
Abstract
Study Design
Systematic Review.
Objective
To evaluate neurological outcomes, complication rates, and operative characteristics of the posterior transdural approach for thoracic disc herniation causing myelopathy.
Methods
A systematic review was conducted in accordance with PRISMA 2020 guidelines. MEDLINE, Embase, and PubMed were searched from inception to January 2026. Studies including adult patients undergoing posterior transdural decompression for thoracic disc herniation were eligible. Two reviewers independently performed study selection, data extraction, and methodological quality assessment using the Joanna Briggs Institute checklist for case series. Extracted variables included patient demographics, disc characteristics, operative details, neurological outcomes, follow-up duration, and complications.
Results
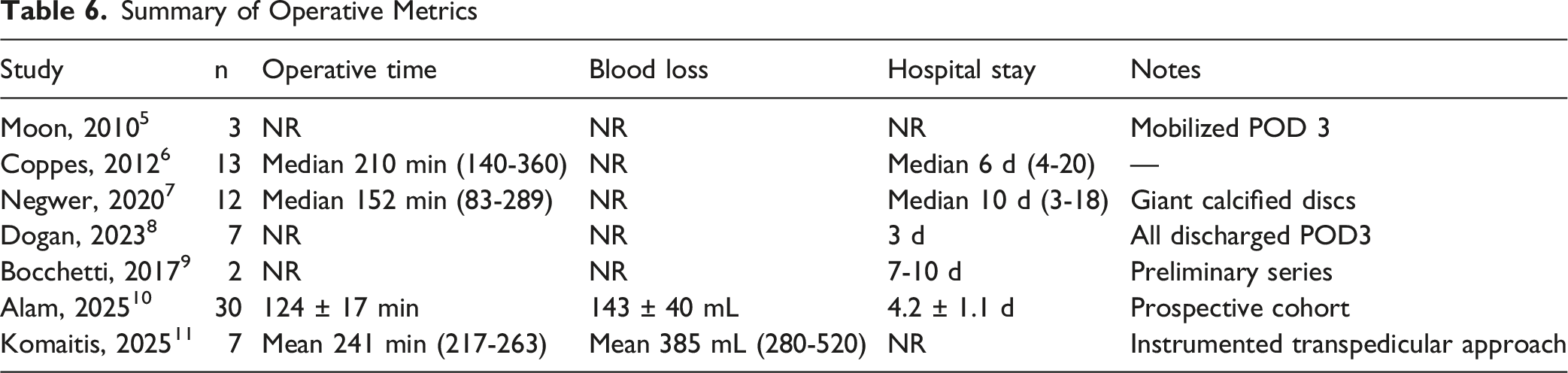
Seven Level IV studies comprising 74 patients were included. The weighted mean age was 52.8 years, and 70.3% of discs were calcified. The posterior transdural corridor was utilized in all cases; however, ventral durotomy was performed in 72 of 74 patients (97.3%), with preservation of the ventral dura reported in selected cases. Across studies reporting extractable outcome data, 76% of patients demonstrated neurological improvement, 21% remained stable, and 1.4% experienced persistent neurological deterioration. Transient postoperative neurological worsening occurred in 9.5% of patients and resolved in nearly all cases. Cerebrospinal fluid leakage occurred in 4.1%, with reoperation required in 2.7%. No mortality was reported. Reported operative time varied across studies, ranging from a mean of 124 min in the prospective cohort to a mean of 241 min in the transpedicular–transdural series, with other studies reporting median values between 152 and 210 min.
Conclusion
Posterior transdural decompression for thoracic disc herniation causing myelopathy is associated with favorable neurological outcomes and a low rate of permanent morbidity, even in predominantly calcified or giant disc pathology. In appropriately selected patients, this technique appears to provide effective ventral decompression with an acceptable safety profile.
Introduction
Thoracic disc herniation (TDH) is an uncommon but potentially disabling cause of myelopathy, accounting for less than 1% of symptomatic disc disease. Owing to the narrow thoracic spinal canal, kyphotic alignment, and frequent ventral or calcified disc morphology, surgical management remains technically demanding. Historically, simple laminectomy was associated with poor neurological outcomes due to inadequate ventral decompression and spinal cord manipulation, prompting the development of alternative approaches, including transthoracic, thoracoscopic, transpedicular, costotransversectomy, and transfacet pedicle-sparing techniques.1,2
Although anterior and thoracoscopic approaches provide direct ventral access, they are associated with approach-related morbidity, including pulmonary and cardiothoracic complications. Posterolateral strategies aim to reduce systemic morbidity but may provide limited visualization of centrally located or densely calcified discs. The posterior transdural approach has emerged as an alternative technique that allows direct visualization and removal of ventral pathology through a posterior corridor while avoiding thoracotomy. However, this technique requires intentional dural opening and manipulation of neural structures, raising concerns regarding cerebrospinal fluid leakage and neurological injury.
