
Abstract
Study Design
Retrospective cohort study.
Objectives
To investigate sagittal profiles including sagittal shape and alignment in relation to proximal junctional kyphosis (PJK) following deformity correction in patients with adolescent idiopathic scoliosis (AIS).
Methods
A total of 282 AIS patients who underwent deformity correction were categorized into 2 groups according to the presence of PJK at the 2-year follow-up: the PJK group (n = 48) and the non-PJK group (n = 234). Sagittal shape was classified as normal thoracic kyphosis (TK), hypo-TK with/without thoracolumbar kyphosis (TLK), and cervico-thoracic kyphosis. Changes in Roussouly classification and correction relative to the functional T10 pelvic angle target were assessed to evaluate sagittal restoration and its association with PJK.
Results
The upper instrumented vertebra (UIV) level differed significantly between the 2 groups (P = 0.002). The mean absolute Δ sagittal vertical axis (SVA) was also greater in the PJK group (P = 0.008). Regarding sagittal shape, the PJK group was most prevalent in normal TK (43.8%) and cervico-thoracic kyphosis (31.3%), whereas the non-PJK group was most prevalent in hypo-TK without TLK (40.2%) (P < 0.001). Multivariate logistic regression showed that lower UIV level, cervico-thoracic kyphosis, and greater ΔSVA were significantly associated with PJK.
Conclusions
UIV level, cervicothoracic kyphotic profile, and greater changes in the SVA were the contributing factors of development of radiographic PJK. In contrast to adult spinal deformity, PJK in AIS rarely causes serious clinical sequelae but instead represents reciprocal changes driven by the original sagittal shape and subsequent alterations in sagittal alignment.
Keywords
Introduction
Surgical decision-making in adolescent idiopathic scoliosis (AIS) has traditionally been guided by the degree of coronal curvature and its progression, which are closely related to truncal imbalance and poor self-perception.1,2 In contrast, adult spinal deformity (ASD) is primarily driven by sagittal decompensation, which is mainly caused by the loss of lumbar lordosis (LL). 3 The main goal of corrective surgery in AIS is to achieve sufficient coronal correction while minimizing residual deformity and safely rebalancing the trunk, whereas ASD surgery focuses on restoring sagittal harmony to resolve global decompensation.1,3 Meanwhile, mechanical failure is one of the important postoperative complications in ASD surgery, and it has been shown to be associated with various factors, including preoperative sagittal parameters. 4
Proximal junctional kyphosis (PJK) is one of the most common mechanical failures in ASD, with an incidence of approximately 20%–40%.3,4 In addition, proximal junctional failure (PJF), which shows a variable incidence of 11.5%–23.7%, represents a catastrophic complication that can lead to neurological deficits, the need for revision surgery, and a poor health-related quality of life. 4 Among various factors, radiological parameters have been most widely established, including the upper instrumented vertebral (UIV) level and several sagittal modifiers such as pelvic incidence (PI)–LL mismatch, lumbar morphology, distribution index, and functional alignment.3,5–7 Furthermore, recent advances in the understanding of spinal shape have highlighted the importance of global alignment and thoracic kyphosis (TK), suggesting that the spinal shape plays a crucial role in the development of PJK following deformity correction in ASD.8–11
In AIS, sagittal imbalance has also been shown to contribute to the progression of the scoliotic curve. In particular, relative anterior spinal overgrowth alters the spinal shape and has a significant impact on TK and rotational instability. 1 Recent studies have emphasized the importance of restoring TK and achieving a balanced sagittal profile to achieve satisfactory long-term outcomes. 12 Although AIS presents a distinct spinal shape compared to normal spines, efforts to interpret PJK from this perspective remain limited. 1
While PJK has been shown to be closely related to spinal shape and sagittal alignment, including PI–LL mismatch, TK, Roussouly classification, and functional alignment, little is known about how these parameters differ in AIS and how they influence the development of PJK. Therefore, this study aimed to investigate sagittal profiles–including sagittal shape and alignment–in relation to PJK following deformity correction in AIS, and to interpret the clinical significance of PJK manifested as a reciprocal change after corrective surgery.
Methods
This retrospective cohort study was conducted at a single center in accordance with the current guidelines of Strengthening the Reporting of Observational Studies in Epidemiology and strictly followed the ethical guidelines of the Declaration of Helsinki. 13 The concept and procedures for this study were approved from the Institutional Review Board of our hospital (IRB number: 2026GR0008).
Patients and Surgical Technique
We initially reviewed 386 patients with AIS who underwent deformity correction between March 1, 2015, and February 28, 2023. Inclusion criteria were (1) AIS patients aged 10-18 years and (2) those who underwent deformity correction using rod derotation with pedicle screw instrumentation through a posterior approach. Exclusion criteria were (1) follow-up of less than 2 years, (2) incomplete medical records, (3) history of previous spinal surgery or infection, and (4) non-idiopathic spinal pathology. A total of 282 patients were finally included.
Posterior spinal fusion following pedicle screw instrumentation and rod derotation was performed in all included patients. Regarding the instrumentation system, poly-axial pedicle screws were utilized at the all functional segments, including UIV; no proximal hook were used. After pedicle screw insertion, the rods (titanium alloy) were inserted in the cephalad-to-caudal direction. The rod on the concave side was contoured to exaggerate the normal sagittal alignment by approximately one-third, and the convex rod was contoured accordingly. Furthermore, standard surgical procedures were followed to minimize proximal junctional stress, including the preservation of the posterior ligaments at the UIV and UIV+1 levels as much as surgically feasible.
The UIV selection was determined by Lenke classification, structural characteristics of proximal thoracic curve, radiographic shoulder balance, and the sagittal profiles. Specifically, PT (particularly, T2) was selected as the UIV when the proximal thoracic curve was structural (Lenke types 2 and 4) and/or when the left shoulder was preoperatively elevated. For patients with non-structural proximal thoracic curves but structural main thoracic curves (Lenke types 1, 3, and 6) who presented a level or higher right shoulder, the UIV was selected at the upper thoracic (UT, particularly T3 or T4) levels. In contrast, for patients with Lenke type 5 curves, a selective thoracolumbar/lumbar fusion was performed, typically selecting the UIV level at mid-thoracic region (MT, T7-T9) based on the magnitude of thoracic curve in order to optimize shoulder balance.
Group Allocation Based on the PJK
Included patients were categorized into 2 groups based on the presence of PJK: the PJK group (n = 48) and the non-PJK group (n = 234) (Figure 1). PJK was defined as a proximal junctional angle (PJA) ≥ 10° at the 2-year follow-up or an increase of at least 10° compared with the preoperative measurement.
