
Abstract
Study Design
Systematic review and meta-analysis.
Objective
To compare expandable and static interbody cages in MIS-TLIF with respect to subsidence, radiographic outcomes, fusion rates, and patient-reported outcomes.
Methods
Following PRISMA 2020 guidelines and a preregistered PROSPERO protocol, we searched PubMed/MEDLINE, Embase, Scopus, Web of Science, the Cochrane Library, and OVID through December 2025. Studies reporting clinical or radiographic outcomes of MIS-TLIF using expandable or static cages were included. Random-effects meta-analyses were performed, and risk of bias was assessed using Joanna Briggs Institute tools.
Results
Twenty-three studies encompassing 1838 patients and 2074 fused levels met inclusion criteria. Expandable cages demonstrated a lower pooled subsidence rate than static cages (12.8% vs 25.7%), representing roughly a 50% relative reduction. When subsidence occurred, its magnitude was similar between groups (5.33 mm vs 4.54 mm). Improvements in VAS back pain (4.27 vs 4.29), VAS leg pain (3.80 vs 4.28), and ODI (20.16 vs 28.29) were comparable. Sensitivity analyses limited to low-risk studies showed consistent trends, although Egger’s regression suggested possible small-study effects for subsidence.
Conclusions
In MIS-TLIF, expandable cages are associated with lower subsidence rates while achieving radiographic and clinical outcomes similar to static cages. However, only three studies directly compared the two cage types; the synthesis largely relies on indirect comparisons is susceptible to confounding. These findings should not be regarded as evidence of a causal effect of cage design.
Keywords
Introduction
Minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) has become a widely adopted surgical approach for the treatment of degenerative lumbar spine disorders, offering reduced soft-tissue disruption, lower blood loss, shorter hospitalization, and faster recovery compared with traditional open techniques, while achieving comparable fusion rates and clinical outcomes.1,2,3 Central to the success of MIS-TLIF is the selection and placement of the interbody cage, which provides immediate anterior column support, restores disc height, contributes to sagittal alignment, and facilitates biological fusion through load sharing and graft containment.4,5
Historically, static interbody cages with fixed dimensions have been the standard implants used in MIS-TLIF. However, inserting a static cage through a narrow minimally invasive corridor often requires forceful impaction and aggressive distraction, which may increase the risk of endplate violation and subsequent cage subsidence.6,7 To address these limitations, expandable cage technology was introduced. Expandable cages are inserted in a collapsed configuration and expanded in situ, theoretically reducing insertional trauma, improving endplate contact, and allowing more controlled restoration of disc height and segmental lordosis8,9
Cage subsidence remains one of the most commonly reported complications following lumbar interbody fusion, with reported rates ranging from approximately 10% to 40%, depending on implant design, patient factors, and the criteria used to define subsidence.8,10–12 Clinically significant subsidence may lead to loss of disc height, recurrent foraminal stenosis, sagittal imbalance, and, in some cases, the need for revision surgery.12–14 Given these consequences, reducing subsidence is a major objective in interbody cage design, particularly in MIS-TLIF where endplate preservation is critical.
Expandable cages offer theoretical biomechanical advantages that may mitigate subsidence, including improved endplate coverage, more uniform load distribution, and reduced peak stresses during insertion and expansion.15,16 Nevertheless, the clinical literature comparing expandable and static cages in MIS-TLIF remains heterogeneous. Most available studies are retrospective, vary widely in patient selection, surgical technique, implant design, follow-up duration, and subsidence definitions, and frequently report conflicting findings.17–19 Moreover, several recently published meta-analyses evaluating expandable vs static cages have yielded inconsistent conclusions regarding subsidence and clinical benefit, and many have pooled data across different fusion approaches rather than focusing specifically on MIS-TLIF.20–22
Given these limitations, the true impact of expandable vs static cages on subsidence, radiographic alignment, and patient-reported outcomes in MIS-TLIF remains uncertain. A focused synthesis restricted to MIS-TLIF is needed to clarify whether expandable cage technology confers meaningful advantages over static implants or whether observed differences are primarily driven by patient- or technique-related factors. Accordingly, this systematic review and meta-analysis aimed to compare expandable and static interbody cages specifically in the context of MIS-TLIF. The primary objective was to evaluate differences in cage subsidence rates and subsidence magnitude between cage types. Secondary objectives included comparison of radiographic outcomes, such as lumbar and segmental lordosis, as well as clinical outcomes, including pain and disability measures. By synthesizing the available evidence within a uniform surgical approach, this study seeks to provide spine surgeons with a clearer, evidence-based framework for cage selection in MIS-TLIF.
