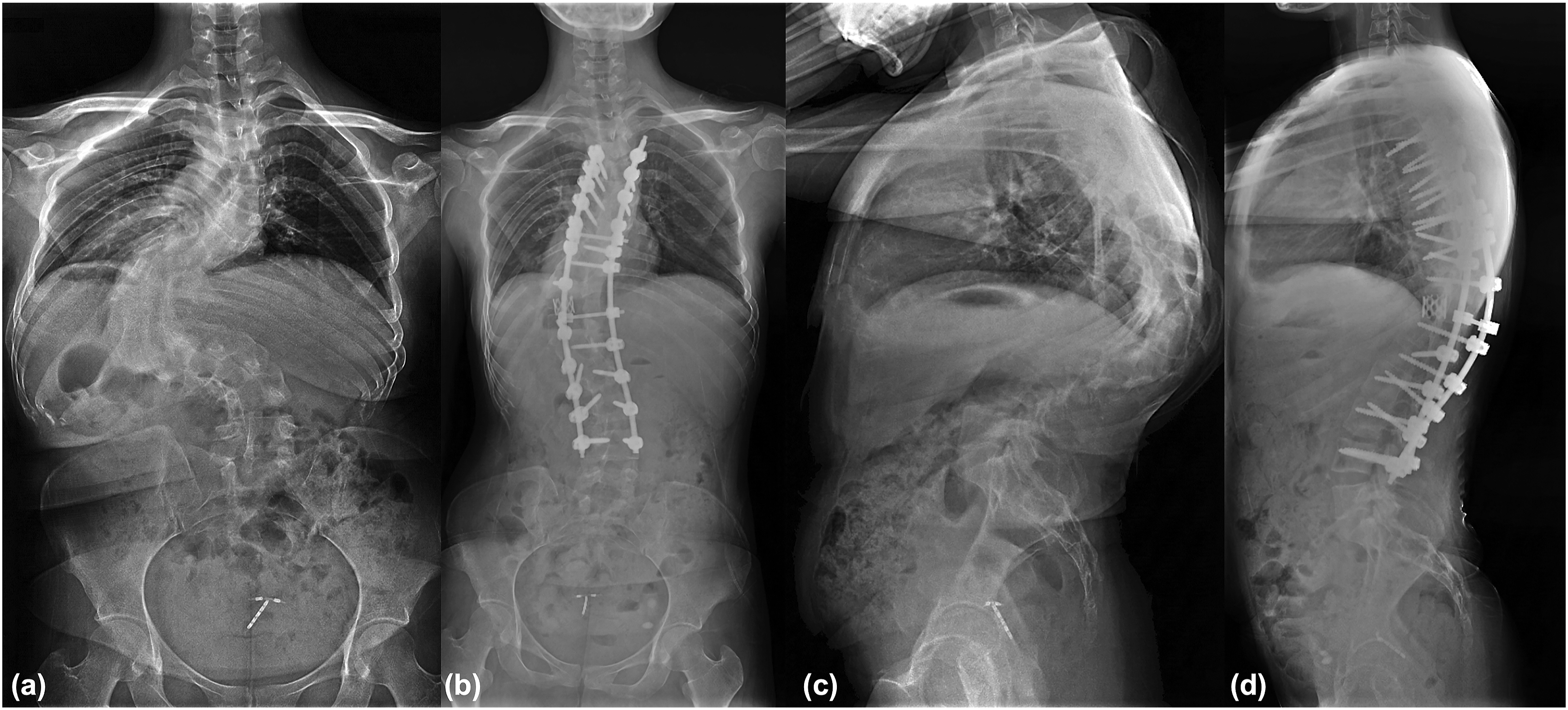
All patients underwent PSF under general anesthesia. The spine was exposed through a posterior midline approach, and pedicle screws were inserted at the planned levels. The osteotomy technique—Smith–Petersen osteotomy (SPO), Ponte osteotomy, pedicle subtraction PSO, BDBO, VCR, or a combination of osteotomies—was selected according to surgical planning. Appropriately contoured rods were connected to the screws, and correction was achieved through vertebral derotation, concave distraction, convex compression maneuvers and thoracoplasty. Fluoroscopy confirmed satisfactory implant positioning and balanced shoulder–pelvic alignment before final tightening. Posterolateral fusion was completed using autologous and allogeneic bone grafts placed along the decorticated lamina and facet joints. Titanium cage with bone grafts was placed for interbody fusion in patients underwent VCR. Representative case examples were presented in Figures 3 and 4. Continuous intraoperative neuromonitoring (IONM) including somatosensory evoked potentials (SSEPs) and transcranial motor evoked potentials (MEPs) was applied throughout the procedure, with MEPs serving as the standard for detecting neurological compromise. An actionable IONM alert was strictly defined as a ≥80% decrease in MEPs amplitude, or a complete loss of the MEPs signal, compared to the established baseline. A 38-year-old female with congenital spine deformity who underwent 19-week staged halo-pelvic traction combined with posterior spinal fusion (PSF). The main curve Cobb angle improved from 147.5° preoperatively to 74.2° post-traction, and further to 65.3° at the last follow-up after PSF. The maximal kyphosis (MK) improved from 129.7° preoperatively to 65.0° post-traction, and further to 52.8° at the last follow-up after PSF. The correction rate of main curve Cobb angle and MK was 55.7% and 59.3%, respectively. The deformity angular ratio (DAR) was markedly reduced from 21.1 preoperatively to 10.6 post-traction, and ultimately to 9.3 at the last follow-up after PSF A 35-year-old female with congenital spine deformity who underwent one-stage posterior spinal fusion (PSF) and apical vertebral column resection. The main curve Cobb angle was corrected from 132.6° preoperatively to 60.7° at the last follow-up after PSF. The maximal kyphosis (MK) was corrected from 125.9° preoperatively to 56.8° at the last follow-up after PSF. The correction rate of main curve Cobb angle and MK was 54.2% and 54.9%, respectively. The deformity angular ratio (DAR) was markedly reduced from 22.1 preoperatively to 10.1 at the last follow-up after PSF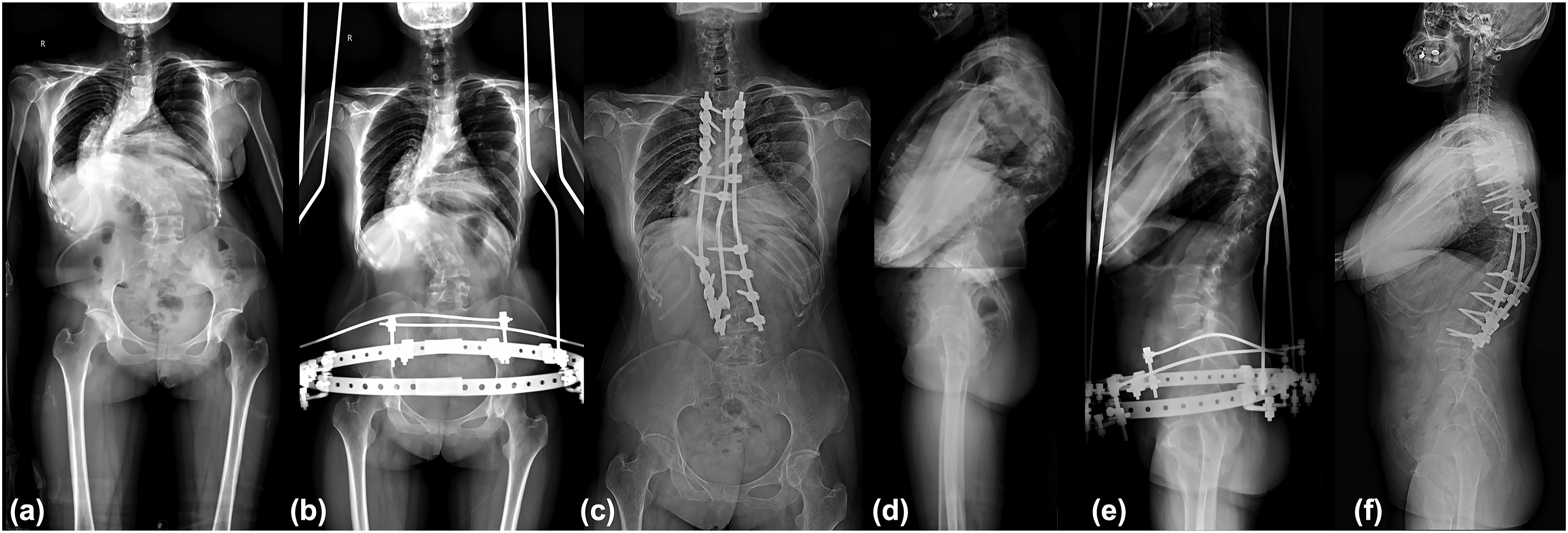
Evaluation of Radiographic Deformity Correction
