
Abstract
Study Design
Retrospective observational study.
Objectives
Degenerative spinal disease, most commonly affecting the cervical and lumbar regions, is a leading cause of disability among the elderly, with its prevalence rising globally. Although urinary dysfunction is a recognized complication, its prevalence and associated risk have not been systematically evaluated in a large-scale population-based setting.
Methods
Data from the Korean Health Insurance Review and Assessment Service were analyzed using eight annual datasets from 2009 to 2016, each representing a 3% random sample of the national population. Patients were categorized into cervical, lumbar, combined, and control groups. Meta-analysis was conducted to calculate pooled prevalence of urinary dysfunction. Multivariable logistic regression incorporating age, sex, and Charlson Comorbidity Index score was performed to estimate adjusted odds ratios, which were subsequently meta-analyzed to derive pooled effect sizes.
Results
The mean number of patients across datasets was 455,461. The pooled prevalence of urinary dysfunction was 8.7% (95% CI, 8.1–9.3%) in the cervical group, 9.1% (95% CI, 8.3–9.9%) in the lumbar group, 13.7% (95% CI, 12.8–14.7%) in the combined group, and 5.2% (95% CI, 4.8–5.5%) in controls. The pooled adjusted odds ratios were 1.58 (95% CI, 1.52–1.65) for cervical disease, 1.49 (95% CI, 1.47–1.51) for lumbar disease, and 2.24 (95% CI, 2.16–2.33) for combined disease.
Conclusions
Cervical and lumbar degenerative spinal disease are independently associated with increased urinary dysfunction risk, with the highest risk in patients with combined involvement. Clinicians should be attentive to urinary symptoms in this population, particularly when both regions are affected.
Keywords
Introduction
Degenerative spinal disease represents one of the most prevalent and burdensome musculoskeletal disorders worldwide, and the cervical and lumbar regions in particular are most commonly affected due to their greater range of motion, frequently resulting in various neurological deficits that often necessitate surgical intervention.1,2 Approximately 266 million individuals globally suffer from degenerative spinal disease and low back pain annually, with spinal stenosis alone affecting over 103 million individuals worldwide. 3 As global life expectancy continues to rise and fertility rates decline, the world’s population is undergoing a profound demographic shift toward older age groups, directly amplifying the burden of these conditions. 4 Given this trajectory, understanding the full clinical impact of degenerative spinal disease, including its effects on visceral function, is of critical public health importance.
Urinary dysfunction is an increasingly recognized but often underappreciated complication of degenerative spinal disease, affecting patients across both cervical and lumbar levels of spinal involvement. Regardless of the level of spinal pathology, compression of neural structures disrupts the intricate neurological pathways governing bladder function, including descending cortical and pontine inhibitory pathways as well as lumbosacral afferent and efferent innervation of the detrusor muscle.5–7 As a consequence, patients with degenerative spinal disease at any spinal level may present with a broad spectrum of lower urinary tract symptoms, including urinary urgency, frequency, hesitancy, incomplete bladder emptying, and urinary retention.5–14 Lower urinary tract symptoms have been reported in up to 50–60% of patients with degenerative cervical myelopathy,5,8 while voiding dysfunction has been documented in up to 73.9% of patients with lumbar spinal canal stenosis. 9 Neurogenic bladder has been urodynamically confirmed in 20–50% of patients with cervical myelopathy, 6 and bladder dysfunction in lumbar spinal stenosis may similarly progress to include recurrent urinary tract infections and upper urinary tract deterioration in severe cases. 7 Despite this high prevalence across spinal levels, urinary symptoms remain frequently overlooked in routine clinical evaluations, which tend to prioritize motor and sensory outcomes.
