
Abstract
Study Design
Retrospective cohort study.
Objectives
To examine the impact of non-tobacco nicotine (NTN) dependence on pseudarthrosis and postoperative complications following posterior cervical fusion (PCF).
Methods
The TriNetX national database was queried for adult patients (18-80 years) who underwent a primary posterior cervical fusion (2012-2025). Patients were stratified into 3 cohorts: non-tobacco nicotine-dependent (NTND) patients, tobacco-dependent (TD) patients, and non-dependent controls. Patients underwent propensity-score matching, and pairwise comparisons (NTND vs control, TD vs control, NTND vs TD) were performed. The primary outcome was pseudarthrosis development, and secondary outcomes included medical/surgical complications.
Results
A total of 7102 patients were included. At 3 years, NTND patients had higher rates of pseudarthrosis (2.51% vs 1.84%, P = 0.019) compared to matched controls. Compared to controls at 3 months and 3 years, NTND was associated with significantly higher risks of all other postoperative complications (P < 0.05) except DVT. Compared to controls, TD patients had higher rates of all postoperative complications at 3 months and 3 years, except pseudarthrosis (P < 0.05). Compared to TD patients, NTND patients had higher rates of cervical fracture and pneumonia at 3 months (P < 0.05), and higher rates of cervical fracture at 3 years (P < 0.05). At 3 months, the NTND cohort demonstrated lower rates of opioid abuse/dependence, readmission, and emergency service use (P < 0.05).
Conclusions
Non-tobacco nicotine dependence is associated with risk of perioperative and long-term complications following posterior cervical fusion compared to control patients, yet is not significantly different from TD patients. Providers may consider this data during preoperative counseling and surgical optimization.
Level of Evidence
III.
Keywords
Introduction
Posterior cervical fusion (PCF) is commonly indicated to address an array of traumatic and/or degenerative cervical spine pathologies, including but not limited to: cervical myelopathy, cervical radiculopathy, instability, and spinal cord trauma.1,2 Despite advances in surgical technique, implant manufacturing, and novel image guidance, complications like pseudarthrosis and infection remain clinically significant, especially in patients with modifiable risk factors. 3 Identification and optimization of these risk factors is an important component of perioperative management in patients scheduled to undergo a posterior cervical fusion.2,4
Tobacco smoking has been consistently identified as a major modifiable risk factor for poor surgical outcomes due to deleterious effects on bone fusion and wound healing. Multiple systematic reviews and meta-analyses have shown that patients that smoke cigarettes have significantly lower rates of bony fusion and higher rates of pseudarthrosis after spinal fusion compared to non-smokers.5,6 In cervical spine surgery specifically, smoking has been associated with increased perioperative morbidity and higher rates of pseudarthrosis in patients who underwent anterior cervical corpectomy. 7 Hilibrand et al looked at patients undergoing multilevel anterior cervical decompression and fusion using autogenous interbody grafting and found worse clinical outcomes (pain levels, medication usage, daily activity level) in the smoking group compared to non-smokers. 8 A systematic review and meta-analysis by Nunna et al, found that smoking status carried a global risk of non-union for all spinal fusion procedures, regardless of location, number of segments fused, or grafting material. 9 Smoking has also been associated with increased rates of wound complications leading to elevated risk of infection, with the mechanism attributed to impairment in the normal phagocytic activity of neutrophils and macrophages against bacteria.7,10–14 Berman et al performed a retrospective literature review and demonstrated a clear, increased rate of perioperative complications following spinal fusion in patients who smoke at both biochemical and clinical level. 14
It is postulated that nicotine may disrupt the coupling between angiogenesis and osteogenesis needed for effective bone regeneration, and ultimately fusion. 15 Nicotine has also been shown to compromise blood perfusion via vasoconstriction, with potential major implications for subsequent arthrodesis. 16 While the overall rates of cigarette use have been declining over the last several decades, there has been a rise in non-tobacco nicotine (NTN) products, including electronic cigarette/vaping devices and nicotine pouches. 17 These products are branded by their respective companies as being safer alternatives to traditional cigarette smoking and are often continued perioperatively.18,19 There has been emerging clinical evidence in lumbar surgery that suggests that non-tobacco nicotine dependence is associated with increased perioperative and long-term complications, including pseudarthrosis and fracture risk. 16
Given the increasing prevalence of NTND and the biologic plausibility that nicotine from these products may independently affect bone healing, additional evidence is needed, particularly in the posterior cervical fusion patient populations. 17 The purpose of this study was to evaluate the association between NTN dependence (NTND) and postoperative outcomes following posterior cervical fusion, with a primary interest in pseudarthrosis rates. Overall, we hypothesized that NTND use would be associated with higher rates of pseudarthrosis and postoperative complications compared to patients without perioperative nicotine exposure.