14
The PJA was measured as the sagittal Cobb angle between the superior endplates of the UIV and UIV+2. In addition, severe PJK was recorded when the PJA was ≥28°, and PJF was defined as any case requiring revision surgery due to mechanical failure at the proximal junctional level.
15
A study flowchart. AIS, adolescent idiopathic scoliosis; PJK, proximal junctional kyphosis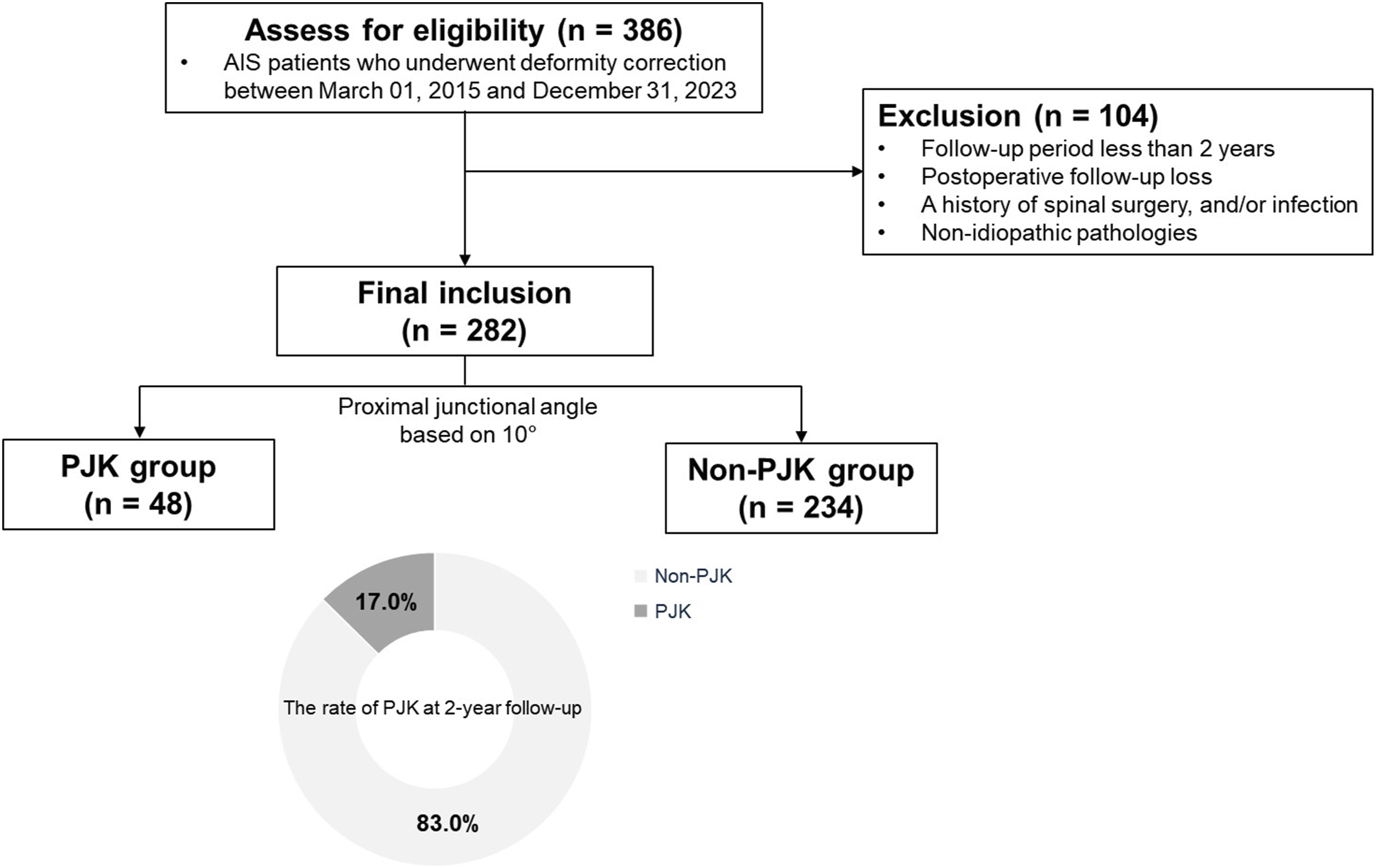
Data Collection and Radiological Analysis
Baseline characteristics included age, sex, and body mass index (BMI), Lenke classification, number of fused segments, UIV level, and the lowest instrumented vertebra (LIV) level. The UIV level was categorized as proximal thoracic (PT, T1 and T2), upper thoracic (UT, T3–T6), and mid-thoracic (MT, T7–T9) regions, whereas the LIV level was classified as thoracolumbar (T11–L1) or lumbar (L2–L5) regions. 16 Radiological parameters were measured on whole spine anteroposterior and lateral radiographs captured preoperatively, at 6 weeks postoperatively, and at the 2-year follow-up. Coronal parameters included the Main Cobb’s angle, and coronal balance (CB). Sagittal and spinopelvic parameters included sagittal vertical axis (SVA), TK, LL, PI, sacral slope (SS), and pelvic tilt (PT). The PJA was evaluated at both 2-year follow-up and the most recent follow-up to assess the progression of PJK beyond 2 years.
Regarding the sagittal alignment correction, the T10-pelvic angle (T10PA) were measured to assess the functional alignment. Based on the functional alignment target for T10PA in patients aged <35 years, the T10PA correction was categorized as overcorrection (>+3.5°), functionally corrected (within ±3.5°), or undercorrection (<−3.5°). 7 Additionally, the PI–LL mismatch as a sagittal modifier in the Scoliosis Research Society–Schwab classification was recorded as 0 (<10°), + (10° ≤ value <20°), and ++ (≥20°). 3 Regarding spinal shape in sagittal alignment, the sagittal classification proposed by Abelin-Genevois et al for AIS was adopted: type 1 (normal TK), type 2a (hypo-TK without thoracolumbar kyphosis), type 2b (hypo-TK with thoracolumbar kyphosis), and type 3 (cervicothoracic kyphosis). 17 The Roussouly classification was also assessed and proper restoration was evaluated based on changes in Roussouly types between postoperative and 2-year follow-up radiographs.5,18 In addition, changes in sagittal balance defined as a shift in SVA from a negative to a positive value or vice versa and ΔSVA were analyzed between the postoperative and 2-year follow-up.