Despite increasing use in selected cases, the existing literature on transdural decompression for thoracic myelopathy consists primarily of small retrospective case series. Outcomes, complication profiles, and operative characteristics have not been systematically synthesised, and the relative safety of this approach—particularly in calcified or giant disc pathology—remains incompletely defined.
The purpose of this study was to perform a systematic review of published case series reporting outcomes of posterior transdural decompression for thoracic disc herniation presenting with myelopathy. We aimed to evaluate neurological outcomes, complication rates, and operative metrics in order to better define the safety profile and clinical role of this technique.
Methods
Protocol and Reporting
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 3 The review protocol was developed a priori and followed throughout the study.
Data Sources and Search Strategy
A comprehensive electronic search was performed in the following databases from inception to the final search date, January 2026: MEDLINE, Embase, and PubMed. The search strategy combined controlled vocabulary (eg, MeSH/Emtree terms) with free-text keywords and applied Boolean operators, truncation, and database-specific syntax. Key concepts included (1) thoracic disc herniation (eg, thoracic disc herniation, thoracic vertebrae, disc, disk, herniation, prolapse, extrusion, protrusion) and (2) surgical approach (eg, transdural, trans-dural, intradural, intra-dural, posterior, dorsal, transpedicular, laminectomy, laminoplasty, costotransversectomy).
No language limits were applied during the search. During screening, only English-language full-text articles were included due to feasibility constraints.
Eligibility Criteria