The shared burden of urinary dysfunction across different levels of degenerative spinal disease underscores the need for a comprehensive, population-based assessment of this association. However, the existing literature is largely limited to single-center studies, small cohorts, and selected surgical populations, precluding generalizability. To our knowledge, no large-scale population-based study has systematically examined the association between degenerative spinal disease and urinary dysfunction while distinguishing between cervical, lumbar, and combined spinal involvement. The purpose of this study was to investigate the association between degenerative spinal disease and urinary dysfunction using a large, nationwide health insurance claims database, thereby minimizing selection bias inherent to institution-based cohorts. Furthermore, we aimed to compare the risk of urinary dysfunction across three distinct groups—cervical, lumbar, and combined cervical and lumbar degenerative disease—to better characterize the overall impact of degenerative spinal disease on urinary function.
Materials and Methods
The study protocol was approved by the Institutional Review Board of Yonsei University Gangnam Severance Hospital (IRB No. 3-2018-0041). All procedures were conducted in accordance with the ethical standards of the Declaration of Helsinki and the institutional guidelines of Yonsei University.
Data Source
This study analyzed patient data obtained from the Korean Health Insurance Review and Assessment Service (HIRA). Korea maintains universal health coverage through either national health insurance or medical aid programs. HIRA evaluates and processes medical fee claims submitted by healthcare providers seeking reimbursement. The database contains de-identified patient information including demographics, diagnostic codes, and medication records. Researchers can access statistically representative sample datasets following anonymization and random sampling procedures. This investigation utilized HIRA datasets HIRA-NPS-2009, 2010, 2011, 2012, 2013, 2014, 2015, and 2016, encompassing data from 2009 to 2016. Each dataset represented a 3% random sample drawn from the total patient population for the respective year. The HIRA datasets included all individuals who sought medical care at healthcare facilities for any diagnosis or symptom. The findings presented herein represent the authors’ independent analysis of these data and do not reflect the official positions of HIRA or the Korean Ministry of Health and Welfare.
Study Population and Diagnostic Codes
