
Abstract
Study Design
Retrospective multi-hospital cohort study.
Objectives
Retropharyngeal hematoma (RH) after anterior cervical spine surgery (ACSS) is an uncommon but potentially fatal complication due to rapid postoperative airway compromise. As outpatient ACSS increases and shorter postoperative observation periods are adopted, the safe monitoring window for RH remains unclear. We characterized the timing of symptom onset and operative intervention for clinically significant RH after ACSS to inform postoperative observation practices.
Methods
Following institutional review board approval, all cervical spine procedures performed across eight hospitals (2013–2023) were reviewed. Patients undergoing ACSS who returned to the operating room within 72 hours were identified. Cases of clinically significant RH requiring operative evacuation were included. Timing of symptom onset and return to the operating room was abstracted from operative, anesthesia, and nursing documentation.
Results
Twenty-five patients developed postoperative RH, representing 0.29% of 8,609 anterior cervical spine procedures. Median time to symptom onset was 9 hours (IQR 4–15; range 1–34). Twenty-two patients (88%) developed symptoms within 24 hours, including four in the post-anesthesia care unit. Median time to return to the operating room was 11 hours (IQR 5–20). Oxygen desaturation occurred in 32%, and 20% required emergent bedside decompression. Three patients (12%) died during hospitalization, including two from anoxic brain injury following airway compromise.
Conclusions
Clinically significant RH after ACSS most commonly presents within the first 24 postoperative hours. These findings suggest that brief postoperative observation periods (4–8 hours) after ACDF may not capture the majority of severe airway events in this operative RH cohort.
Keywords
Introduction
Anterior cervical spine surgery (ACSS) is one of the most performed spinal procedures, frequently used to treat cervical radiculopathy and myelopathy. ACSS encompasses anterior cervical discectomy and fusion (ACDF), cervical disc replacement (CDR), and anterior cervical corpectomy and fusion (ACCF). Advances in surgical technique and perioperative care have supported a growing trend toward performing ACSS in outpatient settings, with many patients discharged the same day. Proponents of outpatient ACSS emphasize benefits such as reduced healthcare costs, lower risk of hospital-acquired complications, and improved patient satisfaction.1,2
While ACSS is generally considered safe, there are inherent risks. One of the most serious postoperative complications is the development of a retropharyngeal hematoma (RH), which can lead to rapid airway obstruction. Hematoma development after surgery is not uncommon but when confined to the cervical spine, airway compromise can occur. It has been reported that as little as 20 mL of blood in the retropharyngeal space can lead to tracheal deviation. 3 Although RH incidence is low (reported approximately 0.2%–1.9%), its consequences can include hypoxic injury, cardiac arrest, and death if not promptly recognized and treated.1,4,5
Detection and management of RH is a true surgical emergency that requires a multidisciplinary team to both diagnose and treat. Initial management may include urgent bedside decompression, endotracheal intubation, and prompt return to the operating room. Its unpredictable nature continues to be a key consideration in discharge planning and raises concerns about the safety of same-day discharge following ACSS.
While outpatient ACSS has been shown to be safe in appropriately selected patients, existing literature primarily evaluates overall complication rates, risk factors, and readmissions within small cohorts. Although RH is a recognized complication, detailed hour-level characterization of symptom onset—particularly among cases requiring operative intervention—remains limited. The purpose of this study was to retrospectively evaluate RH following ACSS across multiple hospitals within a single health system, with the primary objective of defining the temporal distribution of symptom onset. Improved characterization of this timing may inform postoperative monitoring protocols and discharge planning, acknowledging that discharge decisions remain multifactorial.
Methods
This study was reviewed and approved by the Institutional Review Board prior to data collection. A retrospective review was performed of cervical spine procedures conducted across eight hospitals within a single health system between January 1, 2013, and December 31,2023.
A total of 9,149 cervical spine surgeries were identified, of which 8,609 were performed via an anterior approach. Within the anterior cervical cohort, patients returning to the operating room within 72 hours of the index procedure were identified, yielding 193 cases of early reoperation for concerns including bleeding, hematoma evacuation, drainage, or wound exploration.