Studies were selected according to the PICOTS framework as follows: • • • • • •
Exclusion Criteria
Studies were excluded if they involved pediatric patients, non-thoracic disc herniations, or do not specifically evaluate a transdural surgical approach. Case reports, review articles, editorials, conference abstracts without full data, technical notes lacking clinical outcomes, and cadaveric or biomechanical studies were excluded. Studies not reporting postoperative outcomes or with insufficient methodological detail were also excluded, as will non-English publications.
Study Selection
Two reviewers independently screened titles and abstracts, followed by full-text review. Disagreements were resolved by consensus with the senior author. A total of 3056 records were identified, of which 992 duplicates were removed. After screening 2064 abstracts, 7 studies met the inclusion criteria, as shown in Figure 1. PRISMA chart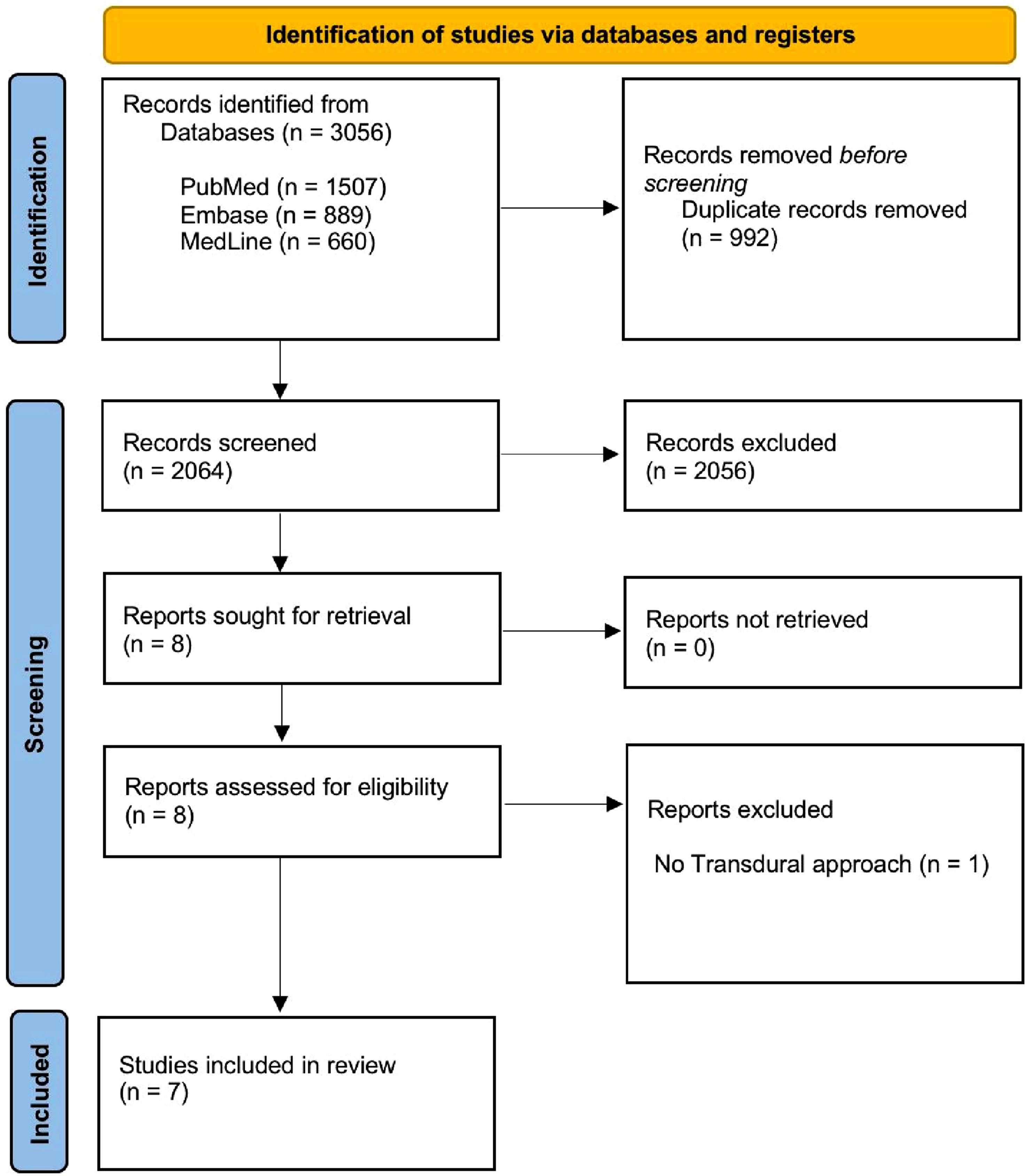
Data Extraction
Two reviewers independently performed data extraction using a standardized form that included study characteristics (author, year, country, design), patient demographics and clinical presentation, radiological features of the thoracic disc herniation (level, location, calcification, canal occupation), detailed surgical technique variables related to the transdural approach, perioperative parameters (operative time, blood loss, length of stay), postoperative neurological and functional outcomes, duration of follow-up, and reported intraoperative and postoperative complications.
Quality Assessment
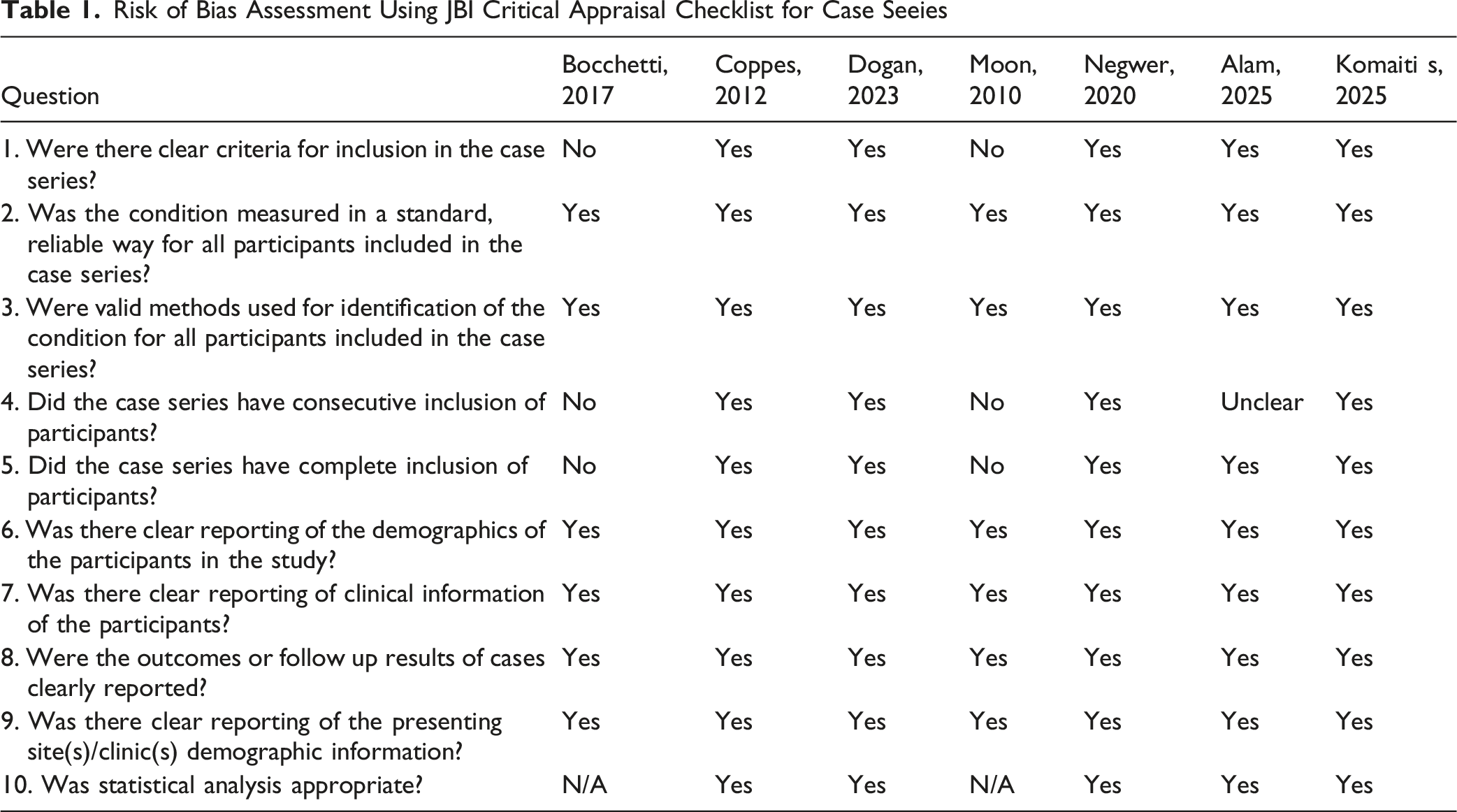
Risk of Bias Assessment Using JBI Critical Appraisal Checklist for Case Seeies
Results