The number of patients in the datasets ranged from 1,382,317 to 1,468,033, with a mean of 1,426,145 patients per dataset. To reflect the characteristics of degenerative spinal disease patients, individuals aged 49 or younger were excluded from the analysis in each dataset. Additionally, thoracic degenerative spinal disease cases were excluded due to insufficient patient numbers for statistically meaningful analysis compared to cervical and lumbar degenerative disease cases. The International Classification of Diseases, 10th Revision (ICD-10) codes for thoracic degenerative spinal disease used for exclusion are listed in Supplemental Table 1.
Following exclusion criteria, patients in each dataset were classified into four groups based on diagnostic codes: cervical group (cervical degenerative spinal disease only), lumbar group (lumbar degenerative spinal disease only), combined group (concomitant cervical and lumbar degenerative spinal disease), and control group (Figure 1). The ICD-10 codes for cervical and lumbar degenerative spinal disease are presented in Supplemental Tables 2 and 3, respectively. Patients without diagnostic codes for either cervical or lumbar degenerative spinal disease were classified as the control group. Diagram of patient group classification and patient numbers derived from nationwide Health Insurance Review and Assessment Service (HIRA) sample datasets from 2009 to 2016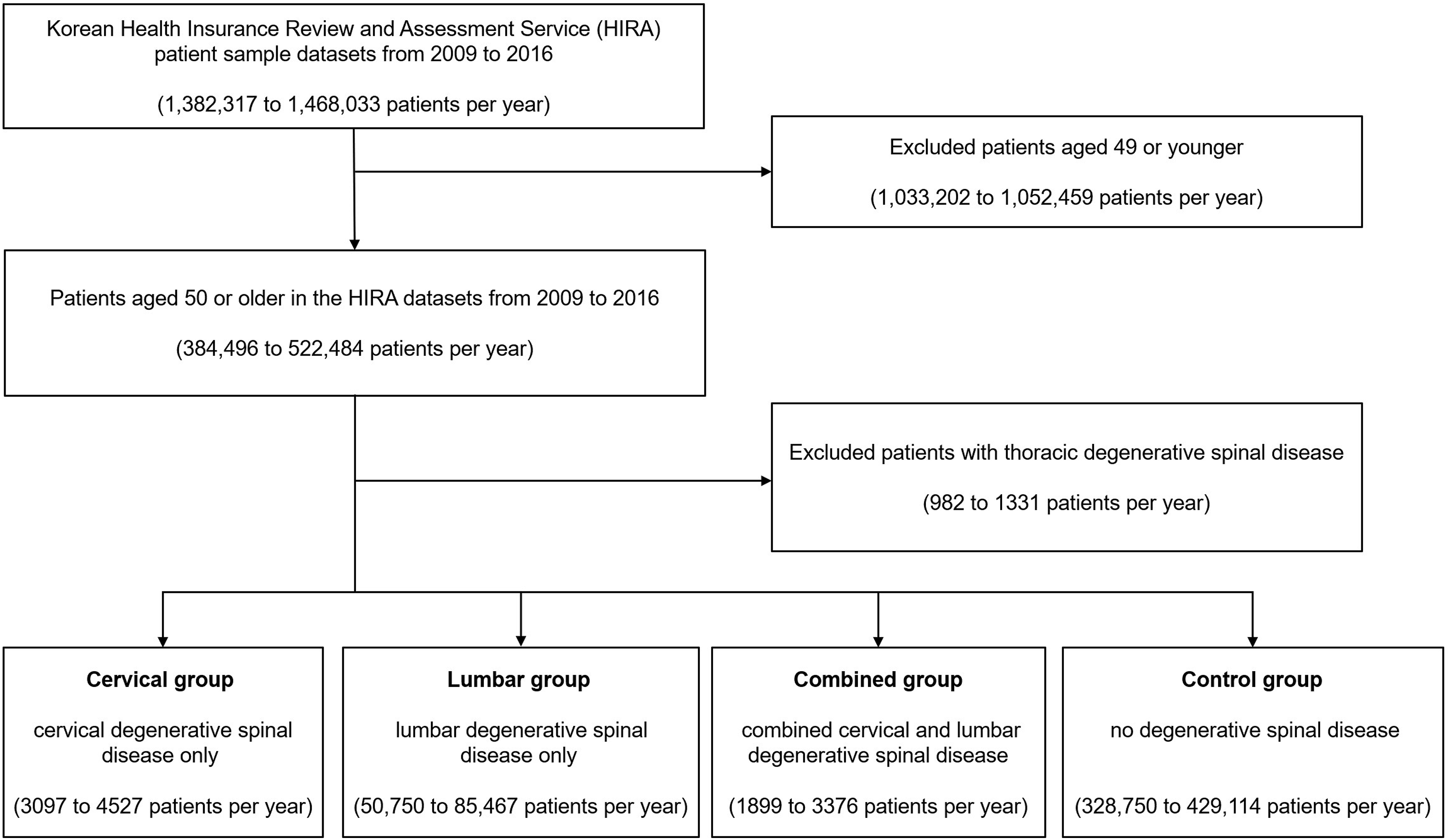
Diagnostic codes related to urinary dysfunction were selected through careful review of ICD-10 major categories G (Diseases of the nervous system), N (Diseases of the genitourinary system), and R (Symptoms, signsz and abnormal clinical and laboratory findings, not elsewhere classified), and are presented in Supplemental Table 4.
Multivariable logistic regression analysis was performed to examine the association between degenerative spinal disease and urinary dysfunction, with sex, age, and Charlson Comorbidity Index (CCI) as confounding factors, and adjusted odds ratios (aORs) were calculated. The ICD-10 codes for CCI 15 are presented in Supplemental Table 5, and scores were assigned according to each comorbidity. All diagnoses were considered present if the corresponding diagnostic code appeared in the dataset, regardless of the order of diagnosis.
Statistical Analysis
The number of patients with cervical or lumbar degenerative spinal disease and urinary dysfunction was determined in each annual dataset, and multivariable logistic regression analysis was performed to calculate aORs. Meta-analysis of the annual patient numbers and aORs was conducted to determine the pooled prevalence and pooled odds ratios of urinary dysfunction in patients with cervical or lumbar degenerative spinal disease. Statistical significance was set at P < 0.05. All statistical analyses were performed using SAS version 9.4 software (SAS Institute, Cary, NC, USA) and RStudio version 4.5.2 (RStudio Team, Boston, MA, USA).
