
Abstract
Purpose
The inherently practical nature of clinical skills means they may be less amenable to online or technology-supported teaching and learning than other domains within health science education. There is a dearth of literature and limited knowledge regarding staff and student perceptions of digitally enhanced practical teaching across health science disciplines. The aim of this study was to explore staff and students’ perceptions to digitally assisted teaching and learning methods in practical health sciences education as well as the perceived barriers to and opportunities for use.
Methods
A cross-sectional online survey was distributed among third level institutions, examining staff and student experiences of digitally enhanced practical teaching, perceived opportunities and barriers and personal experiences of practical skill assessment. Descriptive statistics were used to analyse quantitative data while open ended questions were analysed using content analysis.
Results
Forty-one staff and 96 students competed the survey. Attitudes towards digitally enhanced practical teaching were mixed; staff described digital tools as holding potential while students believed tools were not best utilised by educators. Of the staff who had not carried out digitally enhanced assessment (56%, n = 23), 39% (n = 9) struggled to identify an appropriate technology supported method to assess learning outcomes.
Conclusion
The current study identified the importance of maximising aspects of traditional teaching and technology enhanced teaching and ensuring a balance between teaching approaches for student success.
Keywords
Rationale
Practical skills training is a core component of many health science courses.1–3 Practical skills, or competencies, are learned task-oriented skills, such as communicating, handling, and treating a patient, taking a medical history and conducting laboratory-based tests. Health science students must demonstrate certain practical skill knowledge and competencies that will enable them to work professionally within a healthcare setting.4,5 Teaching and learning practical skills is an area which many would not traditionally consider suited to online or distance learning methods. However, rapidly evolving technologies in the 21st century 6 has seen increased technological integration into classroom settings to support theoretical and practical teaching in the form of blended learning.7,8 In the context of practical teaching in the health sciences, some examples of digital technologies include live and/or recorded video footage, online presentations with audio, simulations, and technologically enhanced teaching props.
Restrictions associated with the Covid-19 pandemic required greater reliance on digital education and required educators to demonstrate innovation in the delivery of practical skill teaching and assessment to support students in obtaining core clinical competencies. For example through narrated power-point presentations, 9 recorded skill demonstrations, 10 live lectures delivered over video conferencing platforms,11,12 web-based simulations 13 and e-learning modules. 14
Although technology facilitated remote learning throughout the pandemic, its successful adaptation has been challenging. Common barriers reported by staff and students include unreliable internet, lack of familiarity with digital technologies, lack of skill suitability for remote learning approaches and excessive use of online teaching platforms.15,16 The use of technology in teaching has also provided staff and students with many unique opportunities not always available to them through traditional teaching; digital technologies facilitate safe practice prior to real-life clinical exposure, with the ability to bring learning to life through interactive and engaging digitised learning resources. 15
Digitally enhanced teaching has received increasing attention in recent years. 8 While research has explored staff and student perceptions of remote learning within health science disciplines,7,17–21 there is an evidence gap exploring perceptions of digitally enhanced practical skill teaching and assessment across health science disciplines. There is also a gap in the literature identifying staff and student perceived opportunities and barriers to digitally enhanced teaching in the health sciences generally, and in practical skill acquisition specifically.
In the post Covid-19 era, institutions are presented with a unique opportunity to reconsider approaches to practical skill teaching. Exploring what works well and what doesn’t work well when teaching practical skills using technology can improve competency teaching moving forward. 15
Thus, the primary aim of the current study was to explore staff and student perspectives of digitally enhanced practical teaching across the health sciences. A secondary aim was to identify opportunities and barriers related to the acquisition of practical skills using technology. Specifically, this study’s objective was to address the following research questions: 1. What are staff and student attitudes towards digitally enhanced practical teaching in the health sciences? 2. What are staff and student attitudes towards digitally enhanced practical skill assessment in the health sciences? 3. What are staff and student perceptions of the barriers to and opportunities for digitally enhanced practical teaching? 4. What works well and what doesn’t work well when teaching practical skills using digital technologies?
Methods
This study has received ethical approval from the Trinity College Dublin School of Medicine Research Ethics Committee (ID 20210604). Informed consent was required and obtained before commencing the survey, and participants were advised they could withdraw at any time, until the survey was submitted anonymously.
Survey development and design
The research team carried out an extensive review of the literature 15 and identified key topics and themes for consideration, informing the development of an online survey. Questions were further informed through consults with academic staff and a student advisory group. The survey was piloted and branching logic tested, after which minor edits were made.
The survey was designed using Qualtrics, a popular design management software.
It was categorised into four main sections: background Information; personal experiences of digitally enhanced practical teaching; perceived opportunities and barriers; experience of practical skill assessment. An additional section on online resource development training was included in the staff survey. Based on whether the participant indicated that they were a staff member or a student, the survey branched to questions specific to practical skill teaching or learning using skip logic. Survey sections included a mixture of open and close ended questions. Closed response options comprised of a 5-point Likert scale: 1 = strongly disagree, 2 = somewhat disagree, 3 = neither agree nor disagree, 4 = somewhat agree, 5 = strongly agree. The survey took approximately 15 min to complete. Once submitted, participants were thanked for their participation. A copy of the survey is available as supplementary material.