Each of the 193 cases underwent detailed chart review. Cases were included if a postoperative retropharyngeal hematoma was confirmed following an anterior cervical procedure (ACDF with or without corpectomy). Cases involving epidural hematoma, abscess, or superficial wound complications without retropharyngeal involvement were excluded. After applying these criteria, 25 patients comprised the final study cohort. These cases represented 12.9% of the 193 early reoperations within 72 hours and corresponded to an incidence of 25 of 8,609 anterior cervical cases (0.29%).
This methodology captured clinically significant retropharyngeal hematomas requiring operative evaluation within 72 hours of the index procedure. Nonoperative hematomas, delayed presentations beyond 72 hours, or cases managed outside the health system may not have been captured.
Operative notes, anesthesia records, and nursing documentation were reviewed to determine the timing of clinical symptom onset in relation to completion of the index procedure. Time zero was defined as the completion of skin closure for the index operation. Two independent reviewers abstracted timing data from operative, anesthesia, and nursing documentation. Symptom onset was defined as the earliest documented clinical change attributable to hematoma formation, including neck swelling, dysphagia, stridor, voice change, anxiety, respiratory distress, oxygen desaturation, or documented concern for expanding hematoma. Discrepancies were resolved by consensus with senior spine surgeon adjudication. Time to return to the operating room (TTOR) was defined as the interval from completion of skin closure of the index procedure to the start of the subsequent operative intervention. One patient had incomplete documentation regarding TTOR and was excluded from TTOR median calculations.
Continuous variables are reported as median (interquartile range [IQR]) and range; categorical variables are reported as counts and percentages.
Results
Demographic Characteristics and Timing of Symptom Onset and Operative Intervention Among Patients With Postoperative Retropharyngeal Hematoma Following Anterior Cervical Spine Surgery
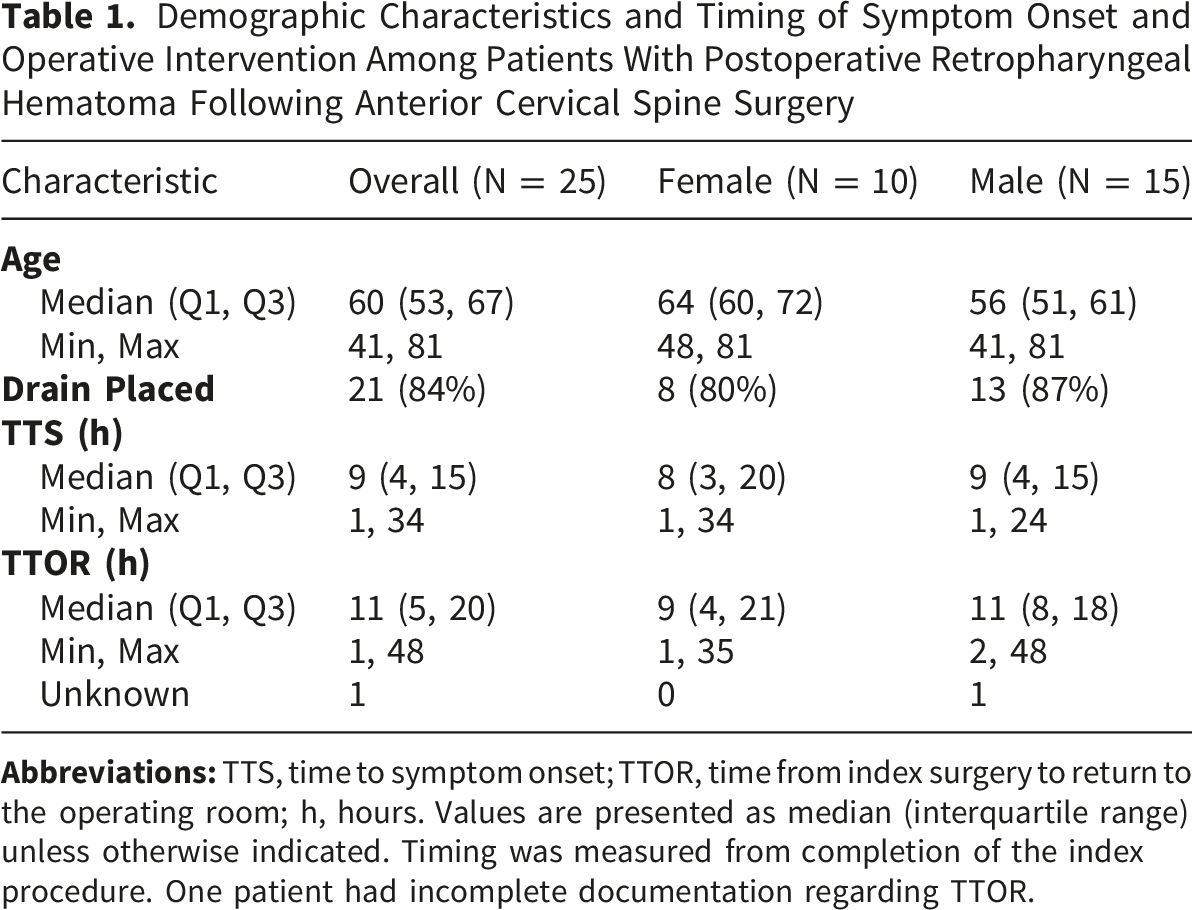
Most procedures involved multilevel constructs. Four patients (16%) underwent single-level fusion, six (24%) underwent two-level fusion, Twelve patients (48%) underwent three-level fusion, and three patients (12%) underwent fusion of four or more levels. Overall, 15 patients (60%) underwent fusion of three or more levels.
