
Abstract
Study Design
International Expert Cross-Sectional Survey.
Objectives
To establish international expert consensus on the definition, diagnostic criteria, imaging requirements, and surgical management of recurrent lumbar disc herniation (RLDH).
Methods
A comprehensive survey was developed based on current literature and disseminated globally via professional, academic, and personal networks among clinicians with expertise in spinal disorders. The survey covered core definitions, clinical symptoms, imaging criteria, and surgical preferences. Consensus was predefined as ≥70% agreement. Statistical analysis included descriptive statistics, Chi-square tests, Rasch analysis, and post-hoc analysis using adjusted standardized residuals with Bonferroni correction.
Results
A global cohort of 510 experts participated (62% neurosurgeons, 30% orthopedic surgeons), primarily from Europe (42%), North America (25%), and Asia (19%). Strong consensus was reached for defining RLDH as a new herniation at the same level (83.5%) and same side (72.4%) as the index surgery, following a pain-free interval (77.0%). No consensus was reached on interval duration. MRI confirmation was considered necessary (96.7%), with differentiation from postoperative scar tissue (87.0%). Open microdiscectomy remains the global gold standard (43%), with significant geographic (P < 0.0001) and specialty-based (P < 0.0001) variations. North Americans more often preferred tubular microdiscectomy (25%), Asians full endoscopic techniques (25%), and Europeans open microdiscectomy (56%). Neurosurgeons favored open procedures (55%), while orthopedic surgeons preferred full endoscopic approaches (29%) and fusion (21%).
Conclusions
This study establishes a foundation for an international consensus definition of RLDH as a new herniation at the same level and side as the initial herniation, with a pain-free interval and MRI confirmation differentiating from postoperative scar tissue.
Keywords
Introduction
Sciatica refers to pain that travels down the leg along the sciatic nerve. In most cases, this radiating pain is caused by lumbar disc herniation (LDH), a condition where the intervertebral disc protrudes and compresses adjacent nerve roots. 1 The lifetime incidence of sciatica ranges between 13% and 40%. 2
Approximately 85% of patients with LDH receive non-surgical treatment. However, patients with persistent symptoms often require surgery. Surgical options for a lumbar discectomy include open microdiscectomy, tubular discectomy and full endoscopic procedures.3,4 Yet, even after successful initial lumbar discectomy, a subset of patients presents with recurrent symptoms. 5 However, the diagnosis of Recurrent Lumbar Disc Herniation (RLDH) remains subject to debate.
Clinicians often encounter ambiguity regarding the classification of RLDH. Currently, various definitions have been proposed for RLDH, leading to significant inconsistency in the literature. Some authors strictly define RLDH as a new herniation occurring at the same level and side (ipsilateral) as the initial surgery. Conversely, other authors adopt a broader definition, including herniations on either the ipsilateral or contralateral side of the index level. 6 Furthermore, diagnostic criteria often require a postoperative pain-free interval. However, the required duration of this interval varies widely, ranging from 1 month to 6 months.7,8
Currently, this heterogeneity in definitions makes it challenging to compare outcomes across studies or develop standard treatment guidelines. Specifically, this lack of consensus limits the synthesis of Level I evidence studies regarding RLDH, as results cannot be reliably combined. A clear, uniform definition is essential to reduce misdiagnosis and improve clinical management and generalizability.
Therefore, this study aims to provide consensus on the definition of RLDH. In addition, this study evaluates the role of clinical symptoms, and imaging criteria in diagnosing RLDH as well as current treatment strategies. To achieve this, we conducted an international expert survey to evaluate various components defining RLDH.
Methods
Study Design and Survey Development
An expert survey was developed following a comprehensive review of relevant literature. A first version of the survey was presented at the 40th International Society for Minimal Intervention in Spinal Surgery (ISSMISS) in Zurich and the 2025 Dutch Spine Society (DSS) congresses, as well as through academic and personal networks.
Based on initial feedback, the survey was refined; specifically, a dedicated section regarding imaging criteria was integrated to improve classification. The final version of the survey was disseminated through the Dutch Neurosurgical Society (NVVN), the MaxMore newsletter and distributed among academic and personal networks. The survey was hosted via Microsoft Forms.