Statistical Analysis
Statistical analyses were performed using Python (version 3.11.5; Python Software Foundation, Wilmington, DE, USA) with the matplotlib package (version 3.7.2). The normality of data distribution was assessed using the Kolmogorov–Smirnov test. After confirming data homogeneity or heteroscedasticity, the Student’s t-test was applied for continuous variables, which were expressed as mean ± standard deviation (SD), and the chi-square or Fisher’s exact test was used for categorical variables expressed as counts and percentages, as appropriate. Changes within groups for continuous variables were analyzed using the paired t-test. Following univariate and bivariate screening, multivariate logistic regression was performed to identify associations between PJK and related factors in AIS, accounting for overfitting. 19 Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs). The intraclass correlation coefficient (ICC) was utilized to determine the interobserver reliability of the radiographic measurements obtained by 2 independent, board-certified orthopedic surgeons. The degree of agreement was classified as poor (<0.50), moderate (0.50-0.75), good (0.75-0.90), or excellent (>0.90). 20 A P-value of <0.05 was considered statistically significant.
Results
The PJK Occurrence and Baseline Characteristics in AIS Cohort
Baseline Characteristics Between Two Groups
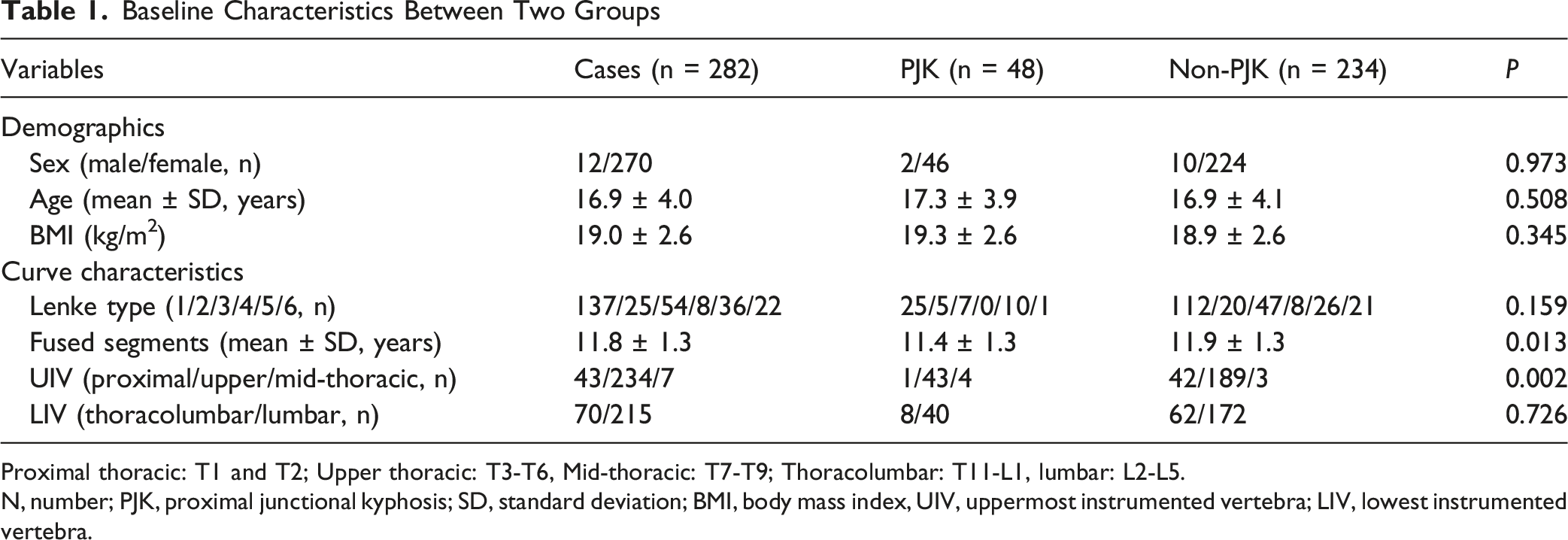
Proximal thoracic: T1 and T2; Upper thoracic: T3-T6, Mid-thoracic: T7-T9; Thoracolumbar: T11-L1, lumbar: L2-L5.
N, number; PJK, proximal junctional kyphosis; SD, standard deviation; BMI, body mass index, UIV, uppermost instrumented vertebra; LIV, lowest instrumented vertebra.
Coronal, Sagittal and Spinopelvic Parameters
Radiological Parameters for Curve Magnitude Between PJK and Non-PJK Group
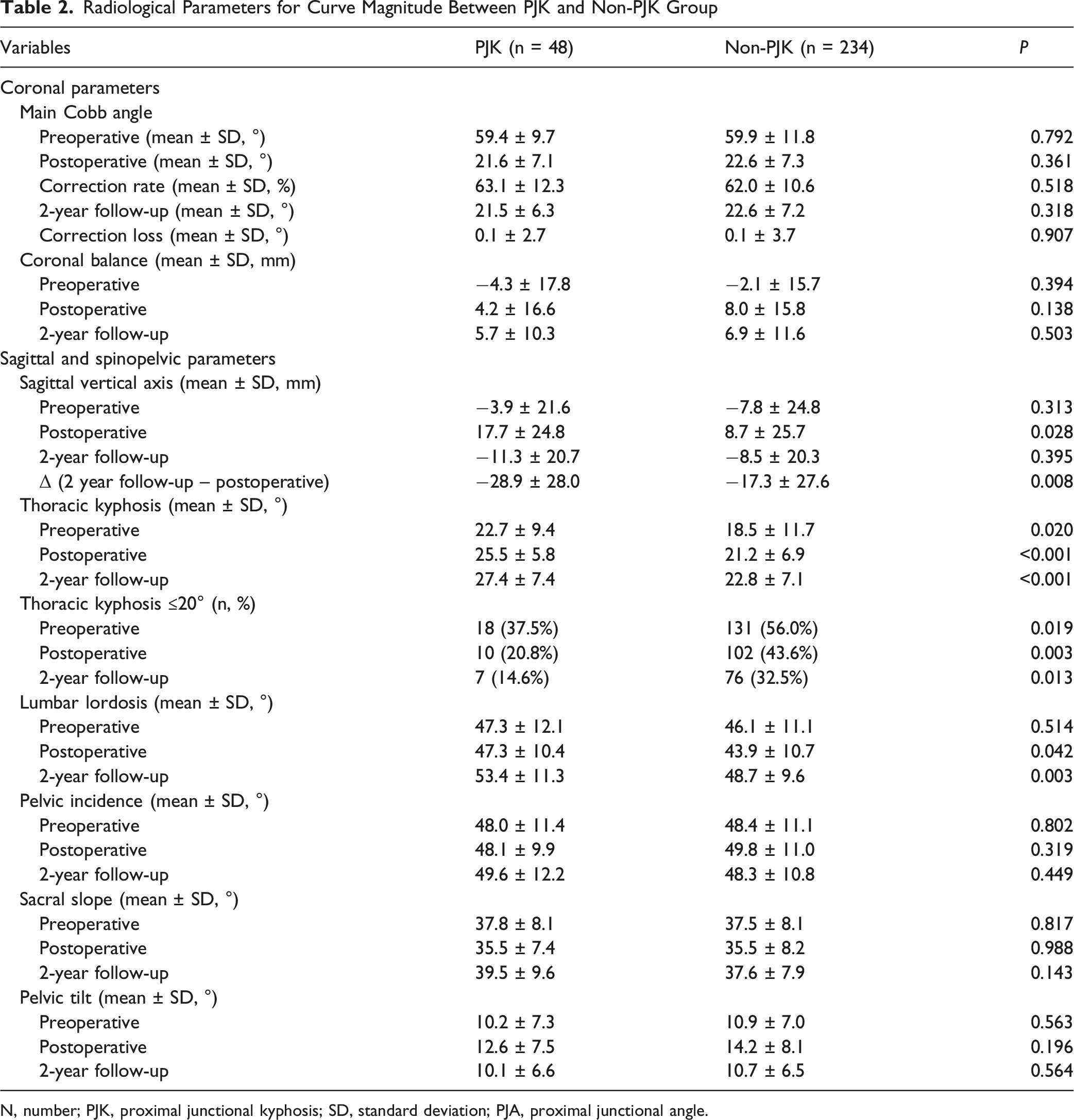
N, number; PJK, proximal junctional kyphosis; SD, standard deviation; PJA, proximal junctional angle.