Seven Level IV studies5-11 comprising 74 patients were included (Table 1). Six were retrospective case series5-11 and one was a prospective observational cohort. 10 The pooled cohort included 42 males and 32 females (male-to-female ratio 1.3:1). The weighted mean age across all studies was 52.8 years, with individual study means ranging from 45.2 to 58.0 years and an overall reported age range of 17 to 94 years.
Calcified disc herniations were reported in 52 of 74 patients (70.3%). Giant disc herniations, defined as occupying more than 40-50% of the spinal canal, were explicitly described in 19 patients (25.7%), all of whom were included in two dedicated giant-disc cohorts.7,11 Ventral dural opening was performed in 72 of 74 patients (97.3%), ventral dura preservation was reported by Bocchetti et al. 9 Posterior instrumentation was used in 7 patients (9.5%), all within a single study. 11 Intraoperative neuromonitoring was reported in four studies7-9,11 and was utilized in 28 of 74 patients (37.8%).
Studies Demographics and Characteristics

Technical Strategies
Across the included studies, several recurring technical strategies were described to improve ventral access while minimizing spinal cord manipulation. These included CSF drainage after durotomy, sectioning or suspension of the dentate ligament, microscope-assisted visualization, gentle or gravity-assisted cord displacement, and avoidance of forceful disc-space exploration. For calcified or giant discs, authors described controlled internal debulking or piecemeal removal using hooks, punches, high-speed drilling, CUSA, or ultrasonic bone instruments. Intraoperative neuromonitoring was reported in four studies and was used in 28 of 74 patients, most commonly in contemporary series involving calcified or giant discs. Detailed study-level technical strategies are provided in Supplemental Table 1.
