
Abstract
Study Design
Cross-sectional Survey-Based Study.
Objectives
Existing classification systems for upper cervical spine trauma lack structured guidance for clinical decision-making. While the AO Spine Upper Cervical Injury Classification (UCIC) provides a comprehensive framework, it lacks an accompanying injury score. This study aimed to develop the AO Spine Upper Cervical Injury Score (UCIS) based on global perceived injury severity scores (ISS).
Methods
Data from a global survey of 159 surgeons were analyzed. Surgeons assigned a perceived ISS (0-100) to each UCIC variable relative to the need for surgical stabilization. Median ISS values for injury morphology, neurologic status, and modifiers were translated into an integer-based scoring system.
Results
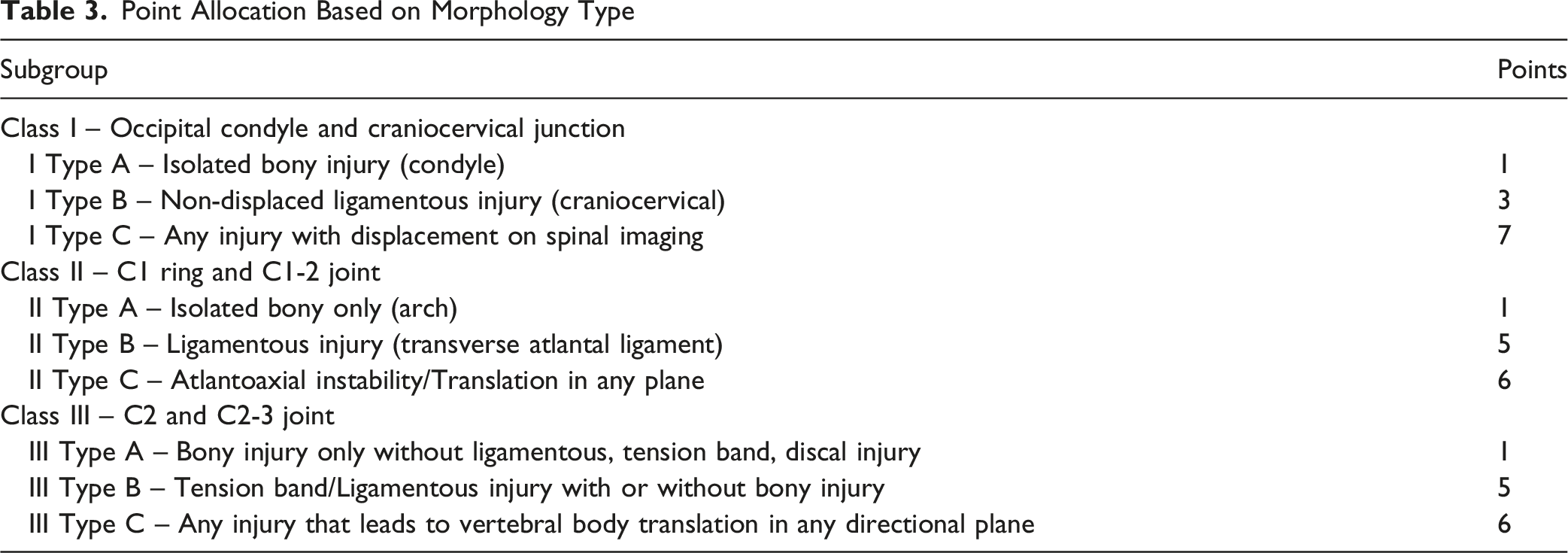
Stable Type A injuries were assigned 1 point, while unstable ligamentous and translational injuries received higher scores (eg, Type IIB = 5 points; Type IC = 7 points). For neurologic status, N0 received 0 points, N1/N2 received 1 point, and N3/4 were consolidated to 6 points. Unexamined patients (NX) were allocated 3 points. Modifiers M1 (nonunion risk) and M3 (comorbidities) were assigned 3 points (ISS 60.0), while M2 (instability received 4 points (ISS 75.0).
