
Abstract
Study Design
Retrospective analysis of a multicenter prospective adult spinal deformity (ASD) database.
Objective
In ASD surgery, fusion to the sacropelvis improves stability but increases morbidity. Stopping at L5 preserves motion but predisposes to distal junctional failure (DJF). This study aims to identify risk factors for DJF in ASD patients undergoing posterior fusion with lowest instrumented vertebra (LIV) at L5.
Methods
Patients undergoing posterior fusion with LIV-L5 and minimum two-years follow-up were included. Demographic data, radiographic parameters, and patient-reported outcome measures were collected. The primary endpoint was surgical extension to the pelvis (EP) for DJF. Patients were divided into EP and NoEP. Survival analysis and multivariate regression were used to identify predictors of DJF and postoperative malalignment.
Results
Eighty-one patients met inclusion criteria, with a mean follow-up of 4.50 years. Fifteen patients (18.5%) required EP due to DJF. The EP group demonstrated significantly worse preoperative global alignment, including higher sagittal vertical axis (SVA) and global tilt. Postoperative SVA was a strong predictor of DJF: patients with postoperative SVA >45 mm had a 5-year survival free from EP of 48.6%, compared with 95.1% in well-aligned patients (p<0.001). Multivariate analysis identified older age and higher preoperative SVA as independent risk factors for postoperative malalignment.
Conclusions
Choosing L5 as LIV is safe in well-aligned ASD patients, with approximately 80% remaining free from pelvic extension at five years. Inadequate postoperative sagittal correction, significantly increases the risk of DJF. Older patients with preoperative malalignment may benefit from primary fusion to the sacrum.
Introduction
In adult spinal deformity (ASD) surgery, fusion to the pelvis is associated with increased perioperative morbidity, postoperative stiffness, and higher rates of mechanical complications and revision surgery.1-4 A meta-analysis suggests that fusion short of the sacrum is associated with fewer reoperations, 5 although other studies report no significant differences in outcomes between fusion to L5 and fusion to the sacrum.6,7 In patients with advanced L5/S1 degeneration, severe loss of lumbar lordosis, L5–S1 stenosis, or an oblique L5–S1 takeoff, extension of fusion to the pelvis remains necessary to achieve optimal outcomes. 8
The primary controversy concerns the safety of stopping fusion at L5, as revision rates due to distal extension have been reported as high as 38.5% to 40%.9,10 Fusion ending at L5 has been associated with lower rates of pseudoarthrosis, implant-related complications, and proximal junctional kyphosis compared with fusion to the sacrum or pelvis. 11 Conversely, fusion distal to L5 provides better restoration of lumbar lordosis and sagittal balance, with fewer distal junctional failures (DJF). 11 DJF represents the primary cause of revision surgery in patients fused to L5. 11 When considering L5 as the lower instrumented vertebra (LIV), identification of risk factors for DJF is therefore essential to optimize LIV selection and minimize the risk of revision surgery. 12
Only a limited number of studies have evaluated risk factors for distal failure in patients with L5 as the lower instrumented vertebra (LIV), with most emphasizing the importance of adequate preoperative alignment and lordosis.13-15 Few have incorporated postoperative alignment into their analyses, focusing mainly on spinopelvic parameters such as lumbar lordosis 16 or PI–LL mismatch, 17 without specific evaluation of global alignment.
The present study aims to identify patients at risk of distal failure after long ASD fusions ending at L5, incorporating both preoperative and immediate postoperative alignment. We hypothesize that postoperative global alignment, reflecting the mechanical environment at the L5–S1 segment after deformity correction, is a stronger predictor of distal failure than preoperative parameters.
Materials and Methods
A retrospective analysis was performed on a prospective multicentric ASD database, including patients from six European centers across four countries. Ethical approval was obtained from the Institutional Review Boards (IRBs) of all participating centers (PR(ATR)127/2010; KEK-ZH: Nr.2013-0335; ATADEK 2014-609; HULP-PI1167), and informed consent was acquired from all enrolled patients prior to inclusion. This study was reported in accordance with the STROBE statement. Inclusion criteria for the database were age above 18 years, coronal Cobb angle ≥20°, sagittal vertical axis (SVA) ≥5 cm, pelvic tilt (PT) ≥25°, or thoracic kyphosis (TK) ≥60°. For this particular study, additional criteria included the following: 1) posterior fusion involving at least four instrumented segments, 2) LIV at L5, and 3) a minimum two-year follow-up. Surgical indications were determined by each operating surgeon, with no predefined criteria for LIV selection.
