
Abstract
Study Design
Retrospective study.
Objectives
Pelvic incidence (PI) is traditionally considered a fixed anatomical parameter; however, postoperative variability has been reported in adult deformity cohorts. Data regarding PI behavior in adolescent Scheuermann’s kyphosis (SK), particularly according to deformity subtype and distal fusion level, remain limited. This study aimed to evaluate PI variability in thoracic (TSK) and thoracolumbar (TLSK) SK and to analyze its relationship with spinopelvic parameters.
Methods
102 consecutive SK patients who underwent single-stage posterior pedicle screw fusion(2015–2021) were retrospectively reviewed; 52 met inclusion criteria (TSK n=30,TLSK n=22). Thirty age-matched healthy controls were included. Radiographic parameters (TK,TLK,GK,LL,CL,PI,PT,SS,SVA,PI–LL mismatch) were measured on standardized standing whole-spine radiographs. Reliability was assessed using ICC and smallest detectable change(SDC95). Intergroup comparisons, correlation, and exploratory multivariate regression analyses were performed.
Results
Reliability for PI, PT, and SS was excellent(ICC 0.92–0.97). Preoperatively, TLSK demonstrated lower PI and SS than TSK(p<0.05). At final follow-up(mean 4.6±2.2 years), PI increased significantly in TLSK (ΔPI +6.18°), exceeding SDC95, whereas no significant change was observed in TSK. The intergroup ΔPI difference was 5.22°(p=0.050). Distal fusion(≥L3) was associated with greater ΔPI. ΔPI correlated positively with postoperative PT and SS and negatively with LL. In multivariate analysis, postoperative PT(positive) and LL(negative) remained independently associated with ΔPI (R2=0.345, p=0.001).
Conclusions
TLSK patients exhibit lower baseline PI and modest postoperative PI increase compared with TSK. Postoperative PI variability appears related to pelvic posture and lumbar alignment rather than definitive anatomical remodeling. These findings highlight the importance of comprehensive spinopelvic assessment during surgical planning and follow-up of Scheuermann kyphosis.
Keywords
Introduction
Scheuermann’s kyphosis (SK) is classically defined by the presence of ≥5° of anterior wedging in at least three consecutive vertebral bodies. 1 SK is commonly divided into typical and atypical forms. 14 The typical variant usually has an apex in the mid-thoracic region (T7–T9) and meets Sørensen’s criteria, whereas the atypical variant more often has an apex at the thoracolumbar or lumbar levels, where classic radiographic findings such as disc space narrowing, endplate irregularities, and Schmorl’s nodes may be present, although Sørensen’s criteria are not always fulfilled. 2
The balance between the pelvis and spine is essential in determining overall global spinal alignment. 15 Although pelvic incidence (PI) has traditionally been considered a fixed anatomical parameter, 6 recent studies have reported postoperative changes in PI.1,3,4 However, these observations are largely derived from adult deformity cohorts, 8 and postoperative PI behavior in adolescent SK remains unclear.10,12,17 The literature has not clearly compared thoracic (TSK) and thoracolumbar (TLSK) variants with respect to PI, and the influence of fusion extending into the lower lumbar segments remains uncertain.12,16,17 Therefore, this study aims to address this gap by evaluating PI variability across SK subtypes and its relationship with other spinopelvic parameters. While posterior spinal fusion remains the standard surgical treatment for progressive SK, motion-preserving growth-modulation approaches such as flexible posterior vertebral tethering have recently been reported, with longitudinal assessment of spinopelvic parameters (PI, PT, SS) during follow-up. 23
Material and Method
Patient Selection and Clinical Investigation
Following ethics committee approval, this retrospective single-center study was conducted at a tertiary referral spine center. A total of 102 patients with Scheuermann kyphosis who underwent single-stage posterior pedicle screw fusion between January 2015 and March 2021 were retrospectively reviewed. All surgical procedures were performed by the same spine surgery team according to standardized surgical and follow-up protocols. Inclusion criteria were: (1) diagnosis of Scheuermann kyphosis under the age of 20 according to Sorensen criteria, defined as anterior wedging of at least 5° in three or more consecutive vertebral bodies; (2) visibility of the pelvis, femoral heads, and C2 in all standing AP/lateral spine radiographs taken before and after surgery; and (3) follow-up period of at least 2 years. Exclusion criteria were postural kyphosis, congenital deformity, neuromuscular disease, previous spinal surgery (including anterior procedures), and revision surgery. Of the 102 initially screened patients, 50 were excluded. 27 patients were excluded because they did not meet the radiographic inclusion criteria required for reliable spinopelvic measurements, including incomplete visualization of the pelvis, femoral heads, or cervical spine. 17 patients were excluded because of insufficient follow-up or missing clinical/radiographic data. 6 patients were excluded because, although they had previously been diagnosed with Scheuermann kyphosis, they did not fulfill the classical Sorensen criteria. Consequently, 52 patients met all eligibility criteria and were included in the final analysis. To form the control group, thirty healthy participants were selected from our institution’s radiographic database. The control cohort was selected to match the age and sex distribution of the Scheuermann kyphosis cohort(p<0.05). These individuals had undergone full standing spinal radiography as part of routine health screening (e.g., pre-employment/occupational assessment) and only those without a known spinal deformity or history of spinal or pelvic surgery were included. To ensure comparability with the patient cohort, control radiographs were obtained using the same standardized standing lateral imaging protocol (neutral upright posture; images were repeated in case of inadequate positioning, e.g., insufficient overlap of the femoral heads). Individuals with structural spinal deformities (e.g., scoliosis or pathological kyphosis), spondylolisthesis, previous fracture/trauma sequelae, congenital or neuromuscular conditions affecting alignment, or inadequate image quality for reliable measurement were excluded from the control group.