Conclusion
The AO Spine UCIS is a simplified scoring system that translates global consensus on injury severity to a clinically applicable score. It was built upon a foundational survey demonstrating minimal geographic or experiential variability in severity ratings. The UCIS serves as a clinically relevant tool to complement the validated AO Spine UCIC system and provides the necessary framework for the future development of a treatment algorithm for upper cervical spine injuries.
Introduction
The upper cervical spine, which extends from the occiput to the C2-3 joint, is particularly vulnerable to traumatic injury due to its distinct biomechanical properties, which allow greater mobility.1,2 Additionally, injuries to the upper cervical spine can be life-threatening, necessitating prompt identification and management.2–4 However, the currently available classification systems for injuries to the upper cervical spine are largely descriptive in nature and lack clinical utility.5–12 For example, while the Anderson and D’Alonzo classification for odontoid fractures is useful for efficient communication about fracture patterns and can broadly guide operative vs nonoperative management for odontoid process injuries, there is still substantial controversy regarding the treatment of odontoid waist (Anderson and D’Alonzo Type 2) fractures. 10 Additionally, many of the well-studied classification systems for the upper cervical spine are anatomically limited to a single level or region. Consequently, treatment decisions for injury to the upper cervical spine are often based on individual surgeon experience rather than evidence or consensus-based algorithms.
To address these shortcomings, the AO Spine developed the AO Spine Upper Cervical Injury Classification (UCIC) system. 13 This is the first comprehensive system to incorporate all injuries from the occiput to C2-3 into a single, cohesive classification. The system classifies injuries based on anatomic location (I, II, or III), injury type (A, B, or C), neurologic status, and case-specific modifiers. 13 The UCIC system has been globally validated and shown to be an accurate and reproducible tool. In a multi-center validation study, the UCIC system demonstrated greater than 80% accuracy for injury classification as well as “substantial” overall interobserver reliability (k = 0.729) and “excellent” intraobserver reproducibility (k = 0.82). 13 While the demonstrated reliability of the UCIC system is an important first step, the classification system alone is insufficient to guide practice management. The logical next step, following the precedent of the AO Spine Thoracolumbar and Subaxial Cervical classification systems, is to establish an injury score to accompany the UCIC system and guide treatment.14,15