Methods
Study Design
Institutional Review Board approval is not required for this work, as all cohorts were defined from de-identified and aggregated data. A retrospective cohort study was performed using TriNetX (2012-2025), a nationwide health outcomes research database drawing from over 100 million patients. The study aimed to provide a matched cohort analysis of outcomes following posterior cervical fusion in patients stratified by different preoperative nicotine/tobacco exposure status.
Cohort Definitions
Current Procedural Terminology (CPT) and International Classification of Diseases, Revision 10 (ICD-10) codes form the basis of terminology definitions in the TriNetX system. As a result, posterior cervical fusion was defined through TriNetX by CPT (22 614, 22 600) and corresponding ICD-10-PCS codes (0RG-(1/2)-(0/3/4)-(J/K/Z/7)-1 series). (Appendix 1). Non-tobacco nicotine dependence (NTND) cohort was defined by the presence of ICD-10 code F17.20 and the absence of tobacco dependence diagnoses (F17.22, F17.29, F17.21). This guaranteed that tobacco exposure was excluded in the NTND cohort. NTND, TD, and control cohorts were developed using previously cited methodology from database studies assessing nicotine effects on other orthopaedic procedures.20,21
The control cohort had no instance of nicotine dependence (ICD-10-CM-F17, ICD-10-CM-Z87.891), nicotine prescription (RX-NORM-7407) or tobacco abuse (ICD-10-CM-Z71.6, ICD-10-Z72.0) at any time before or up to 3 years after their index posterior cervical fusion (Appendix 1).
The NTND cohort was required to have nicotine dependence (ICD-10-CM-F17.20) but no instance of tobacco dependence (ICD-10-Z72.0, ICD-10-CM-F17.2(1/2/9)) within 3 months of their index posterior cervical fusion (Appendix 1).
The tobacco dependent (TD) cohort was required to have an instance of tobacco dependence (ICD-10-Z72.0, ICD-10-CM-F17.2(1/2/9)) within 3 months of their index posterior cervical fusion (Appendix 1).
Propensity Score Matching
Differences between unmodified cohorts (control, NTND, TD) were statistically significant on preliminary review across all demographics and several key comorbidities. As such, the cohorts were balanced using the TriNetX propensity score matching (PSM) system, which employs a 1:1 nearest neighbor matching. Patients were matched across various demographics including age at surgery, sex, race, BMI. Patients were also matched for comorbid histories including type 2 diabetes, vitamin D deficiency, and long-term steroid use. Selection of covariates for which propensity score matching was performed is cited from previous literature assessing cervical fusion outcomes in NTND and TD cohorts. 20
Given the design of the TriNetX interface, the 3 cohorts can only be compared through pairwise analysis. Therefore, 3 separate but identical 1:1 propensity score matching (PSM) analyses were performed.
Outcome Definitions
Outcomes are defined through CPT and ICD-10 codes. Outcomes were assessed within predefined time windows (eg, up to 3 years following the index event), and follow-up duration reflects real-world data availability rather than uniform longitudinal tracking. The outcomes of interest in this study include pseudarthrosis, cervical fracture, hospital readmission, emergency service use, opioid abuse, sepsis, pneumonia, and deep vein thrombosis (DVT)/pulmonary embolism (PE). The definitions for each of these outcomes are listed in Appendix 2. All outcomes assessed including pseudoarthrosis are administratively inferred based on implementation of ICD and CPT coding used by physicians during follow up period after index event. These outcomes are not radiographically confirmed nor chart-validated events and should be interpreted accordingly. Readmission codes are operationalized with inpatient billing codes, emergency use with broad CPT/HCPCS/SNOMED, and infection codes. The results of this study should be interpreted accordingly given broad use of these billing codes. Selection of outcomes codes used to define outcomes was selected according to previously published literature.20,21
Outcomes were compared in 2 timeframes, first short-term outcomes from the day of the procedure to 3 months of follow-up, and second longer-term outcomes for all instances from 1 year to 3 years postoperatively. Pseudarthrosis was only measured from 1 year to 3 years postoperatively.