Respondents
The study targeted clinicians with specific expertise in spinal disorders. This included spine surgeons, neurosurgeons, orthopedic surgeons, neurologists, and other specialists involved in the diagnosis and treatment of LDH.
Ethical Considerations
Because this study involved a survey of professionals and did not involve patient data or interventions, formal ethical approval was not required. Participation was voluntary and providing contact information was optional.
Survey Structure
The final questionnaire consisted of five sections: 1. Core Definitions: Assessing expert agreement on key definitions of RLDH. 2. Clinical and Surgical Considerations: Exploring factors that influence diagnosis and surgical management. 3. Classification Dimensions: Identifying parameters essential for a standardized classification system. 4. Imaging Criteria: Exploring the role of imaging in diagnosing RLDH. 5. Respondent Characteristics: Collecting demographic and professional background data.
The complete survey can be found in Appendix I. The survey included both categorical variables (e.g., specialty, geographic region, surgical preferences) and ordinal variables derived from Likert-scale items assessing agreement with diagnostic and clinical statements. Likert-scale responses were measured on a 5-point scale ranging from “strongly disagree” (1) to “strongly agree” (5). For consensus analysis, responses were dichotomized into agreement (“agree” and “strongly agree”) vs non-agreement, in accordance with predefined thresholds.
Data Collection
The survey was available online from October 2025 – February 2026. We utilized Microsoft Forms to record responses automatically. None of the questions were required to fill in. All imaging related questions reflected expert opinion rather than direct imaging analysis. We did not collect any personally identifiable information, with the exception of optional email addresses.
Statistical Analysis
Data were exported to Microsoft Excel and subsequently imported into R (version 4.2.2) 9 for analysis. Descriptive statistics were used to summarize the data; categorical variables were reported as frequencies and percentages. Consistent with current literature, consensus for Likert scale items was defined a priori as an agreement rate of ≥70% (combining ‘agree’ and ‘strongly agree’) among respondents. 10
To evaluate the influence of respondent characteristics, subgroup analyses were performed using Chi-square tests of independence. Significant global results were followed by post-hoc analysis of adjusted standardized residuals to evaluate specific group differences. Subgroups with insufficient sample sizes (N <80) were excluded from comparative analyses to ensure statistical robustness. A Bonferroni correction was applied to all significance thresholds to ensure the statistical reliability of these multiple comparisons.
Rasch Analysis of Diagnostic Criteria
In addition to conventional consensus analyses, a post-hoc Rasch analysis was performed to evaluate whether key diagnostic statements regarding RLDH collectively measured a single underlying construct reflecting the stringency of expert definitions. Likert-scale items addressing core definitional, clinical, and imaging criteria were analyzed using a polytomous Rasch partial credit model. The lowest response category was coded as zero. Model estimation was performed using marginal maximum likelihood estimation, and person–item maps were generated using the Jamovi (version 2.6.45) 11 Item Response Theory (IRT) package.
Model fit was assessed using item fit statistics (infit and outfit mean square values), residual correlations (centered Q3 statistics), and the mean absolute deviation of Q3 (MADaQ3). Item difficulty parameters were interpreted as reflecting relative expert endorsement, with lower logit values indicating broader agreement. The Rasch analysis was exploratory and intended to complement, rather than replace, the predefined consensus thresholds used in the primary survey analysis.