A surgical drain was placed in 21 patients (84%). Among these, 12 had closed-suction JP drains (57%), 3 had Penrose drains (14%), and 2 had Hemovac drains (10%); drain type was not documented in 4 cases (19%).
Oxygen desaturation events were documented in 8 patients (32%), and bedside or floor decompression prior to transfer to the operating room was required in 5 cases (20%). The median time from completion of the index procedure to symptom onset was 9 hours (IQR, 4–15; range, 1–34 hours). Four patients (16%) became symptomatic in the post-anesthesia care unit. Overall, 22 patients (88%) developed symptoms within 24 hours postoperatively, while three patients (12%) developed symptoms at or beyond 24 hours, including two at 24 hours and one at 34 hours.
Three patients (12%) died during the same hospitalization despite operative evacuation of the retropharyngeal hematoma. Two deaths were attributable to anoxic brain injury following cardiopulmonary arrest secondary to airway compromise. One of these patients arrested prior to evacuation and subsequently died after surgical intervention. The second underwent evacuation with concurrent tracheostomy but sustained irreversible hypoxic injury. A third patient died on postoperative day 21 after failure to wean from mechanical ventilation following hematoma evacuation.
The fatal cases in this cohort provide additional insight into the challenges associated with rapidly progressive postoperative retropharyngeal hematoma. One case involved an 81-year-old female who underwent C4–6 ACDF with hemicorpectomy for cervical myelopathy. Approximately 3 hours postoperatively, she developed difficulty breathing and clearing secretions. Despite bedside decompression of the cervical wound, multiple attempts at endotracheal intubation were unsuccessful. The patient was transported to the operating room with temporary ventilation through a laryngeal mask airway. Additional intubation attempts failed, prompting emergent otolaryngology consultation. Attempts at both tracheostomy and cricothyrotomy were unsuccessful because of extensive calcification of the thyroid cartilage, cricoid cartilage, and tracheal rings, ultimately requiring airway control through an intubating laryngeal mask airway prior to hematoma evacuation.