Recruitment
Recruitment was achieved through convenience sampling. Inclusion criteria required participants to be studying or teaching a health science at a tertiary educational institution (i.e. university, post-secondary college or equivalent). Students and staff within the health sciences were invited to take part in the survey through distribution of a promotional flyer advertising the study online through the social media platform Twitter (since rebranded X) in November 2021 and was live for 3 weeks.
Data handling and analysis
Data was exported to SPSS (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp) and filtered to identify participant subgroups based on survey pathways. Due to the branching element of the survey, not all questions were completed by all participants resulting in variation in sample sizes between responses. Descriptive statistics were performed on quantitative data while qualitative data collected from open-box responses was analysed using content analysis. 22 After familiarisation, open box data was coded and clustered by codes, with similar codes gathered together within their overarching theme. This process was conducted iteratively by both authors with meetings to discuss and agree upon emerging themes, using the community of enquiry framework as a thematic lens. 23 The community of enquiry framework is often used in the context on online and digital education and consists of three main presences; cognitive, social and teaching.
Results
Participant Details.
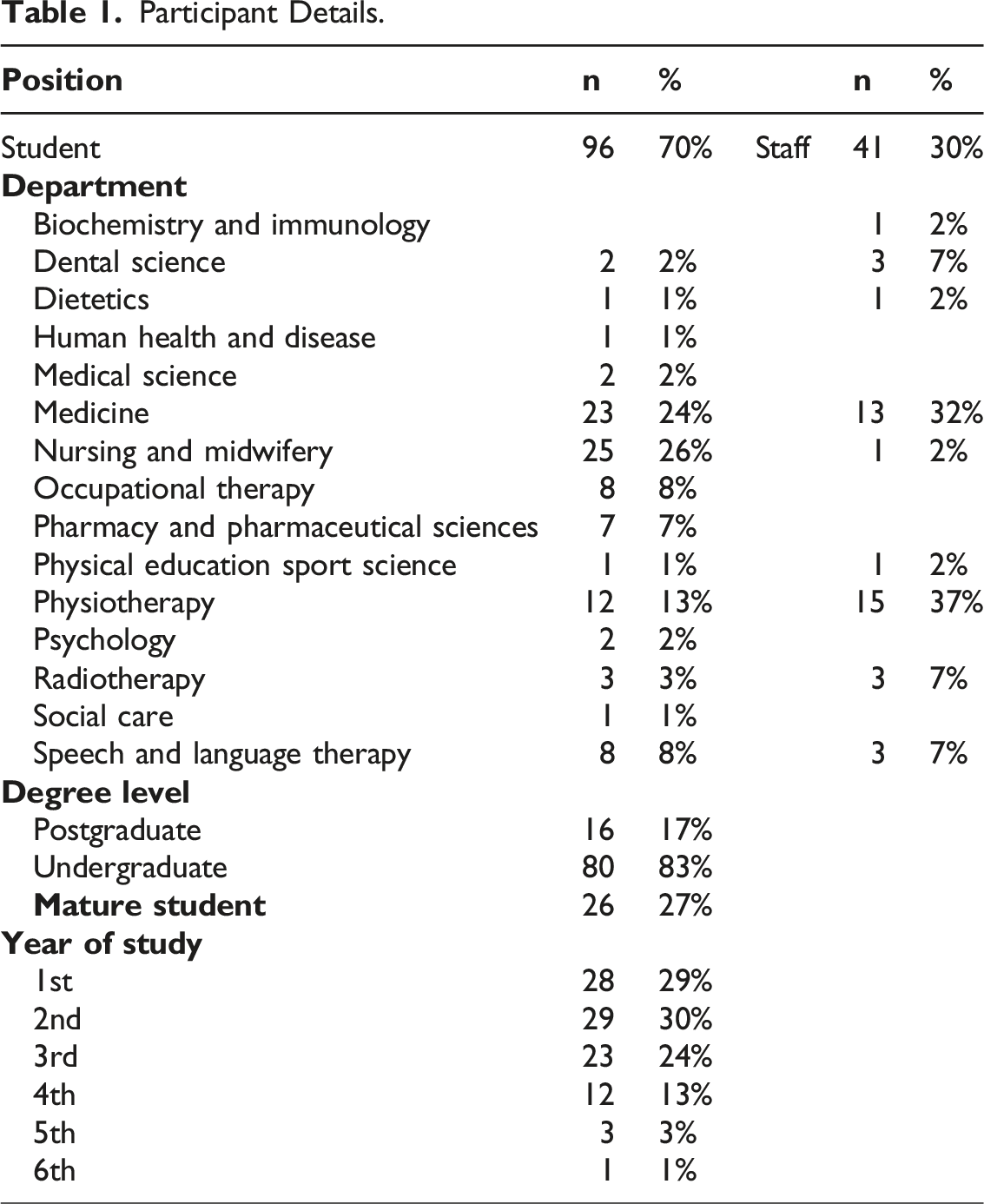
Staff reported teaching a range of practical skills, including performing wet-laboratory tests, taking a patient’s history, taking physiological measurements, assessing patients and treating patients. Technology was incorporated into practical skills teaching by 78% (n = 32) of educators. The main types of technology used by educators are detailed in Figure 1. Other forms of technologically enhanced teaching not listed included online game-based learning platforms and providing remote access to clinical software. Three educators did not integrate technology with practical skill teaching due to a lack of confidence in the efficacy of this approach (n = 1), lack of access to technologies (eg simulation; n = 2) and because the practical skill did not require the use digital technologies (n = 2). Digital technologies used by educators to support practical skill teaching.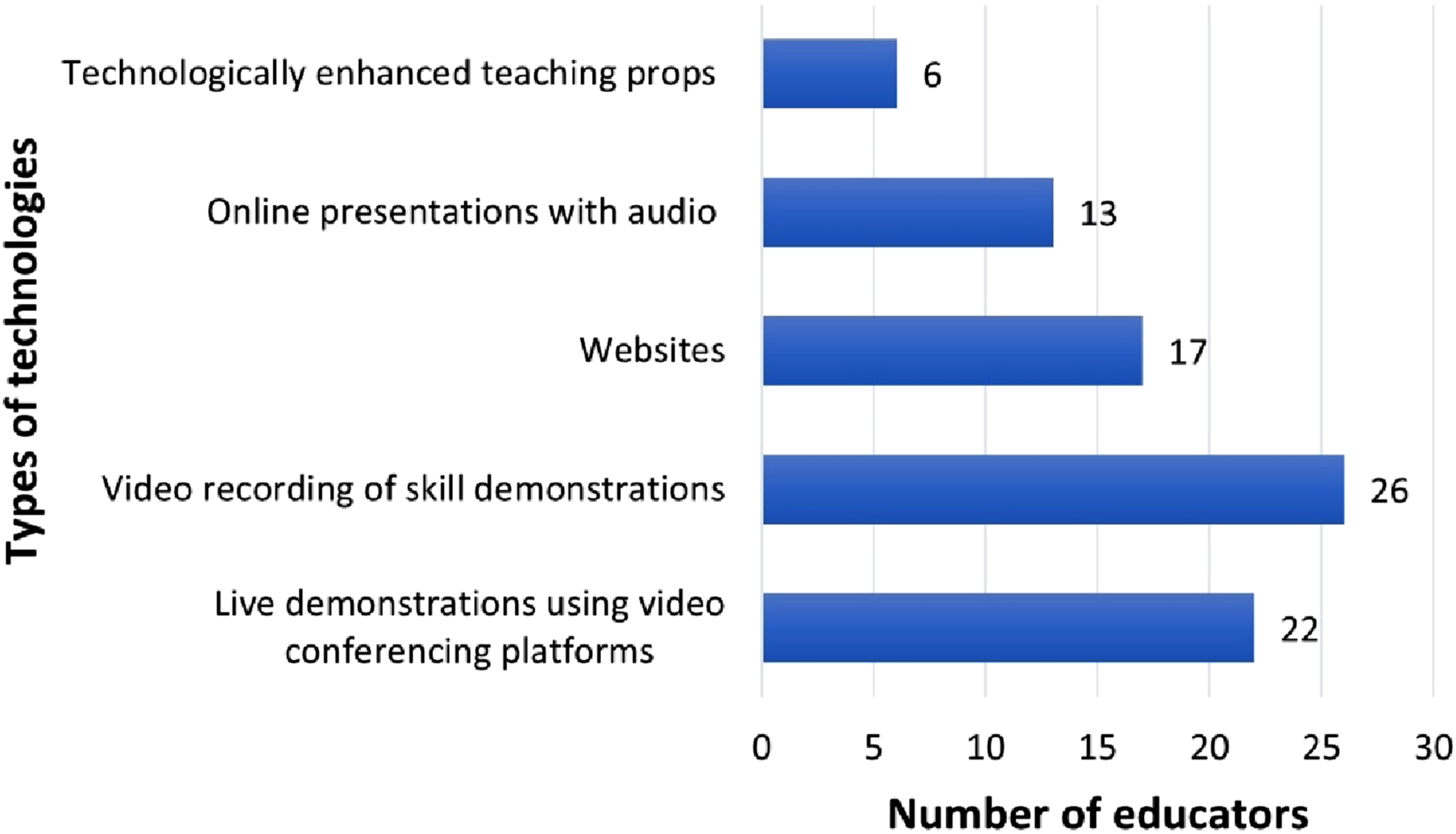
Of the academic staff, 71% (n = 29) engaged in training to enhance their skills in the use of digital technology for online learning. Training led to improved self-reported ability to teach or assess practical skills online or with other digital technology (76%, n = 22), improved ability to develop teaching materials (69%, n = 20) and improved confidence in teaching and assessing (72%, n = 21).