Results
Prevalence of Urinary Dysfunction in Patients With Degenerative Spinal Disease and in the Control Group
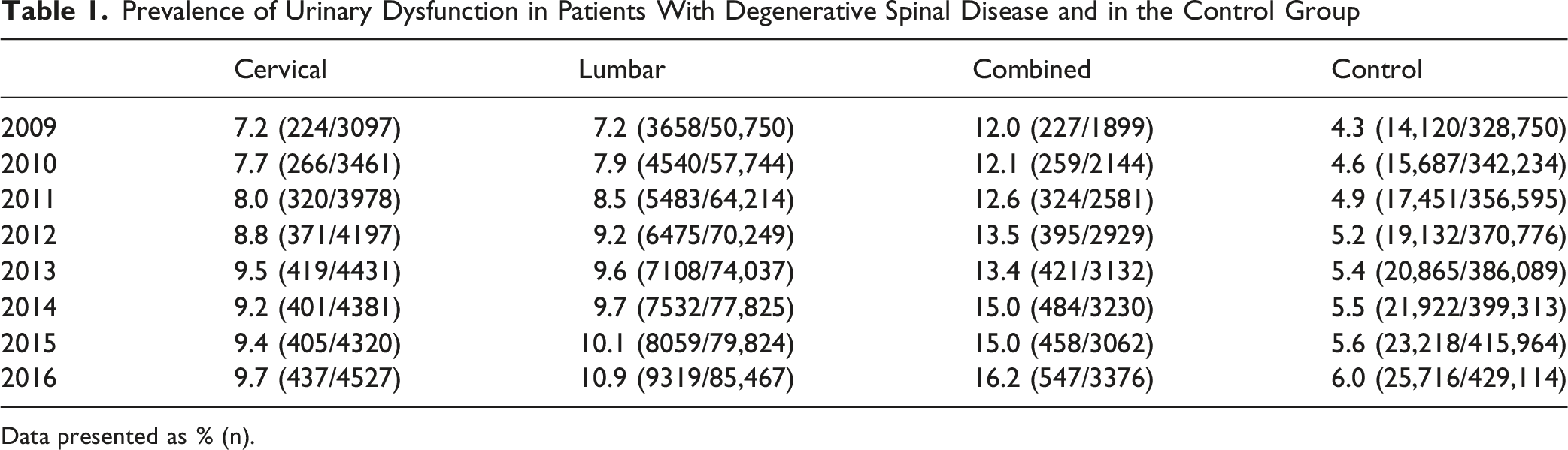
Data presented as % (n).
The forest plot of the meta-analyzed prevalence of urinary dysfunction in patients with degenerative spinal disease from 2009 to 2016 is presented in Figure 2. The pooled prevalence of urinary dysfunction was 8.7% (95% CI, 8.1–9.3%) in the cervical group, 9.1% (95% CI, 8.3–9.9%) in the lumbar group, 13.7% (95% CI, 12.8–14.7%) in the combined