A second fatal case involved a 53-year-old female who underwent C5–7 ACDF with multilevel hemicorpectomies for cervical myeloradiculopathy. Approximately 11 hours postoperatively, she developed throat tightness, dysphagia, shortness of breath, anxiety, and a muffled voice. Evaluation at the bedside revealed an expanding cervical hematoma, prompting immediate activation of anesthesia and the rapid response team. Bedside hematoma evacuation was initiated while preparations for airway management were underway. Despite these measures, progressive airway compromise developed, and endotracheal intubation was unsuccessful because of marked airway swelling. The patient subsequently became cyanotic, developed bradycardia, and progressed to cardiopulmonary arrest requiring approximately 8–10 minutes of resuscitation. Oxygenation was temporarily restored with placement of a laryngeal mask airway, after which she underwent emergent tracheostomy and operative hematoma evacuation. Despite successful airway control and surgical intervention, the patient ultimately sustained irreversible hypoxic brain injury.
A third fatal case involved a 63-year-old female who underwent C3–7 ACDF for cervical stenosis and radiculopathy. Notably, symptom onset occurred approximately 34 hours postoperatively, representing the latest presentation in the cohort. She was reportedly recovering well, breathing and eating comfortably aside from expected postoperative pain. During routine nursing evaluation, she denied dysphagia or other airway complaints but was noted to have elevated blood pressure. She subsequently vomited and became acutely unresponsive, prompting activation of a code blue. On arrival, she was pulseless and apneic with concern for airway obstruction from an expanding cervical hematoma. Bedside decompression