Clinical Neurological Outcome
Summary of Outcomes
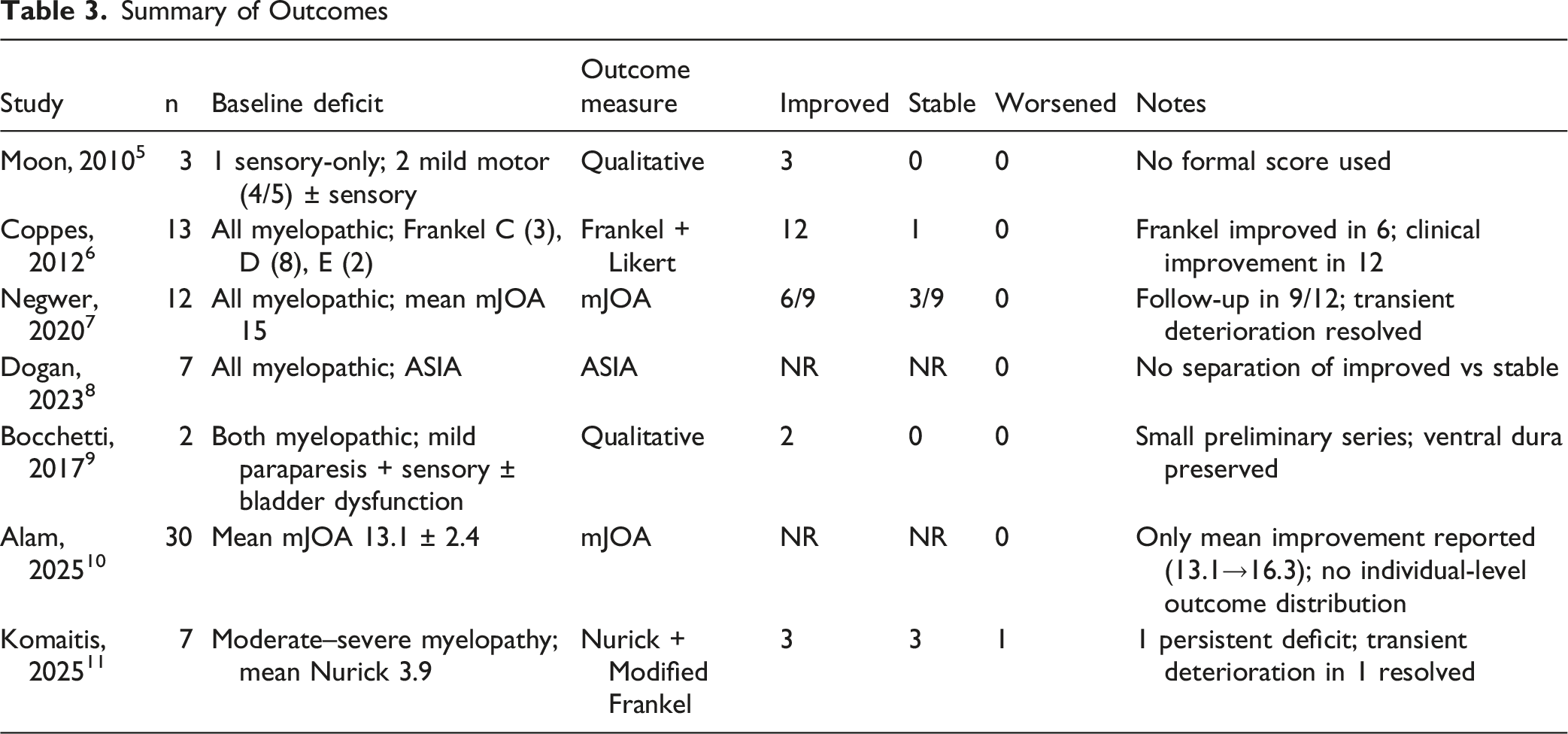
Two studies8,10 did not provide categorical patient-level distribution. Dogan et al. 8 reported that all seven patients were neurologically stable or improved at follow-up, with no deterioration. Alam et al. 10 demonstrated significant mean mJOA improvement (13.1 to 16.3; P < 0.001) in a prospective cohort of 30 patients, with no permanent neurological deficits reported, although individual outcome stratification was not available.
Across the total pooled cohort of 74 patients, only one case of persistent neurological deterioration was reported (1.4%), with the majority of patients demonstrating neurological improvement or stability at final follow-up.
Follow-up duration varied substantially between studies, limiting comparability of long-term neurological recovery rates.