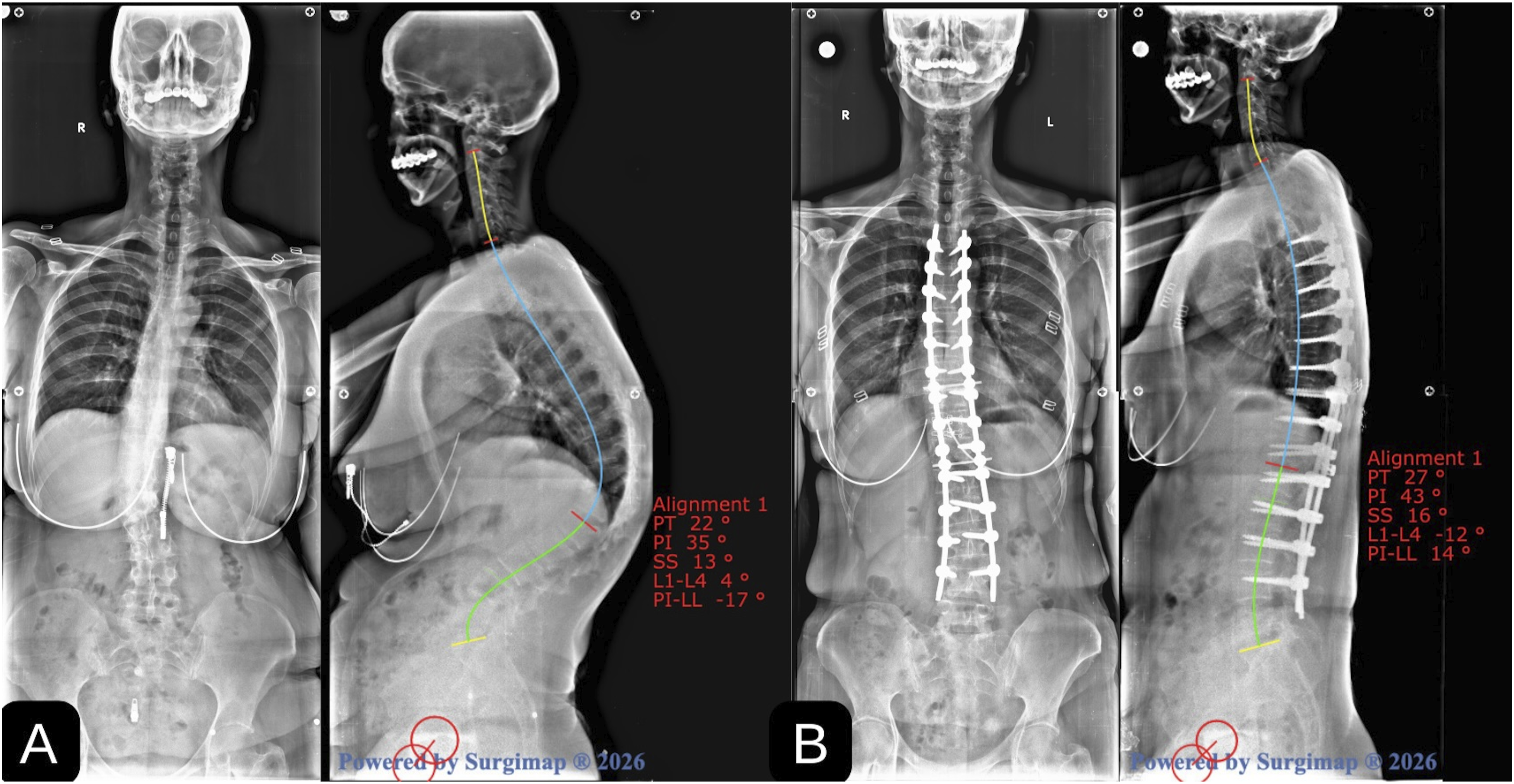
Patients were divided into two groups according to the kyphotic apex level: thoracic Scheuermann kyphosis (TSK; apex T9 or higher) and thoracolumbar Scheuermann kyphosis (TLSK; apex T10 or below) (Figures 1 and 2).
7
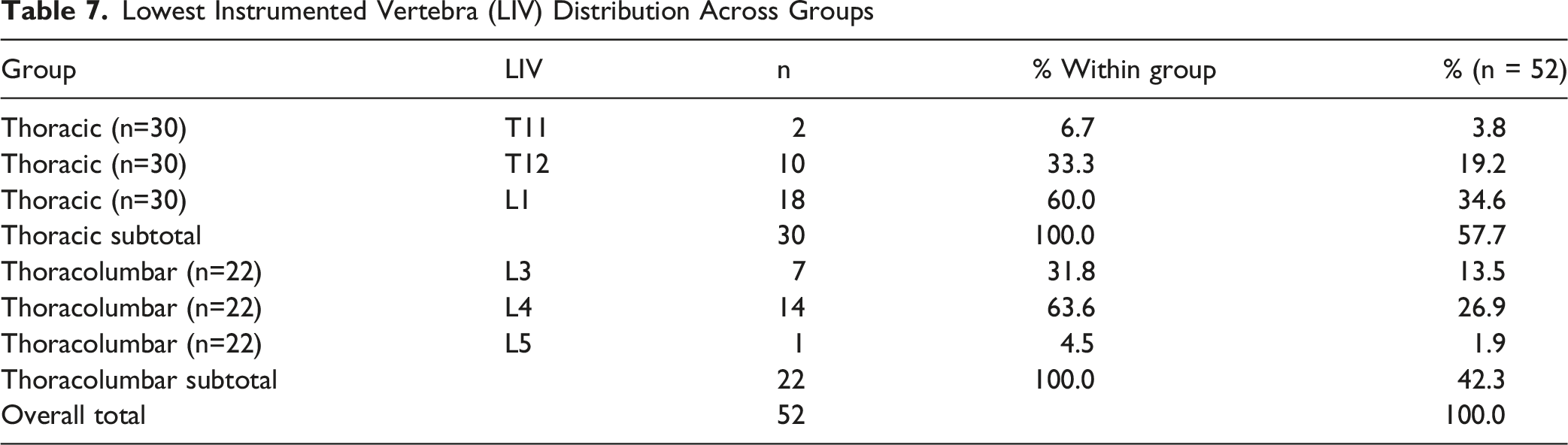
All operated patients had a preoperative global kyphosis angle greater than 70°. The lowest instrumented vertebra was selected as the sagittal stable vertebra (SSV) or SSV-1, while the upper instrumented vertebra (UIV) was chosen as the proximal end vertebra (PEV) of the kyphotic deformity. The lowest instrumented vertebra (LIV) was recorded for each patient. For secondary analyses, distal fusion was categorized as proximal LIV (L2 or higher) and distal LIV (L3 or lower), and compared between categories along with ΔPI, fusion length, and kyphosis correction magnitude. Accordingly, 30 patients were included in the TSK group, 22 in the TLSK group, and 30 in the control group. Preoperative (A) and postoperative third year (B) radiographs of a 19-year-old female with Thoracic Scheuermann Kyphosis with an apex at T9. Posterior spinal fusion (T3–L1) was achieved with use of pedicle screws and rods system Pre- (A) and postoperative third year (B) radiographs of a 18-year-old female with Thoracolumbar Scheuermann Kyphosis with an apex at T11-T12. Posterior spinal fusion (T4–L4) was achieved with use of pedicle screws and rods system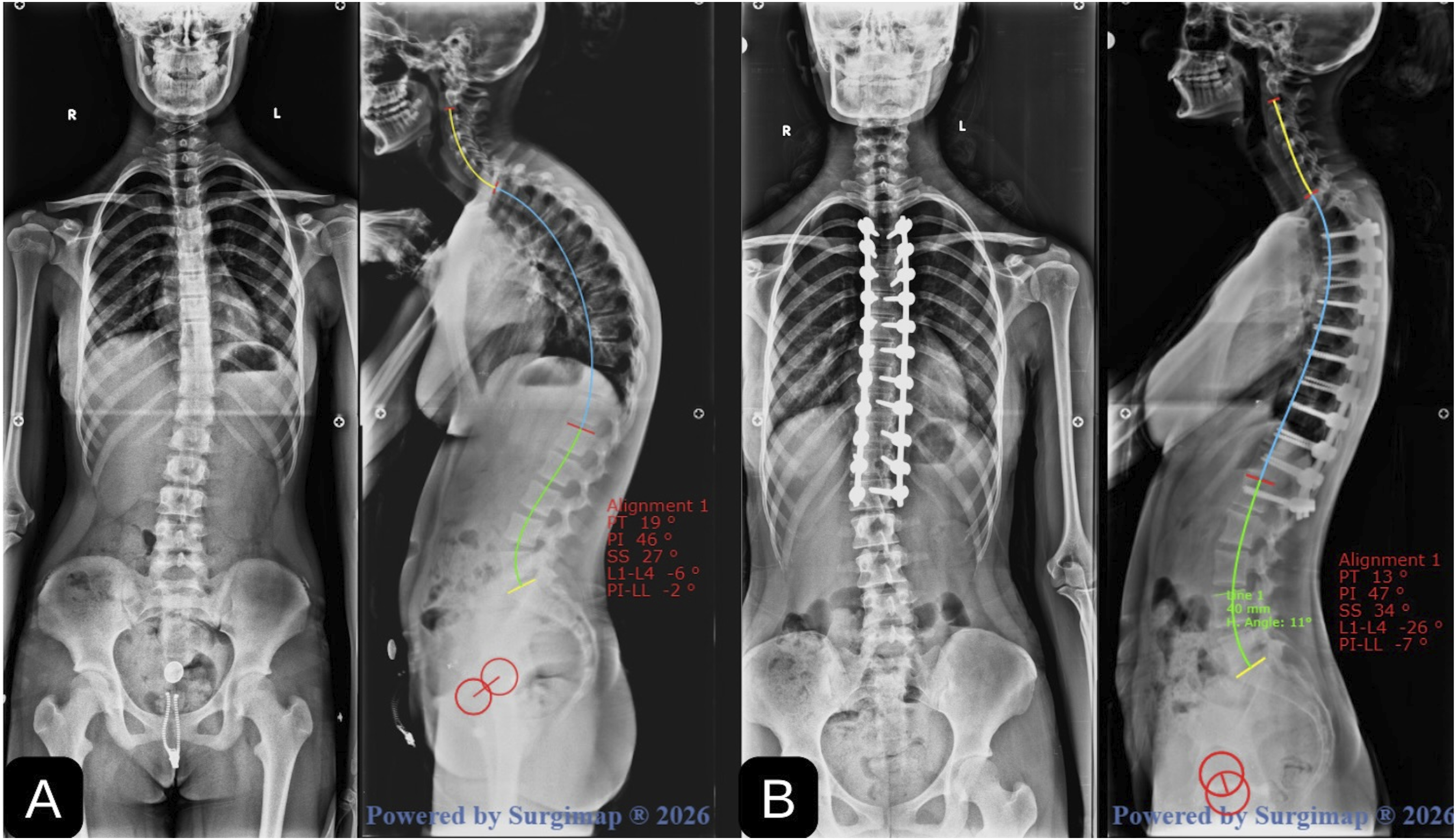
Radiological Evaluation
In the surgical group, preoperative and postoperative long-cassette standing whole-spine anteroposterior (AP) and lateral radiographs were obtained using a standardized acquisition protocol. In the control group, a single long-cassette standing whole-spine radiograph was obtained using the same protocol. Patients stood barefoot, looking straight ahead, with knees and hips fully extended; upper-extremity positioning was standardized to minimize shoulder overlap (fists on clavicles). Pelvic rotation was minimized by neutral