Demographic data, radiographic parameters, patient-reported outcome measurements (PROMs), and surgical variables were collected. Radiographic data included sagittal, coronal, spinopelvic, and global alignment parameters preoperatively and first postoperative standing x-rays. MRI evaluation of the L5-S1 disc was not part of the prospective data collection. Preoperative MRI images were retrieved when possible and retrospectively evaluated according to the Pfirrmann classification. 18 Selected PROMs were SF-36, SRS-22r, and the Oswestry Disability Index (ODI version 2). Additionally, data on adverse events and subsequent revision surgeries throughout the follow-up period were collected. The need for surgical revision for extension to the pelvis was established as the endpoint for survival analysis. Patients were divided into two groups based on whether they had extension to the pelvis (EP) or not (NoEP). Both groups were compared.
Statistical Analyses
Continuous variables were descriptively analyzed using mean values and standard deviations, while categorical variables were presented as the number and percentage of patients. The normal distribution of the data was assessed using the Kolmogorov-Smirnov test. Statistical comparisons were made using Chi-square or Fisher’s exact test and Student’s t or Mann-Whitney U tests depending on the normal distribution of the variables. Statistical significance was set at p < 0.05 for all tests. Survival analysis was performed using the Kaplan-Meier method. Areas under the curve (AUC) for ROC curves were calculated for the most predictive variables, and survival was compared between predictive variables. The statistical analysis was executed using SPSS 25 (IBM Corp).
Results
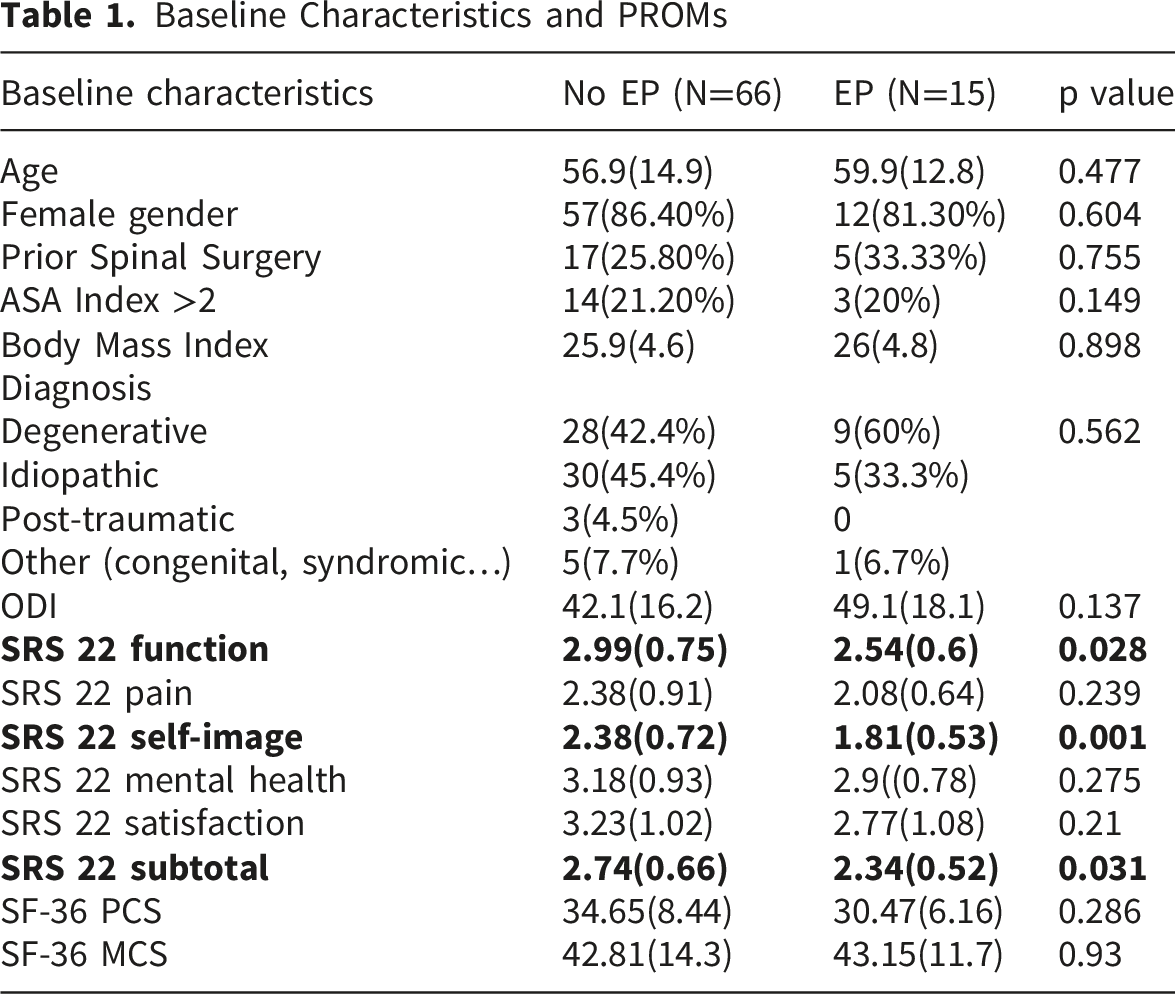
Baseline Characteristics and PROMs