of the anterior cervical incision was immediately performed, releasing blood and multiple clots. Return of spontaneous circulation was achieved, and the patient was transported emergently to the operating room, where endotracheal intubation was ultimately achieved after multiple attempts in the setting of distorted anterior airway anatomy. Operative exploration demonstrated only small residual clots and no active bleeding source. Despite successful resuscitation and operative intervention, the patient ultimately sustained irreversible hypoxic injury.
The cumulative incidence of symptom onset over time is illustrated in Figure 1, demonstrating that approximately 50% of patients became symptomatic by 9 hours postoperatively. Symptom onset following anterior cervical spine surgery among patients with operative retropharyngeal hematoma. Symptom onset curve among patients with operative retropharyngeal hematoma demonstrating time from completion of surgery to symptom onset. Data represent only patients with operative RH (N = 25). Dashed lines indicate the median time to symptom onset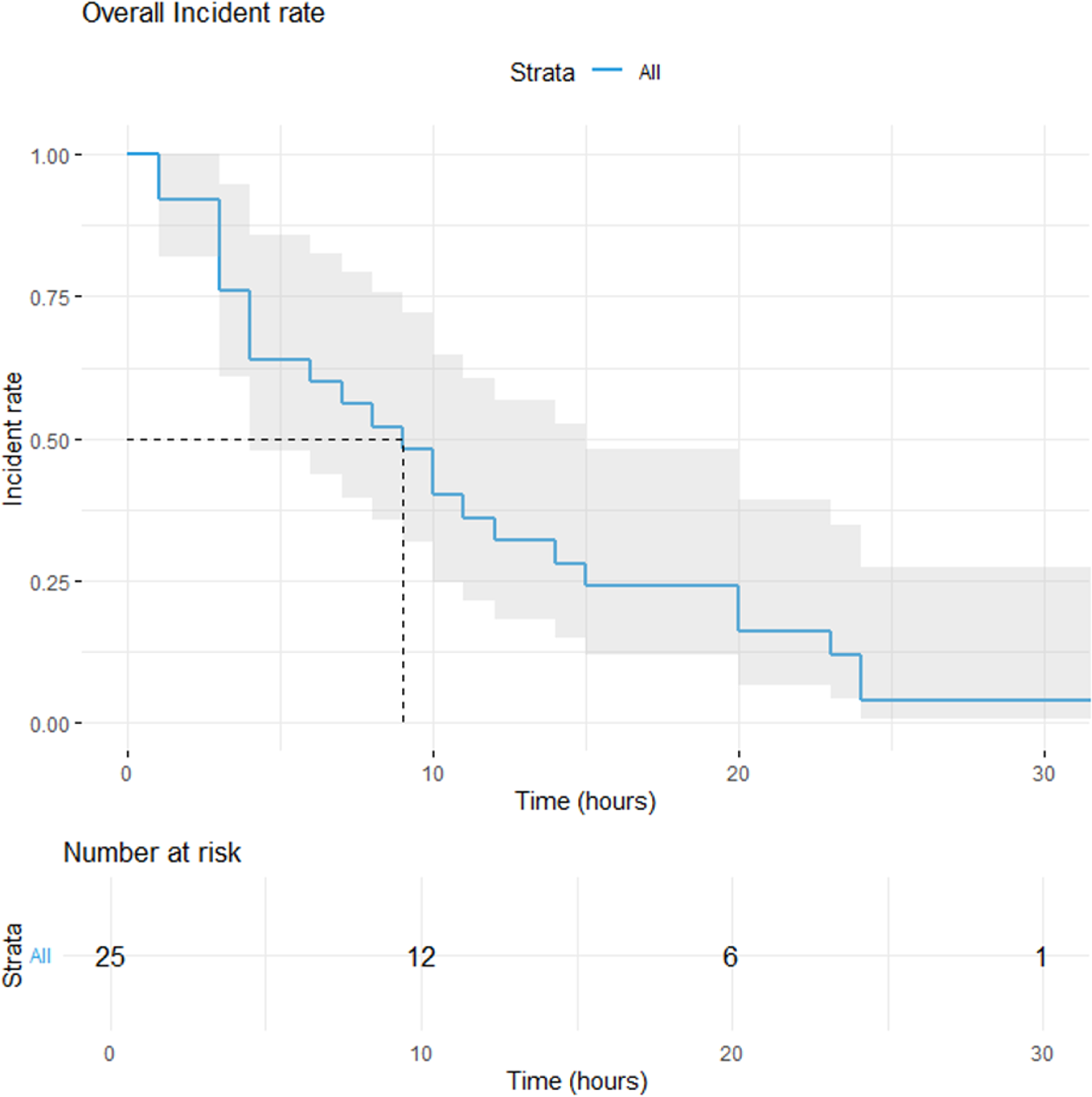
The median time to return to the operating room was 11 hours (IQR, 5–20; range, 1–48 hours). The distribution of time to operative intervention following the index surgery is shown in Figure 2. Incidence of return to the operating room following symptom onset among patients with operative retropharyngeal hematoma. Incidence curve among patients with operative retropharyngeal hematoma demonstrating time from index procedure to return to the operating room for hematoma evacuation. Data represent only patients with operative RH (N = 25). Dashed lines indicate the median time to operative intervention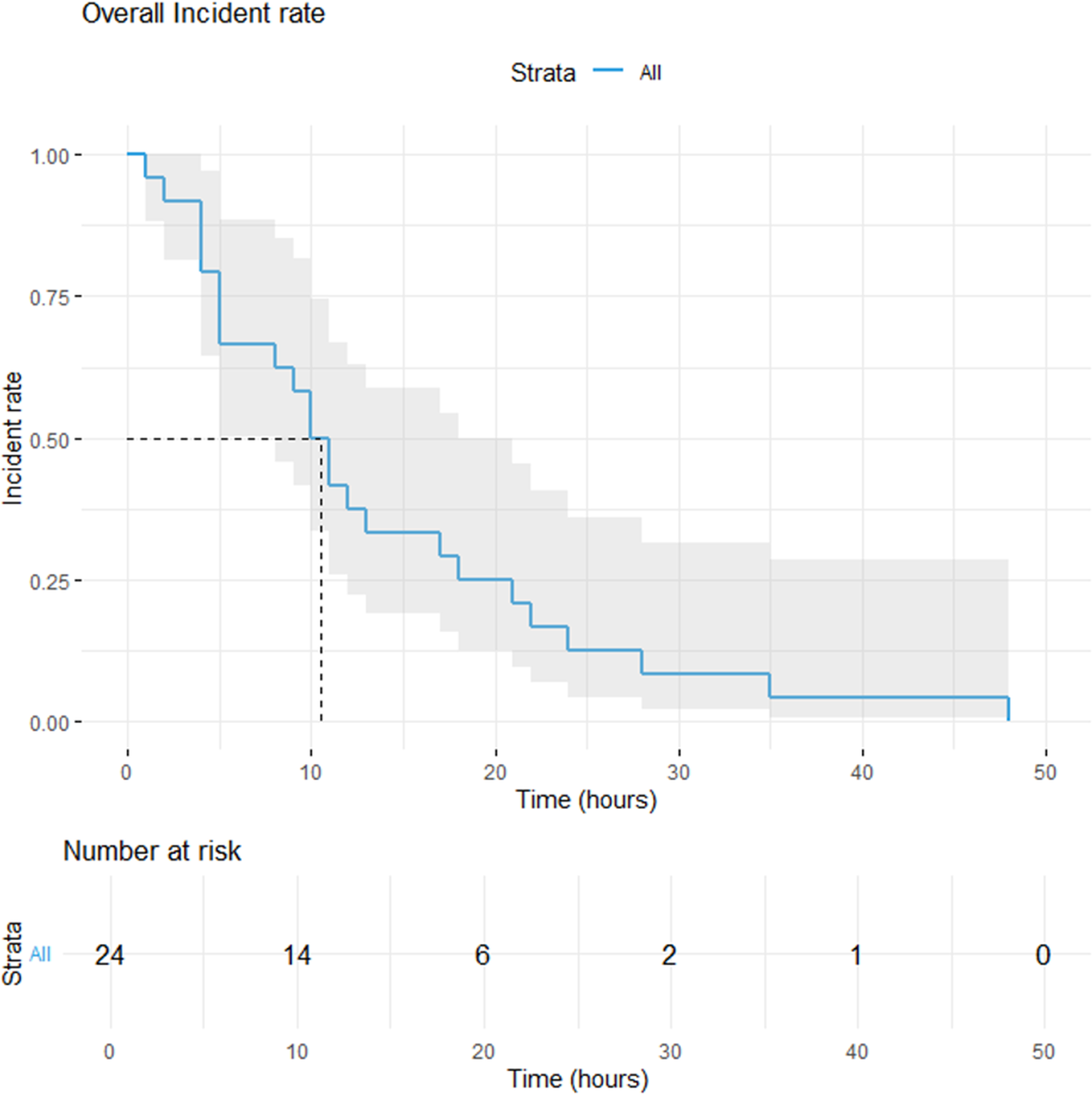