pelvic positioning and confirmation of near-overlap of the femoral heads on lateral radiographs; images showing substantial femoral head displacement were repeated whenever possible. Radiological measurements were performed using Surgimap (Nemaris Inc., USA) and included: thoracic kyphosis (TK, T5–T12), thoracolumbar kyphosis (TLK, T10–L2), global kyphosis (GK; Cobb angle between the upper and lower end vertebrae of the kyphotic curve), cervical lordosis (CL, C2–C7), lumbar lordosis (LL, L1–S1), pelvic incidence (PI), sacral slope (SS), pelvic tilt (PT), C7 sagittal vertical axis (SVA), and PI–LL mismatch (Figure 3). Two independent spine surgeons measured PI, PT, and SS to assess inter-observer and intra-observer reliability. Intraclass correlation coefficients (ICCs), standard error of measurement (SEM), and smallest detectable change at the 95% confidence level (SDC95) were calculated and reported; observed longitudinal changes (e.g., ΔPI) were interpreted in relation to SDC95. Inter-observer ICC was calculated using a two-way random-effects model (absolute agreement), and intra-observer ICC was calculated using a two-way mixed-effects model (absolute agreement). SEM was calculated as SD×√(1−ICC), and SDC95 was calculated as 1.96×√2×SEM.
Statistical Analysis
Statistical analyses were performed using NCSS 2020 (NCSS LLC, Kaysville, Utah, USA). Continuous variables are presented as mean ± standard deviation (or median [min–max] where appropriate), and categorical variables are presented as numbers and percentages. Normality was assessed using the Shapiro-Wilk test and graphical methods. Intergroup comparisons were performed using Student's t-test for normally distributed variables, otherwise using the Mann-Whitney U test. Preoperative and postoperative comparisons were assessed using paired-sample t-tests (or nonparametric equivalents where appropriate). Categorical variables were compared using chi-square, Fisher’s exact test, or Freeman-Halton tests as appropriate. Relationships were assessed