Surgical Characteristics
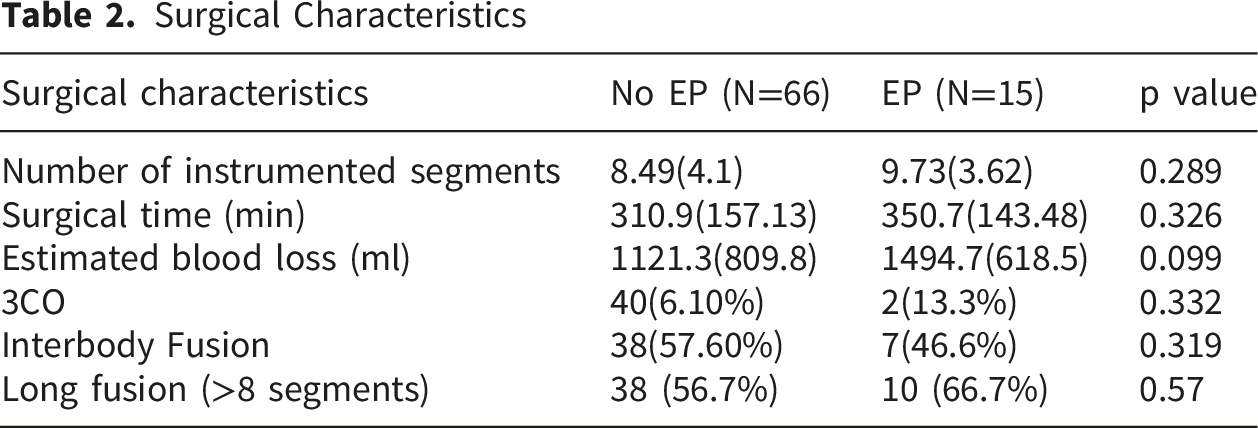
Fifteen patients (18.5%) had surgery for extension to the pelvis (EP) due to distal segment degeneration in 5 cases, mechanical failure in 4, sagittal malalignment in 3, and L5 fracture in 3. Revision surgery for EP, occurred in 53.4% before the two-year mark. Survival rates were 93.8% at 1 year, 90.1% at 2 years, and 80% at 5 years (Figure 1). Survival curve of patients fused to L5, with extension to the pelvis defined as the terminal event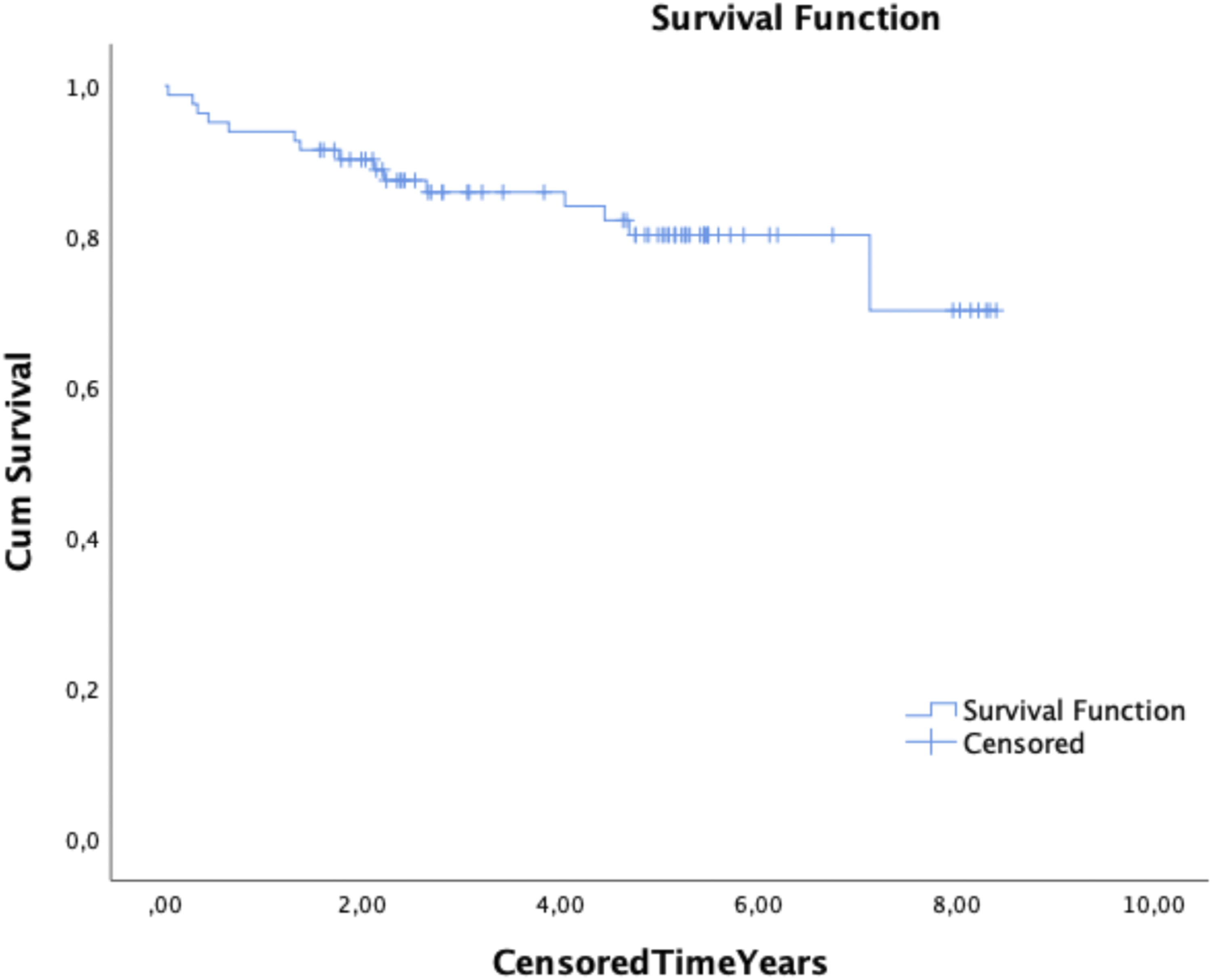
Preoperative Radiographic Parameters

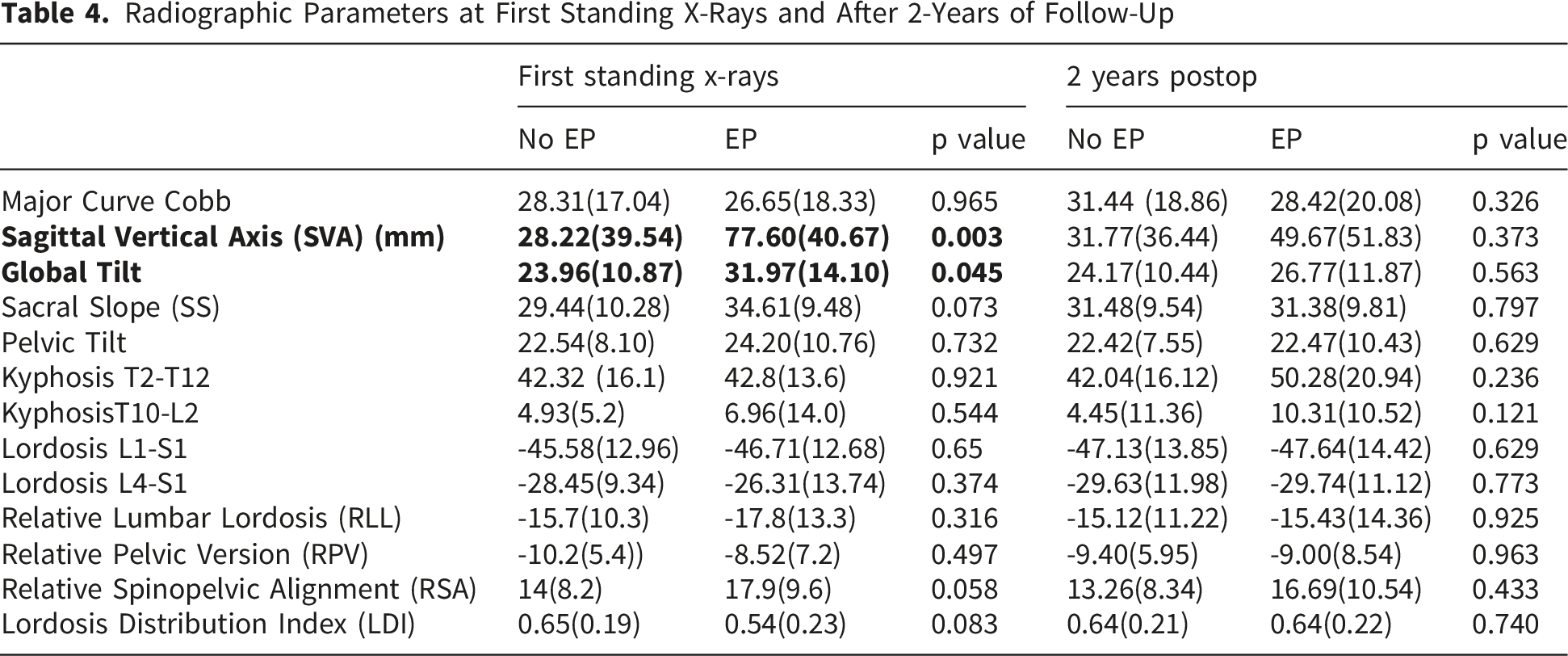
Radiographic Parameters at First Standing X-Rays and After 2-Years of Follow-Up
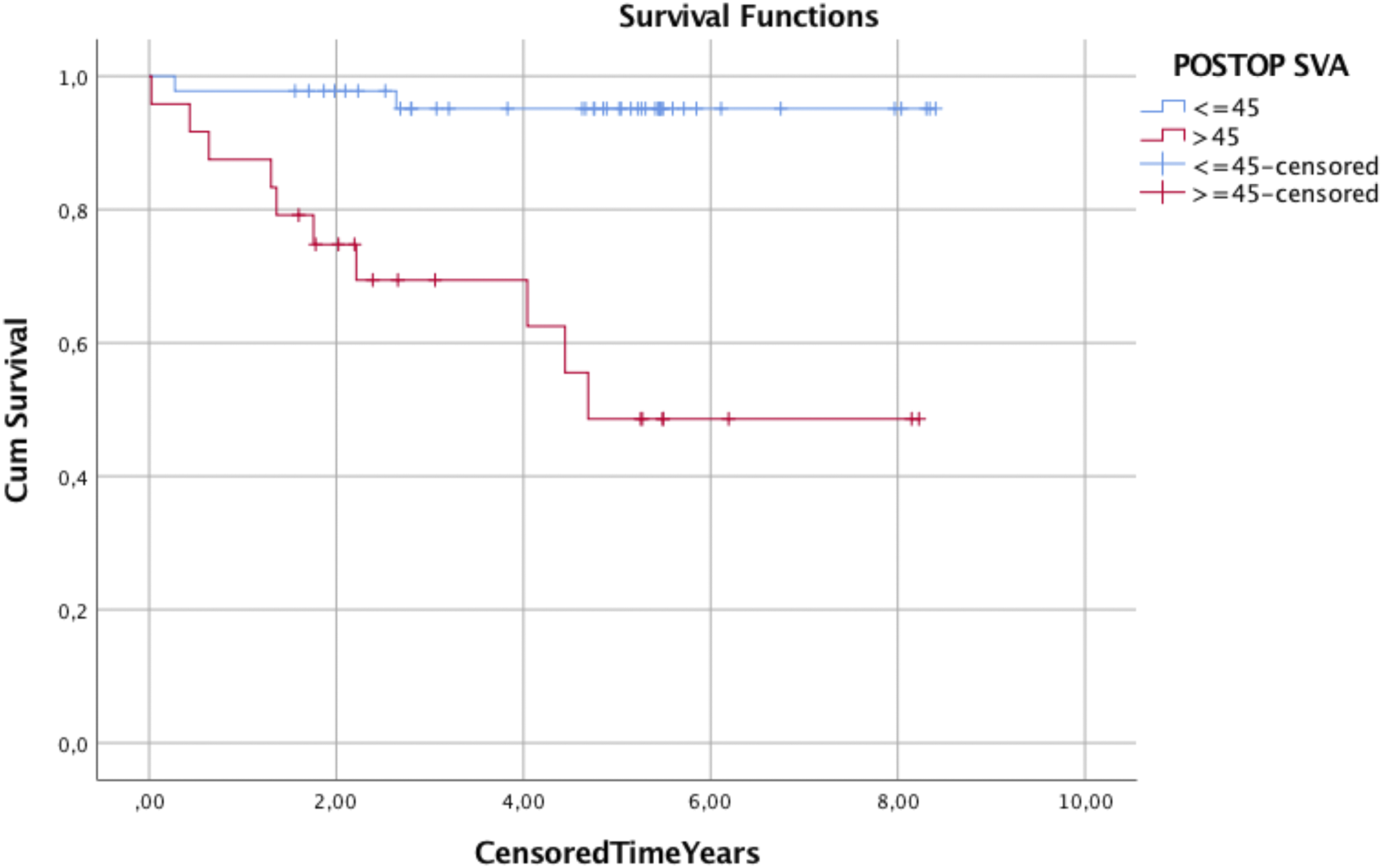
Preoperative SVA (preSVA) and first postoperative SVA (poSVA) were the most accurate predictors of EP (preSVA: AUC 0.746, p=0.02; cut-off