Digitally enhanced practical teaching
When asked whether their attitude towards using digital technology to teach practical skills is positive, negative, indifferent or mixed, staff and students predominantly held mixed attitudes (58%, n = 79).
Students described experiencing guilt if they were “not working long hours doing college work as… (there is) … no separation from study space and home space’’. Students felt that there was a “lack of empathy from staff’’ for the quantity of additional work students took on when distant learning. However, academics felt that they lacked support when designing and developing online learning resources.
Staff emphasised the importance of recognising when to incorporate technology into practical skill teaching, perhaps as an adjunct to “pre-lab preparation’’. By facilitating pre-class preparation and providing a “rich contextual backdrop to the clinical material’’, students benefit from “more valuable’’ in-person class-time. Staff believe that blended learning provides the best opportunities for students to engage with preparatory materials online while gaining practical hands-on experience in-person. “it can be used to reinforce and consolidate learning but should not be the sole means of learning a new practical skill’’
The importance of hand-on practical experience to “improve muscle memory… and confidence’’ was emphasised; without in-person practice, students lacked confidence in their ability to apply their learning to a clinical setting: “(when) applying your skills to real people in a healthcare setting, you need to be confident that you are able to do these practical skills. Learning them online won’t give you that confidence’’.
Digitally enhanced practical assessment
Approximately one third of students (38%, n = 36) had been assessed on a practical skill using digital technology. Of the staff who had not carried out digitally enhanced assessment methods (56%, n = 23), 39% (n = 9) struggled to identify an appropriate digitally enhanced assessment method to measure learning outcomes and 13% (n = 3) lacked confidence in using digital technology for assessment. The most commonly used form of digital assessment was writing assignments online (used by n = 12 educators), followed by submitting pre-recorded videos (n = 11 educators), live online demonstrations (n = 10 educators), and live oral examinations (n = 10 educators). Other forms of online assessments reported were the use of online questionnaires (n = 9), online peer assessment (n = 3) and assessments using virtual or augmented reality (n = 1).