An intraoperative source of bleeding was identified in 16 cases (64%). Bleeding involving the longus colli muscle, whether arterial or venous in origin, was the most commonly identified source (n = 9). Additional sources include venous bleeding from structures such as the external jugular vein or anterior venous plexus (n = 4) and multiple or diffuse bleeding sources (n = 3). No discrete bleeding source was identified in 9 cases (36%).
Discussion
In recent years, there has been a continued shift toward performing ACSS, particularly anterior cervical discectomy and fusion (ACDF), in outpatient settings. Improvements in surgical technique, perioperative care pathways, and economic incentives have contributed to this trend. Although outpatient ACSS has been shown to be feasible and safe in carefully selected patients,2,6 postoperative retropharyngeal hematoma (RH) remains one of the most feared complications due to the risk of rapid airway compromise and potentially catastrophic outcomes.
The principal finding of this study is that clinically significant RH most commonly presents within the first 24 postoperative hours, although the timing of onset remains variable. In our cohort, the median time to symptom onset was 9 hours (interquartile range [IQR], 4–15; range, 1–34), and 88% of patients developed symptoms within 24 hours of surgery. Notably, 16% became symptomatic in the post-anesthesia care unit (PACU). This hour-level resolution provides clinically actionable insight beyond prior studies that have reported timing by postoperative day or lacked sufficient temporal precision. Importantly, although rare (0.29% incidence), operative RH carried substantial morbidity and mortality in this cohort, with three in-hospital deaths. The overall mortality attributable to RH in the anterior cervical cohort was 3 of 8,609 cases (0.035%).