point 31 mm, sensitivity 66.7%; specificity 71.8%; Youden Index 0.527; poSVA: AUC 0.825, p<0.001cut-off point 45 mm, sensitivity 83.3%, specificity 76.4%, Youden Index 0.587) (Figure 2). At 5 years, 95% of patients with poSVA ≤45 mm did not require EP compared to 48.6% of those with poSVA >45 mm (p < 0.001) (Figure 3). (A) Receiver operating characteristic (ROC) curve for preoperative sagittal vertical axis (SVA) as a predictor of extension to the pelvis (EP) (AUC = 0.75, p = 0.002). (B) ROC curve for 6-week postoperative SVA as a predictor of EP (AUC = 0.83, p < 0.001) Survival curves of patients fused to L5 stratified by postoperative SVA ≤ 45 mm versus > 45 mm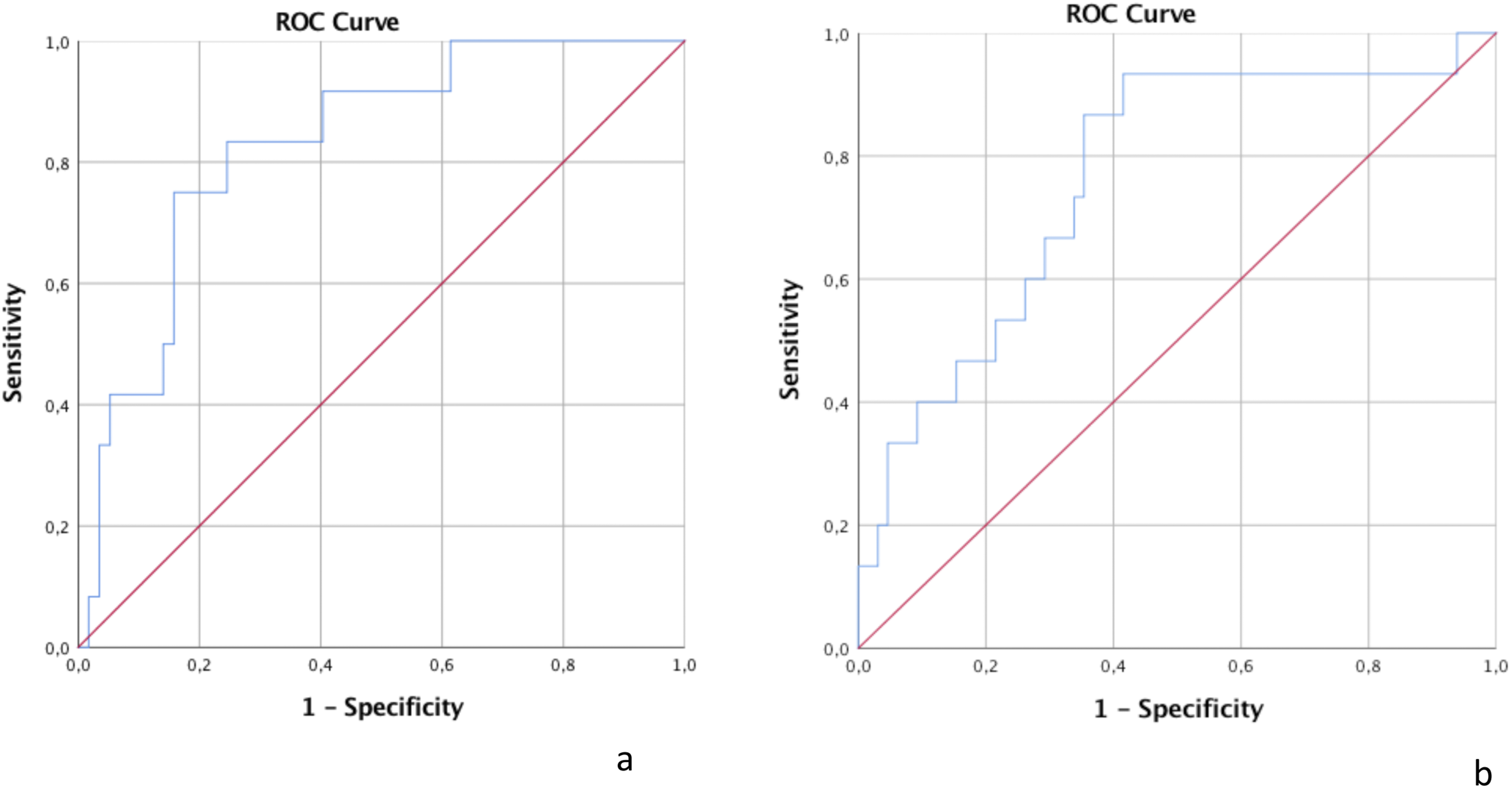
Multivariate analysis for EP yielded only postoperative SVA as significant associated factor (OR 1.020, 95% CI 1.003-1.037, p=0.042). Multivariate analysis for predictors for poSVA>45 revealed a statistically significant association with preoperative sagittal vertical axis (preSVA) (OR 1.024, 95% CI 1.009–1.040, p=0.02) and advanced age (OR 1.065, 95% CI 1.015–1.118, p=0.012).
Discussion
This study underscores the importance of accurate pre- and postoperative global malalignment as significant factors associated with increased risk of DKJ in patients with L5 as LIV. Among patients who attained optimal immediate postoperative global alignment, 95.1% remained free from extension to the pelvis at 5 years, suggesting that, in well-selected and properly aligned patients, ending instrumentation at L5 can be a safe option. It should be noted, however, that only a small proportion of the overall adult spinal deformity population in our database was treated with L5 as LIV, reflecting substantial selection bias and indicating that these findings apply only to a highly selected subgroup.