Radiographic parameters were assessed using standing posteroanterior and lateral full-length radiographs. In the HPT+PSF group, measurements were obtained at 4 time points: pre-traction, post-traction, postoperative (2 weeks after surgery), and at the latest follow-up. In the PSF group, evaluations were conducted preoperatively, postoperatively, and at the latest follow-up. The measured parameters included the main curve Cobb angle, maximal kyphosis (MK) angle, coronal balance distance (CBD), and sagittal vertical axis (SVA). The deformity correction rate was calculated as the difference between the first and the last measurement points. All radiographic measurements were performed independently by 2 spine surgeons who were not involved in the surgical treatment of the patients. Measurements were conducted on digital radiographs using a standard Picture Archiving and Communication System. The mean values of the 2 measurements were calculated and used for the final statistical analysis.
Evaluation of Surgical Variables and Complications
In the HPT+PSF group, the duration of traction was recorded. Surgical variables, including operative time (ORT), estimated blood loss (EBL), SRS–Schwab osteotomy grade, and intraoperative neurological monitoring (IONM) alerts, were compared between the 2 groups. Traction-related and surgery-related complications were recorded. Neurological deficit was classified based on the duration of symptoms (transient or permanent) and anatomical level of involvement (spinal cord or nerve root). A transient deficit was defined as a new-onset neurological deficit that resolved completely within the follow-up period, whereas a permanent deficit was defined as one persisting at the last follow-up. Nerve root deficits were defined as unilateral motor or sensory disturbances consistent with a specific dermatome or myotome. Spinal cord deficits were characterized by bilateral sensorimotor deficits, long tract signs, bowel/bladder dysfunction, or paraplegia indicative of myelopathy.
Pulmonary Function Test
Pulmonary function tests (PFT) were conducted pre-traction, post-traction, and at the last follow-up in the HPT+PSF group. In the PSF group, tests were performed preoperatively and at the latest follow-up. Parameters including forced vital capacity (FVC), percentage of predicted FVC (FVC%), forced expiratory volume in one second (FEV1), and percentage of predicted FEV1 (FEV1%) were recorded.
Statistical Analysis
All statistical analysis were performed using IBM SPSS Statistics, version 27 (IBM Corporation, Armonk, NY, USA). The Shapiro-Wilk test was performed to determine whether continuous variables had a normal distribution. Continuous variables with a normal distribution are presented as the mean ± standard deviation; otherwise, the median and interquartile range are used. The counts and percentages are presented for categorical variables. Repeated-measures analysis of variance (ANOVA) and post hoc tests were used to compare differences in continuous variables between groups and across different measurement time points; for categorical variables, the Pearson chi-square test or Fisher’s exact test was applied. A two-sided P value of less than 0.05 was considered statistically significant.