group, and 5.2% (95% CI, 4.8–5.5%) in the control group. Forest plots of the pooled prevalence of urinary dysfunction in patients with degenerative spinal disease from 2009 to 2016: (A) cervical, (B) lumbar, and (C) combined groups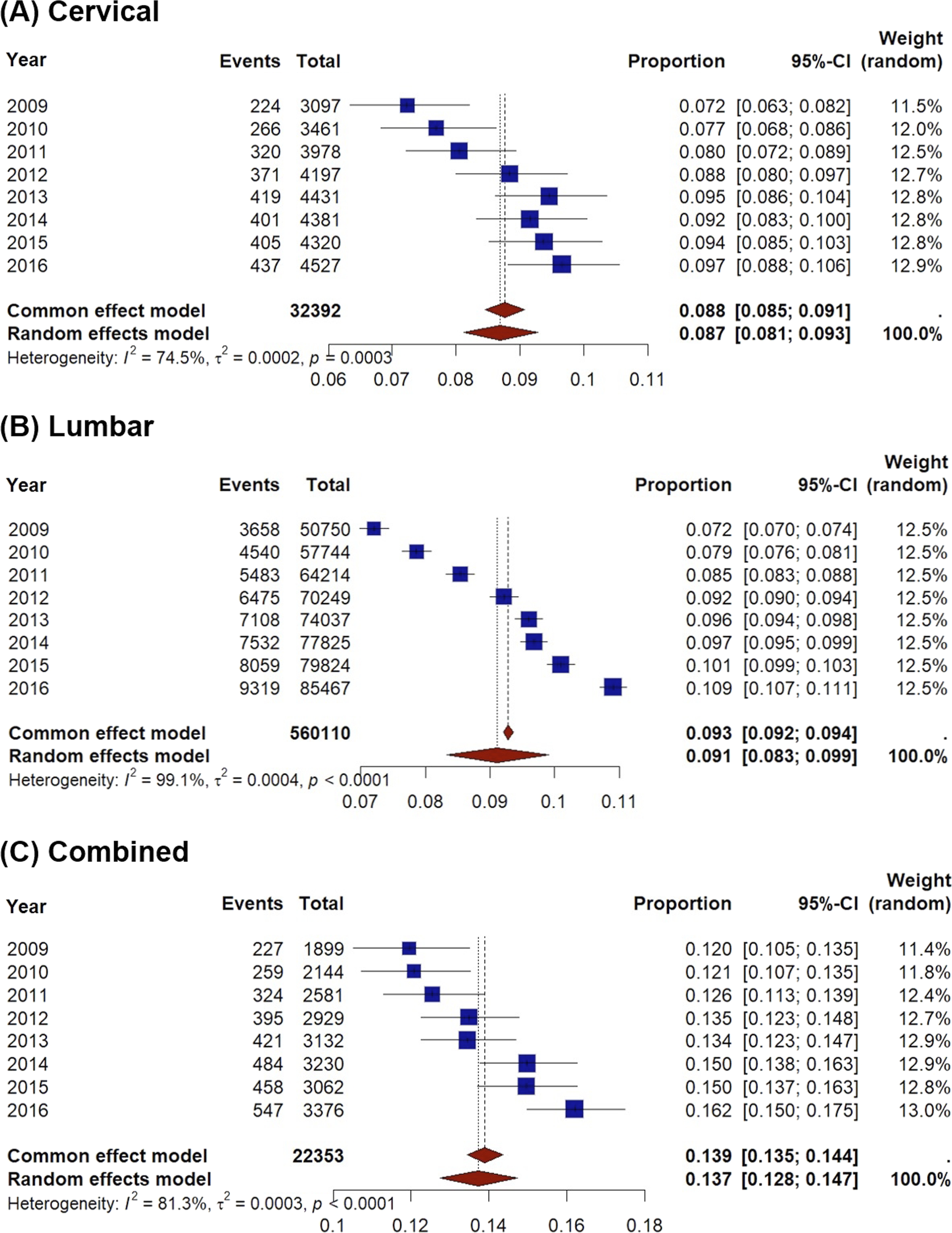
Multivariable logistic regression analysis was performed incorporating age, sex, and CCI score as confounding variables, and the adjusted aORs for each group from 2009 to 2016 were calculated. The results are presented in Supplemental Tables 6 to 8.