Functional Alignment, Spinal Shape, and Sagittal Balance
Functional Alignment, Spinal Shape, Sagittal Balance Between PJK and Non-PJK Group in Adolescent Idiopathic Scoliosis
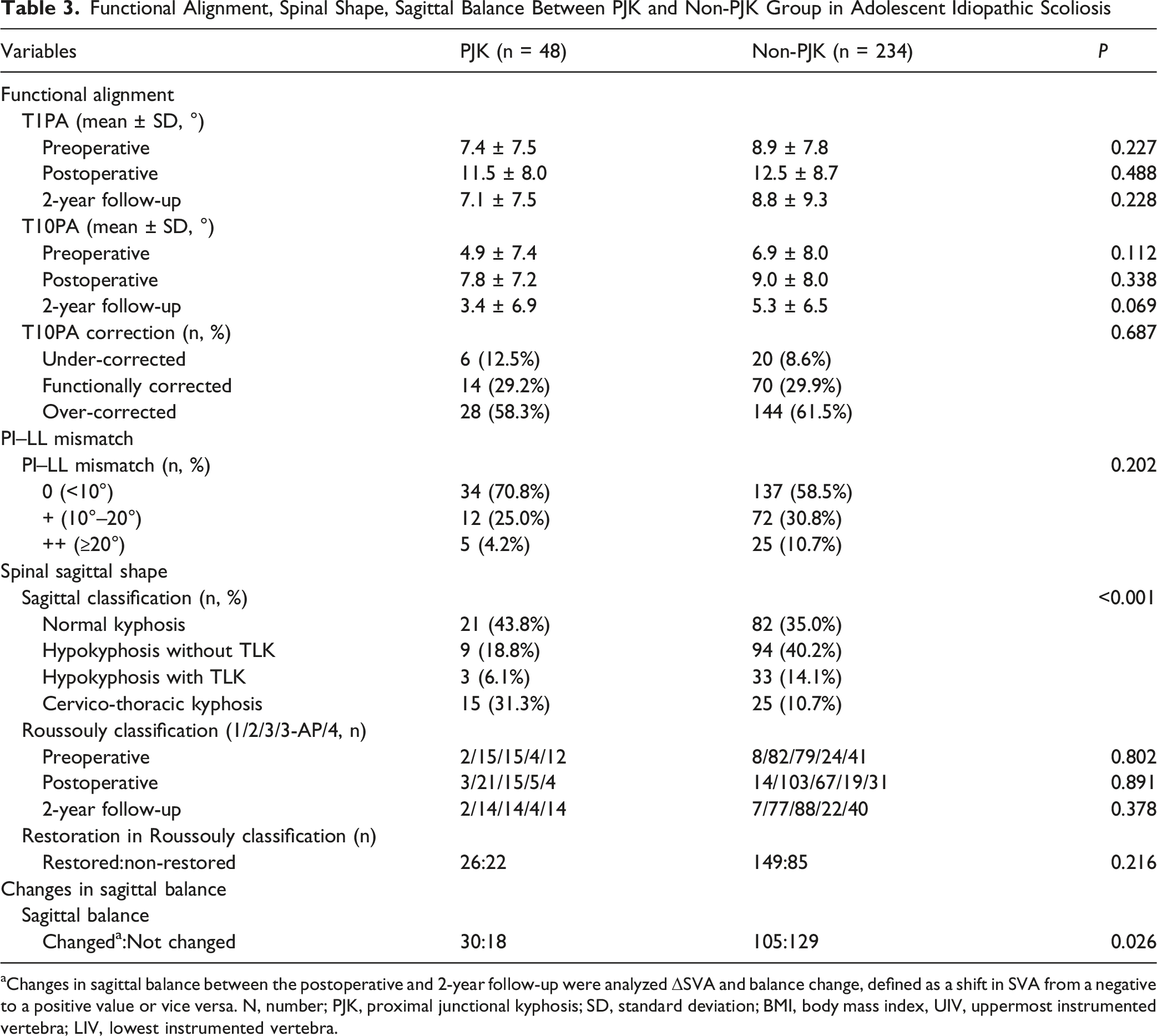
aChanges in sagittal balance between the postoperative and 2-year follow-up were analyzed ΔSVA and balance change, defined as a shift in SVA from a negative to a positive value or vice versa. N, number; PJK, proximal junctional kyphosis; SD, standard deviation; BMI, body mass index, UIV, uppermost instrumented vertebra; LIV, lowest instrumented vertebra.