using Pearson correlation. Since pelvic incidence is geometrically related to pelvic parameters in standing radiographs (PI = PT + SS), regression models using PI as the dependent variable and including derived terms such as PT, SS, or PI-LL are mathematically cyclical; Therefore, multivariate regression analysis using PI as the dependent variable was not performed. The statistical significance level was set at p ≤ 0.05. Since this is a retrospective cohort study, no prior sample size calculation was performed, and all eligible cases were included during the study period. To provide a practical assessment of sample adequacy, a sensitivity analysis was performed using a two-sided α = 0.05 for primary group comparison (ΔPI difference between TLSK and TSK). With TLSK n=22 and TSK n=30, and using the pooled standard deviation (SD_pooled ≈ 9.23°) for ΔPI obtained from Table 4, the current sample size provides approximately 80% power to detect an intergroup difference of approximately 7.40° in ΔPI (standardized effect size d≈0.80); smaller differences may be detected with lower power. This post-hoc sensitivity analysis is provided for context only and should not be interpreted as evidence of prospective statistical power (Figures 2, and 3). Measurements of pelvic incidence (PI), pelvic tilt (PT), and sacral slope (SS)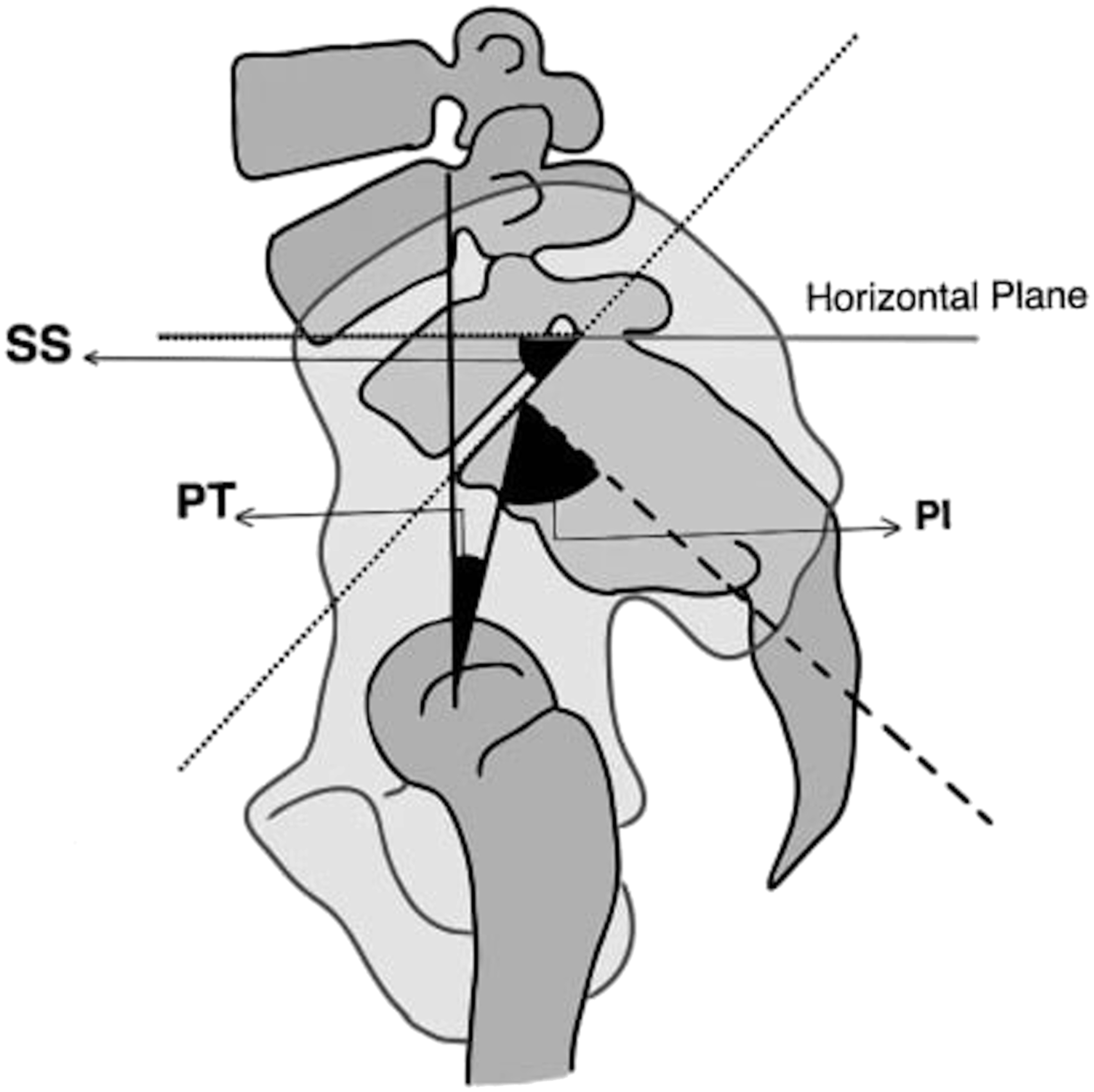
Results
Demographic and Baseline Characteristics of the Study Cohort (Operated Patients and Controls)
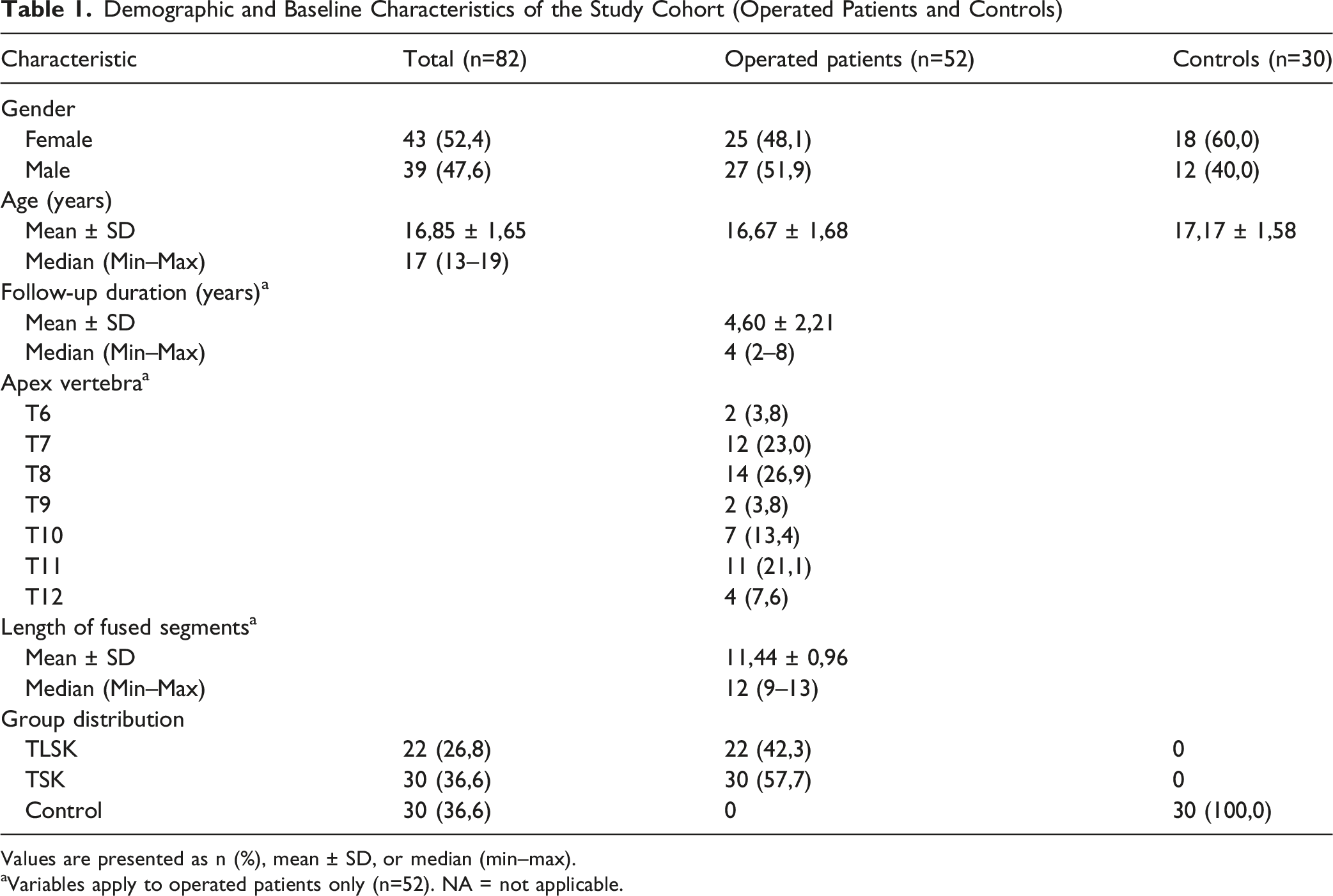
Values are presented as n (%), mean ± SD, or median (min–max).
aVariables apply to operated patients only (n=52). NA = not applicable.
Inter- and Intra-observer Reliability of Pelvic Parameters (PI, PT, SS) Measured on Standing Lateral Radiographs
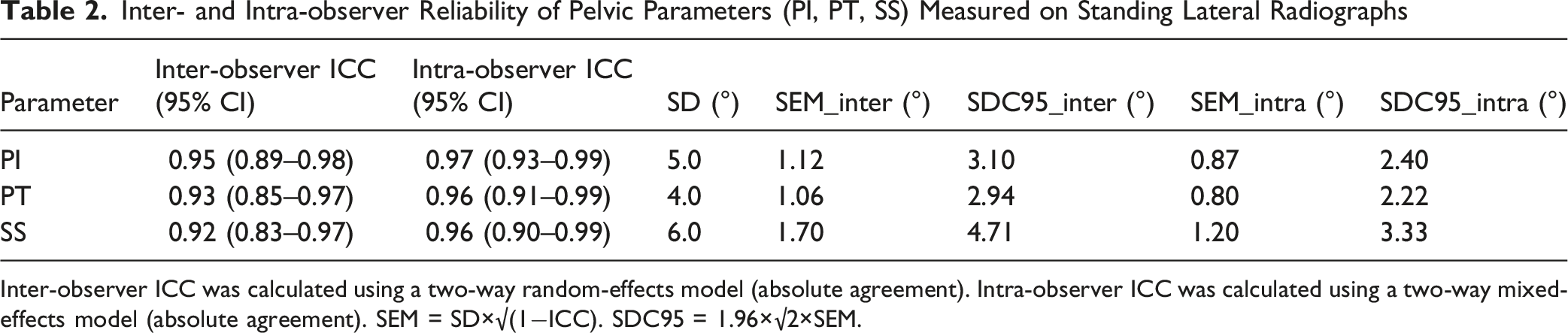
Inter-observer ICC was calculated using a two-way random-effects model (absolute agreement). Intra-observer ICC was calculated using a two-way mixed-effects model (absolute agreement). SEM = SD×√(1−ICC). SDC95 = 1.96×√2×SEM.