Statistical Analysis
The Compare Outcomes analytic arm of TriNetX was used to perform measure of association analyses in this study. This analysis outputs the number of patients in each compared cohort who meet query criteria, the number of patients with each outcome, the risk of the outcome, the risk difference (RD) between cohorts, the risk ratio (RR) between cohorts, and the odds ratio (OR) between cohorts. 95% confidence intervals (CI) were employed for all risk ratio and odds ratio comparisons made between cohorts. A two-sided z-test of proportions is used to generate P-values for each independently analyzed outcome. A P-value <0.05 was considered statistically significant (Figure 1). Cohort Selection for Posterior Cervical Fusion Patients Stratified by Nicotine and Tobacco Exposure
Results
Control vs NTND
A total of 74,132 control and 7241 NTND patients were identified. Before matching, both cohorts had statistically different distributions of age, white/black race, male sex, vitamin D deficiency, long-term steroid use, obesity, and type 2 diabetes (P < 0.0001 for all). Propensity score matching across these same variables corrected these distributions such that all P > 0.40. The final cohort consisted of 7102 control and 7102 NTND patients. The average follow-up at 3 months was 83.1 days (control) vs 84.9 days (NTND), and at 3 years was 1.92 years (control) vs 2.16 years (NTND).
Postoperative Complications Following Posterior Cervical Fusion: Non–Tobacco Nicotine–Dependent Patients vs Controls

Bold denotes statistical significance.
Abbreviations: NTND: Non-Tobacco Nicotine Dependent, CI: Confidence Interval, DVT: Deep Vein Thrombosis, PE: Pulmonary Embolism.