Methods
Protocol Registration
This systematic review and meta-analysis was conducted according to a predefined protocol registered in PROSPERO (CRD420261277207). The study was performed and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, and the completed PRISMA checklist is provided in the supplementary materials.23,24
Eligibility Criteria
We included clinical studies evaluating minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) performed for degenerative lumbar spine pathology. Eligible studies were required to clearly specify the type of interbody cage used (expandable or static) and to report extractable data on cage subsidence and/or radiographic or clinical outcomes.
Both randomized and non-randomized comparative studies, as well as prospective and retrospective cohort studies and case series, were considered eligible, provided that preoperative and postoperative data for at least one predefined outcome were available. Studies involving non-lumbar pathology, non-degenerative indications, or fusion approaches other than MIS-TLIF were excluded unless lumbar MIS-TLIF data could be isolated. Additional exclusion criteria included cadaveric or biomechanical studies, review articles, editorials, technical notes without clinical outcomes, and conference abstracts without available full-text manuscripts. When overlapping patient cohorts were identified, only the most complete or most recent report was retained to avoid duplication.
Search Strategy
A comprehensive literature search was performed in PubMed/MEDLINE, Embase, Scopus, Web of Science, the Cochrane Library, and OVID from database inception through December 2025. The search strategy combined controlled vocabulary terms and free-text keywords related to “minimally invasive transforaminal lumbar interbody fusion,” “expandable cage,” “static cage,” “subsidence,” “radiographic outcomes,” and “clinical outcomes.” Searches were limited to English-language publications. Reference lists of eligible studies and relevant review articles were manually screened to identify additional studies. Duplicate records were removed prior to screening. Detailed search strategies for each database are provided in the Appendix.
Study Selection
All retrieved records were imported into a citation management system, and duplicates were removed. Two reviewers independently screened titles and abstracts for relevance, followed by full-text review of potentially eligible studies using the predefined inclusion and exclusion criteria. Disagreements at any stage were resolved by discussion, with a third reviewer consulted when necessary. The study selection process is summarized in a PRISMA flow diagram (Figure 1). prisma flow diagram
Data Extraction
Data extraction was performed independently by two reviewers using a standardized data extraction form. Extracted variables included study design, country, sample size, patient demographics, underlying pathology, bone mineral density (when reported), body mass index, surgical levels, cage type (expandable or static), and duration of follow-up. Radiographic outcomes, including subsidence rates, subsidence magnitude, lumbar lordosis, and segmental lordosis—were recorded using the definitions provided by each study. Clinical outcomes, including visual analog scale (VAS) scores for back and leg pain and Oswestry Disability Index (ODI) scores, were extracted when available.
When outcome data were reported as medians, ranges, or interquartile ranges, established statistical methods were applied to estimate means and standard deviations. For studies reporting multiple postoperative time points, the longest available follow-up was used for analysis. All extracted data were cross-checked for accuracy, and discrepancies were resolved by consensus.
Risk of Bias Assessment
Methodological quality and risk of bias were assessed independently by two reviewers using the Joanna Briggs Institute (JBI) critical appraisal tools appropriate for each study design, including tools for randomized controlled trials, cohort studies, and case series.25–27 Studies were categorized as having low (≥70%), moderate (50-69%), or high (<50%) risk of bias based on their overall JBI scores. Disagreements in quality assessment were resolved through discussion, with involvement of a third reviewer when required.