Dural Repair
Dural Repair Techniques
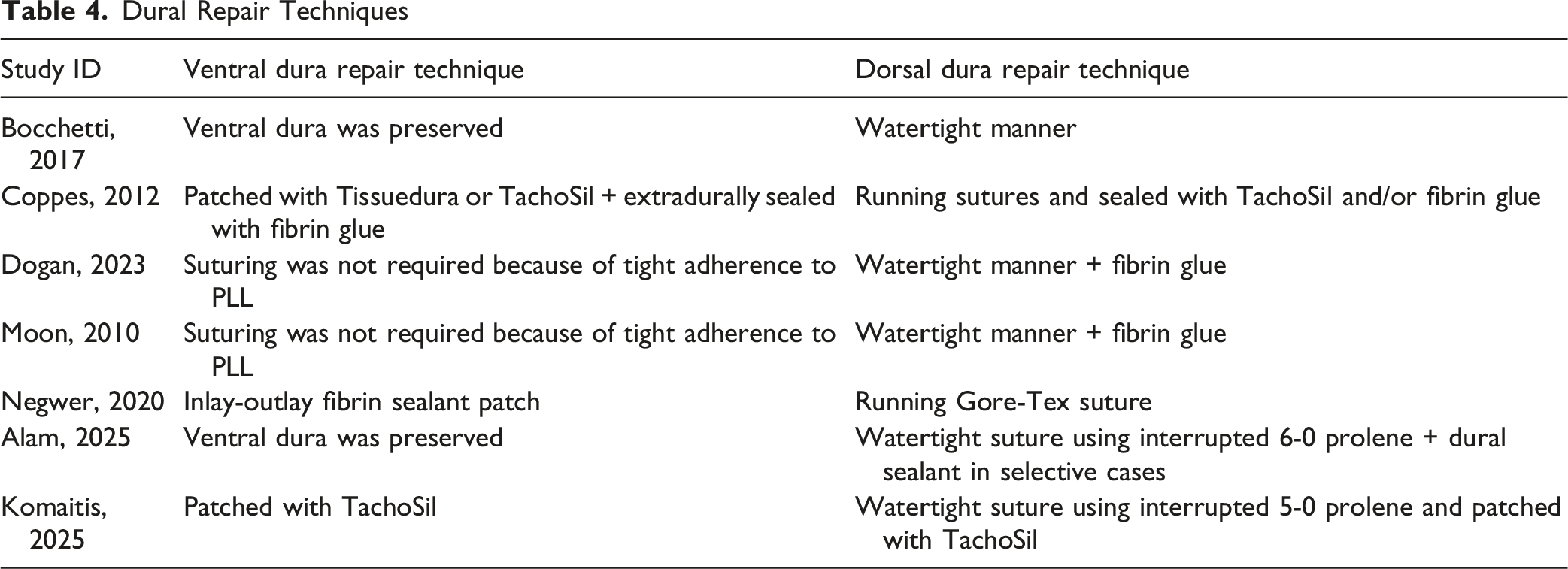
Dorsal dural closure was consistently performed in a watertight fashion, most commonly using running or interrupted sutures (eg, Prolene or Gore-Tex), frequently augmented with fibrin sealants or patch materials. Despite variability in technique, the overall CSF leak rate remained low (4.1%), with only one case requiring reoperation.
Complications
Summary of Complications
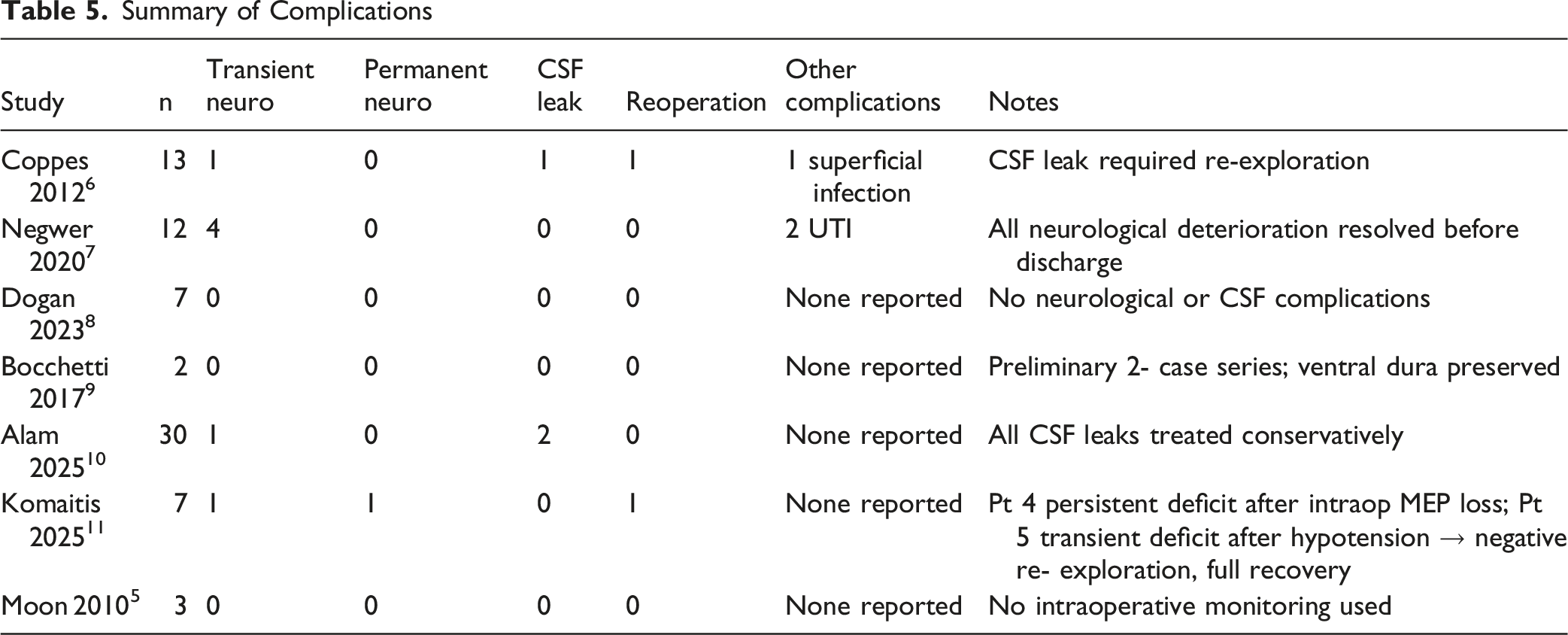
Persistent neurological deterioration was reported in a single patient (1.4% of the total cohort), occurring in the Komaitis series following intraoperative neuromonitoring signal loss. 11
Cerebrospinal fluid (CSF) leakage occurred in three patients overall (4.1%). Two cases were reported in the prospective cohort by Alam et al. 10 (6.7%) and were managed conservatively without reoperation. One case was reported by Coppes et al. 6 (7.7%) and required surgical re-exploration. No CSF leaks were observed in the remaining studies.
Reoperation was required in two patients (2.7%): one for persistent CSF leakage 6 and one for postoperative neurological deterioration with negative surgical exploration. 11 Other reported complications included two urinary tract infections 7 and one superficial wound infection. 6 No mortality was reported in any study.
Within the limitations of small case series and short follow-up in several studies, permanent neurological morbidity and reoperation rates were low.
Operative Metrics
Summary of Operative Metrics
Discussion
Thoracic disc herniation (TDH) causing myelopathy remains a surgically challenging entity due to the narrow thoracic canal, kyphotic alignment, and frequent ventral or calcified disc morphology. The optimal surgical approach remains debated, with options including transthoracic, thoracoscopic, transpedicular, costotransversectomy, transfacet pedicle-sparing, and transdural posterior techniques. This systematic review specifically evaluated outcomes of the posterior transdural approach in 74 patients across seven Level IV series5-11 and demonstrates three principal findings: (1) neurological improvement or stability was achieved in the majority of cases; (2) permanent neurological deterioration was rare; and (3) overall complication and reoperation rates were low despite a high proportion of calcified or giant disc pathology.
Interpretation of Neurological Outcomes
Across studies reporting extractable patient-level data, neurological improvement was observed in approximately three-quarters of patients, with only one case of persistent deterioration in the pooled cohort. 11 Importantly, the majority of included cases involved centrally located and frequently calcified discs, a pathology typically considered technically demanding. This suggests that direct ventral decompression through a transdural corridor can achieve satisfactory cord decompression without the morbidity traditionally associated with anterior access.