Risk Ratio Forest Plot for Postoperative Complications: NTND (exposure) vs controls (reference)
Control vs TD
A total of 75,124 control and 19,347 TD patients were identified. Before matching, both cohorts had statistically different distributions of age, white/black race, male sex, vitamin D deficiency, long-term steroid use, obesity, and type 2 diabetes (all P < 0.0001). Propensity score matching across these same variables corrected these distributions such that all P > 0.15. The final cohort consisted of 19,093 control and 19,093 TD patients. The average follow-up at 3 months was 83.7 days (control) vs 84.6 days (TD) and at 3 years was 1.92 years (control) vs 1.85 years (TD).
Postoperative Complications Following Posterior Cervical Fusion: Tobacco-Dependent Patients vs Controls
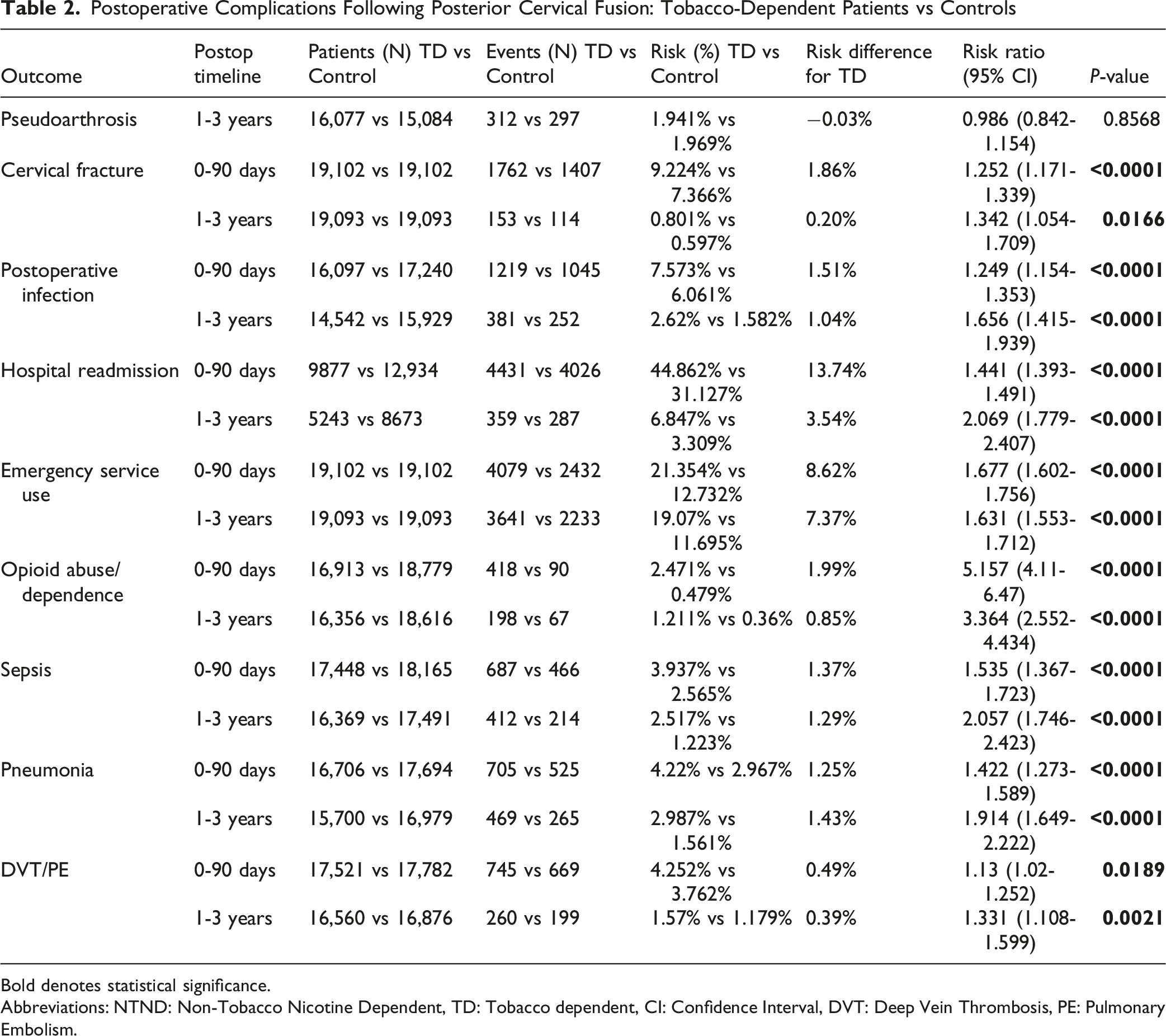
Bold denotes statistical significance.
Abbreviations: NTND: Non-Tobacco Nicotine Dependent, TD: Tobacco dependent, CI: Confidence Interval, DVT: Deep Vein Thrombosis, PE: Pulmonary Embolism.

Risk Ratios for Postoperative Complications: TD (exposure) vs controls (reference)
NTND vs TD
A total of 7298 NTND and 19,355 TD patients were identified. Before matching, both cohorts had statistically different distributions of age, male sex, vitamin D deficiency, long-term steroid use, obesity, and type 2 diabetes (all P < 0.02). Propensity score matching across these same variables and race corrected these distributions such that all P > 0.25 except white race (P > 0.09). The final cohort consisted of 7160 NTND and 7160 TD patients. The average follow-up at 3 months was 85.0 days (NTND) vs 84.1 days (TD) and at 3 years was 2.16 years (NTND) and 1.85 years (TD).