Data Synthesis and Statistical Analysis
Meta-analyses were performed using Comprehensive Meta-Analysis (CMA) software, version 4.0. Outcomes were pooled only when reported in at least two studies. For continuous variables, effect sizes were calculated using standardized mean differences (SMDs) with corresponding 95% confidence intervals. For dichotomous outcomes, pooled proportions were calculated. Statistical significance was defined as a two-sided P value <0.05. Heterogeneity was assessed using the I2 statistic, representing the proportion of total variability attributable to between-study heterogeneity rather than chance. I2 values were interpreted as unimportant (0-40%), moderate (30-60%), substantial (50-90%), or considerable (75-100%). 28 Given that fewer than ten studies contributed to most pooled analyses, prediction intervals were not calculated; instead, 95% confidence intervals were reported to aid interpretation. Publication bias was evaluated using Egger’s regression test when at least three studies contributed to an outcome, recognizing the limited power of this test in small meta-analyses.29–31 Outcomes reported by only a single study were categorized as single-study factors and summarized descriptively but were not included in pooled analyses.
Results
Study Selection and Characteristics
Included Studies and Features
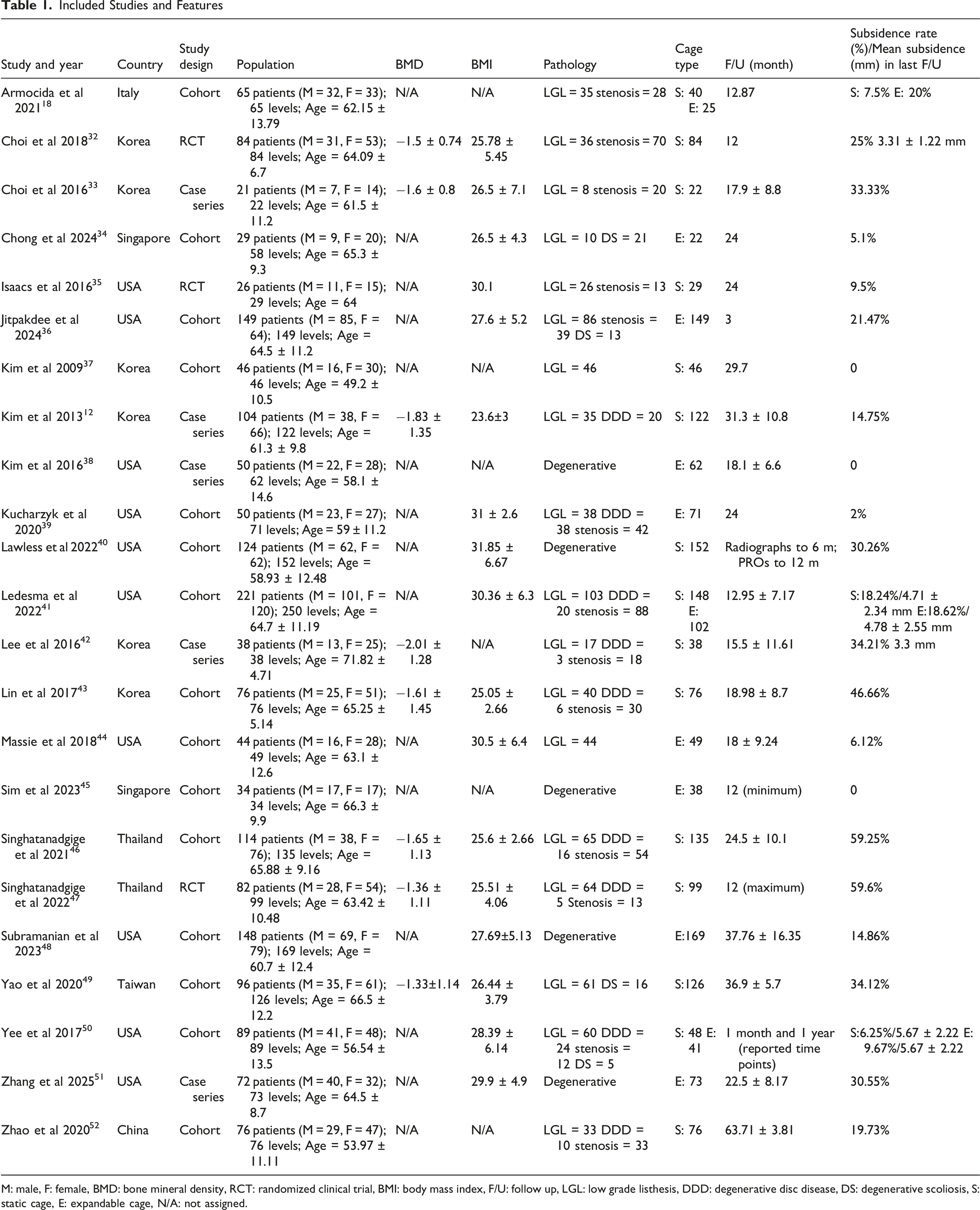
M: male, F: female, BMD: bone mineral density, RCT: randomized clinical trial, BMI: body mass index, F/U: follow up, LGL: low grade listhesis, DDD: degenerative disc disease, DS: degenerative scoliosis, S: static cage, E: expandable cage, N/A: not assigned.