Staff reported that asking students to submit videos of skill demonstration can present issues. Poor set up of equipment during remote assessment (e.g. “positioning of camera’’, ‘’poor lighting’’) lead to difficulties “discretely verifying measurements taken by student’’. Some students felt they were “without clear and proper feedback’’ following remote assessment.
Students worried that examiners were unable to accurately appraise skill competency through a webcam, resulting in difficulty receiving “an accurate grade’’. However, staff described the ability to pause and rewind pre-recorded submissions as a feature of online assessment that supported accurate grading and feedback, as they could “review and assess the (skill) performance in detail’’. During remote live skill assessments, educators perceived students as “more prepared and confident than usual, and more prepared for what to expect’’. This was potentially due to students’ ability to “control their exam environment’’; many students described feeling “more relaxed’’ and reduced ‘’assessment anxiety’’ when carrying out an exam at home: “the use of MS Teams when carrying out an oral patient consultation worked okay as it was very similar to how it would be in person yet being in the comfort of your home while doing it made it slightly less stressful.’’
Perceived challenges
The main challenges to digitally supported practical teaching perceived are outlined in Figure 2. There was a high level of agreement that a lack of “hands on” experience and access to equipment were challenges. One student reported that “You can’t replace real life with a computer screen’’. Many perceived challenges were not unique to practical teaching, and relate primarily to the reduced opportunity for human interactions (eg peer learning and social cues). Perceived challenges using digital technology to learn practical skills.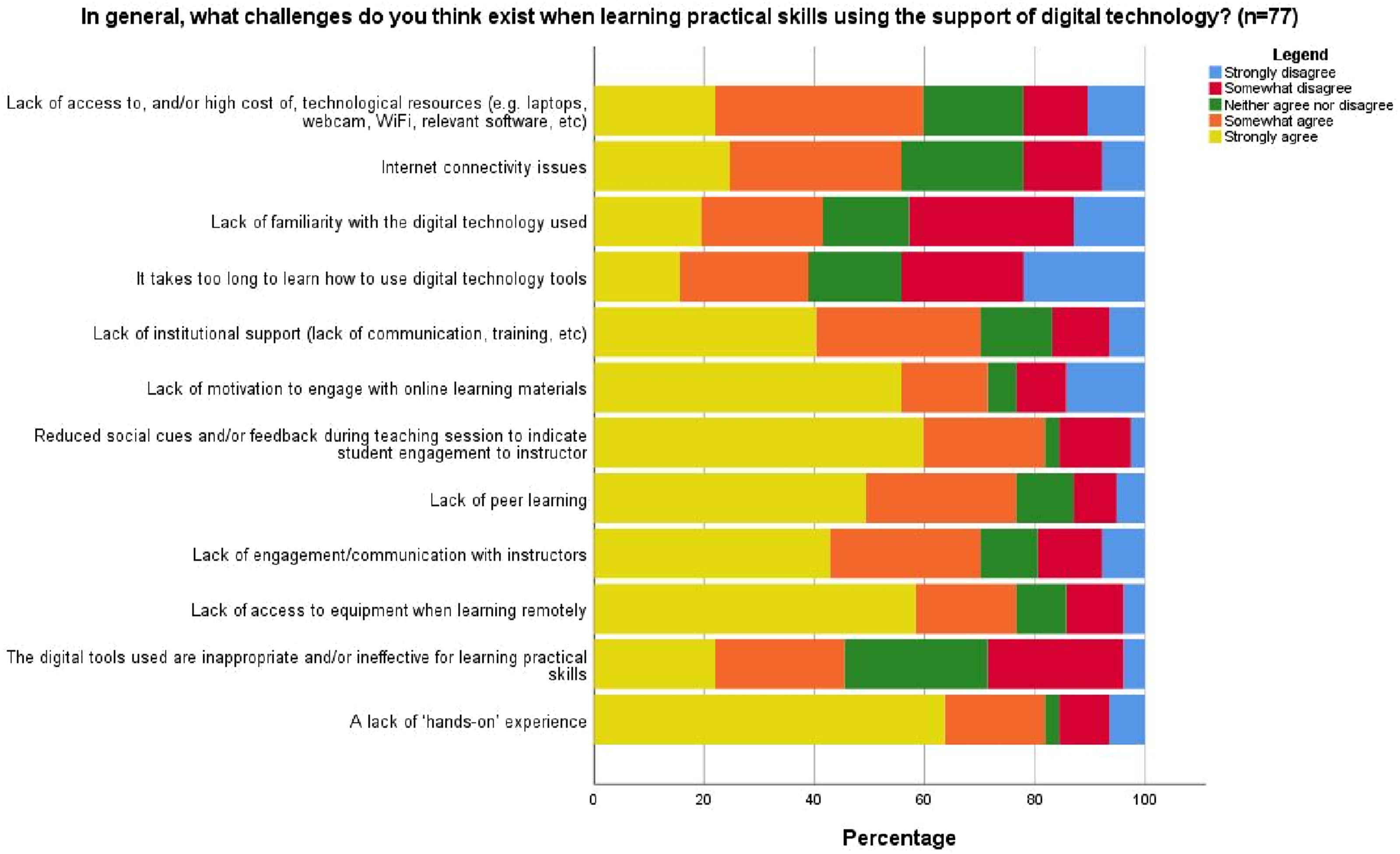
Educators disclosed hesitancy recording their practical skill teaching due to “either… lack of confidence, patient confidentiality concerns or concerns about potential reuse or misuse of recordings’’. However, students reported that a barrier to successful integration of technology in practical skill teaching is educator acceptance of digitally enhanced teaching: “a lot of the success of online learning depends on the instructor's willingness to be creative and engage with the technology. It is very apparent when a professor is opposed to using digital learning, and it sort of detracts from the whole experience.’’