To this end, we recently published a global validation study establishing that the hierarchical nature of the UCIC is consistent across all geographic regions and experience levels.1 The current study represents the essential next step in this research, translating those validated severity ratings into a simplified, integer-based AO Spine Upper Cervical Injury Score (UCIS) to accompany the classification and serve as a practical tool for the global surgical community. The specific surgical thresholds that dictate which injury score warrants operative management will be established in a future study.
Methods
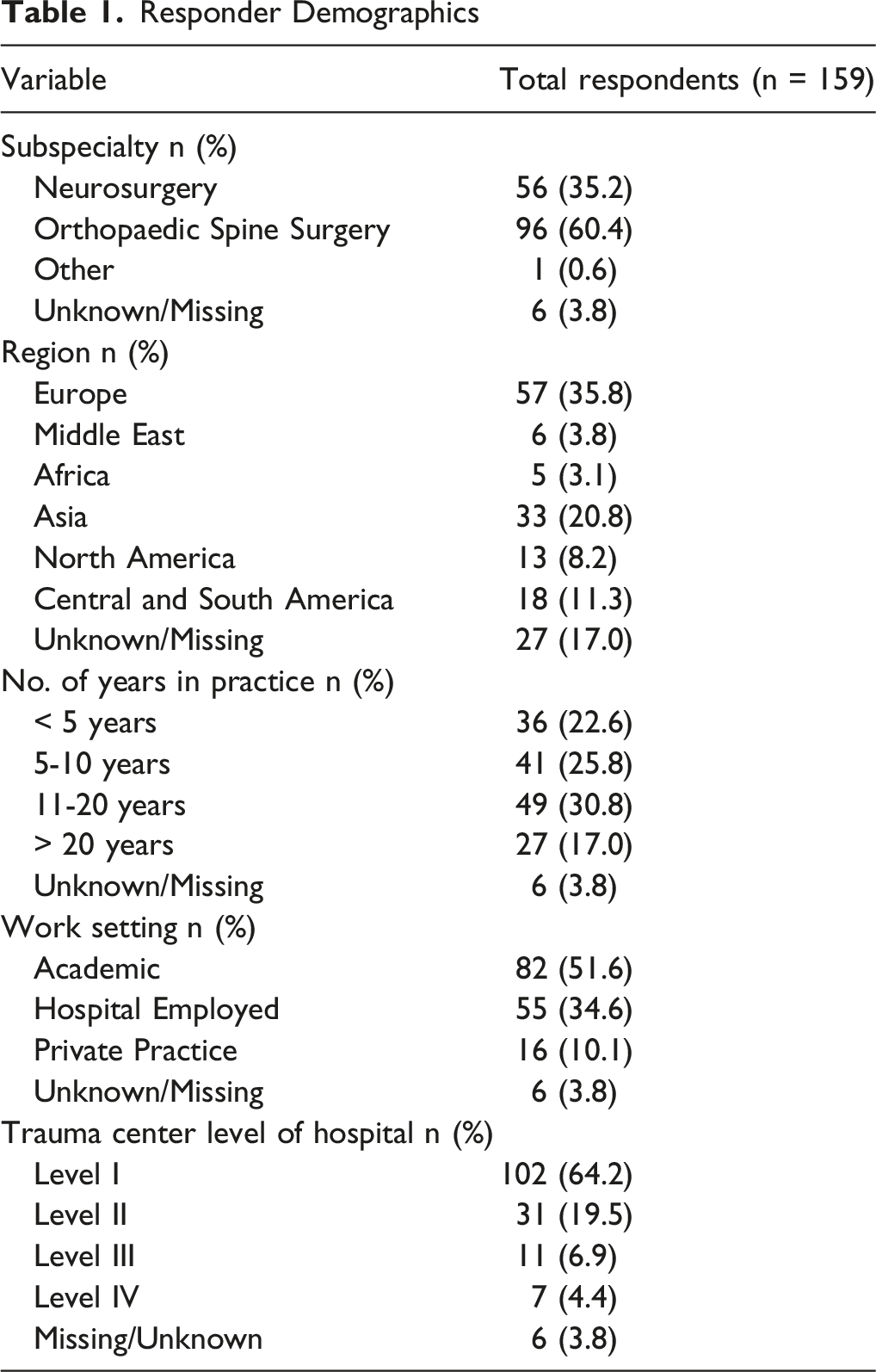
The AO Spine Upper Cervical Injury Classification (UCIC) system was developed by a consensus of spine surgeons through a previously described process. 1 To establish the clinical validity of the system’s hierarchy, a survey was previously distributed to the members of the AO Spine Cervical Classification Validation Group, composed of spine surgeons from six different regions (Europe, the Middle East, Africa, Asia, North America, and Central and South America). For each variable in the UCIC system, respondents were asked to assign a numerical severity grading from 0 (minimal severity) to 100 (highest severity), relative to the need for surgical stabilization. Survey responses with at least one valid answer were included in the final analysis. The complete methodology, respondent demographics, and detailed results of the survey have been published previously. 1
An analysis of the collected survey results was used to develop a simplified injury score. The median injury severity score (ISS) for each subgroup of the classification system was determined by subgroup and added into an integer-based point system. Non-integer values were avoided as they would be impractical for clinical use. Additionally, it is important to note that the M4 modifier was not assigned a point value, as vascular injury typically does not factor into decision-making for surgical stabilization of the spinal column and is therefore not applicable to this injury scoring system.