Results
Baseline Characteristics
Baseline Characteristics
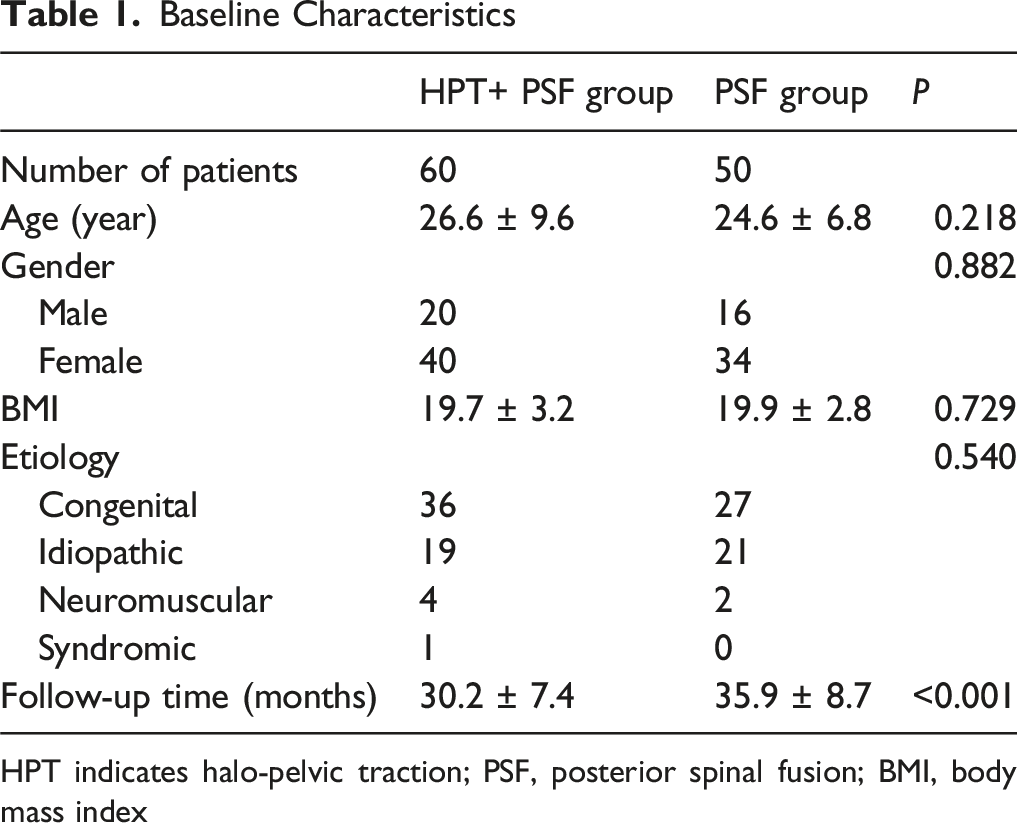
HPT indicates halo-pelvic traction; PSF, posterior spinal fusion; BMI, body mass index
Radiographic Parameters
Comparison of Radiographic Parameters
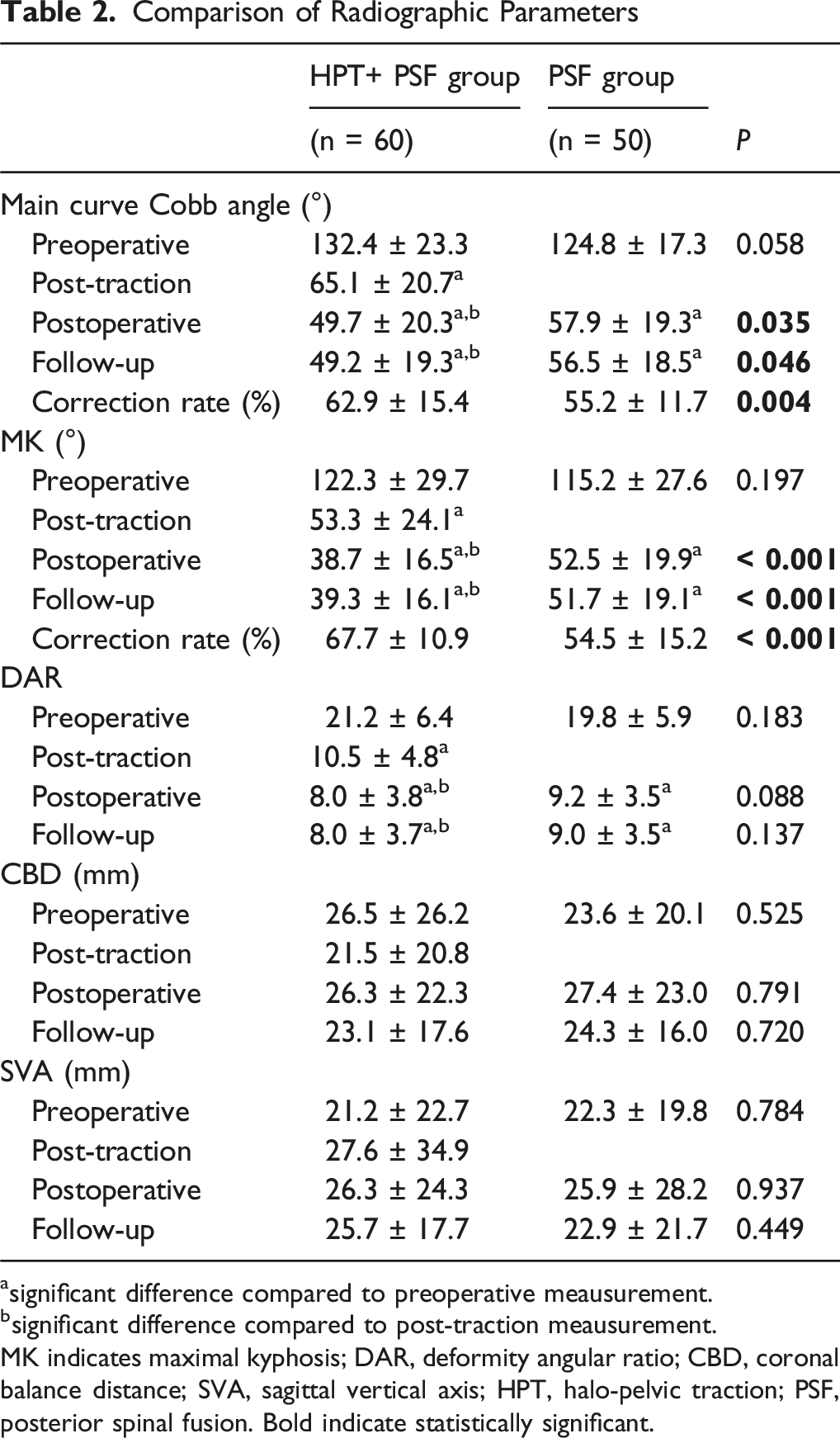
asignificant difference compared to preoperative meausurement.