The aORs of urinary dysfunction for each year from 2009 to 2016 were meta-analyzed and presented as a forest plot in Figure 3. The pooled aORs were 1.58 (95% CI, 1.52–1.65) in the cervical group, 1.49 (95% CI, 1.47–1.51) in the lumbar group, and 2.24 (95% CI, 2.16–2.33) in the combined group. Forest plots of the pooled adjusted odds ratios (aORs) for urinary dysfunction in patients with degenerative spinal disease from 2009 to 2016: (A) cervical, (B) lumbar, and (C) combined groups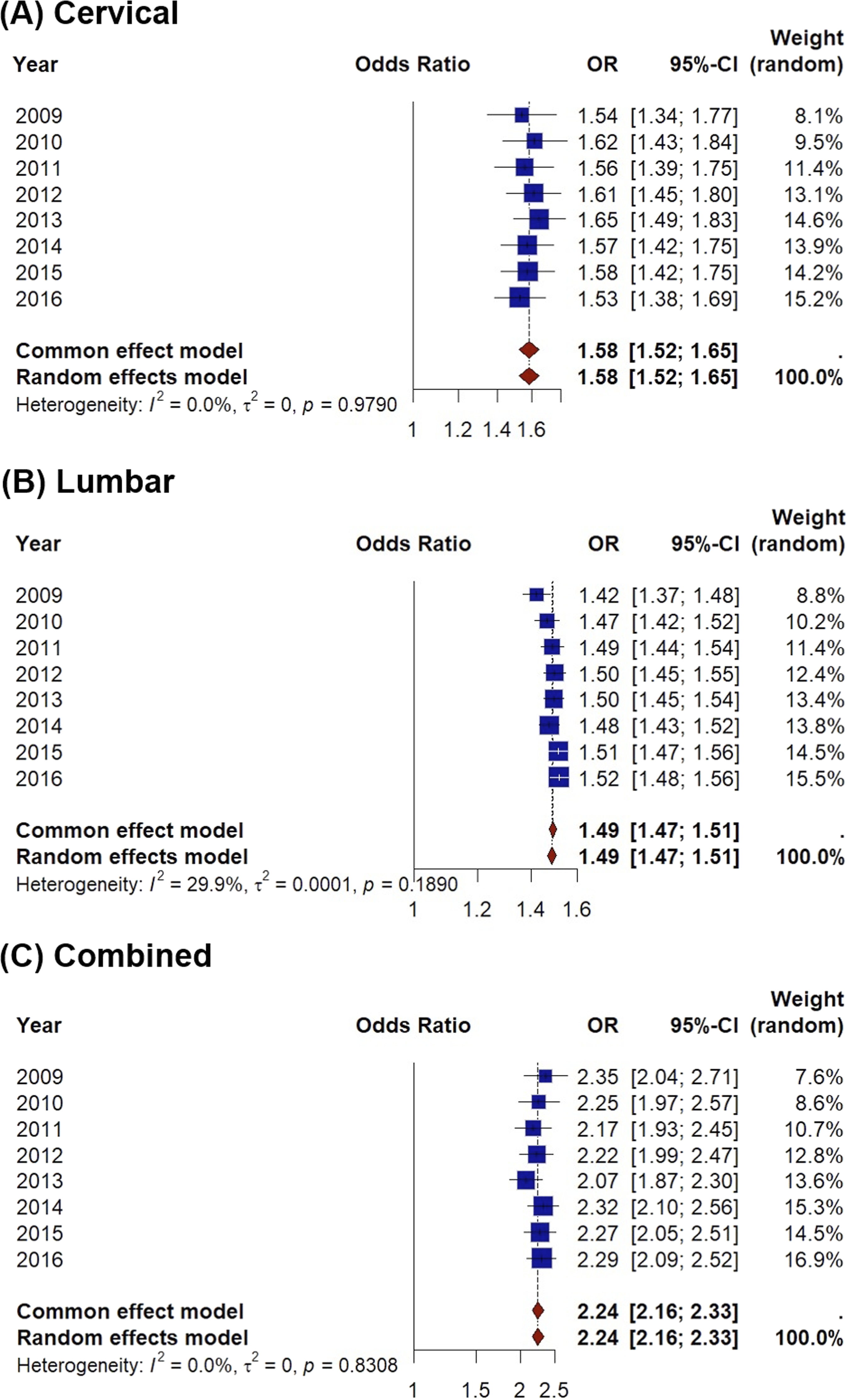
Discussion
This large-scale, population-based study demonstrated that degenerative spinal disease at both cervical and lumbar levels is independently associated with a significantly increased risk of urinary dysfunction. The pooled prevalence of urinary dysfunction was 8.7% in the cervical group, 9.1% in the lumbar group, and 13.7% in the combined group, all substantially higher than the 5.2% observed in the control group. After adjustment for sex, age, and CCI score, the pooled aORs were 1.58, 1.49, and 2.24 for the cervical, lumbar, and combined groups, respectively. Notably, patients with concurrent cervical and lumbar involvement demonstrated the highest prevalence and risk, suggesting a cumulative effect of multilevel spinal pathology on urinary function.