These findings have important implications for postoperative monitoring and observation practices. Several outpatient ACDF protocols recommend observation periods of 4–8 hours,1,7-9 often based on early mobilization, pain control, and the absence of immediate complications. Tally et al reported average hospital stays of 4.7 hours for single-level and 5.4 hours for two-level ACDF, while Trahan et al proposed discharge criteria that included a minimum of 6 hours of postoperative monitoring in the absence of concerning findings. 8 While these protocols may be appropriate for many patients, our timing distribution suggests that a substantial proportion of RH cases begin after these commonly used same-day discharge windows. Furthermore, the cumulative incidence curve (Figure 1) illustrates that approximately 50% of patients became symptomatic by the median onset time of 9 hours, reinforcing that meaningful risk persists beyond the early recovery period.
Our findings complement and extend prior large-database studies. Avetisian et al analyzed more than 430,000 ACDF cases and identified 140 patients who developed RH, with many presenting after discharge. 10 Although Avetisian et al demonstrated that timing is critical for postoperative management, their reliance on administrative data limited the ability to capture symptom onset within the first postoperative day. In contrast, our study leverages detailed operative, anesthesia, and nursing documentation to provide hour-level symptom onset data, allowing for a more precise definition of the highest-risk postoperative window. These findings reflect a selected cohort of clinically significant hematomas requiring operative evacuation and do not capture nonoperative, delayed, or out-of-system presentations.
Early recognition remains essential, as clinical deterioration may occur rapidly. Oxygen desaturation occurred in 32% of patients and was associated with earlier and more severe clinical presentation. These patients developed symptoms at a mean of 8.9 hours postoperatively, with a median onset of approximately 4 hours, reflecting a right-skewed distribution. Patients who desaturated underwent more extensive surgery, with a mean of 3.4 operative levels and 75% involving multilevel (≥3-level) anterior cervical exposure. Furthermore, 20% of the overall cohort required emergent bedside or floor decompression prior to operative evacuation, representing the most fulminant presentations. All patients in this subgroup became symptomatic within 6 hours, experienced oxygen desaturation, and had undergone multilevel surgery (mean 3.6 levels), frequently with inclusion of corpectomy.
The role of surgical drains in preventing retropharyngeal hematoma remains controversial. Drains were placed in 84% of patients in our cohort, yet RH still occurred, suggesting that drain use alone does not eliminate risk. In several cases, symptom onset occurred shortly after drain removal. However, given the small sample size and absence of a comparator cohort, the relationship between drain management—including drain type or timing—and hematoma development cannot be determined. Although causal inference is not possible in this retrospective study, this temporal association indicates that low drain output should not be interpreted as reassurance. Accordingly, these observations underscore the need for continued vigilance following drain removal; however, no conclusions regarding drain management can be drawn from this study.
Surgical extent also appears to influence RH presentation. In this cohort, 60% of patients underwent fusion of three or more levels, consistent with prior literature identifying increasing operative levels and surgical complexity as risk factors for postoperative hematoma. 4 Although our study lacks a non-RH comparative group and therefore cannot quantify relative risk, multilevel surgery was associated with earlier clinical presentation. Patients undergoing 1–2 level ACDF developed symptoms later (mean 12.6 hours) compared with those undergoing multilevel procedures (≥3 levels; mean 6.2 hours). This temporal difference suggests that increasing surgical extent may not only increase susceptibility to hematoma formation but also accelerate clinical deterioration, supporting heightened postoperative vigilance following higher-complexity anterior cervical procedures. A descriptive stratified analysis of symptom onset and time to reoperation by clinically relevant subgroups is provided in Supplemental Table 2.
Airway management remains a critical component of the treatment of postoperative retropharyngeal hematoma. Prior authors have emphasized the importance of avoiding prolonged or repeated unsuccessful attempts at endotracheal intubation in the setting of rapidly progressive airway compromise. Debkowska et al highlighted the potential role of emergent surgical airway access, including cricothyrotomy, when conventional airway management is unsuccessful and emphasized the need for rapid progression to definitive airway control in patients with evolving postoperative cervical airway obstruction. 11 Consequently, spine surgeons should maintain familiarity with emergent surgical airway techniques, including cricothyrotomy, ensuring they possess the baseline knowledge and technical awareness required when advanced anesthesia or otolaryngology support is delayed or unavailable.