Results
Responder Demographics
Median Injury Severity Score for Each Variable in AO Spine Upper Cervical Injury Classification System

Point Allocation Based on Morphology Type
Point Allocation Based on Neurologic Status and Modifiers
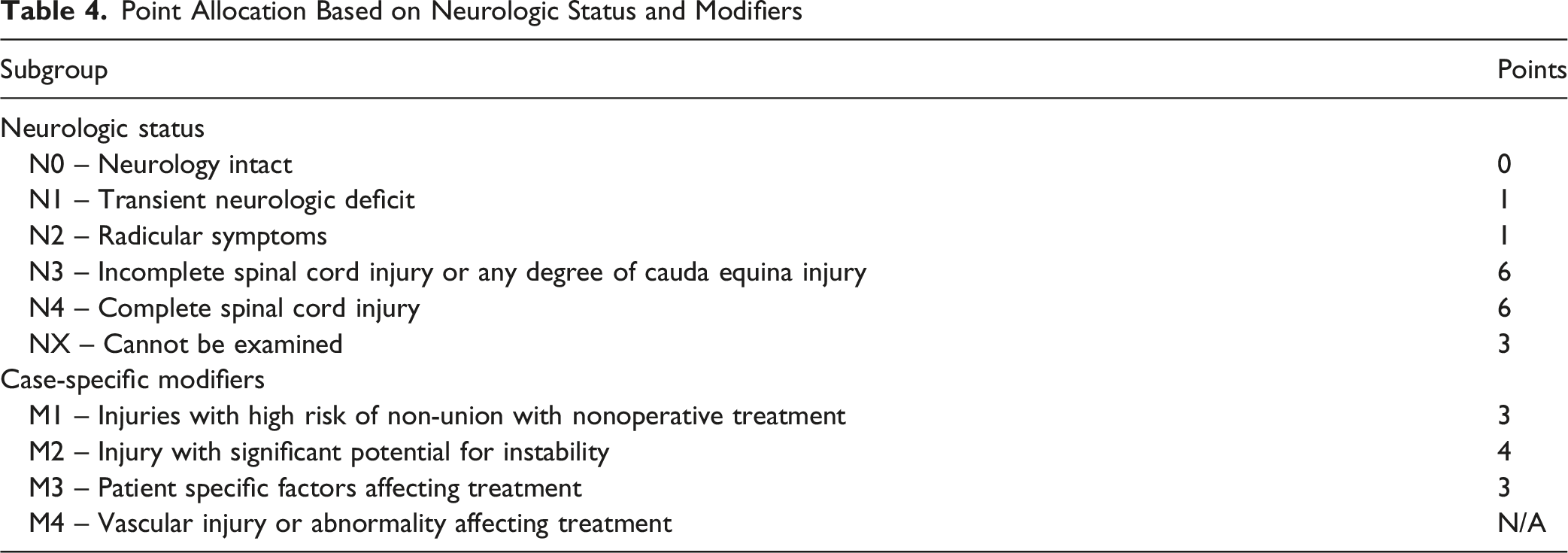
The scoring system for case-specific modifiers can be seen in Table 4. While the modifiers representing secondary clinical challenges, such as high risk of nonunion (M1) and patient-specific comorbidities (M3), each had an assignment identical to perceived severity ratings (Median ISS 60.0), M1 was awarded 3 points while M3 was awarded zero. Although the ISS reflects perceived clinical importance, point allocation within the UCIS was intentionally designed to reflect the directional influence of each modifier on the likelihood of surgical stabilization. This is because the patient-specific modifiers may either push a surgeon towards surgery, or away from surgery. The M2 modifier, which indicates potential for future instability, received an injury score of 4. This higher value emphasizes instability as a key factor necessitating surgical intervention and is corroborated by its high perceived severity rating (Median ISS 75.0). This is because patient-specific modifiers such as M3 may either push a surgeon toward surgery or, appropriately discourage operative management, and therefore were not assigned additive points to avoid inflating injury severity. Finally, the M4 modifier (vascular injury) was not assigned a score as it does not apply to this scoring algorithm and does not influence the surgical decision-making process for upper cervical spine injuries (Table 4).