bsignificant difference compared to post-traction meausurement.
MK indicates maximal kyphosis; DAR, deformity angular ratio; CBD, coronal balance distance; SVA, sagittal vertical axis; HPT, halo-pelvic traction; PSF, posterior spinal fusion. Bold indicate statistically significant.
Pulmonary Function Outcomes
Comparison of the Pulmonary Function
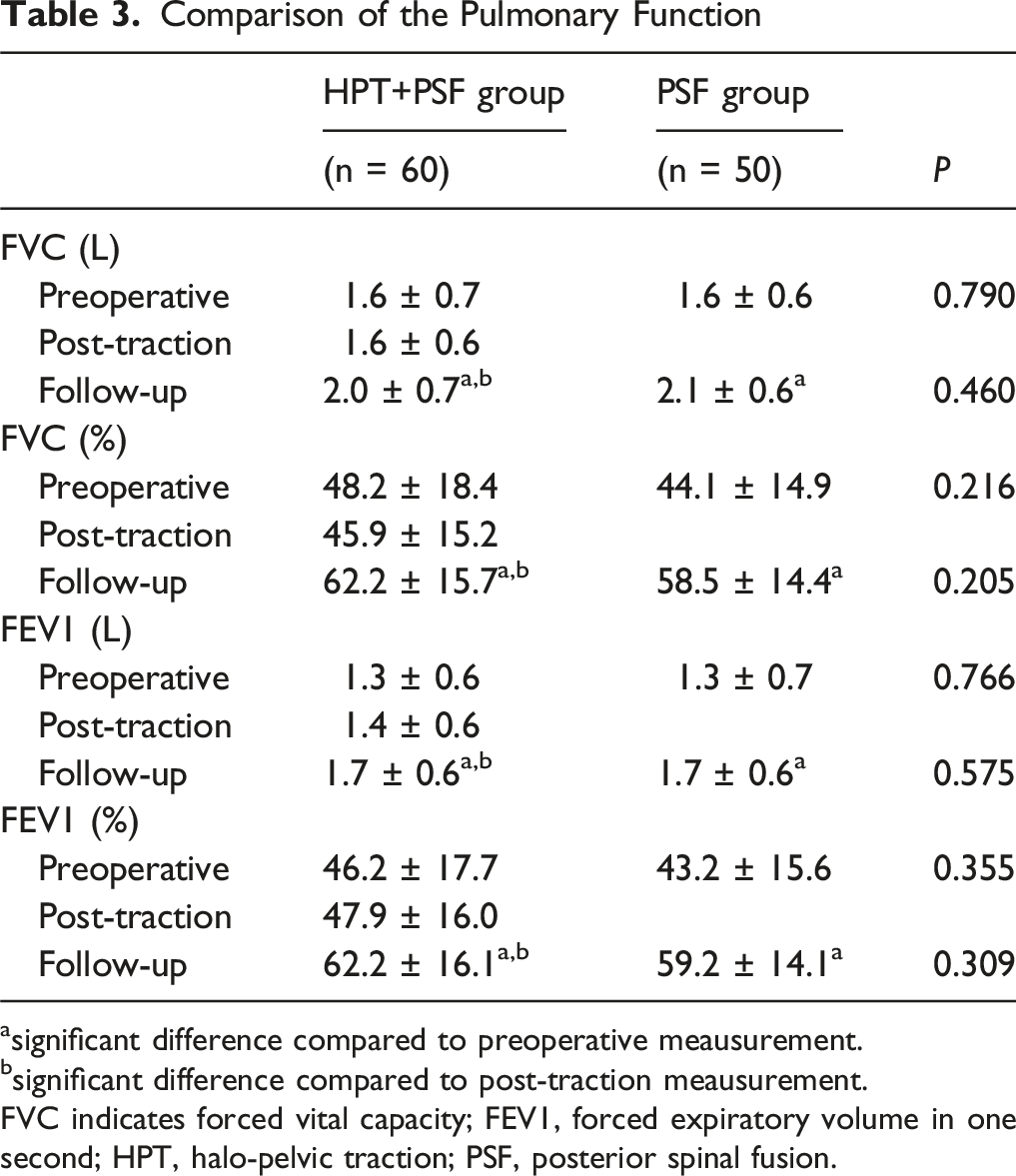
asignificant difference compared to preoperative meausurement.
bsignificant difference compared to post-traction meausurement.
FVC indicates forced vital capacity; FEV1, forced expiratory volume in one second; HPT, halo-pelvic traction; PSF, posterior spinal fusion.