Primary Outcome: Cage Subsidence
Results of Meta-Analysis for Subsidence and Radiologic and Patient-Reported Outcomes in MIS TLIF


summary of percentage changes in all outcomes: Expandable vs static cages
Among studies reporting subsidence magnitude, the mean depth of collapse was similar between cage types. Expandable cages demonstrated a pooled mean subsidence of 5.33 mm, compared with 4.54 mm for static cages, indicating that when subsidence occurred, its severity was comparable across devices (Table 2).
Radiographic Outcomes
Preoperative global and segmental lumbar lordosis were similar between expandable and static cage cohorts. Both cage types were associated with postoperative improvement in lumbar and segmental lordosis (Figure 3). Expandable cages demonstrated numerically greater mean improvements in both global and segmental lordosis; however, confidence intervals overlapped substantially, and heterogeneity was high. As such, no definitive radiographic superiority of either cage type could be established based on the pooled data (Table 3). comparison of radiographic outcomes: Lumbar and segmental lordosis between expandable and static cages the Joanna Briggs Institute (JBI) Tool for Case Series

Patient-Reported Outcomes
Both expandable and static cages were associated with substantial and clinically meaningful improvements in patient-reported outcomes. Postoperative axial back pain and radicular leg pain improved significantly from baseline in both groups, with nearly identical reductions in VAS scores (Figure 4). Disability, as measured by the Oswestry Disability Index, also improved markedly in both cohorts (Figure 5). Although static cage cohorts demonstrated numerically larger ODI improvements, this finding was accompanied by extreme heterogeneity and should be interpreted cautiously. Overall, pooled analyses demonstrated no consistent or clinically meaningful differences in pain relief or functional improvement between expandable and static cages. comparison of clinical outcomes: Vas pain scores comparison of clinical outcomes: Odi between expandable and static cages

Fusion Rates and Complications
Fusion rates were high for both cage types, with pooled rates exceeding 90% in both groups. Reported complication rates were low across studies and included incidental durotomy (0.76%), transient neurological deficits (0.27%) and wound infection (0.1%). Revision procedures were uncommon and were infrequently attributed directly to cage migration or subsidence.