Postoperative Complications Following Posterior Cervical Fusion: Non–Tobacco Nicotine–Dependent vs Tobacco-Dependent Patients
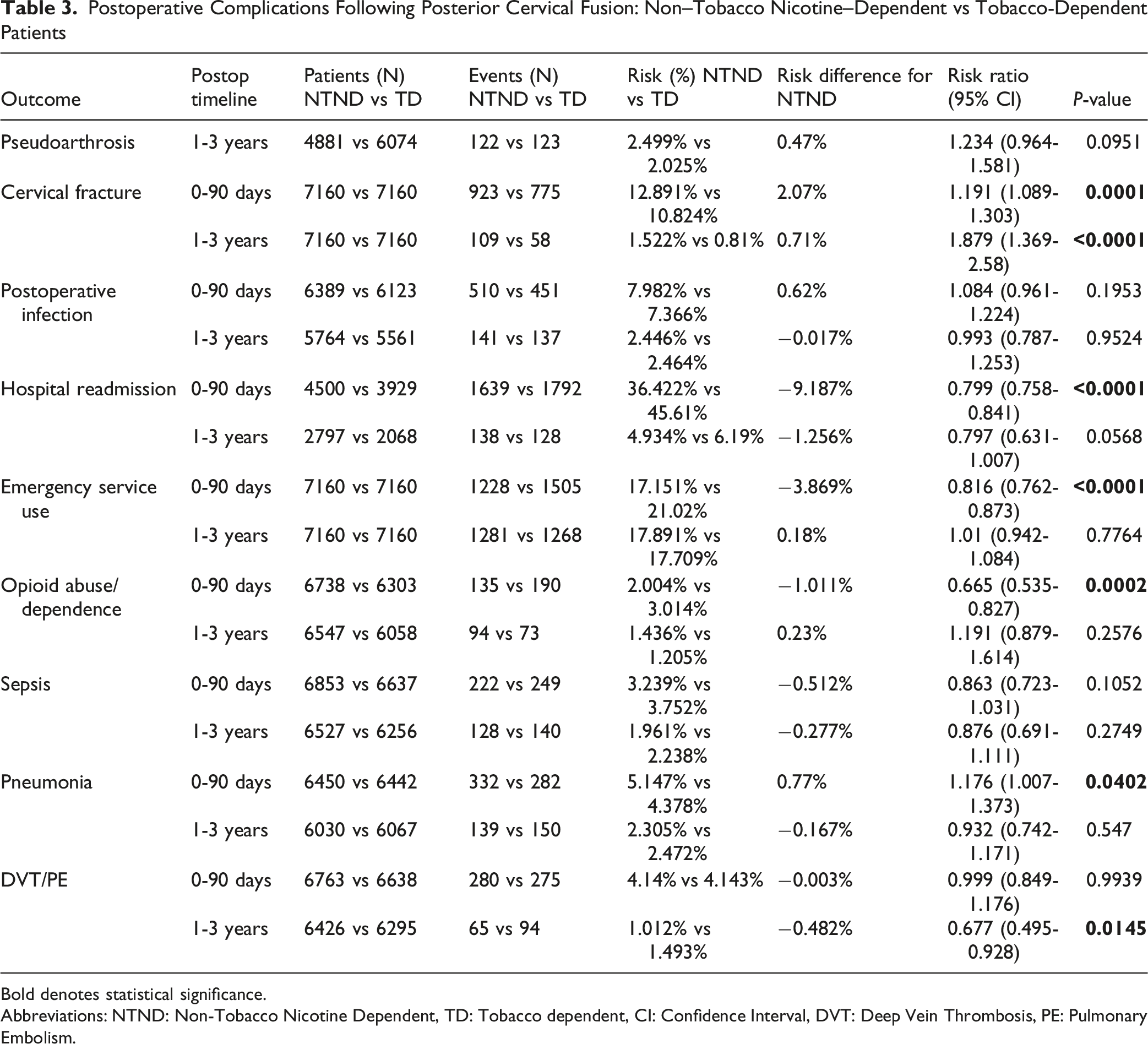
Bold denotes statistical significance.
Abbreviations: NTND: Non-Tobacco Nicotine Dependent, TD: Tobacco dependent, CI: Confidence Interval, DVT: Deep Vein Thrombosis, PE: Pulmonary Embolism.

Risk Ratios for Postoperative Complications: NTND (exposure) vs TD (reference)
Discussion
In this large, propensity-matched national database analysis utilizing the TriNetX dataset, non-tobacco nicotine dependence (NTND) was associated with a significantly increased risk of perioperative complications as well as long-term complications following posterior cervical fusion when compared to the matched control cohort. Most notably, NTND patients had higher rates of pseudarthrosis at long-term follow-up compared with matched cohorts, while conventional tobacco users had pseudarthrosis rates comparable to controls. In addition to higher pseudarthrosis rates, the NTND group had increased risks of cervical fracture, postoperative infection, postoperative hospital utilization, readmission, opioid abuse, pneumonia, and deep vein thrombosis.