Surgical Variables
Surgical Variables
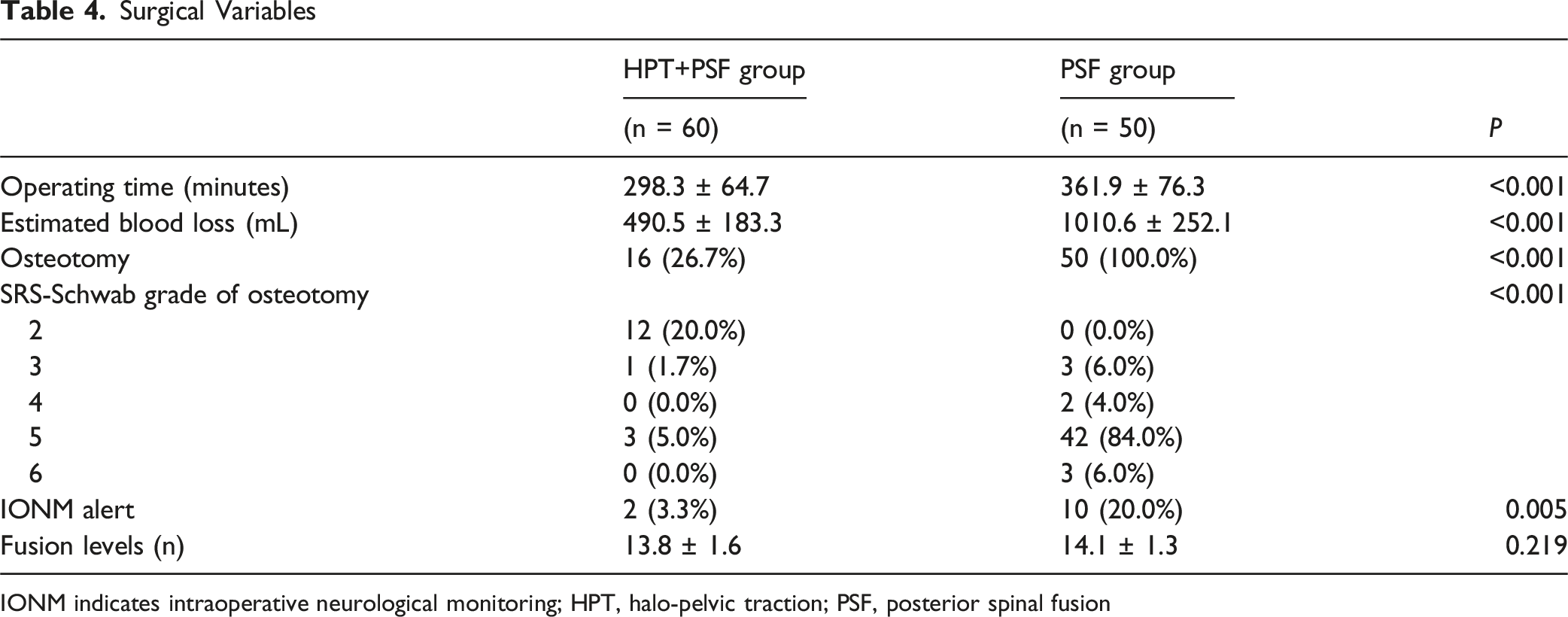
IONM indicates intraoperative neurological monitoring; HPT, halo-pelvic traction; PSF, posterior spinal fusion
Complications
Complications in Both Groups
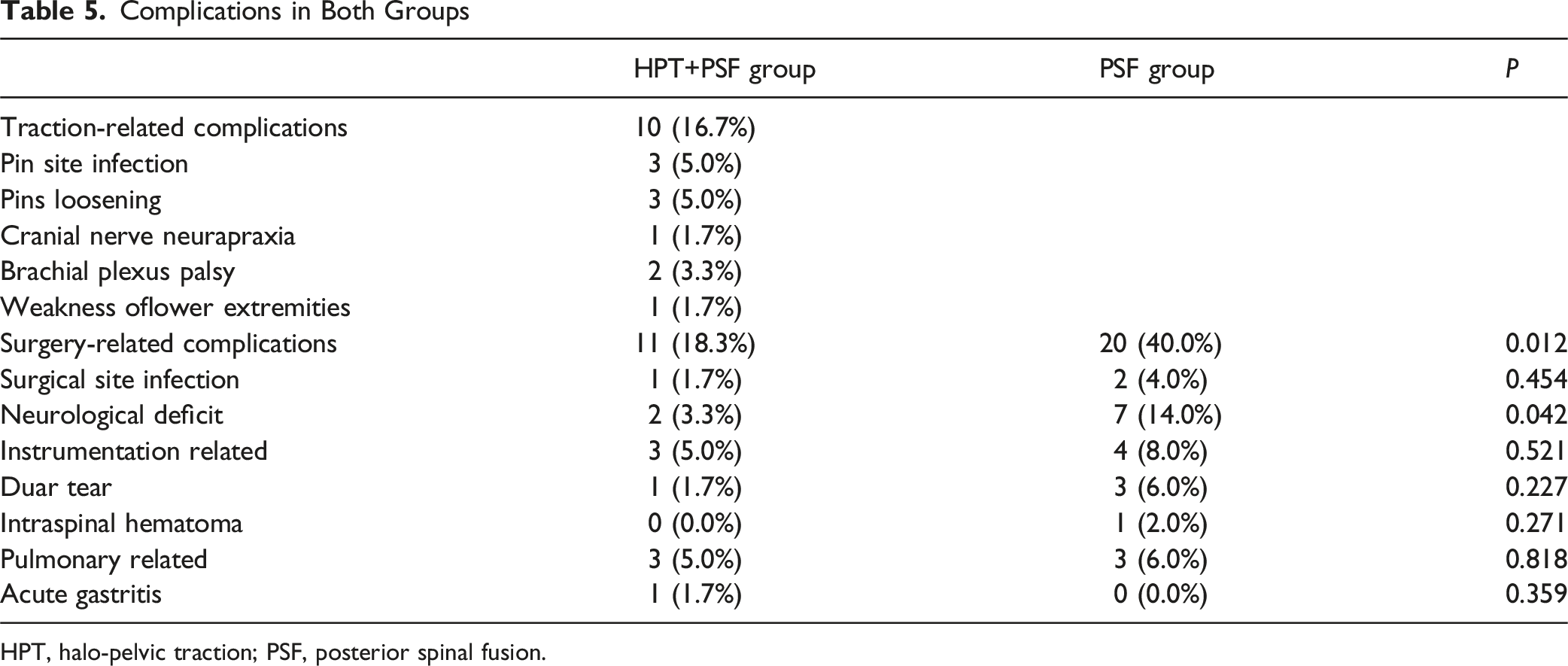
HPT, halo-pelvic traction; PSF, posterior spinal fusion.