Results
Respondents' Demographics
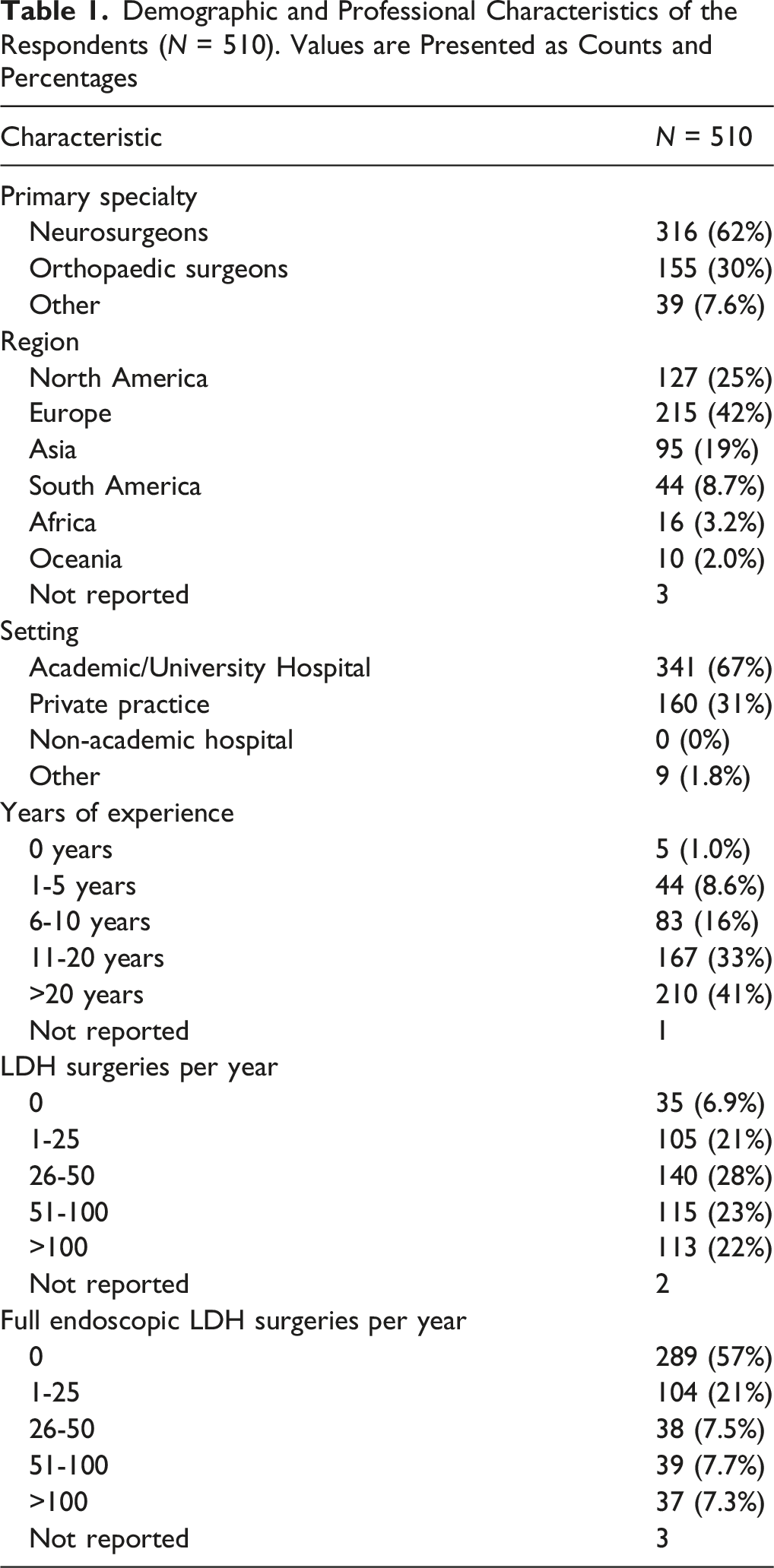
A total of 510 experts completed the survey. The majority of respondents were neurosurgeons (62%) and orthopedic surgeons (30%). Respondents represented a global sample, though most responses originated from Europe (42%) and North America (25%) (Figure 1). Global distribution of respondents (N = 510). The map illustrates the number of respondents per continent
Demographic and Professional Characteristics of the Respondents (N = 510). Values are Presented as Counts and Percentages
Core Definitions
Among the respondents, over 80% agreed or strongly agreed with the statement that RLDH is a new herniation at the same level following prior discectomy. Over 70% of respondents also agreed or strongly agreed with the statement that RLDH requires occurrence on the same level and side as the index herniation (Figure 2). Agreement on the same level and same side as index herniation in diagnosing RLDH
Furthermore, over 75% agreed or strongly agreed with the statement that a pain-free period is required. However, the single most common response regarding minimum pain-free duration was that a specific minimum interval is not required. Among those specifying intervals, the most common were 1 month, 3 months, and 1 week (Figure 3). Agreement and minimum duration for pain-free interval in diagnosing RLDH
Clinical Considerations
With regards to clinical considerations, it was found that 65.4% of respondents, agreed that symptoms of RLDH should be consistent with the operated level. Most specialists disagreed or strongly disagreed that back pain without new leg pain should be considered as a RLDH case (Figure 4). Agreement on clinical considerations in diagnosing RLDH
MRI Classification
Most experts did require an MRI to confirm the diagnosis of RLDH (96.7%). Furthermore, most experts found it important that RLDH should be clearly distinguishable from postoperative scar tissue (87.0%). No consensus was found that this distinction routinely required contrast-enhanced MRI, since 63.9% agreed or strongly agreed with this statement (Figure 5). Agreement on imaging criteria in diagnosing RLDH
Classification Dimensions
Of the respondents, 53.2% agreed that a standardized classification system is necessary. Regarding dimensions to include, location, imaging morphology, clinical presentation, and pain-free time interval were most often chosen. Number of recurrences, index procedure, and patient risk factors were less commonly chosen (Figure 6). Classification dimensions of RLDH
Surgical Considerations
The most preferred treatment was open microdiscectomy, followed by full endoscopic, fusion and tubular microdiscectomy (Figure 7). Treatment preference for RLDH; overall (A), by region (B) and by specialty (C)
Statistical analysis revealed significant geographic variations in the preference for surgical techniques (
Furthermore, the preference of surgical intervention for RLDH significantly differed based on the surgeon’s primary specialty (
Rasch Analysis of Diagnostic Criteria