The association between nicotine use and impaired bony fusion observed in this study is supported by basic science literature demonstrating adverse effects of nicotine on bone biology. Early experimental work using animal studies has shown that systemic nicotine exposure impairs bone healing by reducing osteoblast activity and compromising cells’ regenerative capacity, which results in impaired bone formation. 22 Animal studies have also looked more directly at fracture healing and osteogenesis, demonstrating nicotine decreases bone perfusion and suppresses the expression of key osteogenic mediators, including bone morphogenetic protein-2 (BMP-2) ultimately impairing new bone formation. 15 Beyond its effect on osteoblast function, nicotine appears to disrupt coordinated coupling of angiogenesis and osteogenesis which is essential to bone regeneration. Additional studies have shown that nicotine alters osteoblast and osteoclast gene expression in a dose-dependent manner, with higher levels suppressing bone-forming activity and favoring bone resorption. 23 In rabbits, transdermal nicotine exposure weakened fracture repair and led to increased rates of nonunion. 24 These studies together provided the biologic framework for the increased pseudarthrosis and fracture risk that is seen in nicotine-dependent patients, even in the absence of combustible tobacco exposure.
Although there is limited data exploring the effects of NTND in spinal fusion populations, there is a growing body of orthopaedic literature suggesting that NTND adversely affects musculoskeletal healing. In Achilles tendon repair, experimental models have shown impaired soft-tissue and tendon healing with electronic cigarette devices, specifically a significantly reduced load-to-failure and inferior biomechanical properties of the Achilles repair. 25 Ashour et al conducted a systematic review evaluating wound healing amongst patients undergoing general surgery operations that use E-cigarettes, and concluded that vaping should be stopped in the perioperative period due to greater incidence of wound healing complications. 26 In arthroplasty patient populations, a large systematic review by Zaidi et al, found electronic cigarette use was associated with impaired wound healing and increased postoperative complications, prompting the authors to recommend routine assessment of electronic cigarette use during the preoperative risk stratification. 27 While fracture-specific risk factors and patients’ comorbidities must be considered, there is consistent literature demonstrating adverse outcomes across orthopaedic subspecialties in patients with non-tobacco nicotine dependence, regardless of delivery method. These studies collectively provide important context for interpreting the increased rates of pseudarthrosis and secondary adverse outcomes observed in the present study.
Spine-specific data evaluating the impact of NTND on fusion outcomes remains limited and largely from retrospective database analyses. Early studies using national datasets demonstrated that NTND was associated with higher rates of pseudarthrosis and postoperative complications following lumbar decompression and fusion, suggesting nicotine exposure, regardless of combustible tobacco, may adversely affect the biology behind arthrodesis. 21 More recent lumbar-specific investigations have reinforced this association. Hirpara et al, investigated NTND patients that underwent anterior lumbar interbody fusion and found higher rates of pseudarthrosis, revision surgery, postoperative opioid use, emergency department visits, pneumonia, ventilator support, and sepsis compared to those without NTND. 28 These clinical findings are supported by mechanistic studies that showed that nicotine use suppresses osteogenic differentiation and bone-forming capacity, providing the biologic plausibility for impaired fusion healing in nicotine-exposed patients. 29 Cervical spine-specific evidence has also begun to emerge. Lawand et al looked at outcomes following ACDF and found NTND patients had higher rates of pseudarthrosis, revision surgery, dysphagia, adjacent segment disease, ED visits, and opioid abuse compared to non-users at mid-term follow-up. 20 These findings suggest that the adverse effects of nicotine exposure on fusion biology may persist across spinal regions and surgical approaches, even in the setting of evolving modern instrumentation.
In addition to impaired fusion, NTND in the present study was associated with increased risks of cervical fracture, opioid abuse, and several medical complications, including pneumonia, and deep vein thrombosis. The observed increase in fracture risk among NTND patients is consistent with prior orthopaedic literature demonstrating nicotine exposure adversely affects bone quality and healing, potentially increasing susceptibility to fracture.20,21 Nicotine has been shown to impair osteoblast function, inhibit angiogenesis, and promote bone resorption.30,31 The increased postoperative opioid use may reflect increased postoperative pain sensitivity, as nicotine has been shown to modulate pain perception pathways and enhance opioid reinforcement.32,33 Studies have shown that nicotine may also sensitize patients to nociceptive stimuli which could contribute to elevated pain perception postoperatively. 34 The findings in the present study suggest the impact of NTND following posterior cervical fusion extends beyond fusion success alone and encompasses a broader scope of postoperative morbidity and healthcare utilization.