The association between cervical degenerative spinal disease and urinary dysfunction is well-established in the literature. 16 Cervical spinal cord compression disrupts descending inhibitory pathways originating from the pontine micturition center, resulting in detrusor overactivity and loss of voluntary bladder control. Lieberman et al reported a 50% prevalence of moderate-to-severe lower urinary tract symptoms in elective cervical surgery patients, with significantly higher odds in those with myelopathy. 8 Similarly, urodynamic studies by Kim et al confirmed neurogenic bladder in approximately 50% of patients with cervical spondylotic myelopathy, primarily characterized by detrusor-sphincter dyssynergia and involuntary contractions. 17 Kimura et al identified moderate-to-severe symptoms in 59.8% of patients referred for urological evaluation, noting improvements following decompression. 5 Misawa et al observed subjective urinary complaints in 52% of compressive myelopathy cases, with 90% showing postoperative recovery. 18 More recently, Kanematsu et al prospectively reported a 34.7% prevalence of urinary dysfunction, with 20%–46% of patients improving after surgery. 19 The pooled prevalence of our cervical group was 8.7%, somewhat lower than previously reported values; however, this reflects the nature of our large-scale data, which includes non-surgical patients identified via various diagnostic codes. Multivariable analysis showed a pooled aOR of 1.58, demonstrating that cervical degenerative spinal disease is an independent risk factor for urinary dysfunction.
Lumbar degenerative spinal disease has similarly been recognized as a significant contributor to voiding dysfunction through compression of lumbosacral nerve roots governing afferent and efferent innervation of the detrusor muscle. Sone et al found that 73.9% of patients with lumbar spinal canal stenosis had urological complaints. 9 Deen et al reported some degree of bladder dysfunction in all studied patients, with a subset recovering post-laminectomy. 20 Additionally, Orlin et al identified abnormal uroflowmetry or post-void residual volume in 68.4% of preoperative lumbar surgery patients. 21 Beyond the direct nerve root compression caused by spinal stenosis, structural changes in the lumbosacral spine, including decreased lower lumbar lordosis, have also been suggested as a contributing factor to voiding dysfunction. 22 The pooled prevalence of 9.1% and aOR of 1.49 observed in our lumbar group are also somewhat lower than estimates from some clinically selected surgical series; as with the cervical group, this is likely attributable to the unselected nature of our population-based data rather than a true underestimation of risk, and nonetheless confirms an independent association between lumbar degenerative spinal disease and urinary dysfunction.
The prevalence of urinary dysfunction in patients with combined cervical and lumbar degenerative spinal disease has been rarely investigated. Tandem spinal stenosis, most commonly involving concomitant cervical and lumbar stenosis, is frequently overlooked despite being reported in up to 60% of patients with spinal stenosis, with delayed diagnosis associated with serious complications. 23 Clinically, tandem spinal stenosis presents with neurogenic claudication, progressive gait disturbance, mixed motor neuron findings, and sphincter disturbance.24,25 Given that micturition is governed by both supraspinal pathways descending through the cervical cord from the pontine micturition center and peripheral lumbosacral innervation of the detrusor,26,27 concurrent pathology at both levels may simultaneously disrupt these mechanisms, producing a cumulative impairment exceeding that of single-level disease. The present study supports this hypothesis, with the combined group demonstrating the highest pooled prevalence of 13.7% and aOR of 2.24, providing population-level evidence of a cumulative effect of multilevel spinal pathology on urinary dysfunction.