Rasch analysis demonstrated acceptable global model fit (MADaQ3 = 0.086, P < 0.001), supporting unidimensional measurement of a latent construct representing the stringency of expert definitions of RLDH. Person reliability was modest (0.41), reflecting tight clustering of respondents and high conceptual agreement among experts rather than measurement instability. While most statements showed acceptable statistical fit, the item considering RLDH based on back pain without radicular symptoms was weakly associated with the latent construct and poorly targeted to the expert responses. Detailed results of the Rasch analysis are provided in the Appendix (Appendix: Table C-D; Appendix: Figure A-B).
Discussion
In summary, most respondents agreed that RLDH is defined as a new herniation occurring at the same level and on the same side as the initial herniation with confirmation on MRI clearly distinguishable from postoperative scar tissue. Moreover, most experts agreed that there must be a pain-free period after the first surgery, although the exact minimum duration remains undefined. The requirement that symptoms must match the operated level did not meet the strict 70% threshold, although it gained substantial majority support (65.4%); back pain alone, without pain radiating into the leg, was not considered a recurrence. Based on current literature and the responses of this international survey, we suggest the diagnostic algorithm for RLDH, presented in Figure 8. Diagnostic algorithm for RLDH
The strong agreement on the same level and side criterion likely reflects the surgical complexities inherent to reoperation. A recurrent herniation on the same side (ipsilateral) forces the surgeon to operate through scar tissue and altered anatomy. In contrast, a herniation on the opposite side allows the surgeon to work through relatively untouched tissue planes, similar to a first-time surgery. Therefore, the distinction is clinically important: operating on the same side may be technically more difficult and carries higher risks than operating on the opposite side.12,13 A reason why some experts believe that the contra-lateral side should also be considered RLDH may be that it is possible that during initial discectomy the disc on the contra-lateral side was damaged, then fragments in the disc could protrude from this damaged site and cause symptoms on the opposite side. 10 Nevertheless, the majority of experts believe that RLDH appears ipsilateral.
The consensus that a pain-free interval is required might be that this interval helps distinguish between a RLDH and residual disc material. If there is no period of relief, the persistent pain suggests that herniated material is still present and the nerve was never fully decompressed. 14
A major finding of this survey was the high agreement on the need for MRI confirmation, specifically to tell the difference between recurrent disc material and postoperative scar tissue (epidural fibrosis). This distinction may be vital for choosing the right treatment. Surgeons may be reluctant to operate on scar tissue alone because the results are often poor. 15 Unlike a herniation, scar tissue often adheres to the nerve and removing this scar tissue carries a higher risk of dura tears. 16 In addition, previous research suggests that while scar tissue is visible on scans, it is not always the cause of pain. 17 Therefore, surgery solely to remove scar tissue is generally discouraged.