Detailed Information of Neurological Deficits in Both Groups
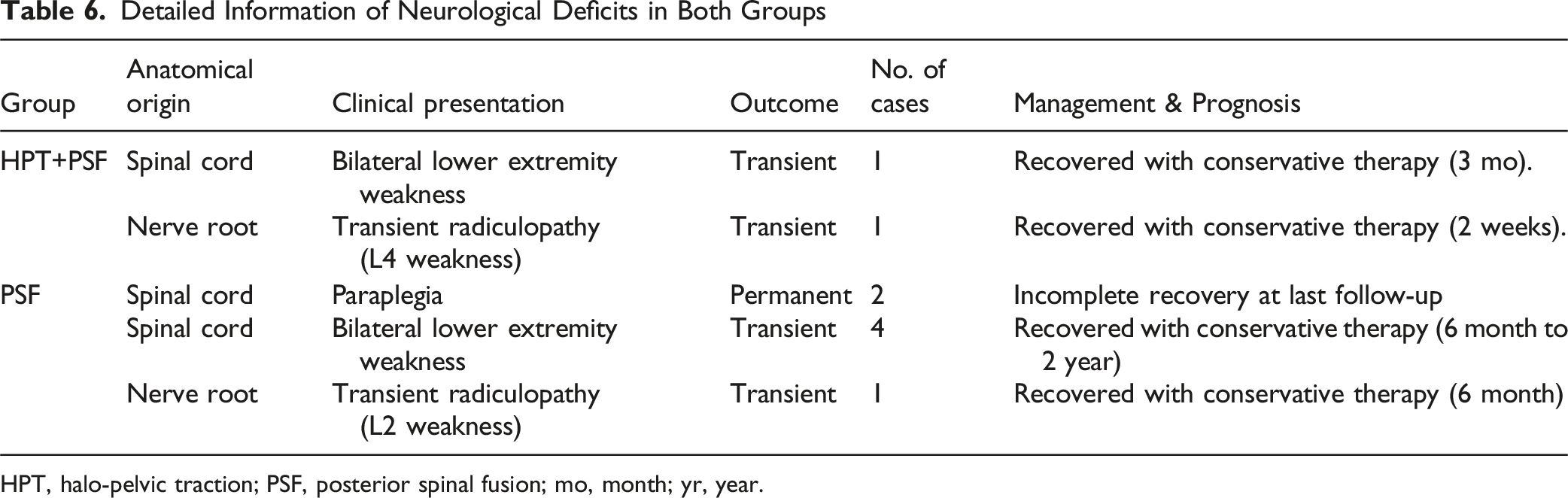
HPT, halo-pelvic traction; PSF, posterior spinal fusion; mo, month; yr, year.
Discussion
The management of severe rigid spine deformities remains one of the most formidable challenges in spine surgery, largely due to the technical complexity of deformity correction and the elevated risk of neurological injury. Since its introduction in 1971, HPT has served as an important modality in the preoperative management of complex spinal deformities. Nonetheless, its clinical use has progressively declined with the advancement and popularization of modern internal fixation techniques. Patients with severe rigid spine deformities frequently exhibit cardiopulmonary insufficiency, gastrointestinal disturbances, and poor nutritional status, all of which exacerbate the risks associated with one-stage corrective procedures. Such operations are often characterized by prolonged operative duration, excessive intraoperative blood loss, and a potential for irreversible spinal cord injury. Moreover, achieving satisfactory correction through a one-stage procedure and 3-CO remains technically demanding and is often associated with disproportionately high surgical risks and morbidity when the Cobb angle exceeds 100°. The findings of this study suggest that a staged strategy incorporating HPT followed by PSF provides a more effective and safer alternative for addressing the multifaceted challenges.