Multivariate Logistic Regression Model for PJK in the AIS Cohort
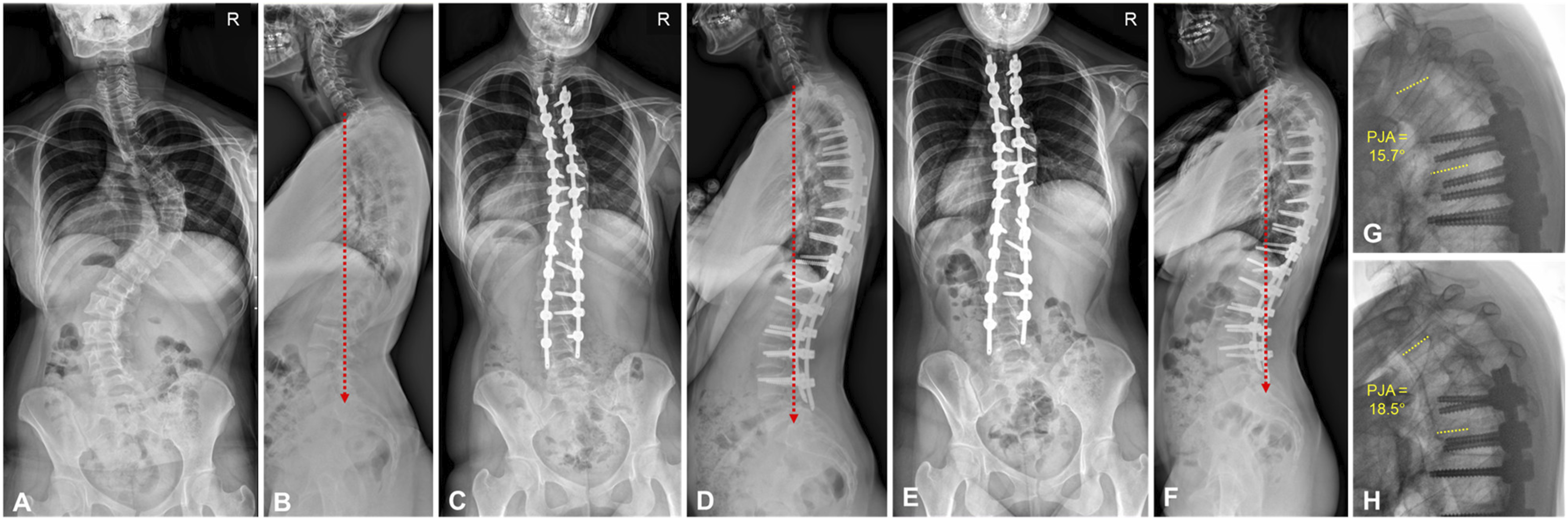
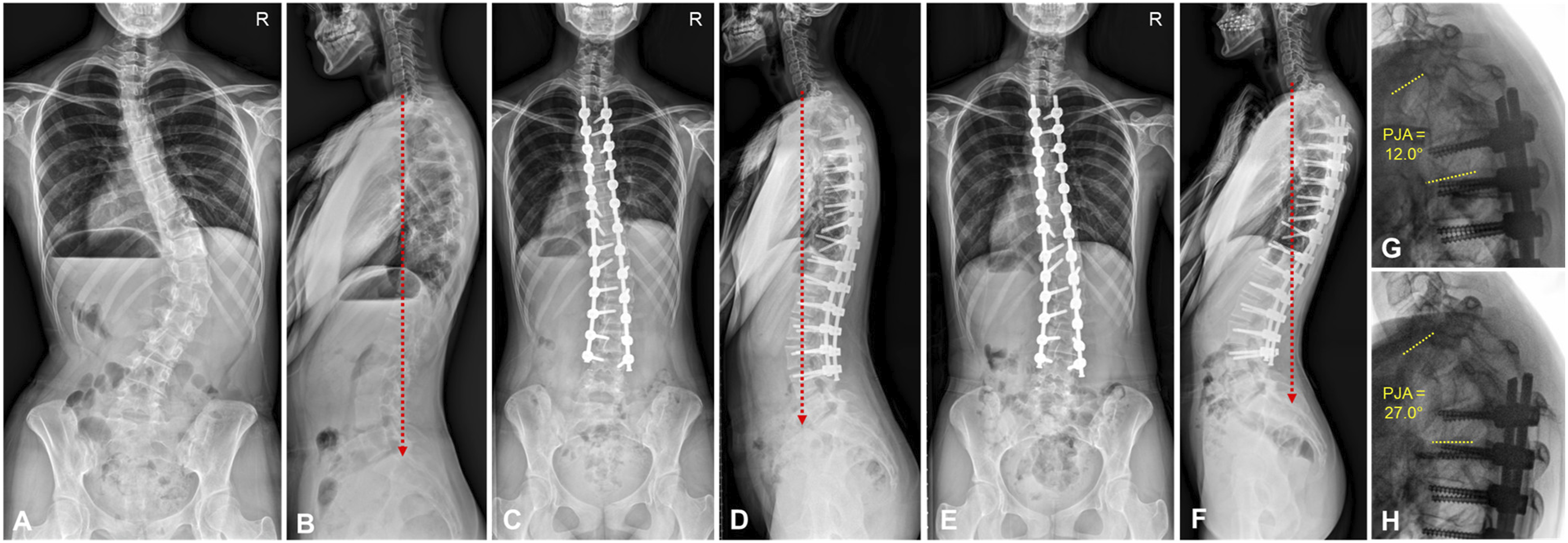
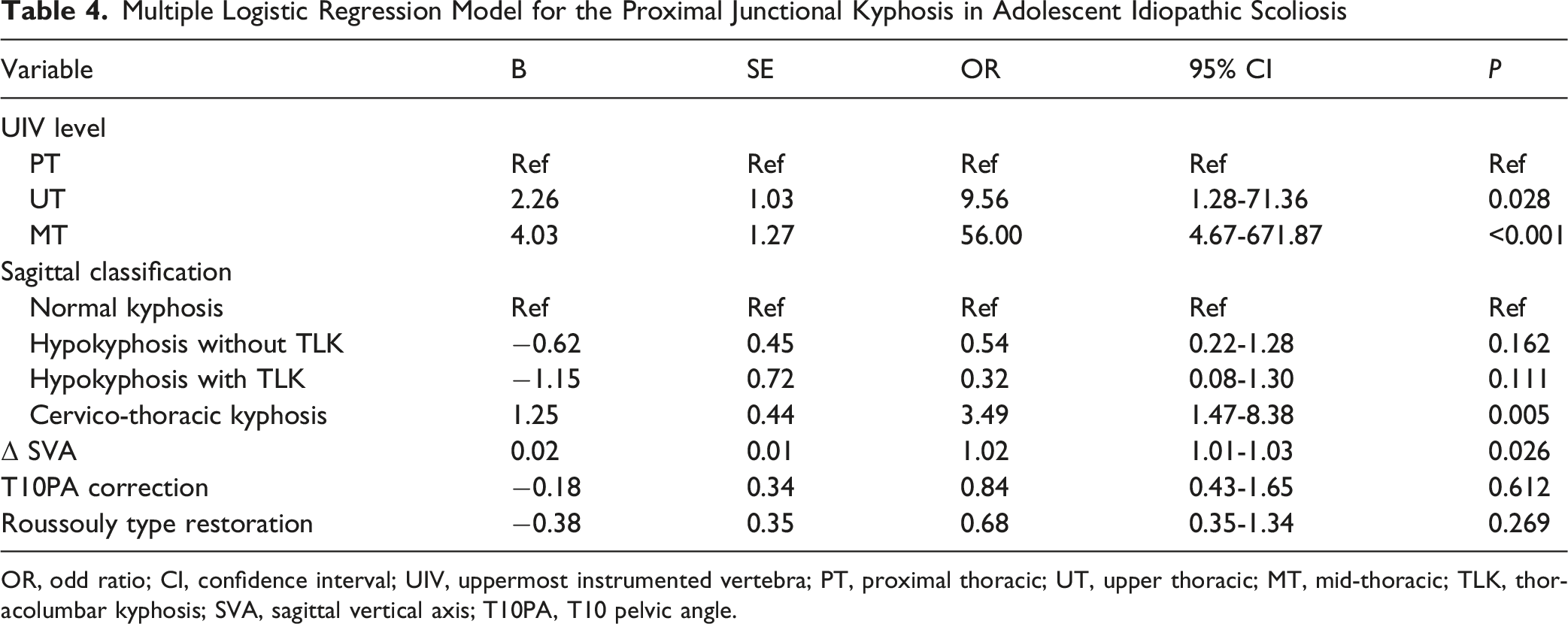
The multivariate logistic regression analysis demonstrated that the UIV level, sagittal classification, and ΔSVA were significantly associated with the development of PJK. Compared with the PT level, UIV at the UT (OR, 9.56; 95% CI, 1.28-71.36) and MT (OR, 56.00; 95% CI, 4.67-671.87) regions showed a significantly increased risk of PJK (Figure 2). Among the sagittal classifications in AIS, with type 1 (normal TK) as the reference, cervicothoracic kyphosis (type 3) demonstrated a significant association with PJK (OR, 3.49; 95% CI, 1.47-8.38) (Figure 3). In addition, ΔSVA was significantly associated with an increased risk of PJK (OR, 1.02; 95% CI, 1.01-1.03) (Figure 4). However, no significant associations were observed for functional alignment (T10PA correction) or restoration of the Roussouly type (Table 4). Case presentation of adolescent idiopathic scoliosis (AIS) with proximal junctional kyphosis (PJK) associated with uppermost instrumented vertebra level. (A and B) A 18-year-old female with Lenke 5 AIS with normal thoracic kyphosis. (C and