Taken together, the fatal cases in this cohort demonstrate the narrow therapeutic window that may exist once airway compromise develops after anterior cervical spine surgery. Catastrophic deterioration occurred despite inpatient monitoring, prompt bedside decompression, rapid response activation, anesthesia involvement, and operative intervention. While prompt airway control remains paramount, it is not possible from this retrospective study to determine whether earlier or alternative airway interventions would have altered outcomes. These cases nevertheless highlight the challenges of emergent airway management in rapidly evolving retropharyngeal hematoma and underscore the importance of early recognition and timely escalation of care before progressive airway distortion further complicates management.
Limitations
This study has several limitations. Its retrospective design introduces potential selection and documentation bias. Case ascertainment relied on return to the operating room within 72 hours and therefore captures only clinically significant retropharyngeal hematomas requiring operative evaluation. Mild hematomas managed nonoperatively, delayed presentations beyond 72 hours, and cases managed outside the health system may not have been captured. Accordingly, the reported timing distribution reflects severe events rather than the full spectrum of postoperative hematoma.
The absence of a non-hematoma comparator cohort precludes risk-adjusted analysis and causal inference regarding operative levels, drain use, or other perioperative variables. Symptom onset timing was abstracted from clinical documentation and may be subject to imprecision despite structured review and adjudication. Operative duration could not be reliably extracted across cases due to heterogeneous documentation and was therefore not included in the analysis. Patient-level comorbid risk factors were not analyzed due to the absence of a non-hematoma comparator cohort. Accordingly, the observed timing distribution should not be interpreted as population-level risk, but rather as representative of clinically significant cases captured by this study design.
Conclusion
Retropharyngeal hematoma following anterior cervical spine surgery is rare but potentially catastrophic. In this cohort of clinically significant cases requiring operative evaluation, 88% manifested within 24 postoperative hours, including three fatal events. These findings suggest that very short postoperative observation windows may not capture the majority of severe events in this operative cohort, particularly following multilevel anterior cervical procedures. While discharge decisions remain individualized, heightened vigilance during the first 24 hours appears warranted.
Supplemental Material
Supplemental Material - Retropharyngeal Hematoma after Anterior Cervical Spine Surgery: Timing of Symptom Onset and Implications for Postoperative Observation
Supplemental Material for Retropharyngeal Hematoma after Anterior Cervical Spine Surgery: Timing of Symptom Onset and Implications for Postoperative Observation by Nicholas E. Runge, Jonathan T. Avon, Kishan C. Trivedi, BS, Nilesh M. Patel, MD in Global Spine Journal.
Supplemental Material
Supplemental Material - Retropharyngeal Hematoma after Anterior Cervical Spine Surgery: Timing of Symptom Onset and Implications for Postoperative Observation
Supplemental Material for Retropharyngeal Hematoma after Anterior Cervical Spine Surgery: Timing of Symptom Onset and Implications for Postoperative Observation by Nicholas E. Runge, Jonathan T. Avon, Kishan C. Trivedi, BS, Nilesh M. Patel, MD in Global Spine Journal.
Footnotes
Acknowledgements
During the preparation of this work the author(s) used Grammarly in order to correct grammar. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Ethical Considerations
This study was approved by the Corewell Health Institutional Review Board (IRB), protocol.
Consent to Participate
Informed consent was waived by the IRB due to the retrospective nature of the study and use of existing clinical data. IRB Approval number: 2023-313. IRB APPROVAL DATE: 03/15/2024.
Author Contributions
Nicholas E. Runge and Nilesh M. Patel contributed to study conception and design. Nicholas E. Runge, Jonathan T. Avon, and Kishan C. Trivedi contributed to manuscript drafting. Jonathan T. Avon and Kishan C. Trivedi contributed to data acquisition and data analysis. All authors contributed to critical revision of the manuscript for important intellectual content, approved the final version for submission, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and/or its supplementary materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.