Interestingly, the statement that contrast-enhanced MRI is routinely necessary reached only 63.9% agreement, failing to meet the consensus threshold. This suggests that while differentiating recurrent disc from scar tissue is mandatory, a substantial proportion of experts believe this can often be achieved without contrast enhancement in modern clinical practice. This is in line with previous research that shows that routine gadolinium-enhanced MRI is unnecessary, as T2-weighted imaging alone provides highly accurate diagnosis of RLDH. Furthermore, the rationale for gadolinium use is that scar tissue typically enhances after contrast injection while RLDH does not. However, this enhancement pattern is inconsistent. Early scar tissue may not enhance, and mature scar tissue (>9 months) similarly may fail to show enhancement. Additionally, some disc material may still exhibit enhancement, meaning that relying on the absence of enhancement as a diagnostic criterion for RLDH may lead to misdiagnosis. 18
The lack of consensus regarding recurrent radicular leg pain consistent with the operated level may stem from experts accounting for the potential vertical (cranial – caudal) migration and horizontal (central, paracentral, subarticular, or foraminal) migration of herniated material, which can result in compression of different nerve roots. For instance, a paracentral herniation at the L4-L5 level, typically associated with L5 radiculopathy, may migrate cranially and compress exiting nerve root L4, leading to a different clinical presentation. 19
Regarding back pain, the survey results indicate that experts generally do not classify cases as RLDH when radiating leg pain is absent. This clinical consensus is corroborated by the Rasch analysis, which identified the back pain without radiating leg pain item as being misaligned with the core diagnostic construct. This finding likely reflects the fact that low back pain without radiation suggests a broad differential diagnosis unrelated to spinal nerve root compression. 20
From a surgical point of view, open microdiscectomy is the dominant surgical technique for RLDH globally. However, our results highlight interesting geographic differences. North American respondents showed a significantly higher preference for tubular microdiscectomy, while European respondents heavily favored standard open microdiscectomy. Conversely, Asian respondents were significantly more likely to prefer full-endoscopic discectomy. This divergence may be attributed to the superior endoscopic training infrastructure in Asia, where these techniques are frequently integrated into national core curricula. By comparison, Europe and North America lack widespread accredited endoscopic fellowships, often leaving surgeons dependent on short-term, industry-sponsored courses. 21
In addition, surgical background played a significant role; neurosurgeons demonstrated a clear preference for open microdiscectomy, while orthopedic surgeons were more inclined towards full endoscopic techniques. The reason neurosurgeons prefer open microdiscectomy could be that, in contrast to orthopedic surgeons, most neurosurgeons are more experienced and comfortable using a microscope but may have less familiarity with endoscopy. 22 Meanwhile, orthopedic surgeons may prefer the full endoscopic approach because they have more familiarity with operating endoscopically. 23
Furthermore, the specific lower preference for full endoscopic techniques compared to open microdiscectomy may also stem from implementation challenges associated with endoscopic spine surgery, including a high learning curve, high start-up costs, and lower reimbursement rates.24,25
Consensus on a standardized classification system did not reach the consensus threshold (53.2%) albeit that pain-free interval, anatomical location, imaging morphology, and clinical presentation were considered as the most important dimensions in the classification of RLDH. Consequently, at this stage we do not propose a rigid classification based on these results.
By resolving the diagnostic variability with regards to RLDH, the consensus definition suggested in this study may serve as a critical foundation for standardizing future research protocols. This definition enables valid cross-study comparisons and facilitates uniform inclusion criteria for prospective clinical trials.
The primary strength of this study is the substantial sample size (N = 510). This large sample size, combined with a broad global distribution across multiple continents, enhances the external validity and generalizability of the findings. Furthermore, the inclusion of both neurosurgeons and orthopedic surgeons ensures a multidisciplinary perspective on RLDH.