D) Deformity correction from T7 to L4 was performed to correct scoliotic curve. (E and F) At 2-year follow-up, PJK was developed. (G and H) The proximal junctional angle was 9.7° at postoperative follow-up, which was aggravated to 22.3° at 2-year follow-up. R, right Case presentation of adolescent idiopathic scoliosis (AIS) with proximal junctional kyphosis (PJK) associated with sagittal spinal shape. (A and B) A 17-year-old female with Lenke 3 AIS with cervico-thoracic kyphosis (type 3). (C and D) Deformity correction from T4 to L4 was performed to correct scoliotic curve. (E and F) At 2-year follow-up, PJK was also observed. (G and H) The proximal junctional angle was 15.7° at postoperative follow-up, which was aggravated to 18.5° at 2-year follow-up. R, right Case presentation of adolescent idiopathic scoliosis (AIS) with proximal junctional kyphosis associated with changes in sagittal balance. (A and B) A 17-year-old female with Lenke 6 AIS with normal thoracic kyphosis. (C and D) Deformity correction from T4 to L4 was performed to correct scoliotic curve and positive sagittal vertical axis (SVA). (E and F) At 2-year follow-up, PJK was also observed with negative SVA, indicating changes in sagittal balance. (G and H) The proximal junctional angle was 12.0° at postoperative follow-up, which was aggravated to 27.0° at 2-year follow-up. R, right Multiple Logistic Regression Model for the Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis OR, odd ratio; CI, confidence interval; UIV, uppermost instrumented vertebra; PT, proximal thoracic; UT, upper thoracic; MT, mid-thoracic; TLK, thoracolumbar kyphosis; SVA, sagittal vertical axis; T10PA, T10 pelvic angle.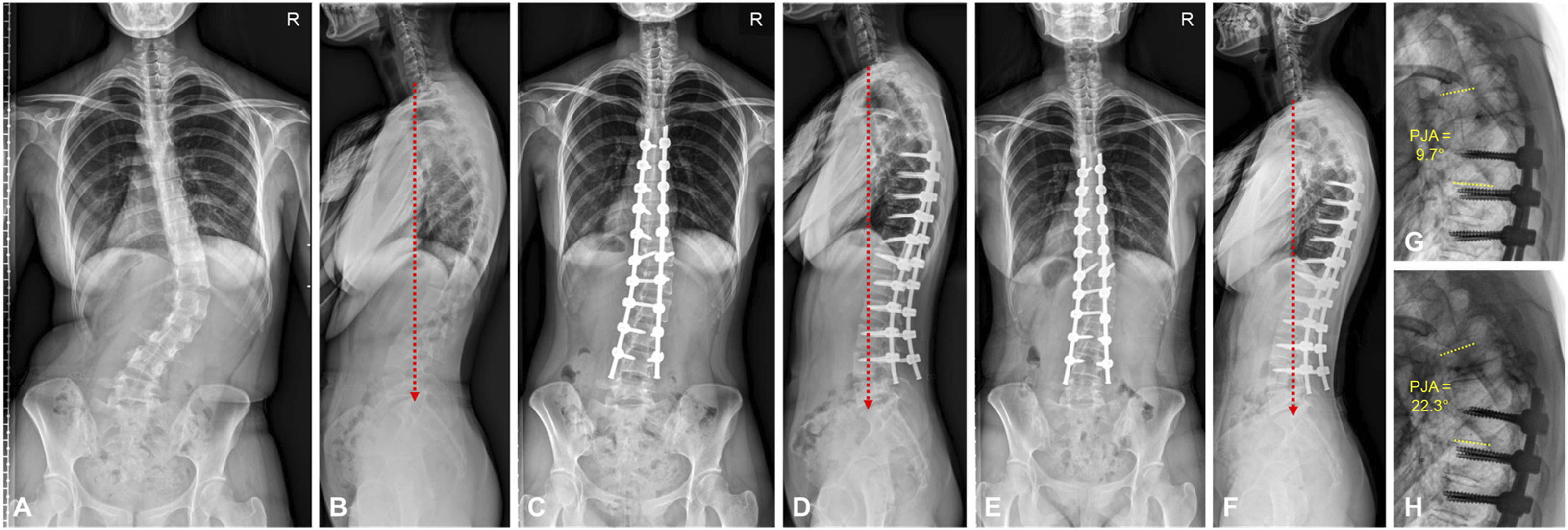
PJK Rates Based on Sagittal Shape
The Rate of Proximal Junctional Kyphosis in Sagittal Alignment According to the Uppermost Instrumented Vertebra (UIV) Level, the Correction of Functional Alignment and the Restoration of Spinal Shape
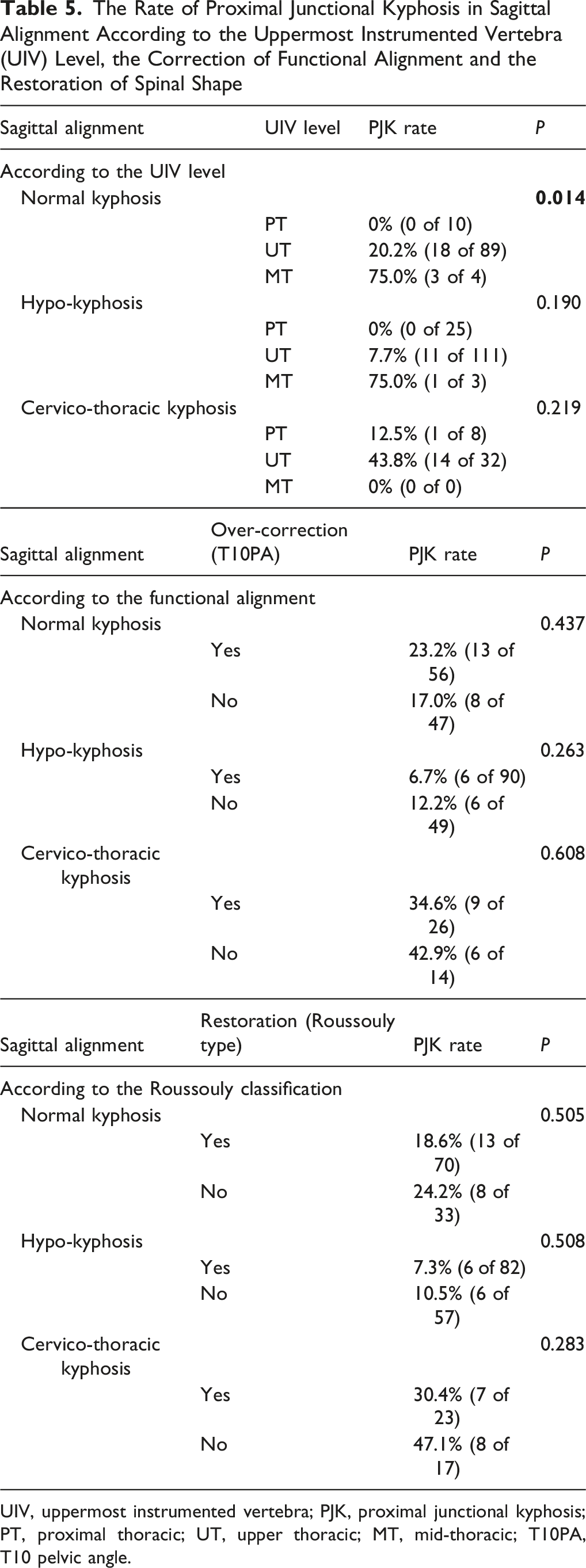
UIV, uppermost instrumented vertebra; PJK, proximal junctional kyphosis; PT, proximal thoracic; UT, upper thoracic; MT, mid-thoracic; T10PA, T10 pelvic angle.
PJA Progression Beyond 2-Years
Proximal Junctional Angle and Its Change Beyond Two-Years Between the Two Groups
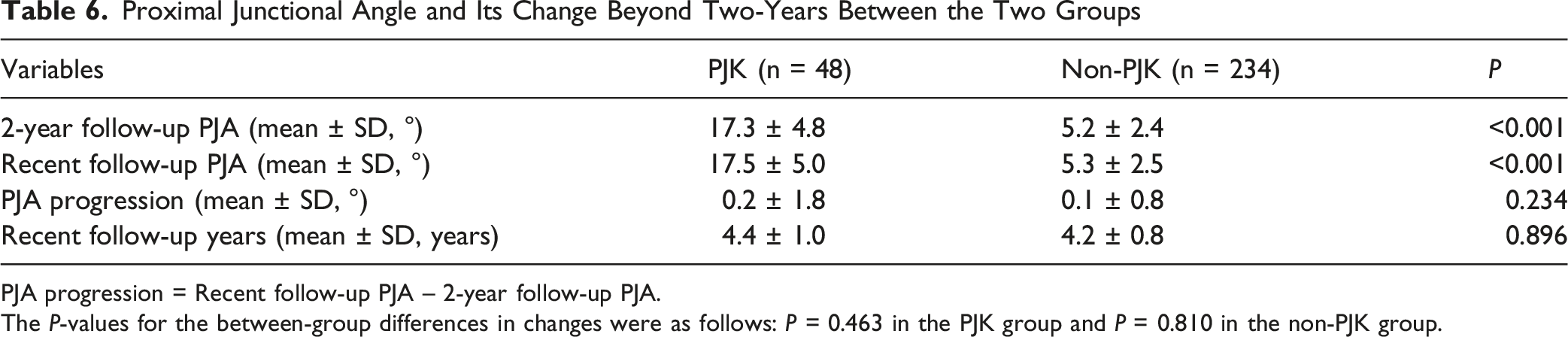
PJA progression = Recent follow-up PJA – 2-year follow-up PJA.
The P-values for the between-group differences in changes were as follows: P = 0.463 in the PJK group and P = 0.810 in the non-PJK group.