Lack of familiarity with digital tools can lead to educators using one tool to meet varied learning outcomes, an approach to practical skill teaching further criticised by students: “Often the tool or technology is seen as a one size fits all but each learning outcome or set of outcomes needs to be reviewed independently’’.
Perceived opportunities
There are many opportunities presented by digitally enhanced practical teaching (see Figure 3). Both staff and students predominantly agreed that digital technologies can encourage strategic innovation in teaching approaches, improves flexibility and accessibility of learning as well as encouraging independent learning. Students however felt that there were unique opportunities still yet to be capitalised on, for example social media as a teaching platform should be better utilised: ‘‘The current trend is for material to be delivered as a PowerPoint with a voiceover, but that is a missed opportunity to use apps like Instagram, TikTok, Twitter, and Snapchat to deliver and learn new information in a way that is appealing to younger people.’’ Perceived opportunities presented by digitally enhanced practical teaching.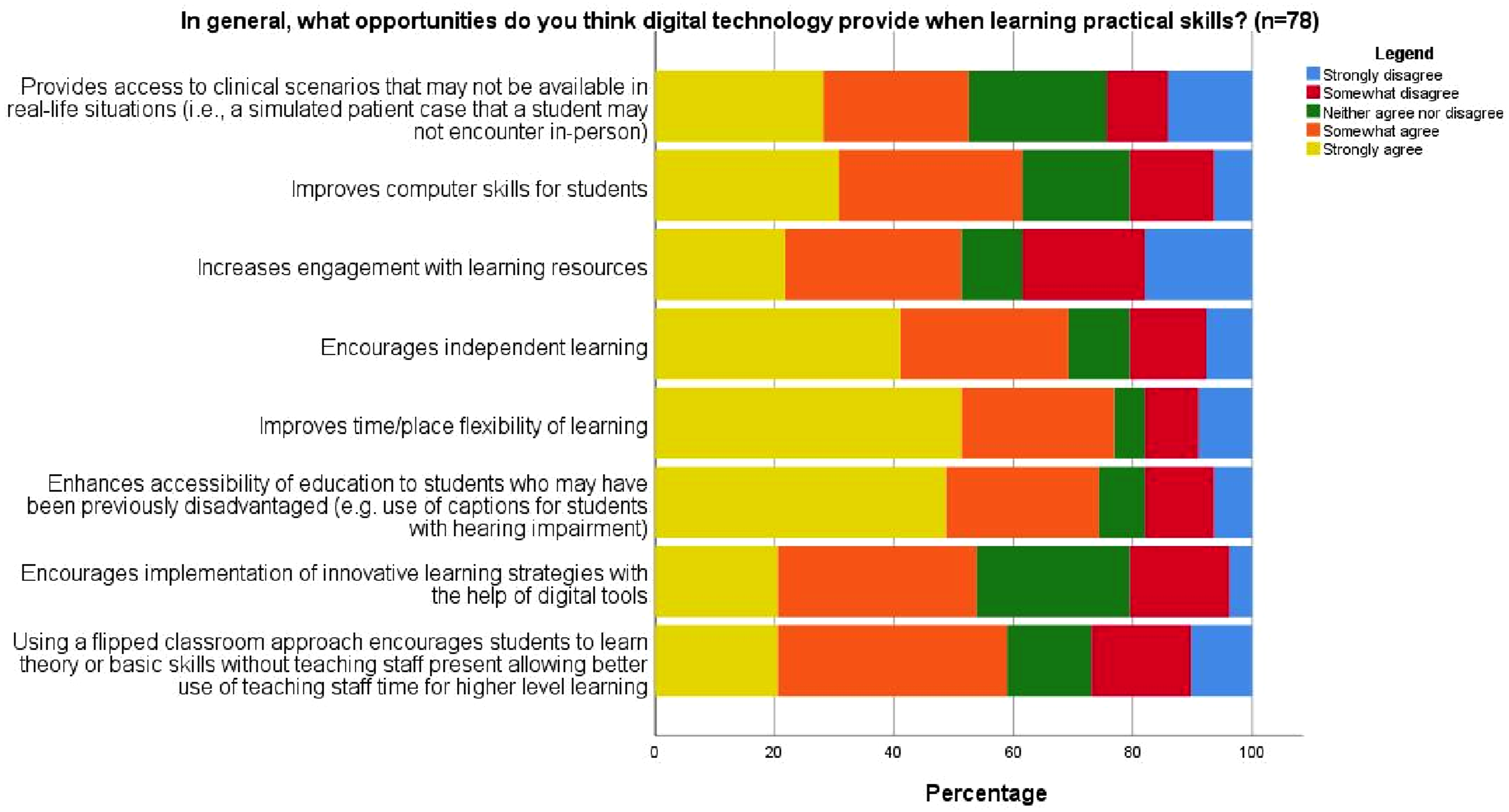
Participants acknowledged that digital technologies hold “huge potential’’ and “opens up education to much more people in society than ever before’’.
What worked well and what didn’t work well
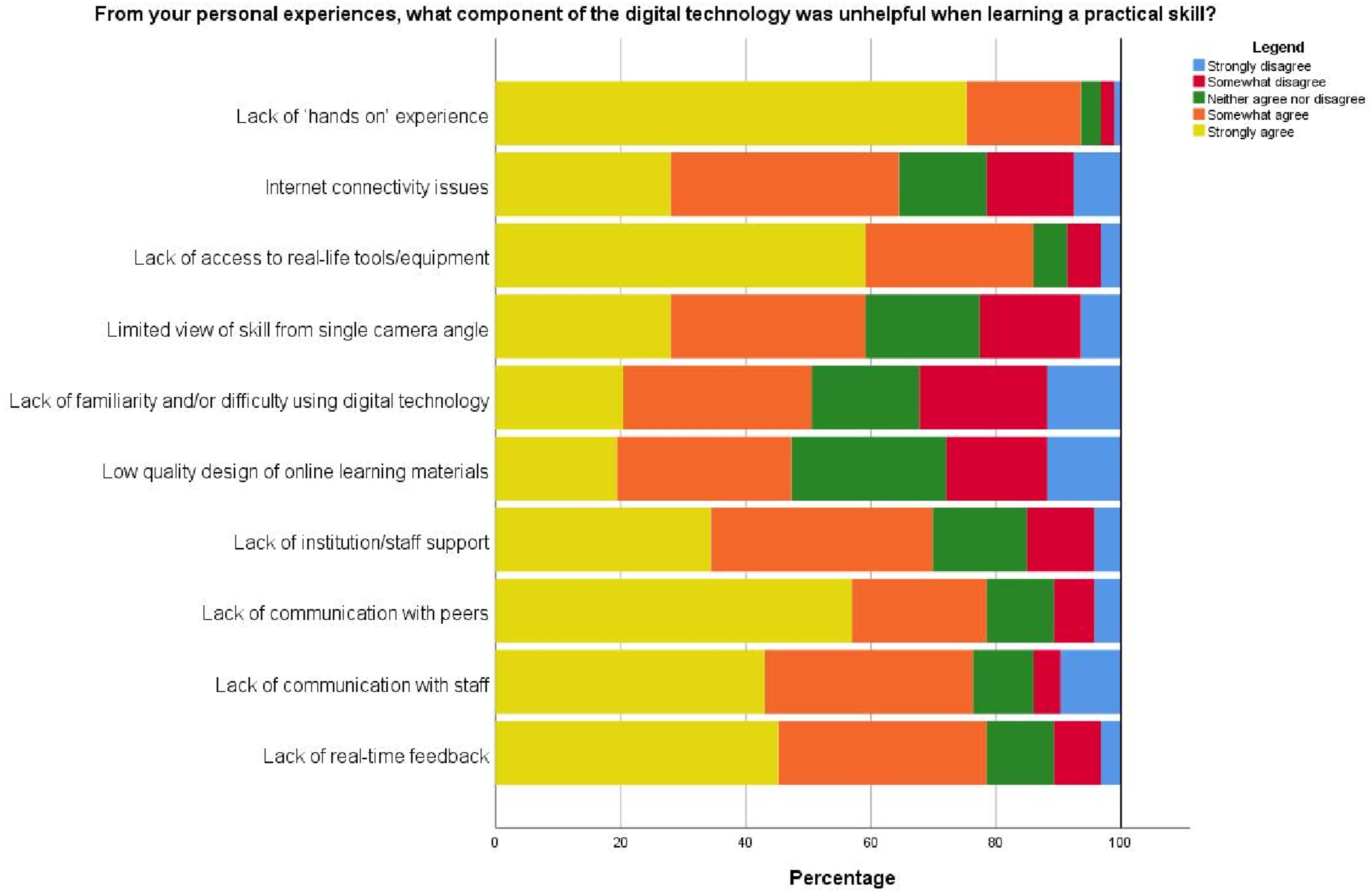
There are features of digital technologies that students and staff perceived as helpful and unhelpful (see Figures 4 and 5) during practical skill learning. Specifically, there are features that impacted student engagement when learning practical skills remotely. Educators noted that the ‘share screen’ option on videoconferencing platforms was useful for providing students with “remote control of software’’, allowing them to gain hands-on experience when learning remotely. Videoconferencing platforms also enable “breakout sessions for role plays, anonymous real time polling and Q + A″ which were useful features to assess students during group work. Staff found that asking students to have their cameras on when they are performing tasks on videoconferencing platforms