An unexpected but notable finding of the present study was that NTND patients demonstrated similar rates of pseudarthrosis and several other complications compared to conventional tobacco users. While NTN products contain less additional chemicals than traditional tobacco products, the high rates of pseudoarthrosis and other complications evident in this study in patients who use these products may be related to differences in the nicotine delivery patterns and systemic exposure from NTN products. Pharmacokinetic studies have shown that electronic cigarettes and other non-combustible nicotine delivery modalities can produce sustained or higher cumulative nicotine levels compared to traditional cigarette smoking, particularly among frequent or habitual users.35,36 Unlike cigarettes, which impose natural breaks between individual doses, non-tobacco nicotine products may facilitate more continuous use throughout the day which may potentially amplify the biologic effects on bone metabolism and vascular function. 36 Behavioral factors may further contribute to this different risk profile. NTN products are often perceived as safer alternatives to cigarette smoking, and thus may be used more liberally or continued perioperatively, especially in the absence of explicit preoperative cessation counseling. As a result, NTND patients may experience ongoing nicotine exposure during the critical perioperative period where early fusion biology is occurring.
There are several potential limitations to this study. As a retrospective database study, the analysis is inherently subject to limitations of administrative coding. The study is subject to limitation including potential misclassification of NTND exposure related coding definitions, post-index selection bias in the control cohort, lack of adjustment for multiple comparisons, differential follow-up between groups, and the use of non-specific outcome measures. One cannot classify the extent of nicotine exposure, dose, duration of use, product type, or perioperative cessation behavior which limits the ability to assess a dose-response relationship. The present study employed inclusion and exclusion criteria to best limit potential misclassification of NTND, TD, and control cohorts. Radiographic confirmation of fusion status was also not feasible, so fusion status was inferred from diagnostic coding which may underestimate or overestimate the true nonunion rate. The diagnosis of pseudoarthrosis in this study relied on ICD-10 diagnostic codes without access to advanced imaging results such as CT scan, which is the most accurate imaging modality for pseudoarthrosis diagnosis (pooled OR 17.02 vs surgical exploration as the gold standard). While TriNetX captures procedure codes for imaging orders, it does not provide access to imaging results or radiologist interpretations that would allow confirmation of diagnoses according to established diagnostic criteria, and this potential misclassification bias should be considered when interpreting results. Additionally, surgical variables like construct type, number of levels, graft choice, and use of biologics could not be controlled. Finally, although propensity matching helps mitigate confounding variables, unmeasured confounders like socioeconomic factors and health behaviors may be present. Tobacco use has been shown to be disproportionately prevalent among individuals with lower socioeconomic status. These populations also face reduced access to healthcare and demonstrate lower rates of compliance which can lead to differential results when comparing those who use tobacco and NTND cohorts when compared to those who abstain. 37 Despite these limitations, the consistency of findings across multiple outcomes aligns with emerging spine-specific and general orthopaedic literature. These results underscore the need for prospective studies incorporating detailed nicotine exposure metrics, radiographic fusion assessment, and standardized perioperative cessation protocols to better delineate the true effect of NTND on posterior cervical fusion outcomes. However, this study also has several notable strengths. It represents the largest analysis to date examining the impact of non-tobacco nicotine dependence on outcomes following posterior cervical fusion. It leverages a national database to capture both perioperative patient factors and long-term outcomes data. The use of propensity score matching allowed for a balanced comparison across cohorts with respect to demographic and clinical variables. Additionally, the inclusion of long-term follow-up allowed for clinically meaningful outcomes to be compared. Future investigation should include time-to-event methods and differential follow-up adjustments which would strengthen analyses conducted in the future.
Conclusion
In this national, propensity-matched analysis, patients with non-tobacco nicotine dependence were found to have a higher risk of pseudarthrosis and an increased risk of postoperative complications after posterior cervical fusion, when compared to control cohorts. When compared to TD, NTND failed to show statistically significant difference of pseudoarthrosis, yet were observed to have higher risk of cervical fracture in the postoperative period. These findings suggest that nicotine exposure from non-combustible sources may be associated with differences in fusion outcomes and postoperative recovery. While causality cannot be established, these results highlight the potential importance of identifying non-tobacco nicotine use and targeted preoperative counseling as part of risk assessment and optimization in patients undergoing posterior cervical fusion.