Comparison Between Groups
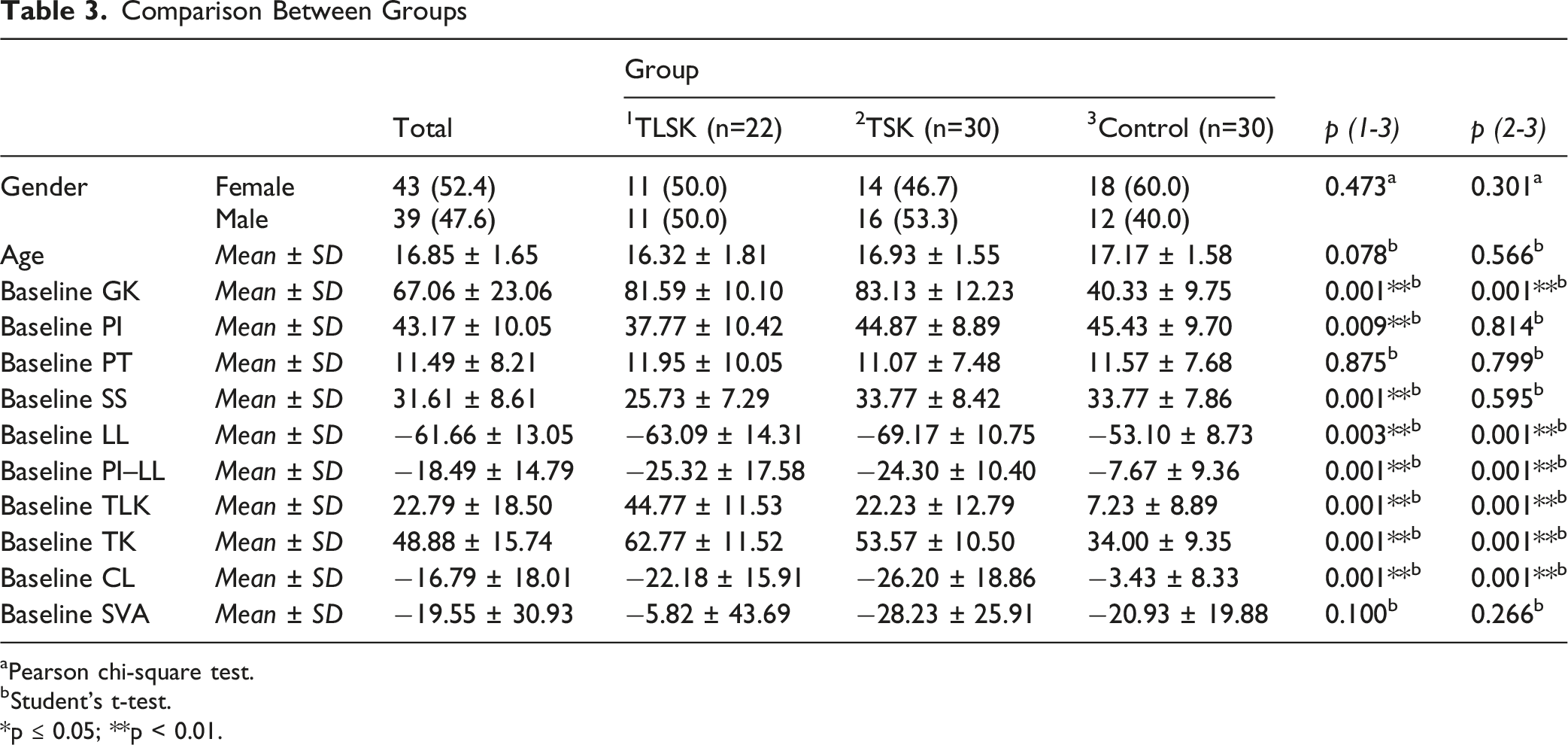
aPearson chi-square test.
bStudent’s t-test.
*p ≤ 0.05; **p < 0.01.
Preoperative, Final Follow-Up, and Change (Δ) in Spinopelvic Parameters in TLSK and TSK, Including Effect Sizes (Mean Differences) and 95% Confidence Intervals
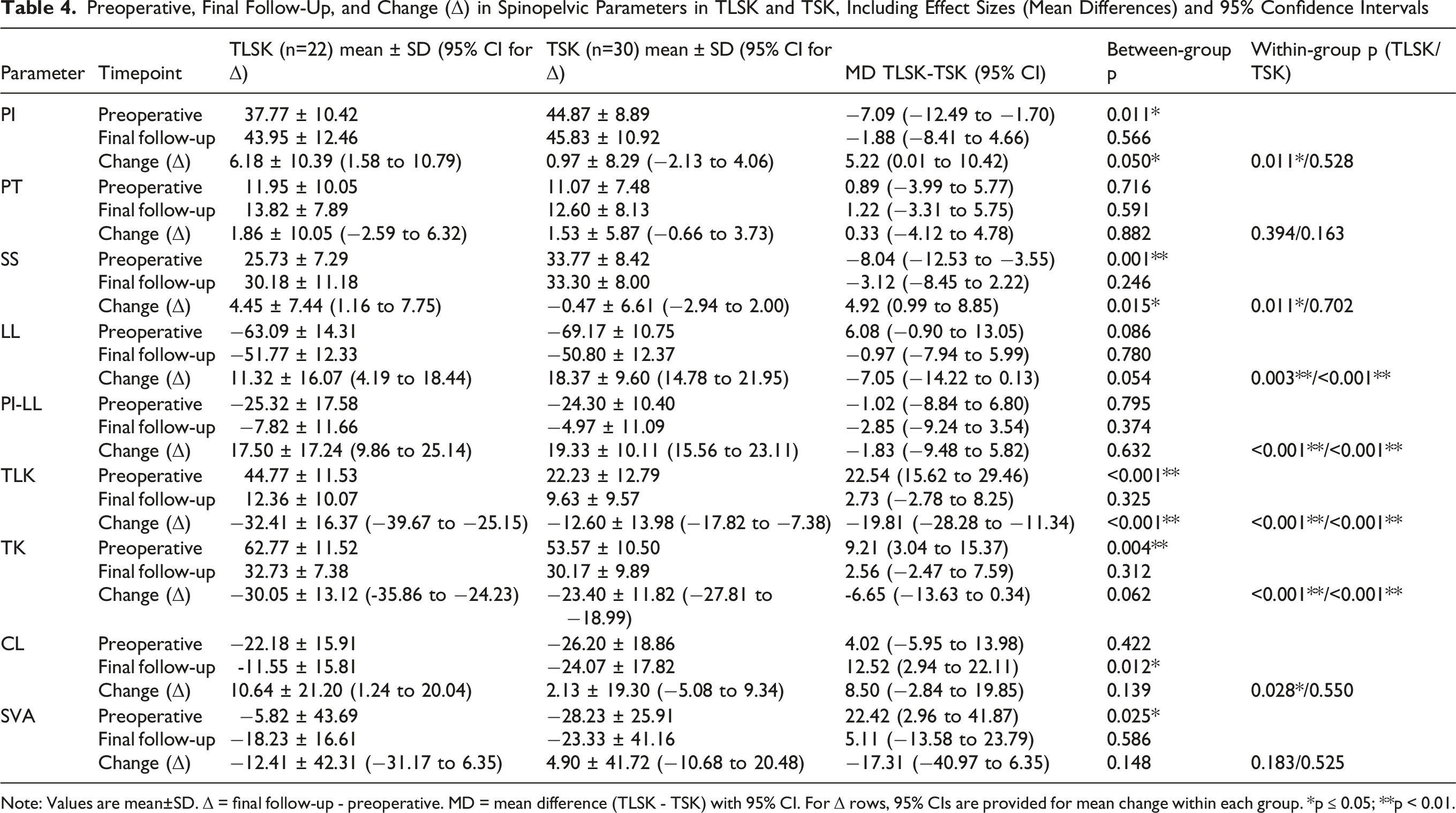
Note: Values are mean±SD. Δ = final follow-up - preoperative. MD = mean difference (TLSK - TSK) with 95% CI. For Δ rows, 95% CIs are provided for mean change within each group. *p ≤ 0.05; **p < 0.01.