worked well for encouraging peer engagement and feedback, however there was strong agreement that lack of engagement, real time feedback and hand on experience were unhelpful when learning practical skills using certain technology. Components of digital technology that were perceived by students as helpful for practical skill learning. Components of digital technology that were perceived by students as unhelpful for practical skill learning.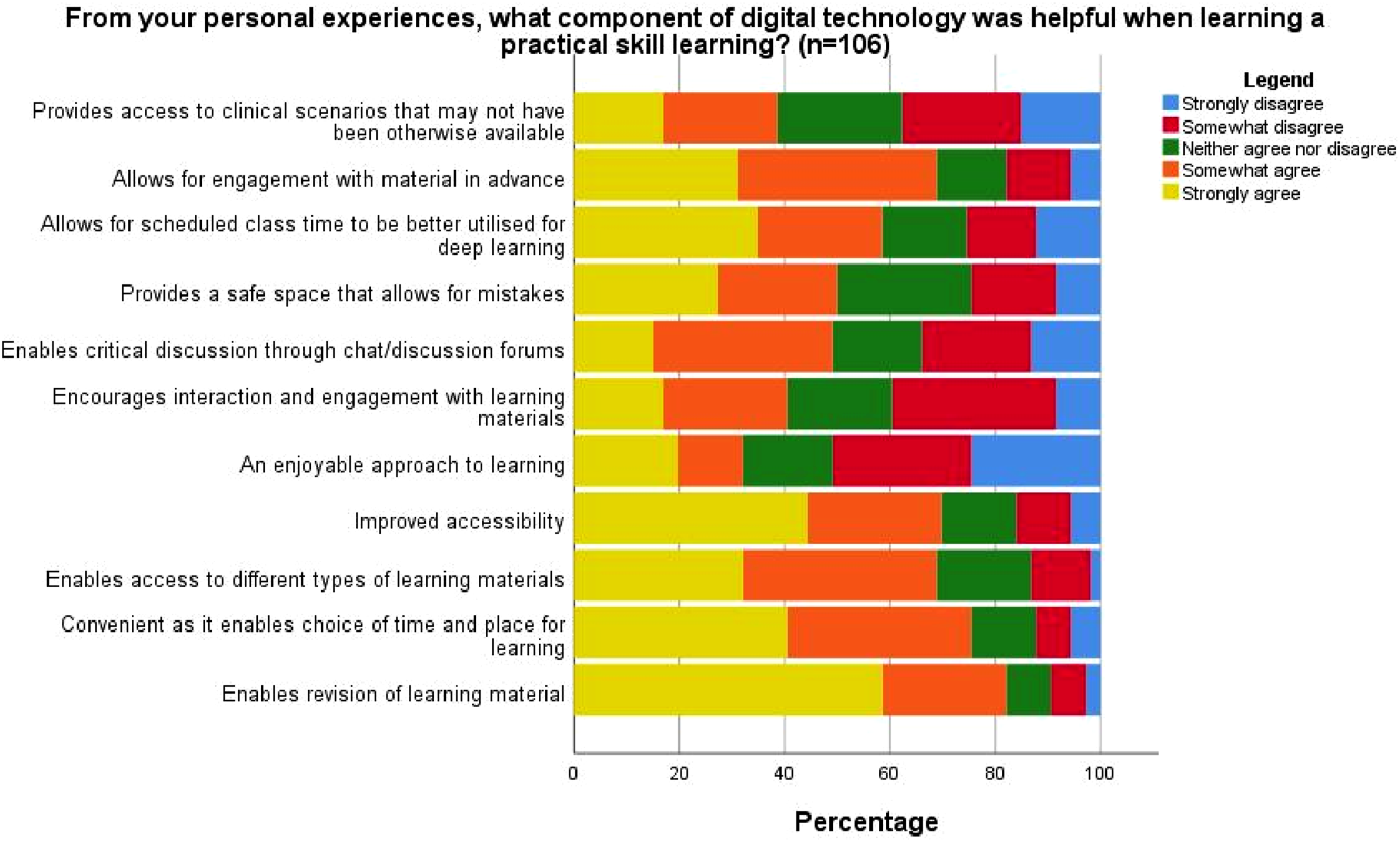
Students expressed exasperation with the “low standard’’ of technological literacy among teaching staff leading to “so much wasted potential’’. However, many staff felt that designing and developing resources for online delivery helped them to structure their learning content systematically, with clear learning outcomes that support student success. Educators could take time to ensure recorded skill demonstrations were of a greater quality than an in-person skill demonstration: “Although I tried to keep videos short, I could take my time recording them instead of working through examples in a crowded room with a time limit’’.
Overall, when viewed through the thematic lens of the community of inquiry framework, the cognitive presence was often well supported by digital technology, the social presence was less supported than the cognitive presence, and both students and staff reported a deficit in the teaching presence.
Discussion
Although the use of digital technologies in teaching has been gaining increasing attention in recent years, 8 the onset of the Covid-19 pandemic triggered a major pivot in how practical skills are taught within the health sciences. The current study attempts to explore and understand the acceptability of digitally enhanced tools for practical skill teaching and assessment by students and educators in the post Covid-19.
Digital tools used in teaching and learning
It is evident that various forms of technology are already integrated into practical skill teaching, however at the time of data collection virtual reality and artificial intelligence were not routinely used or considered for use by our participants, with few having experience of these tools in health science practical education. Current literature would suggest that such tools are now being integrated into many health science courses, with results of their efficacy in supporting practical skill competence inconsistent.24–26 Specific to Physiotherapy, literature