Discussion
The AO Spine UCIC system provides a reliable, consensus-based framework for categorizing injuries to the occiput, C1, and C2.1,13 While the descriptive subtypes of the UCIC system address the shortcomings of previous classification systems, it cannot work in isolation to standardize treatment or guide clinical decision-making.5–12 Thus, similar to previous AO Spine classification systems, the UCIC system needed an accompanying integer-based scoring system in order to guide treatment.14,15 To this end, the AO Spine Cervical Classification Validation Group analyzed the perceived injury severity data to develop the AO Spine UCIS, a simplified point system designed to serve as the foundation for a treatment algorithm. 1
While the UCIS is derived from the relative injury severity ratings assigned by the survey respondents, the exact injury score designation was determined by the author group. As such, in situations where the severity ratings did not clearly translate into a relative score, clinical reasoning was applied. For example, for an NX (unexaminable) patient, survey respondents assigned this a neurologic status with a high median ISS of 80.0, which is higher than the rating for a Type IIB (72.5) or Type IIIB (70.0) injury. A direct translation would have resulted in a score of 5 or 6 points. However, the decision was made to assign a score of 3. This clinical judgement, which deviates from the raw ISS data, follows the precedent of prior AO Spine scoring systems.14,15 The reasoning for this intermediate score is to cautiously avoid the assumption that the patient is neurologically intact, rather than to treat the “unexaminable” status as an injury equivalent to a complete spinal cord injury (a 6-point score). As noted in prior AO injury score studies, an unexaminable patient is frequently a polytrauma case in need of prompt stabilization, and this 3-point score ensures that the high-risk, unknown neurologic status contributes appropriately to the overall injury severity.14,15 Additionally, clinical reasoning was also used to group injury scores. For instance, N3 (incomplete) and N4 (complete) spinal cord injuries received different median ISS ratings (87.5 vs 100.0, respectively), but the decision was made to assign them the same score of 6 points. This reflects the clinical consensus that both N3 and N4 represent the most severe category of neurologic injury, warranting the same maximal point allocation. A similar logic was applied to Type IA, IIA, and IIIA injuries, which were all grouped at 1 point despite different median ISS ratings (20.0, 25.0, and 30.0, respectively) to represent a single clinical category of “stable bony injury”.
The injury severity ratings used to generate the UCIS were derived from a survey of 159 surgeons across six continents. A key finding from the initial validation study was the high degree of consensus regarding the hierarchical nature of the classification. 1 Despite diverse geographic and practice backgrounds, surgeons demonstrated substantial agreement on the relative severity of these injuries. 1 This strong consensus on the score’s values is built upon the reliability of the classification system itself. The UCIC system previously demonstrated “substantial” interobserver reliability (k = 0.729) and “excellent” intraobserver reproducibility (k = 0.82) in a multi-center validation study. 13 Moreover, because the underlying classification was designed to serve as a universal tool that relies on accessible CT imaging rather than MRI, it is expected that its accompanying scoring system, the UCIS, will also achieve widespread adoption.24,25
The UCIS, as established in this study, provides immediate clinical utility by standardizing the language of injury severity. While the specific operative threshold needs further validation through subsequent prospective follow-up study, surgeons can use the UCIS now to categorize injuries based on expert-derived severity. For example, a low total score (UCIS <3) suggests a high global consensus for stability, whereas a high score (UCIS >7) alerts the surgeon to a pattern that 159 global experts identified as having maximum severity. This allows for more objective multi-disciplinary discussions and more accurate triaging in the trauma setting. The generation of a management algorithm however, will require a subsequent global consensus process, similar to the methodology employed in establishing the initial injury severity ratings. 1 This step is crucial to addressing the current variations in treatment that exist for upper cervical spine injuries. The proposed recommendations must also be adaptable to a global context, accounting for potential differences in resource availability across diverse practice environments.14,15 While the treatment algorithm would initially be based on this expert consensus, it would provide the necessary framework to guide future, high-level prospective studies. Rather than viewing the validation of the classification and the creation of the score as a single oversized report, we have intentionally separated them to provide a rigorous, evidence-based progression. The first study established that the hierarchy exists, while this study establishes how to measure it. This stepwise approach follows the established and successful methodology used for both the AO Spine Thoracolumbar and Subaxial Cervical Injury Scores.