Between TLSK and TSK, most sagittal parameters no longer differed at the last follow-up; However, the C2-C7 angle differed at the last follow-up (Table 4; MD 12.52°, 95% CI 2.94 to 22.11; p = 0.012), suggesting less cervical lordosis (smaller magnitude/less negative angle) in the TLSK group.
Correlation Between ΔPI and Postoperative Radiographic Parameters (Overall Cohort)
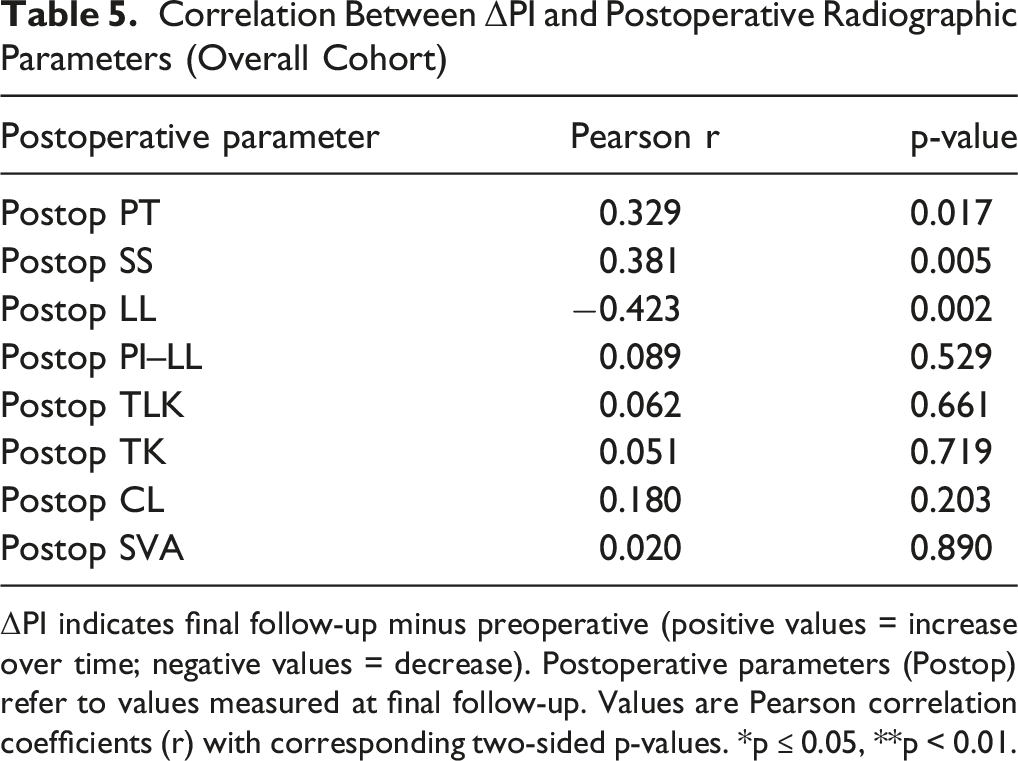
ΔPI indicates final follow-up minus preoperative (positive values = increase over time; negative values = decrease). Postoperative parameters (Postop) refer to values measured at final follow-up. Values are Pearson correlation coefficients (r) with corresponding two-sided p-values. *p ≤ 0.05, **p < 0.01.
Multivariable Linear Regression Model Predicting ΔPI
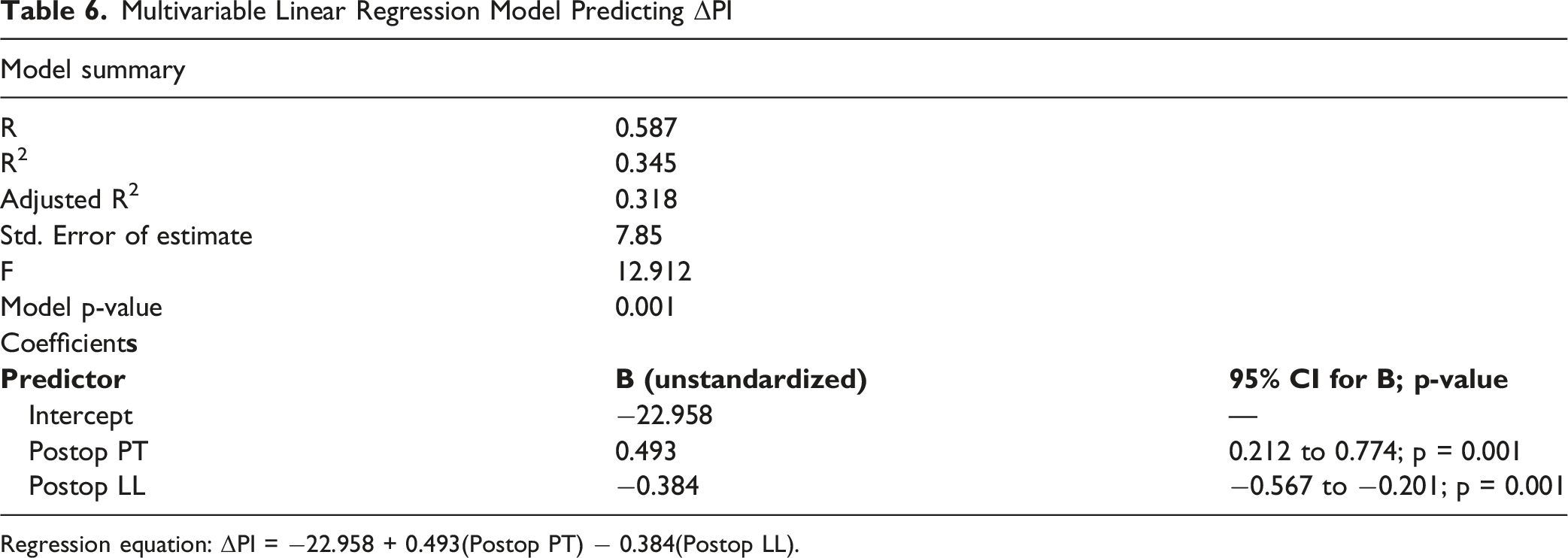
Regression equation: ΔPI = −22.958 + 0.493(Postop PT) − 0.384(Postop LL).