SVA >44 mm has already been associated with increased disc degeneration at L5/S1in patients with fusions ending at L5, although the study mentioning this did not discuss revision surgery rates
19
Another study noted that higher preoperative SVA correlated with distal junctional failure (DJF).
17
In our cohort, not only SVA but also other global alignment metrics less influenced by patient posture (GT, RSA), showed statistically significant differences at baseline. Notably, in our sample 48% of patients with a preoperative SVA >45 mm continued to exhibit malalignment postoperatively
Prior studies have suggested that pelvic incidence (PI) could be related with rapid disc degeneration L5/S1 and DJF in patients undergoing long fusions to L5. However, one study cited PI <48°, while the other referenced PI >50°.9,19 In our analysis, the EP group exhibited a slightly higher PI (57 vs. 53), though the difference was not statistically significant. We also did not observe differences in the lumbosacral fractional curve, which is another factor previously mentioned as a potential risk factor. Probably we could not find differences, due to selection bias, as patients with significant fractional curves and/or foraminal stenosis at L5/S1 are typically not candidates for fusion ending at L5. 8
Lumbar hypolordosis has been previously suggested as a potential factor for DJF15,17. While our data did not reflect this, it may be attributable to selection bias within our sample. Correction of lordosis at the lower lumbar level is crucial for restoring alignment and load distribution, 21 often necessitating inclusion of the L5/S1 disc. Consequently, patients with significant hypolordosis were not considered for fusion ending at L5 in our series (mean preoperative lordosis in our groups was -44.8° and -38.4° respectively). Cho et al, in analyzing failures of fusions to L5, concluded that in cases of hypolordosis and sagittal malalignment, even if the L5-S1 disc is not degenerated, it should be included in the fusion to achieve better correction and minimize the risk of failure due to deformity progression. 14 We observed a trend toward statistical significance (p=0.06) in relative lumbar lordosis (RLL), a GAP Score parameter measuring lumbar lordosis adjusted by PI. 22 RLL serves as a better proxy for assessing the effect of lordosis, as it provides an adjusted value relative to each patient’s PI. This observed trend further supports the notion that patients with hypolordosis are not ideal candidates for ending fusion at L5, even when differences in lordosis are small, as in the present sample. Do et al 17 identified preoperative PI-LL mismatch>40° as a significant factor in multivariate analysis for DJF following fusion to L5. However, in their series, patients had an average preoperative lordosis of -2° in the DJF group and -22° in the non-DJF group. In our experience, such cases are not suitable candidates for fusion ending at L5 from the outset. It is also noteworthy that the degree of lordosis at the L4/S1 segment in our series was substantial in both groups, closely approximating their total lumbar lordosis (-42° and -37°), likely indicating compensation for hypolordosis of the upper lumbar curve thoracolumbar kyphosis. 23 Figure 3 shows a typical case of lordosis maldistribution associated to thoracolumbar kyphosis.
Another factor that could potentially influence the ability of the L5/S1 disc to withstand the altered loads imposed by rigid fixation may be the different spinal shapes according to the Roussouly classification. 24 In non-surgical patients, it has already been shown that the risk of having Modic changes 25 and disc herniation 26 is higher in morphotypes 1 and 2. It is therefore very likely that these morphotypes, in which the apex of the lordosis lies closer to the L5/S1 disc and is consequently exposed to higher mechanical stress, are more prone to develop distal junctional failure (DJF). Due to the lack of statistical power, we were unable to detect any differences within our population, but this is a hypothesis worth exploring in larger studies.
Regarding failure mechanisms, Kwon et al described the development of distal kyphosis in patients experiencing failure of the most caudal pedicle screws. 27 They suggested that wide pedicles at L5, with abundant cancellous bone, might contribute to screw failure in this region, leading to distal kyphosis that disrupts global alignment. This specific anatomy could also be linked to the occurrence of L5 fractures, as observed in 3 cases. Another study examined the prevalence of L5/S1 disc degeneration and found that 69% of patients developed advanced disc degeneration after 5 years of long fusions ending at L5, concluding that deterioration in sagittal alignment was associated with L5/S1 disc degeneration.14,28
The factor most strongly associated with L5 LIV failure was postoperative global malalignment (SVA, GT). From a biomechanical perspective, insufficient correction leads to increased stress at the lumbosacral junction, facilitating failure. 28 One study evaluating postoperative alignment as a risk factor for failure with L5 as the LIV focused exclusively on spinopelvic parameters and did not identify significant differences, except for higher pelvic tilt and reduced lower lumbar lordosis in the extension group, findings that indirectly suggest inadequate global alignment. 16 Do et al also analyzed postoperative parameters; however, in their multivariate regression, only the use of antidepressants/anxiolytics and preoperative PI-LL mismatch >40° remained significant. 17 In our investigation of factors associated with postoperative malalignment, only age and preoperative malalignment were significant, indicating that in elderly, malaligned patients, fusion to L5 may not provide sufficient correction to mitigate the risk of DJF. Such patients might benefit from primary fusion to the sacropelvis, even when their L5/S1 disc appears well-preserved.