Publication Bias and Sensitivity Analysis
The Joanna Briggs Institute (JBI) Tool for Assessing Cohorts
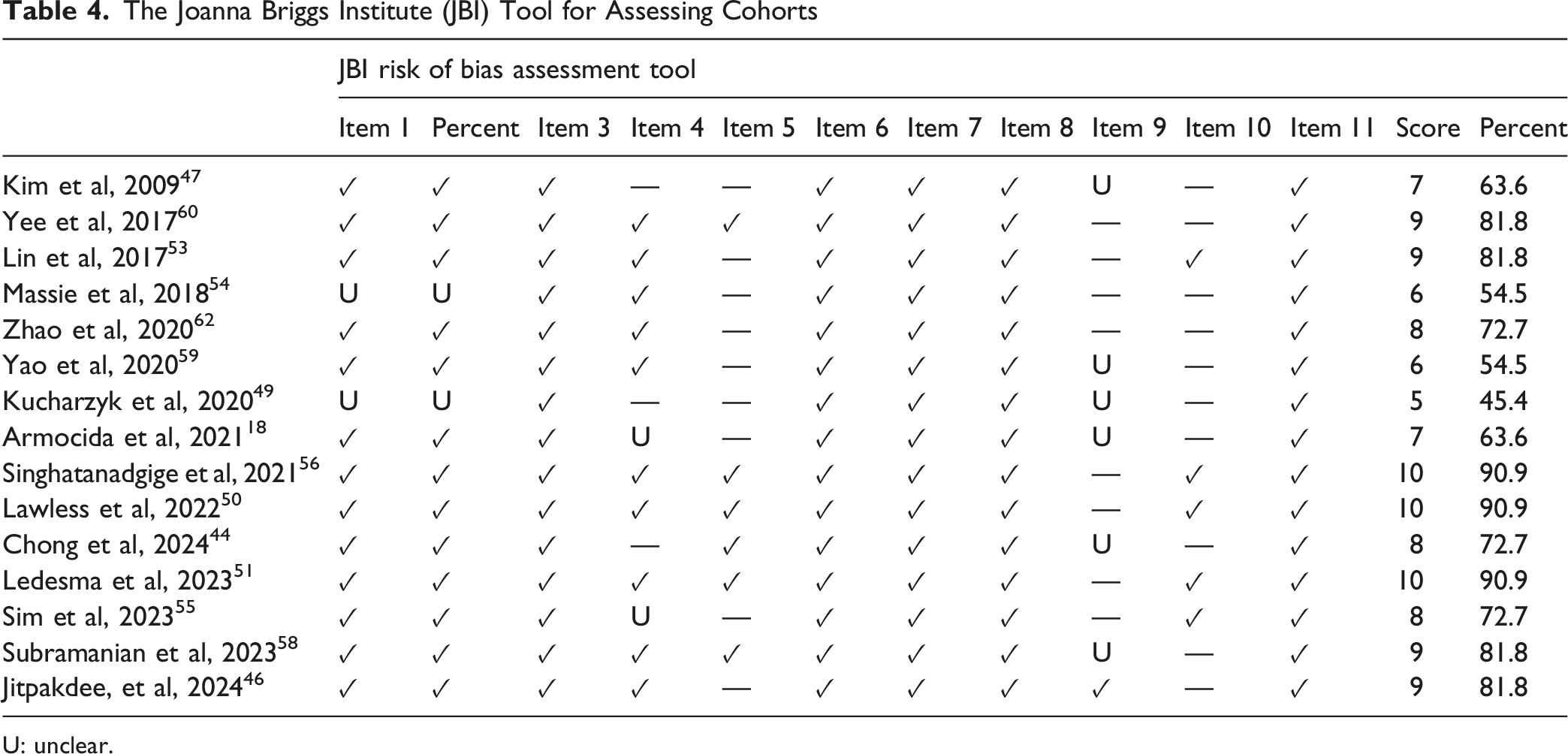
U: unclear.
The Joanna Briggs Institute (JBI) Tool for Assessing
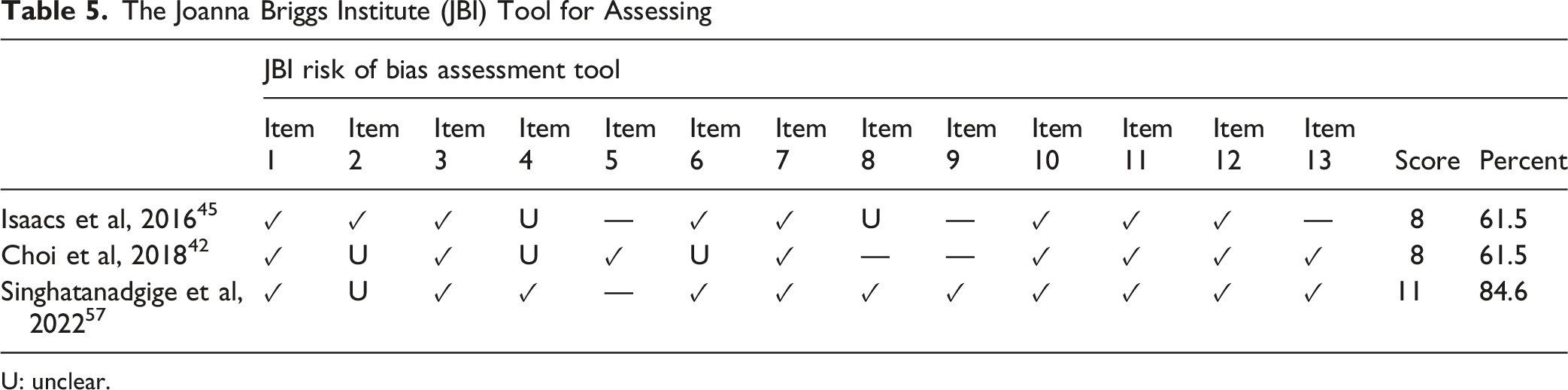
U: unclear.