Lowest Instrumented Vertebra (LIV) Distribution Across Groups
Comparison by LIV Category (Proximal vs Distal)
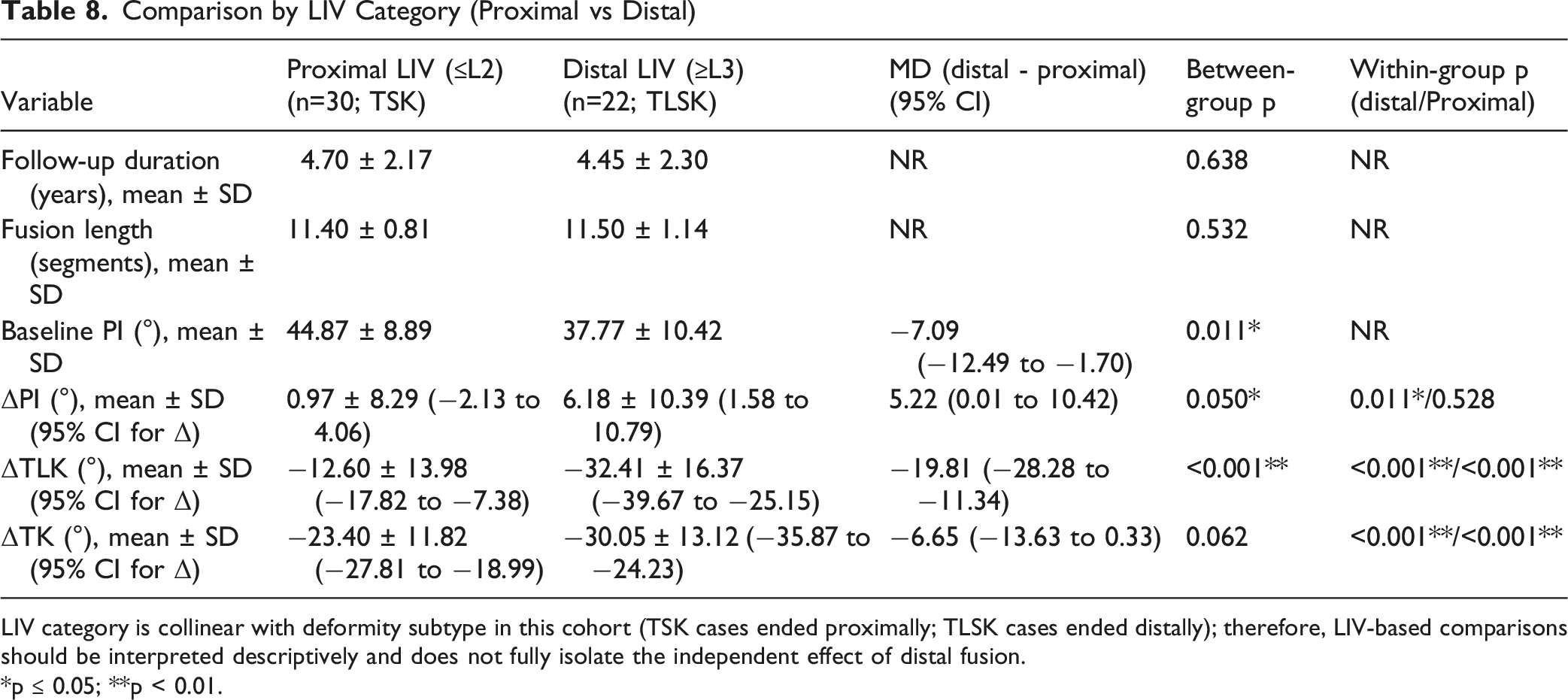
LIV category is collinear with deformity subtype in this cohort (TSK cases ended proximally; TLSK cases ended distally); therefore, LIV-based comparisons should be interpreted descriptively and does not fully isolate the independent effect of distal fusion.
*p ≤ 0.05; **p < 0.01.
The Relationship Between Preoperative to Final Follow-Up Radiological Parameters According to TLSK
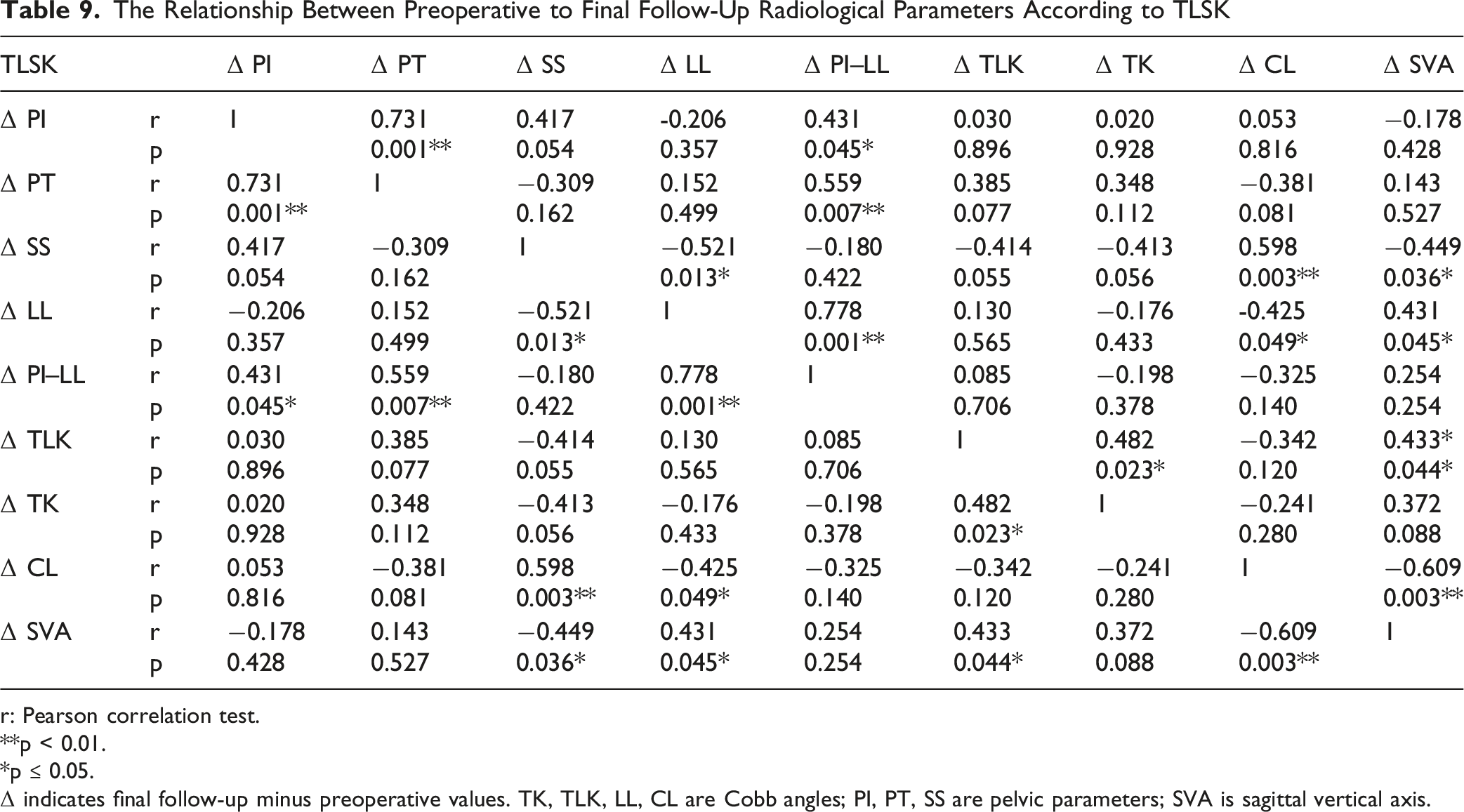
r: Pearson correlation test.
**p < 0.01.
*p ≤ 0.05.
Δ indicates final follow-up minus preoperative values. TK, TLK, LL, CL are Cobb angles; PI, PT, SS are pelvic parameters; SVA is sagittal vertical axis.
Discussion
Pelvic incidence (PI) has traditionally been regarded as a fixed parameter, yet recent studies have challenged this view.4,5,9,11 Jiang et al. 12 emphasized that spinopelvic parameters in Scheuermann’s kyphosis vary according to deformity type. In line with their findings, our study demonstrated that TLSK patients had significantly lower PI and SS values compared with TSK patients, but significantly higher TLK. They attributed these differences to rigid kyphosis and compensatory hyperlordosis, particularly in the lumbar and cervical regions. Jansen et al. 16 also reported that the rate of LL improvement was greater in TSK than TLSK, which is consistent with our observation of less lumbar hyperlordosis in TLSK cases.