The current study is not without limitations. First, the development of the current injury scoring system was based on expert consensus, rather than high-level prospective evidence. However, in the context of severe, unstable upper cervical spine trauma, conducting randomized controlled trials is often unethical. As such, a consensus from a global group of experts offers the most reliable data. This approach follows the precedent of other widely accepted medical scoring systems that were founded upon expert opinion.26–28 Second, the specific expertise of the responding surgeons in upper cervical trauma was not formally evaluated. As such, it is possible that surgeons with limited experience or knowledge could have filled out the survey. This is mitigated, however, by the sample size, which should diminish the impact of outliers. Third, the geographic regions of the responding surgeons were not evenly distributed. For example, North America, Africa, and the Middle East were underrepresented compared to Europe. This may have introduced bias to the global consensus. Finally, the severity ratings were based on the surgeons’ perception of severity, not on prospective clinical outcomes. Thus, future prospective studies should be conducted to further validate the accuracy of the UCIS and to establish and test specific surgical thresholds.
Conclusion
The AO Spine Upper Cervical Injury Score (UCIS) proposed in this article represents a simplified, integer-based system that effectively translates the perceived injury severity ratings into a clinically practical score. This score was built upon a global survey of 159 spine surgeons, which demonstrated a distinct hierarchical progression of injury severity across all three anatomical regions of the upper cervical spine. Additionally, the survey revealed minimal geographic or experiential variability in the underlying severity ratings for each UCIC subgroup. Thus, the UCIS serves as a clinically relevant tool to complement the UCIC system, which has previously demonstrated high reliability and reproducibility. These results suggest that the AO Spine UCIC system, combined with the outlined scoring system, offers a framework for the development of a universally accepted treatment algorithm for upper cervical spine injuries.
Footnotes
Author Note
AO Spine Upper Cervical Classification International Validation Members: Adesh Shrivastava at AIIMS Bhopal, Christian Konrads at University of Tuebingen, ALQROOM RAMI, BhavukGarg at All India Institute of Medical Sciences, Vishal Borse at Leeds General Infirmary, Sebastian F Bigdon at Inselspital, Triki Mohamed Amine at Université de Sousse, Riaz Mohammed at UHW Cardiff, Omar Marroquin H. at Hospital Universitario Fundación Santa Fe de Bogotá, Komal Prasad Chandrachari at Narayana Health, Banerjee Purnajyoti, Parmenion P. Tsitsopoulos at Aristotle University of Thessaloniki, Palaniandy Kamalanathan, Stefano Carnesecchi at Azienda Ospedaliero-Universitaria Pisana, Konstantinos Margetis at Icahn School of Medicine at Mount Sinai, Mutaleeb SHOBODE at National Orthopaedic hospital dala kano Nigeria, Adetunji National Orthopaedic Hospital Toluse Lagos Nigeria, Amanda O'Halloran at Cork University Hospital, Jin Wee Tee at Department of Neurosurgery, The Alfred Hospital, Melbourne, Victoria, Australia, Ron Tamy at Universidad Nacional, Elgafy Hossein, Matias Pereira Duarte at Université de Montréal, Vishal Kumar at PGIMER, Chandigarh, India, Nanfang Xu at Peking University Third Hospital, Selim Ayhan at Baskent University, Máximo-Alberto Diez-Ulloa, Sarvdeep Dhatt at PGIMER, Waeel Hamouda at Cairo University, Eugene Park at Kyungpook National University, Nimrod Rahamimov at Galilee Medical Center, Michal Ziga at Cantonal Hospital St. Gallen, Jeronimo Milano at Neurologica Institute of Curitiba, Giorgio Lofrese