Discussion
This systematic review and meta-analysis synthesized available evidence comparing expandable and static interbody cages specifically in the setting of MIS-TLIF. The principal finding is that expandable cages are associated with a lower pooled incidence of radiographic subsidence compared with static cages, while achieving broadly similar radiographic alignment, fusion rates, and patient-reported outcomes. Importantly, most observed differences arise from indirect comparisons, as only a limited number of studies directly compared both cage types within the same cohort. Consequently, these findings should be interpreted as associative rather than definitive evidence of superiority.
Cage Subsidence: Interpretation and Clinical Relevance
Cage subsidence emerged as the most consistent differentiating outcome between cage types. Expandable cages demonstrated approximately half the pooled subsidence rate observed with static cages. This finding is clinically relevant given the known associations between subsidence, disc height loss, recurrent foraminal stenosis, sagittal deterioration, and potential revision surgery.20,21 However, when subsidence occurred, the magnitude of collapse was similar between expandable and static cages, suggesting that expandable cages may reduce the likelihood of subsidence rather than its severity. Notably, the lower subsidence rates did not translate into superior pain relief, functional recovery, or higher fusion rates in the pooled analyses. This discrepancy suggests that, at the group level, the degree of subsidence captured in the included studies may not reach a threshold for clinical consequence in most patients, or that the patient-reported outcome measures were insensitive to the mechanical differences observed. Until prospective studies demonstrate that reducing subsidence with expandable cages yields a tangible clinical benefit, the practical value of this radiographic advantage remains uncertain.
The lower subsidence rate observed with expandable cages is biomechanically plausible. Importantly, the pooled subsidence rates should be interpreted with caution because the primary studies employed heterogeneous definitions of subsidence, including different radiographic thresholds (eg, any measurable migration vs >2 mm loss of disc height), imaging modalities, and follow-up intervals. This variability may influence the absolute values of the pooled rates and limit their comparability. In situ expansion allows insertion through narrower corridors with less impaction, potentially reducing endplate violation which is a key risk factor for subsidence.8,53,54 Controlled expansion may also improve endplate contact area and distribute axial loads more evenly, lowering peak stresses that contribute to cage migration.9,15,55 Nevertheless, these theoretical advantages depend heavily on surgical technique. Uncontrolled expansion, suboptimal endplate preparation, or over-distraction may negate potential benefits and contribute to early or delayed subsidence, as reported in several single-centre series.17–19
Radiographic Alignment Outcomes
Both expandable and static cages were associated with postoperative improvements in global and segmental lumbar lordosis. Although expandable cages demonstrated numerically greater mean improvements, confidence intervals overlapped substantially and heterogeneity was high. These findings suggest that cage type alone is unlikely to be the dominant determinant of sagittal correction in MIS-TLIF.
Restoration of lumbar and segmental lordosis in MIS-TLIF is influenced by multiple factors beyond cage design, including patient positioning, rod contouring, posterior instrumentation, baseline alignment, pelvic parameters, and surgical technique.56–58 In the present analysis, both cage types produced improvements, but the wide and overlapping confidence intervals, combined with high I2 values, suggest that any modest numerical differences are likely attributable to variations in surgical technique, patient selection, and measurement methodology rather than to an inherent superiority of one cage design. Therefore, attributing lordosis restoration primarily to the type of interbody device is not supported by the current data.