The primary goal of surgical treatment for spine deformity is to achieve satisfactory correction and restore global spinal balance. However, in cases of severe rigid spine deformities, relying solely on spinal instrumentation and low-grade osteotomies often yields suboptimal outcomes due to limited correction potential. To address this challenge, 3-CO techniques have been developed to achieve more powerful corrections. Among these, VCR provides the greatest corrective capability. A study by Riely et al reported that the major radiographic deformity was reduced by 61.6% in the pediatric cohort and by 53.9% in the adult cohort. 14 A systematic review by Yang et al suggested that the mean amount of correction by PVCR was 64.1° in scoliosis and 58.9° in kyphosis, accounting a correction rate of 61.2% and 63.1%, respectively. 15 Despite these impressive outcomes, 3-CO is technically demanding and associated with substantial surgical morbidity. Preoperative HPT offers an alternative strategy by gradually reducing the magnitude and rigidity of the deformity before definitive fusion, thereby decreasing the amount of correction required in the second-stage surgery. However, studies investigating the efficacy of staged HPT followed by PSF remain limited. Zhou et al reported that preoperative HPT combined with multi-level Ponte osteotomies and PSF could yield an overall correction rate of 58.3% in the coronal plane and 63.4% in the sagittal plane, which is comparable to previous studies reported for 3-CO. 2 A recent comparative study by Zhao et al reported that there were no significant differences in correction effects between HPT+PSF and one-stage PSF with PVCR for severe rigid spine deformity patients. 9 In the current study, even combining apical 3-CO and Ponte osteotomies to maximize release in the PSF group, patients in the HPT+PSF group achieved a more greater correction rate of main curve Cobb angle and MK. Following HPT, the main curve Cobb angle and MK were corrected to 65.1° ± 20.7° and 53.3° ± 24.1°, respectively. Although definitive PSF had not yet been performed, the correction achieved showed no significant difference compared with that observed in the PSF group after surgery (main curve Cobb angle, P = 0.062; MK, P = 0.856). Therefore, low-grade osteotomies, rather than apical 3-CO, were performed to further improve correction in the HPT+PSF group. These findings indicate that staged HPT combined with PSF can achieve superior deformity correction to one-stage 3-CO procedures, while potentially reducing surgical aggressiveness and technique requirements. It must be noted that the occurrence of IONM alerts inherently limits the ability to achieve maximal correction. When an alert is triggered, corrective maneuvers must be immediately halted or reversed to restore neural conduction and prioritize neurological safety, thereby compelling the surgeon to accept a suboptimal radiographic alignment. Our subgroup analysis confirmed this clinical compromise, demonstrating significantly lower final correction rates in patients who experienced intraoperative alerts compared to those who did not.
The choice between HPT and Halo-Gravity Traction (HGT) remains a topic of debate. While HGT is widely favored for its less-invasive nature, our center employs a strict stratification strategy based on patient age, etiology, and deformity rigidity. HGT is primarily indicated as the first-line treatment for pediatric patients, particularly those with severe early onset scoliosis aged under 10 years who are candidates for growing rod implantation, as well as for non-ambulatory patients with severe neuromuscular spine deformities. However, for the specific cohort of severe and rigid deformities addressed in this study, the passive, gravity-dependent force of HGT is often insufficient to overcome rigid bony ankylosis. In contrast, HPT establishes a closed mechanical loop between the skull and pelvis, providing an active, 24-hour continuous, and powerful distraction force that functions independently of patient positioning. A recent matched cohort study comparing these 2 modalities found that HPT achieved significantly superior radiographic correction in shorter durations for severe rigid curves compared to HGT. 16 Crucially, the study demonstrated that HPT patients were more likely to be down-staged to lower-grade osteotomies, whereas HGT patients with comparable baseline severity often still underwent 3-CO. We acknowledge that HPT is associated with higher invasiveness, risks and patient discomfort compared to HGT; however, we believe that the superior corrective efficacy and the potential to avoid high-risk 3-CO justify the use of HPT, provided that the manageable traction-related risks are meticulously monitored.
The current study found that both the ORT and the EBL were significantly reduced in the HPT+PSF group. A systematic review by Yang et al suggested that the mean ORT for PVCR was 430 min and the EBL was 2639 mL; However, study by Zhang et al reported that the ORT and EBL could be respectively shortened to 283 min and 842.31 mL by using multiple-level asymmetrical Ponte osteotomies for patients requiring VCR. 17 We considered that the reductions in ORT and EBL could be attributed to several factors. First, preoperative HPT decreases the severity of spinal deformity, facilitating easier exposure of the upper thoracic and lumbar region for pedicle screw placement during surgery, improving intraoperative efficiency. Second, HPT markedly reduces the degree of angular deformity of the main curve, transforming it from an angular shape into a smoother, arc-shaped configuration. Following HPT, the DAR was significantly reduced from 21.2 ± 6.4 to 10.5 ± 4.8 (P < 0.001). This morphological change alleviates allows for satisfactory correction with lower-grade osteotomies, thus avoiding the need for complex and high-risk 3CO. For patients who achieved satisfactory correction through HPT, osteotomy could be avoided, and only in situ spinal instrumentation and fusion were performed. If the placement of pedicle screws in the apical vertebra was challenging, this step could be omitted, and additional satellite rods spanning the apical region could be used for reinforcement instead, which would significantly reduce the ORT. Third, the significantly higher incidence of IONM alerts in the one-stage PSF group inherently prolonged the overall operative time. The process of addressing the IONM alerts introduces substantial intraoperative delays that are largely avoided in the HPT cohort. Collectively, these findings indicate that preoperative HPT not only simplifies the surgical procedure but also enhances its safety and efficiency in managing severe rigid spine deformities.