A gradual increase in the prevalence of urinary dysfunction was observed from 2009 to 2016 across the cervical, lumbar, and combined groups. This trend may be attributable, at least in part, to the rapid aging of the Korean population, resulting in a progressive increase in the number of older individuals at greater risk for urinary dysfunction. In addition, the high accessibility of the Korean healthcare system and the widespread use of diagnostic evaluations and treatments may have contributed to the increased detection of urinary dysfunction over time. Despite year-to-year variations in prevalence, the aORs derived from multivariable analyses remained relatively stable throughout the study period and consistently demonstrated similar associations. Furthermore, clear differences in the risk of urinary dysfunction were observed among the cervical, lumbar, and combined groups, supporting the robustness and consistency of the study findings.
Several methodological strengths merit consideration. First, use of the HIRA national claims database with a 3% random sample of the entire Korean patient population across eight consecutive years yielded a mean analytic cohort of over 455,000 patients per dataset, affording substantial statistical power and minimizing selection bias inherent to institution-based cohorts. Second, the repeated cross-sectional design enabled meta-analysis of annual estimates, enhancing the stability of pooled effect sizes. Third, multivariable logistic regression with adjustment for age, sex, and CCI score ensured that the observed associations reflect the independent contribution of degenerative spinal disease to urinary dysfunction, strengthening the credibility of the reported aORs.
This study has several limitations that warrant consideration. First, as a claims-based analysis, diagnostic accuracy is inherently dependent on the fidelity of ICD-10 coding by clinicians, and subclinical or undiagnosed urinary dysfunction may have been systematically underrepresented, potentially leading to underestimation of true prevalence. Second, the cross-sectional nature of each annual dataset precludes causal inference or assessment of the temporal relationship between spinal disease onset and the development of urinary symptoms. Third, surgery-related variables, including the number of fused levels, operative time, and Foley catheter use, were not available in the database and therefore could not be included in the analysis. Fourth, because the study period ended in 2016, the effects of subsequent technological advances related to lower urinary tract symptoms may not be fully captured in the present study. Finally, while the Korean population provides a uniformly insured and well-characterized cohort, generalizability to other ethnic and healthcare populations should be interpreted with caution.
In conclusion, this large-scale, population-based study provides supportive epidemiological evidence that both cervical and lumbar degenerative spinal disease are independently associated with an increased risk of urinary dysfunction, with combined involvement demonstrating the highest risk, suggesting a possible cumulative impact of multilevel spinal pathology on bladder function. These findings highlight the clinical importance of proactively monitoring urinary dysfunction in patients with degenerative spinal disease, particularly in those with concurrent cervical and lumbar involvement. Integrating urinary symptom assessment into routine evaluations may facilitate earlier detection and potentially improve clinical management and quality of life.
Supplemental Material
Supplemental material - Prevalence and Risk of Urinary Dysfunction in Cervical and Lumbar Degenerative Spinal Disease: A Large-Scale Population-Based Study
Supplemental material for Prevalence and Risk of Urinary Dysfunction in Cervical and Lumbar Degenerative Spinal Disease: A Large-Scale Population-Based Study by Soo-Bin Lee, MD, PhD, Ji-Won Kwon, MD, PhD, Seong-Hwan Moon, MD, PhD, Kyung-Soo Suk, MD, PhD, Hak-Sun Kim, MD, PhD, Si-Young Park, MD, PhD and Byung Ho Lee, MD, PhD in Global Spine Journal
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board (IRB) of the corresponding author’s hospital (IRB No. 3-2018-0041). All methods were performed in accordance with the Declaration of Helsinki and the institutional guidelines of the corresponding author’s hospital.
Consent to Participate
A waiver was granted by the ethics committee.
Author Contributions
Soo-Bin Lee: Data collection, data analysis, manuscript drafting, statistical analysis, resources.
Byung Ho Lee: Study conception and design, supervision, critical revision of the manuscript, final approval of the manuscript.
Soo-Bin Lee, Ji-Won Kwon, Seong-Hwan Moon, Kyung-Soo Suk, Hak-Sun Kim, Si-Young Park: Methodology, data interpretation, manuscript review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.