The favorable neurological profile observed in this review aligns with larger posterolateral and transfacet pedicle-sparing series, which report neurological improvement rates between 60-80% with low permanent deficit rates. 12 However, those series often include mixed soft and calcified discs and employ indirect or lateralized decompression techniques rather than direct intradural ventral exposure. The transdural approach differs conceptually by providing direct visualization of ventral pathology without thoracotomy, potentially reducing manipulation of the spinal cord during ventral disc removal.
In comparison, anterior and transthoracic approaches historically offer excellent ventral exposure but at the cost of approach-related morbidity, including pulmonary complications, chest tube requirements, and longer recovery. 1 Systematic comparisons between anterior and posterior strategies suggest that posterior-based approaches may carry lower systemic morbidity while achieving comparable neurological recovery. 1 Our findings support this trend, particularly in centrally located calcified discs where posterior transdural decompression avoids thoracotomy.
Calcified and Giant Discs: Complexity vs Prognosis
A notable feature of the included cohorts is the high proportion of calcified and giant discs. Calcified morphology is frequently associated with dural adherence, intradural extension, and greater operative complexity. In a comparative cohort of soft vs calcified TDH, 13 calcified discs were associated with significantly higher blood loss and increased intraoperative neuromonitoring alerts, although long-term neurological outcomes were comparable between groups. This pattern is consistent with the broader literature: disc consistency appears to influence surgical complexity rather than ultimate neurological prognosis. 13
Within the transdural series included in this review, transient neurological worsening was more frequently reported in cohorts composed entirely of giant calcified discs. However, persistent deterioration remained rare. This suggests that while calcified morphology increases intraoperative risk, careful microsurgical technique and neuromonitoring can mitigate permanent injury. These findings contrast with earlier historical laminectomy-only series, where cord manipulation without direct disc removal was associated with high paralysis and mortality rates. 14 Modern microsurgical techniques, magnification, and neuromonitoring likely account for the improved safety profile seen in contemporary series.