This study is subject to several limitations. First, in accordance with the American Association for Public Opinion Research (AAPOR) standard definitions, calculation of a conventional response rate was not methodologically appropriate, as non-probability sampling was employed, and the total sampling frame could not be defined. 26 Second, the section regarding MRI criteria was integrated after the initial data collection phase, resulting in a lower number of responses for these specific items. Third, as with all expert surveys, the results represent Level V evidence (expert opinion) and reflect current practice patterns rather than empirically derived clinical outcomes. Fourth, the multidisciplinary composition of respondents may introduce variability in perspectives, as different specialties may approach diagnosis and management differently. However, this diversity was intentional and reflects real-world clinical practice, where RLDH is evaluated and treated across multiple specialties. Future studies may benefit from targeted inclusion of radiologists to further refine imaging-related consensus. Finally, while the global cohort was large, participation from South America, Africa, and Oceania was limited. This could limit the global generalizability of the findings to these specific regions.
A critical area for future investigation involves the comparative efficacy of surgical approaches for RLDH. In this study, the majority of respondents preferred open microdiscectomy. However, from an anatomical perspective, transforaminal approaches may be more advantageous after open surgery because they utilize a trajectory through virgin tissue planes. By avoiding the manipulation of scar tissue, the transforaminal method could theoretically be considered advantageous compared to open microdiscectomy. Given the current lack of large randomized controlled trials for RLDH, future multicenter randomized clinical trials are needed to determine whether transforaminal endoscopic lumbar discectomy is indeed superior to the gold-standard open technique.27,28
Conclusion
This study provides the basis for an international consensus definition of RLDH being a new herniation occurring at the same level and side as the initial herniation, with a pain-free interval and MRI confirmation with differentiation from postoperative scar tissue. The significant geographic and specialty-based variations in surgical preference underscore the need for standardized research protocols to improve the generalizability of clinical outcomes globally.
Supplemental Material
Suppplemental Material - Defining Recurrent Lumbar Disc Herniation (RLDH): An International Survey Study
Suppplemental Material for Defining Recurrent Lumbar Disc Herniation (RLDH): An International Survey Study by Jayant S. Harhangi, Annegien Boeykens, Ellianne J. Dos Santos Rubio, Christian Morgenstern, Benedikt W. Burkhardt, Girish Datar, Kai-Uwe Lewandrowski, Biswadjiet S. Harhangi in Global Spine Journal
Supplemental Material
Suppplemental Material - Defining Recurrent Lumbar Disc Herniation (RLDH): An International Survey Study
Suppplemental Material for Defining Recurrent Lumbar Disc Herniation (RLDH): An International Survey Study by Jayant S. Harhangi, Annegien Boeykens, Ellianne J. Dos Santos Rubio, Christian Morgenstern, Benedikt W. Burkhardt, Girish Datar, Kai-Uwe Lewandrowski, Biswadjiet S. Harhangi in Global Spine Journal
Footnotes
Acknowledgments
The authors would like to thank all spine surgeons and specialists who participated in this international survey.
Ethical Considerations
This study involved a survey of spine professionals. No patient data were collected. Ethical approval was not required. Participation was voluntary and providing contact information was optional.
Consent to Participate
Informed consent was implied by voluntary completion of the survey. Participants were informed about the purpose of the study prior to participation.
Author Contributions
Jayant S. Harhangi: Conceptualization, Methodology, Data curation, Formal analysis, Investigation, Writing – Original Draft. Annegien Boeykens: Supervision, Investigation, Resources, Writing – Review & Editing. Ellianne J. Dos Santos Rubio: Investigation, Resources, Writing – Review & Editing. Christian Morgenstern: Investigation, Resources, Writing – Review & Editing. Benedikt W. Burkhardt: Investigation, Resources, Writing – Review & Editing. Girish Datar: Investigation, Resources, Writing – Review & Editing. Kai-Uwe Lewandrowski: Conceptualization, Supervision, Writing – Review & Editing. Biswadjiet S. Harhangi: Conceptualization, Supervision, Writing – Review & Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
AO Spine Membership
First author: Jayant S. Harhangi (Membership ID: M-090919), Last author: Biswadjiet S. Harhangi (Membership ID: M-042158).
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.