Clinical Outcomes and Fusion
Patient-reported outcomes improved substantially and to a similar degree in both expandable and static cage cohorts. Reductions in axial back pain, radicular leg pain, and disability were nearly identical across cage types, indicating that both technologies effectively achieve the primary clinical goals of MIS-TLIF. Although static cage cohorts demonstrated numerically larger ODI improvements, this finding was accompanied by extreme heterogeneity and likely reflects differences in study populations, follow-up duration, and baseline disability rather than a true device-related effect.
Fusion rates exceeded 90% for both cage types, consistent with prior literature demonstrating high fusion success in MIS-TLIF regardless of interbody device.8,20,21 These findings suggest that biological fusion is influenced more by surgical technique, supplemental fixation, graft material, and patient factors than by whether the cage is expandable or static. While expandable cages often feature larger graft windows, current evidence does not demonstrate a consistent fusion advantage.
Patient Selection and Surgical Implications
The observed reduction in subsidence with expandable cages may be most relevant in higher-risk populations, such as older patients, those with reduced bone mineral density, sarcopenia, or multilevel constructs, factors previously associated with increased subsidence risk.11,54,59–62 Expandable cages may offer particular benefit in these settings by minimizing insertional trauma and preserving endplate integrity. However, their use requires technical expertise and familiarity with expansion mechanics, and potential risks (including mechanism failure, incomplete expansion, or endplate fracture) must be considered. Given the absence of consistent differences in clinical outcomes, cage selection should remain individualized, taking into account patient-specific risk factors, anatomical considerations, surgeon experience, and cost. Expandable cages may be advantageous in selected cases, but static cages remain a reliable and effective option when meticulous technique is employed.
From a health-economic perspective, expandable cages are substantially more expensive than standard static cages, and their insertion requires familiarity with device-specific expansion mechanisms. The learning curve and potential for intraoperative complications such as incomplete expansion or endplate fracture must be considered. Given the absence of demonstrated superiority in pain relief, disability, or fusion rates, any decision to adopt expandable technology based solely on a reduction in radiographic subsidence should be weighed carefully against increased implant cost and technical demands. Formal cost-effectiveness analyses are lacking but would be valuable to guide resource-appropriate utilization.
Limitations
Several limitations must be acknowledged. First, only three studies directly compared expandable and static cages, necessitating reliance on indirect comparisons that are susceptible to confounding by study-level factors such as surgical technique, patient selection, and implant design. In such an analytical framework, observed associations cannot be interpreted as evidence of a causal cage-related effect. Second, substantial statistical and clinical heterogeneity was present across studies for nearly all pooled outcomes. This heterogeneity likely reflects the diversity in study designs, patient demographics, cage materials and geometries, subsidence definitions, imaging modalities, follow-up duration, and measurement methods. Third, although Egger’s regression suggested possible small-study effects for subsidence, the test has limited power given the small number of contributing studies, and publication bias cannot be excluded. Fourth, the existing clinical literature on this topic has yielded conflicting findings, with some single-center series reporting increased subsidence with expandable cages, highlighting that device design, operator experience, and patient factors interact in complex ways that aggregate data cannot fully capture. Fifth, long-term outcomes beyond two years were rarely available, and the absence of standardized radiographic and clinical endpoint definitions limits the reliability of pooled estimates. Furthermore, the absence of a uniform subsidence definition with studies using varying cut-offs, measurement methods, and imaging protocols may have introduced systematic bias into pooled rates. These limitations underscore the preliminary nature of the current evidence and should temper any direct translation of these findings into clinical practice.
Conclusion
In MIS-TLIF, expandable cages are associated with lower pooled rates of radiographic subsidence compared with static cages, while achieving similar radiographic alignment, fusion rates, and clinical outcomes. Most data are from indirect comparisons and heterogeneity across studies was substantial. Consequently, these results show an association, not a proven advantage of one cage over the other.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.