Neurological deficit represents one of the most devastating complications of spinal deformity surgery. The reported incidences of transient neurologic deficits ranging from 2.9% to 29.3% and permanent deficits occurring in 2.0-6.3% of cases.15,18-20 In neurological deficits, the spinal cord injuries were primarily attributed to 2 mechanisms: acute mechanical injury and ischemic injury. The permanent deficits observed in the one-stage PSF group were directly tied to the highly demanding technical steps of the 3-CO procedures. Upon review of the operative records for the 2 patients who sustained permanent deficits, the loss of IONM signals occurred during specific critical maneuvers. In one case, the alert was triggered during the closure of the osteotomy site. Despite immediate reversal of the maneuver, the signals did not fully recover, suggesting a direct mechanical compression related to dural buckling during apical shortening. In the second case, signal loss occurred during the posterior vertebral wall resection and ventral dural sac decompression. Severe adhesions between the ventral dura and the vertebral body complicated the dissection, leading to an acute massive hemorrhage (approximately 1000 mL) from the epidural venous plexus and a sudden drop in mean arterial pressure (MAP) to 70 mmHg. Despite immediate blood transfusion and rapid pharmacological elevation of MAP, the MEPs were permanently lost. These actual case events underscore that while 3-CO provides essential apical shortening, the requisite manipulations carry profound mechanical and acute physiological risks to the spinal cord. Previous studies have demonstrated that preoperative HPT can markedly reduce the incidence and severity of neurological complications—a finding consistent with our results.8,10 In the present study, the incidence of IONM alerts was significantly lower in the HPT+PSF group (3.3%) compared with the PSF group (20.0%); also, the incidence of neurological deficit was significantly lower in the HPT+PSF group, indicating enhanced neurological safety. Several factors may explain this safety advantage. First, HPT utilizes the viscoelastic properties of the spinal cord to mitigate mechanical and ischemic risks. The slow, continuous distraction allows neural tissue to lengthen gradually via biological creep, preventing the spike in intramedullary pressure associated with acute correction. Simultaneously, this gradual stretching promotes neovascularization and allows spinal cord blood flow to autoregulate to the new length over weeks, avoiding the ischemic shock of rapid lengthening. Second, clinically, HPT facilitates correction and decreases the need for high-risk 3-CO, thereby minimizing direct mechanical disturbance to the spinal cord. Third, the significantly reduced intraoperative blood loss in the HPT group helps maintain adequate mean arterial pressure, ensuring optimal spinal cord perfusion. In contrast to the abrupt alignment alterations that occur during one-stage 3-CO, HPT offers the spinal cord sufficient time to adapt to both pathological and physiological changes. For patients with IONM alerts during surgery, reducing the traction distance or removing the traction devices could be tried to protect the spinal cord from distraction injury. Collectively, these factors contribute to a safer correction process and a lower risk of neurological injury.
A critical consideration in adopting the HPT strategy is the duration of treatment. Our cohort underwent a mean of 20 weeks of traction, which indeed places a burden on patients and their families, representing a major downside compared to the one-stage surgery. While prolonged, this duration is strictly underpinned by both biomechanical safety and physiological necessity. Biomechanically, slow distraction (0.5-1 mm/day) is essential to avoid neurological ischemia and release the soft-tissue. Physiologically, a recent study utilizing 3D lung reconstruction demonstrated that the optimal improvement in lung volume is typically achieved after 4 to 6 months of HPT. 21 Notably, in the current study, standard PFT parameters did not show statistically significant improvement immediately post-traction. We attribute this to the physiological lag between anatomical expansion and functional recovery. Although HPT successfully expands the constricted thoracic cage and increases lung volume, the recruitment of atelectatic alveoli for effective gas exchange is a delayed process. The restoration of functional ventilation often requires a longer remodeling period, typically up to one year, to align with the structural expansion. Ultimately, surgeons might argue that foregoing the morbidity associated with prolonged traction is preferable if neurological deficit are merely transient or mild. However, the critical question is whether this burden could be justified by the safety benefits. In the current study, the risks of the one-stage procedure were not limited to transient issues; 2 patients in the PSF group (4.0%) sustained permanent spinal cord injuries. In contrast, the HPT+PSF group incurred no permanent neurological deficits. Thus, the clinical rationale for HPT is to exchange the temporary and manageable morbidity of traction for minimizing the risk of permanent and catastrophic disability. For young patients with such extreme spine deformities, we believe this investment in safety is justified.
One patient in the HPT+PSF group developed severe adding-on, necessitating revision surgery. The principal cause of this mechanical complication was the inappropriate selection of the lower instrumented vertebra (LIV). Although HPT can substantially reduce the magnitude of spinal deformity, the determination of the LIV should be guided by preoperative radiographic evaluation rather than post-traction alignment.
Limitation
Several limitations should be acknowledged in this study. First, the retrospective design and single-center nature may introduce selection and information bias, limiting the generalizability of the results. Second, although all surgeries were performed by an experienced surgical team following standardized protocols, individual variations in surgical decision-making—such as the selection of osteotomy grade or the precise duration of traction—might have influenced the outcomes. Third, the follow-up period, while exceeding 2 years for all patients, may still be insufficient to fully assess long-term complications such as implant failure, loss of correction, or junctional problems. Fourth, the relatively small sample size, particularly in subgroups undergoing 3-column osteotomies, restricts the statistical power for detecting differences in rare complications. Finally, we could not definitively claim the superiority of HPT because of the absence of patient-reported outcome measures (PROMs) such as SRS-22 or SF-36, which limits the evaluation of functional and quality-of-life improvements following different treatment strategies. Therefore, prospective multicenter studies with larger sample sizes, longer follow-up, and inclusion of PROMs are warranted to validate and expand upon our findings.
Conclusion
Staged HPT followed by PSF provides a safe and effective strategy for the management of severe rigid spine deformities. In terms of radiographic correction and perioperative safety profile, this staged approach demonstrated significant advantages over one-stage 3-CO, notably reducing operative time, blood loss, and neurological risks. Preoperative traction effectively decreases deformity stiffness and magnitude, allowing for safer and less aggressive corrective procedures. However, careful patient selection, standardized traction protocols, and precise surgical planning remain essential to minimize traction-related and mechanical complications.
Footnotes
Ethical Considerations
Ethical approval was obtained from the institutional review board at Beijing Chao-Yang Hospital (Approval No. 2025-HU-505).
Consent to Participate
All participants provided informed consent prior to enrollment.
Author Contributions
YH and LJZ were responsible for conceptualizing and designing the study. HHY, JXH, YHY, and HSG collected and analyzed the data. HHY and JXH drafted the original manuscript. YSW, YQZ, and YPZ provided substantial supervision and critical revisions. All authors have read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. If anyone needs the data and information from this study, please contact the correspondence authors.