at Bufalini Hospital – Cesena, Fon-Yih Tsuang, Sathish Muthu at Government Medical College Hospital, Anthony Guanciale at University of Cincinnati, Claudio Bernucci at ASST Papa Giovanni XXIII, Rian Souza Vieira at RRSV, Sokol Trungu at Sapienza University of Rome, Oliver Riesenbeck at University of Muenster, Ulrich Spiegl at University of Leipzig, Joost Rutges at Erasmus MC Rotterdam, Oke Obadaseraye at National Orthopaedic Hospital Enugu, Miltiadis Georgiopoulos at McGill University, Christina Cheng at University Hospitals Cleveland Medical Center, Loya Vijay Kumar at MIOT International, Dewan Asif at Anwer khan modern medical college, Fernando Gonzalez at Hospital Nacional Prof. A. Posadas, Annika Heuer at University Medical Campus Hamburg-Eppendorf, Hany Gendy at Zentralklinik Bad Berka Germany, Juan Muñoz at Universidad Militar Nueva Granada, Natalia Frade-Porto at Complejo Asistencial Universitario de León, Alberto Balestrino at IRCCS Ospedale Policlinico San Martino, Andreas K Demetriades at Royal Infirmary Edinburgh, Mlyavykh Sergey at Privolzhsky Research Medical University, Rakesh Kumar, Banerjee Somok, Andrea Redaelli, Eduardo Laos at Hospital Almenara, Marc Nieuwenhuijse at Amphia Hospital, Nicola Montemurro at Azienda Ospedaliera Universitaria Pisana, Takahiro Sunami at University of Tsukuba, Fady Sedra at Royal London Hospital, Konstantinos Paterakis at University of Thessaly, Slavisa Zagorac at University Clinical Center of Serbia, Daipayan Guha at McMaster University, Georg Osterhoff at University Hospital Leipzig, Anas Dyab at Centre hospitalier de Luxembourg, Martin M. Estefan Nottingham University Hospital, Bharat Dave, Jose Carlos Rodrigues Jr. at Heliopolis Hospital, Norah Foster at Miami Valley Hospital/Wright State University, Ratko Yurac at Clínica Alemana de Santiago, Tommi Korhonen at Oulu University Hospital, Baris Saygili at GVM Spitali Villa Maria Tirana, Naresh Kumar at National University Health System, Petr Vachata at J. E. Purkyně University, Tejeda Martin at Universidad Durango Santander, Sung-Joo Yuh, Amit K Bhandutia at Louisiana State University Health Sciences Center, John P Kleimeyer at Stanford University, Alexander Durst at University of Alberta, Federico Sartor at Hospital Argerich, Joost Dejaegher at KU Leuven University, Gerardo F Zambito-Brondo at Hospital Angeles de las Lomas, Bernhard W. Ullrich at Bergmannstrost, Yuki Fujioka at Higashihiroshima Medical Center, Balgopal Karmacharya at Manipal Teaching Hospital, Edward DelSole at Geisinger Musculoskeletal Institute, Koroush Kabir at University Hospital Bonn, Fernando Melo Filho at BP Campinas, Eugen Cezar Popescu at Clinical Hospital “Prof. N. Oblu” Iasi, Daniel Cruz at Teknon Medical Center Barcelona, Gyanendra Shah at National Academy Medical Sciences, Subbiah Jayakumar at Devadoss Multi-speciality Hospital, Vaibhav Jain at Gandhi Medical College, Govind Gurumoorthy Prabakaran, William Neway at Broward Health Medical Center, Siegmund Lang at University Hospital of Regensburg, Gustavo Uriza Sinisterra at Clínica Universidad de la Sabana Colombia, Dave AG Dizon at University of the Philippines, Nishanth Ampar, Ahmed Fouad Dawoud at WestBay Medicare, Narayan T V Krishna at MIOT Hospital, René Schmidt at AFK Göppingen, Susana Núñez Pereira, Amin Henine at C.O.A Department Douera University Hospital Centre Algiers Medical School of Blida 1 (![]() ) Algeria, Zhi Wang, Hisco Robijn at Regional Hospital of Tienen, Kai Sprengel, Mubder Mohammed Saeed at University of Basrah College of Medicine, Luís Marques at Egas Moniz Hospital, Emiliano Vialle at Cajurú Hospital, Ahmad Arieff Atan at Hospital Tuanku Ja'afar Seremban, Alarcon Olger Rebagliati Martins, Philippe Bancel at Clinique Arago, Héctor Aceituno, Faizan Mohammed at NKPSIMS Nagpur, Wui Ng Bing, Mario Ganau at Oxford University Hospitals