At the two-years follow-up we observed that in patients without pelvic extension, total lumbar lordosis and L4-S1 lordosis had not deteriorated over time, suggesting that there was not loss of correction and that the L5-S1 disc did not significantly deteriorate, reinforcing our hypothesis regarding the durability of fusion to L5 in well selected patients.
The present findings might be helpful to better refine optimal indications for ending fusion at L5. Previous data have already shown that it is imperative that the L5/S1 segment is well preserved (no severe disc degeneration, preserved disc height and facet joints), that there is no relevant stenosis (central or foraminal), and that there should not be an oblique take-off at L5/S1. Our data further support that, in the presence of preoperative sagittal imbalance, fusion to L5 may not provide sufficient distal lordosis or compensatory capacity to maintain appropriate sagittal alignment over time, ultimately increasing the risk of revision to the pelvis, especially in elderly patients. Finally, preoperative lower arc lordosis should be accounted for in preoperative planning, as it is likely to decrease after surgery, further impeding appropriate sagittal correction. Based on these considerations, we recommend limiting fusion to L5 to carefully selected cases meeting all of the following criteria: (1) non-severe L5–S1 disc degeneration (Pfirrmann grade ≤3); (2) preserved distal lordosis, defined as L4–S1 lordosis approximating two-thirds of the ideal lumbar lordosis according to the lordosis distribution index; and (3) absence of significant preoperative sagittal imbalance (e.g., normal SVA and global tilt). In this context, indications for stopping at L5 are primarily restricted to coronal deformities or kyphotic patterns that fulfill the above criteria.
The main limitation of this study is the insufficient data on L5/S1 preoperative disc degeneration (DD). Two studies have already suggested that preoperative DD does not play a role in the further development of subsequent DJF,14,17 although this might be probably related to avoidance to perform surgeries stopping at L5 in patients with advanced disc degeneration. We probably have a similar selection bias, as in the available data of 67.9% of the patients there were no cases with Pfirmann 4 or 5 degeneration. In addition, the well-preserved L4/S1 lordosis could be an indirect proxy for lack of DD, as degeneration has been linked to loss of lordosis. 29 Another limitation is the lack of other biological data, such as osteoporosis, frailty, or sarcopenia, which could have influenced the final outcome. Finally, the indication to stop at L5 entails an inherent risk of selection bias, excluding patients with hypolordosis, relevant lumbosacral junctional curves and L5/S1 disc degeneration.
Conclusions
Choosing L5 as the lower instrumented vertebra (LIV) is safe in well-selected patients, with 80% remaining free from extension to the pelvis at 5 years. In a sample with relatively well-preserved lumbar lordosis, insufficient correction of global alignment parameters was the factor most related to the need for pelvic extension (48% vs. 95.1% survival at 5 years). Elderly patients with preoperative malalignment are less likely to achieve adequate postoperative correction and may benefit from primary fusion to the pelvis.
Supplemental Material
Supplemental Material - L5 Is a Reliable Lower Instrumented Vertebra in Selected Adult Spinal Deformity Patients
Supplemental Material for L5 Is a Reliable Lower Instrumented Vertebra in Selected Adult Spinal Deformity Patients by Susana Núñez-Pereira, Sleiman Haddad, Vila Lluís, Anika Pupak, Eva Jacobs, Alejandro Gómez-Rice, Manuel Ramírez-Valencia, Louis Boissière, Javier Pizones, Yann-Philippe Charles, Ibrahim Obeid, Ahmet Alanay, Frank S. Kleinstueck, Ferran Pellisé, European Spine Study Group, ESSG in Global Spine Journal.
Footnotes
Acknowledgments
Artificial Intelligence Use Statement: The authors used ChatGPT (OpenAI) solely to improve the language and style of the manuscript. The tool was not used to generate scientific content, analyze data, or draw conclusions. All content was written, reviewed, and approved by the authors, who take full responsibility for the accuracy and integrity of the work.
Ethical Considerations
This study was performed according to the Helsinki Declaration and approved by the Institutional Review Board of each participant centre. Informed consent was acquired from all enrolled patients prior to inclusion.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded partly by research grants from Depuy Synthes Spine, Medtronic and Nuvasive.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SNP received research grants from SRS and ISCIII; JP received royalties from Medtronic and Stryker and reseach support from Depuy Synthes; MRV received consultancy fees from Stryker and research support from Orthofix; IO received royalties from Spineart and Clariance and research support from Depuy Synthes; AA received royalties from Zimvie, consultancy fees from ZimVie and Globus Medical and research support from Medtronic, Depuy Synthes and Nuvasive; FK received consultancy fees and reseach support from Depuy Synthes; FP received consultancy fees from Medtronic and Nuvasive; The European Spine Study Group receives research grants from Medtronic, Depuy Synthes and Nuvasive.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.