Since pelvic incidence (PI) is derived from the sacral endplate and femoral head centers, small variations in pelvic rotation, beam projection, or femoral head overlap can affect the measured value and mimic true variation. In this study, radiographs were acquired using a standardized standing long-cassette protocol in a neutral upright position, and images were repeated when positioning was insufficient (including inadequate overlap of femoral heads) to reduce projection-related variability. Measurements were performed by two independent observers, and measurement reliability was quantified using intraclass correlation coefficients (ICCs); furthermore, the standard error of measurement (SEM) and the smallest detectable change at a 95% confidence level (SDC95) were calculated to support the interpretation of longitudinal changes. Using this approach, the postoperative PI increase observed in the TLSK group exceeded the SDC95, suggesting that the variation could not be explained solely by measurement error; whereas the smaller variation in the TSK group remained within the measurement error range. Notably, motion-preserving growth-modulation strategies for SK have also incorporated longitudinal spinopelvic assessment; in a recent cohort of flexible posterior vertebral tethering, global sagittal alignment improved while pelvic parameters (PI, PT, SS) remained largely stable during follow-up, suggesting that postoperative PI variability may differ by treatment strategy and/or pelvic posture during standing radiographs. 23
Pelvic incidence (PI), although traditionally considered a stable morphological parameter after growth,26,28 may appear variable postoperatively when measured on standing radiographs. 24 First, spinopelvic fixation and the lumbopelvic construct may affect measured PI by altering the relationship between the sacrum and pelvis; studies have reported PI changes after long fusions to the pelvis, and S2-alar-iliac (S2AI) fixation with corrective maneuvers may contribute to such variation. 24 In ASD patients instrumented to the pelvis with S2AI screws, clinically meaningful PI changes (≥6°) have been observed in a substantial proportion immediately postoperatively, with proposed explanations including SIJ motion, S2AI screw placement, and sagittal cantilever correction techniques. 24 Second, in adolescent patients, PI may increase during growth and maturation; large pediatric cohorts show an increase in PI across growth stages before stabilization in adulthood.25,26 Third, the postoperative definition/interpretation of pelvic parameters may change if the fusion extends to the lumbosacral junction (L5–S1), as L5 can be considered part of the pelvis (“new sacrum”) and pelvic parameters can be re-evaluated using the L5 superior endplate after a stable lumbosacral fusion. 27 Similarly, when the S1 endplate cannot be identified (e.g., lumbosacral transitional vertebrae), L5-based parameters (L5 incidence) using the superior L5 endplate have been proposed. 28
Rizkallah et al. 10 demonstrated that patients with low baseline PI (<40°) exhibited greater postoperative changes, whereas those with higher PI values showed minimal variation. Consistent with these findings, our TLSK cohort—characterized by a mean preoperative PI of 37.7°—demonstrated a significant postoperative increase. Bederman et al. 17 further suggested that in patients with low PI values, sagittal balance is maintained through adaptive changes in lumbar lordosis (LL) and pelvic tilt (PT). The postoperative increase in PI and sacral slope (SS) observed in our TLSK group supports this compensatory mechanism. While higher PI values are generally associated with greater compensatory capacity, excessively elevated PI has been linked to degenerative spondylolisthesis.18,19 Similarly, Li et al. 13 reported lower PI values (mean 35.1°) in patients with congenital or angular kyphosis secondary to tuberculosis, further corroborating our finding that TLSK patients present with inherently lower PI compared with both TSK patients and healthy controls.
We observed that both TLSK and TSK patients presented with significantly elevated preoperative TK, TLK, GK, LL, and CL values relative to controls, implying that compensatory adaptations in Scheuermann’s kyphosis primarily occur in the lumbar and cervical regions. 12 Moreover, PI and SS values in the TLSK group were significantly lower than those in both controls and the TSK group, consistent with the findings of Li et al, who reported kyphotic cases presenting with low PI values. 13 In addition, the preoperative differences observed in SVA, TK, and TLK became comparable postoperatively, highlighting the effectiveness of surgery in restoring global sagittal balance.16,21 At the final follow-up, only CL was significantly lower in the TLSK group, suggesting that thoracolumbar correction may limit the adaptive capacity of the cervical spine; similarly, Liu et al reported a tendency toward decreased cervical lordosis following thoracolumbar kyphosis surgery. 21
In the TLSK group, moderate to strong associations were identified among spinopelvic parameters (ΔPI–ΔPT, r = 0.731; ΔSS–ΔCL, r = 0.598). Specifically, ΔPI correlated positively with ΔPT, ΔSS correlated positively with ΔCL, while ΔLL correlated negatively with ΔCL. These results indicate that changes in lumbar and pelvic alignment are closely linked to compensatory mechanisms at the cervical level. Our findings are consistent with those of Ye et al., 20 who reported that increased lumbar lordosis may be accompanied by a compensatory reduction in cervical lordosis.
In our study group, postoperative variability in measured PI was associated with pelvic posture and lumbar alignment rather than behaving as a completely fixed value. ΔPI showed a weak positive correlation with postoperative PT (r = 0.329, p = 0.017) and postoperative SS (r = 0.381, p = 0.005), and a moderate negative correlation with postoperative LL (r = −0.423, p = 0.002) (Table 5). In an exploratory multivariate model using ΔPI as the dependent variable, higher postoperative PT remained independently associated with a larger ΔPI (B = 0.493; 95% CI 0.212 to 0.774; p = 0.001), whereas higher postoperative LL was associated with a smaller ΔPI (B = −0.384; 95% CI −0.567 to −0.201; p = 0.001) (R2 = 0.345; Table 6). These findings support interpreting postoperative PI changes within the broader spinopelvic chain, rather than as an isolated “predictor” of PI, especially considering the geometric linkage between PI, PT, and SS in standing radiographs. Consistent with this concept, Bederman et al. The relationships reported between PI and both LL and PT in patients with Scheuermann’s disease 17 and Nasto et al evaluated preoperative alignment parameters related to PI and LL in relation to the risk of postoperative joint kyphosis after posterior correction of Scheuermann’s kyphosis only. 22
This study has certain limitations. The retrospective design inherently carries the risk of selection bias, even though strict inclusion and exclusion criteria were applied. Additionally, the retrospective design limited the sample size to the current cohort. Furthermore, the follow-up period, while sufficient to evaluate short-to mid-term outcomes, may not fully demonstrate the long-term adaptations of pelvic incidence and sagittal balance. In addition, body mass index (BMI) data were not consistently available for the control group because the radiographs were obtained from an institutional screening database. Therefore, matching and comparison between groups with respect to BMI could not be performed and residual confounding related to body habitus cannot be excluded. These limitations should be considered when interpreting our results, and future prospective, multicenter studies with larger patient populations and longer follow-up are warranted.
Conclusion
Patients with thoracolumbar Scheuermann kyphosis demonstrated lower preoperative PI and SS values and showed a modest increase in radiographically measured PI during follow-up, whereas no significant PI change was observed in thoracic cases. Postoperative PI variability appeared to be associated with spinopelvic alignment and pelvic posture rather than definitive anatomical remodeling. These findings highlight the importance of comprehensive spinopelvic assessment during surgical planning and postoperative follow-up of Scheuermann kyphosis. Given the retrospective single-center design and relatively small sample size, the results should be interpreted as preliminary and hypothesis-generating rather than definitive evidence. Further prospective multicenter studies are required to confirm these observations.
Footnotes
Ethics Considerations
This study was approved by the Institutional Review Board of Sakarya University Faculty of Medicine (Approval No: E-71522473-050.01.04-285315). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all patients (or their legal guardians) prior to inclusion in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.