NHS Foundation Trust, Mauro Medina at Hospital San Luis, Aithala P Janardhana at University of Yenepoya, Omar Marroquin at Hospital Universitario Fundación Santa Fe de Bogotá, Luis María Romero Muñoz, Ajiboye Lukman Olalekan at Usmanu Danfodiyo University Teaching hospital Sokoto, Gupta Anuj at Max Superspeciality Hospital, Alejandro Castillo at Hospital Nacional Alberto Sabogal, Himanshu Shekhar at Ninewells Hospital and Medical School, Wiktor Urbanski at Wroclaw Medical University, Devi Prakash Tokala at Grange University Hospital, Yasunori Sorimachi at Japanese Red Cross Maebashi Hospital, Triantafyllos Bouras at Centre Hospitalier de Wallonie-Picarde, Christian W. Müller at Asklepios Klinik Wandsbek Hamburg, Juan Lourido at TTH Hospital, Khoh Phaik Shan at Sultanah Bahiyah Hospital, Tripathi Manjul, Nasser Khan at Hamad Medical Corporation, Stavros I Stavridis at “St Luke's” Hospital Thessaloniki, Catalin Majer at Neuro Spinal Hospital, Paulo Pereira at Centro Hospitalar Universitário São João, Christian Hohaus at Staedt. Klinikum Dessau, Mahmoud Alkharsawi at Tanta University Egypt, Madhivanan Karthigeyan at PGIMER, Alessandro Ramieri, Satyashiva Munjal at ABVIMS and Dr RML hospital, Fernando Gomez at Clinica Lider.
) Algeria, Zhi Wang, Hisco Robijn at Regional Hospital of Tienen, Kai Sprengel, Mubder Mohammed Saeed at University of Basrah College of Medicine, Luís Marques at Egas Moniz Hospital, Emiliano Vialle at Cajurú Hospital, Ahmad Arieff Atan at Hospital Tuanku Ja'afar Seremban, Alarcon Olger Rebagliati Martins, Philippe Bancel at Clinique Arago, Héctor Aceituno, Faizan Mohammed at NKPSIMS Nagpur, Wui Ng Bing, Mario Ganau at Oxford University Hospitals NHS Foundation Trust, Mauro Medina at Hospital San Luis, Aithala P Janardhana at University of Yenepoya, Omar Marroquin at Hospital Universitario Fundación Santa Fe de Bogotá, Luis María Romero Muñoz, Ajiboye Lukman Olalekan at Usmanu Danfodiyo University Teaching hospital Sokoto, Gupta Anuj at Max Superspeciality Hospital, Alejandro Castillo at Hospital Nacional Alberto Sabogal, Himanshu Shekhar at Ninewells Hospital and Medical School, Wiktor Urbanski at Wroclaw Medical University, Devi Prakash Tokala at Grange University Hospital, Yasunori Sorimachi at Japanese Red Cross Maebashi Hospital, Triantafyllos Bouras at Centre Hospitalier de Wallonie-Picarde, Christian W. Müller at Asklepios Klinik Wandsbek Hamburg, Juan Lourido at TTH Hospital, Khoh Phaik Shan at Sultanah Bahiyah Hospital, Tripathi Manjul, Nasser Khan at Hamad Medical Corporation, Stavros I Stavridis at “St Luke's” Hospital Thessaloniki, Catalin Majer at Neuro Spinal Hospital, Paulo Pereira at Centro Hospitalar Universitário São João, Christian Hohaus at Staedt. Klinikum Dessau, Mahmoud Alkharsawi at Tanta University Egypt, Madhivanan Karthigeyan at PGIMER, Alessandro Ramieri, Satyashiva Munjal at ABVIMS and Dr RML hospital, Fernando Gomez at Clinica Lider.
Ethical Considerations
Institutional Review Board approval was not required for this study, as it involved a voluntary, anonymous survey of medical professionals regarding perceived injury severity and did not involve the participation of human patients or the use of private medical records.
Consent to Participate
Informed consent was not required for this study as it did not involve human subjects in a clinical or experimental setting. The study analyzed anonymous, perceived injury severity ratings provided by medical professionals regarding established injury classifications.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma & Infection, a focused group of international experts. AO Spine is a clinical specialty of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Innovation Translation Center, Network Clinical Research and Clinical Evidence.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.