Complication Profile in Context
The pooled CSF leak rate in this review was approximately 4%, with only one case requiring reoperation. This rate compares favorably with reports of posterolateral and costotransversectomy approaches, where CSF leak and wound complications are not uncommon.2,15 Transthoracic and thoracoscopic series report approach-specific pulmonary and cardiopulmonary complications in up to 15-20% of cases.1,16 Notably, the transdural approach shifts risk from pulmonary morbidity to dural management; however, modern watertight closure techniques appear to limit clinically significant CSF-related sequelae.
Reoperation rates across the pooled cohort were low (approximately 3%). This is comparable to, and in some series lower than, rates reported following costotransversectomy or transthoracic discectomy.1,2 Importantly, no mortality was reported in the transdural cohorts, whereas historical laminectomy-only strategies in elderly calcified discs demonstrated nontrivial mortality in medically complex patients. 14
Operative Metrics and Surgical Trade-Offs
Operative time and blood loss varied substantially between series. Instrumented or giant-disc cohorts demonstrated longer operative duration and higher blood loss, reflecting underlying pathology rather than approach-specific inefficiency. Compared with published transthoracic series, which often report prolonged operative times and higher systemic morbidity, the transdural approach may offer a less physiologically demanding alternative in selected patients. However, direct comparisons remain limited by heterogeneity in patient selection and reporting.
Selection Bias and Approach-specific Indications
It is critical to emphasize that transdural approaches are typically selected for centrally located, ventral, or calcified pathology where standard posterolateral exposure may be insufficient. Therefore, outcomes reported in these series likely reflect highly selected cases managed in experienced centers. The absence of comparative controlled trials prevents definitive conclusions regarding superiority over alternative approaches. Rather, the data suggest that the transdural technique represents a viable posterior strategy in appropriately selected patients, particularly when anterior access is undesirable.
Limitations
This review is limited by the exclusively Level IV nature of the included studies, small sample sizes, and retrospective design. Neurological outcomes were assessed using heterogeneous scoring systems (mJOA, Frankel, ASIA, qualitative assessment), necessitating harmonization into simplified categories of improvement, stability, or deterioration. Follow-up duration varied substantially across studies, limiting direct comparison of long-term recovery trajectories. Subgroup analysis by disc consistency, giant morphology, or fixation status was not feasible due to inconsistent reporting and limited stratified data. Publication bias and underreporting of minor complications remain possible. Additionally, no formal meta-analysis was performed due to methodological heterogeneity and low event rates; therefore, the findings should be interpreted descriptively.
Clinical Implications
Despite these limitations, the available evidence suggests that posterior transdural decompression for thoracic myelopathy can achieve favorable neurological outcomes with low permanent morbidity, even in predominantly calcified or giant disc pathology. When compared with anterior or thoracoscopic strategies, the transdural approach may avoid thoracotomy-related systemic complications while providing direct ventral decompression. The choice of approach should remain individualized, guided by disc morphology, surgeon expertise, and patient comorbidity profile.
Future multicenter prospective studies with standardized neurological scoring and direct comparative cohorts are required to better define the relative merits of transdural vs alternative posterior and anterior techniques.
Conclusion
The posterior transdural approach for thoracic disc herniation causing myelopathy demonstrates favorable neurological outcomes with a low rate of permanent morbidity across predominantly calcified and giant disc pathology. Despite technical complexity and the need for dural opening, pooled data from available case series suggest that direct ventral decompression via a transdural corridor can be performed safely in experienced hands. Complication and reoperation rates were low, and persistent neurological deterioration was uncommon.
Supplemental Material
Supplemental material - Posterior Transdural Decompression for Thoracic Disc Herniation Causing Myelopathy: A Systematic Review of Outcomes and Safety
Supplemental material for Posterior Transdural Decompression for Thoracic Disc Herniation Causing Myelopathy: A Systematic Review of Outcomes and Safety by Hussein Akil, MD, Deya AlWady, MD, Rodrigo Muscogliati, MD, Mohammad Badra, MD, Rami Abou Faour, MD, Spyridon Komaitis, MD, Khalid M. Salem, MD, Zeinab Nahle, MD, Farwa Abbas, Elie Najjar, MD in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.