Discussion
In present study, the radiographic PJK rate in AIS was 17.0%, which was not progressed on the PJF. In particular, No cases of PJF were observed during the follow-up period. No patients in our cohort required revision surgery due to PJK. Only 3 patients who presented with severe PJK (PJA ≥28°) experienced mild upper thoracic pain. Our findings demonstrated that sagittal profiles were significantly associated with the development of PJK, with UIV level, cervicothoracic kyphosis, and ΔSVA identified as contributing factors in the multivariate logistic regression model. Considering the relationship between UIV level and sagittal spinal shape, cervicothoracic kyphosis itself not only increased the overall risk of PJK but also that in cases with normal TK, PJK occurred more frequently when the UIV was located in the MT region.
Previous studies have reported a wide range of PJK incidence in AIS. 21 Kim et al noted that PJK typically did not progress significantly beyond the 2-year follow-up in AIS, which is consistent with our data. 22 They also found that a larger TK was significantly associated with PJK, whereas the presence of PJK did not affect patient-reported outcome measures. 22 Ferrero et al reported higher PI, LL, and TK were more likely to develop PJK, and posterior imbalance could be one of the underlying causes of PJK in AIS. 23 The findings from previous studies share several key observations with our results. Radiographic PJK is relatively common after deformity correction for AIS and is often associated with a larger TK. These consistent findings suggest that, although PJK frequently appears radiographically after surgery, its clinical impact remains limited. Such PJK in AIS appears to be influenced by preoperative sagittal shape (cervicothoracic kyphosis), changes in sagittal balance (ΔSVA), and the residual kyphotic contour near the UIV, yet it seldom progresses to PJF, reflecting an adaptive rather than mechanical failure.
In ASD, sagittal decompensation is the main cause of deformity and is further interacted with bone and paraspinal muscle quality in a complex manner.3,24 Given the substantial correlation between radiological parameters and health-related quality of life, recent surgical strategies has been evolved, such as achieving PI-LL match and a functionally aligned correction in relation to T10PA and proper restoration of Roussouly type.3,7,18 When postoperative sagittal decompensation develops near the residual thoracic contour at the UIV, it may result in localized imbalance at UIV level that can progress to PJF, a catastrophic event in ASD. In contrast, AIS present with distinct sagittal characteristics related to relative anterior spinal overgrowth-based thoracic kyphotic morphology, in which radiographic PJK may occur as a compensatory response at the residual kyphotic contour near the UIV following posterior spinal fusion. Therefore, unlike in ASD, PJK in AIS may not simply represent a mechanical complication, but rather a reciprocal change associated with sagittal realignment.
Clement et al described PJK in AIS as a rebalancing phenomenon that occurs due to insufficient postoperative TK compared with the patient-specific TK. 25 The patient-specific TK reflects the natural correlation between greater TK and greater LL. 25 They further suggested that, as the upper segment of non-instrumented regions undergoes postoperative rebalancing, PJK or distal cervical kyphosis may develop as compensatory changes. 25 This concept is consistent with our findings, in which LL at the 2-year follow-up was significantly greater in the PJK group, and cervicothoracic kyphosis was more frequently observed among patients with PJK. Moreover, the relationship between residual kyphotic contour and UIV levels may provide a wider range for such rebalancing, supporting our interpretation of PJK in AIS.
Importantly, in our cohort, the PJK group had significantly greater TK at all time points. Given that preoperative TK was already significantly larger in the PJK group, the greater postoperative TK is more likely to reflect the persistence of the patient’s intrinsic sagittal profile rather than an over-restoration of TK or aggressive rod contouring contributing to proximal junctional stress. In such cases, particularly when a cervicothoracic kyphotic profile is present, the biomechanical interaction between the rigid rod and the upper thoracic shape above the UIV inevitably concentrates mechanical stress at the UIV. Consequently, this localized stress, combined with rebalancing at the upper thoracic non-instrumented segments, further supports our description that PJK in AIS is predominantly a reciprocal change.
In our study, the Roussouly classification and its proper restoration were not associated with the development of PJK in AIS. Contrary to our findings, a previous study reported that restoring the ideal Roussouly sagittal alignment in Lenke type 5 curves could potentially reduce the risk of PJK. 26 This discrepancy may be explained by the characteristics of our adolescent cohort aged <18 years, in whom spinopelvic parameters are potentially subject to change and the physiological reference values for healthy adolescents are not yet fully established. 26 Therefore, applying an adult-derived classification system such as Roussouly classification and functional alignment may have inherent limitation in the AIS population.
This study has several limitations. First, its retrospective design and single-center cohort may have introduced selection bias. Second, radiological analysis was performed using 2D plain radiographs, without incorporating 3D-based parameters that could provide a more comprehensive assessment of sagittal alignment. 27 Third, clinical outcomes were not evaluated; however, previous studies on PJK in AIS have reported that its presence rarely affects patient-reported outcomes. 22 Finally, although we observed the progression of PJK beyond 2 years, these findings do not fully reflect true long-term outcomes. Future studies utilizing long-term follow-up data of 10 years or are warranted. Despite these limitations, our study highlights that the mechanisms of PJK in AIS—still only partially understood—can be interpreted from the perspective of sagittal shape and alignment, supporting the concept of a reciprocal change.
Conclusion
Our findings indicated that UIV level, cervicothoracic kyphotic profile, and greater changes in the SVA were the contributing factors of development of radiographic PJK. In contrast to ASD, PJK in AIS rarely causes serious clinical sequelae but instead represents reciprocal changes driven by the original sagittal shape and subsequent alterations in sagittal alignment.
Supplemental Material
Supplemental Material - Sagittal Profiles and Their Reciprocal Changes Manifesting in Proximal Junctional Kyphosis Following Deformity Correction in Adolescent Idiopathic Scoliosis
Supplemental Material for Sagittal Profiles and Their Reciprocal Changes Manifesting in Proximal Junctional Kyphosis Following Deformity Correction in Adolescent Idiopathic Scoliosis by Hong Jin Kim, Jungwook Lim, Subin Lim, Hyung Rae Lee, Jae Hyuk Yang, and Seung Woo Suh in Global Spine Journal
Footnotes
Ethical Considerations
This retrospective study was approved by the Institutional Review Board of Korea University Guro Hospital (IRB number: 2026GR0008)
Consent to Participate
Informed consent for retrospective analysis of de-identified data was waived.
Author Contributions
HJK and SWS developed study concept and design; HJK, JL performed acquisition, analysis, or interpretation of data; HJK drafted the initial manuscript; All authors contributed to editing and reviewing the manuscript and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2024-00352326).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are not publicly available due to ethical issues but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.