Supplemental Material
Supplemental material - Non-Tobacco Nicotine is Associated with Increased Complications Following Posterior Cervical Fusion: A Retrospective Cohort Study
Supplemental material for Non-Tobacco Nicotine is Associated with Increased Complications Following Posterior Cervical Fusion: A Retrospective Cohort Study by Alec M. Giakas, MD, William A. Green, BS, MEd, Anthony Castro, BS, Eric Tecce, MD,, Mitchell K. Ng, MD, Molly Milano, BS, Yulia Lee, BA, Gregorio Baek, BS, Jonathan Dalton, MD, Grant Thomas, BS, Jarod Olson, BS, Joshua Mathew, BS, Yasmine Eichbaum, BS, Morgan Hitchner, BS, Thomas D. Cha, MD, Alan Hilibrand, MD, Alexander R. Vaccaro, MD, PhD, MBA, Christopher Kepler, MD, MBA, Gregory Schroeder, MD in Global Spine Journal.
Footnotes
ORCID iDs
Ethical Considerations
This study did not require Institutional Review Board approval as it uses publicly available datasets.
Consent to Participate
All patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Author Contributions
AG: None. WG: None. AC: None. ET: None. MN: Stryker. Inc – paid consultant, Johnson & Johnson Ethicon Inc – paid consultant, CurvaFix Inc – paid consultant, Pacira BioSciences Inc – paid consultant, Sage Products Inc – paid consultant, Alafair Biosciences Inc – paid consultant, Next Science LLC – paid consultant, Bonutti Technologies Inc – paid consultant, Hippocrates Opportunities Fund LLC – paid consultant, and Ferghana Partners Inc – paid consultant. MM: None. YL: None. GB: None. JD: None. GT: None. JO: None. JM: None. YE: None. MH: None. TDC: Globus Medical- Paid consultant, K2M- Research support, Kuros- Stock or stock Options, Nuvasive- Research support, Stryker- Paid consultant. ASH: Biomet – IP royalties, CTL America – IP royalties, Paradigm spine – stock or stock options. ARV: Receives royalties from Stryker, Globus, Medtronic, Atlas Spine, Alphatech Spine, SpineWave, Spinal Elements, Curiteva, Elsevier, Jaypee, Stout Medical, Taylor Francis/Hodder and Stoughton, Wolters Kluwer, and Wheel House Medical, and Thieme; has stock or stock options in Accelus, Advanced Spinal Intellectual Properties, Atlas, Avaz Surgical, AVKN Patient Driven Care, Cytonics, Deep Health, Dimension Orthotics LLC, Electocore, Flagship Surgical, FlowPharma, Rothman Institute and Related Properties, Globus, Harvard MedTech, Innovative Surgical Design, Jushi (Haywood), Orthobullets, Parvizi Surgical Innovation, Progressive Spinal Technologies, Sentryx, Stout Medical, See All AI, and ViewFi Health; is a consultant for Curiteva, Medcura, Stryker, Globus, Spinal Elements, Accelus, Wheel House Medical, and Ferring Pharmaceutical; Serves on Scientific Advisory Board / Board of Directors / Committee for National Spine Health Foundation (NSHF), Sentryx, and Accelus; and is a member in good standing/independent contractor for AO Spine. CKK: Clinical Spine Surgery – editorial or governing board, Inion – IP royalties, Regeneration Technologies, Inc – research support. GDS: Advance Medical – paid consultant, AOSpine – board or committee member, AOSpine – other financial or material support, Bioventus – paid consultant, Cerapedics – research support, Cervical Spine Research Society – board or committee member, DePuy, A Johnson & Johnson Company – research support, Medtronic Sofamor Danek – research support, Surgalign – paid consultant, Wolters Kluwer Health – Lippincott Williams & Wilkins – editorial or governing board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted without any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All data are publicly available through the TriNetX interface.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data are included in the manuscript draft, tables, and figures. The raw data are available publicly through the TriNetX interface.
Drug Statement
The drugs mentioned in this study is FDA-approved or approved by corresponding national agency for this indication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.