reviews have reported promise in digital technologies to teach practical skills,27–29 however some highlighted concerns similar to those reported in this work around the need to leverage hybrid rather than fully remote teaching, the use of technology to compliment rather than fully replace traditional learning methods, 30 and the need for staff and students to be supported and trained in the use of such tools.26,29 These results attest to the fact that there is a need for greater emphasis on the teaching presence when using digital tools to support the acquisition of practical competencies, something which our work found was lacking.
Digital tools used in assessment
While there seems to be no doubt that technology has a place in teaching practical skills, our results indicate less certainty with regards to assessment. Despite most staff respondents using technology to teach practical skills, only a third used it to assess practical skills, and methods of assessment (e.g. writing) would indicate that soft skills were more likely to be assessed using technology than hard skills. This could be explained by a lack of confidence by staff and a desire for hands on experience by students. Recent research has provided some evidence to suggest that virtual objective structured clinical examinations (OSCS’s) have construct validity 31 and that digital technology can be used to decrease exam related anxiety among students.32,33 Interestingly simulated immersion in nature through virtual reality has also shown positive effects on anxiety levels when used in advance of examinations in higher level education. 34 Our work would suggest that a lack of confidence and motivation by those who teach practical skills in the health sciences is a barrier to the use of such tools for assessments. It is reasonable to surmise that greater adoption of digitally supported assessments may be seen as an increase in research which supports such methods emerges.
Situating our results in the community of enquiry framework
Distilling the results of this study and considering them in the context of the community of inquiry framework, 23 it is evident that using technology to support practical skill acquisition can provide students with a more flexible and accessible learning experience which enables revision and pre-class preparation therefore supporting social and cognitive presence. This has previously been reported in other similar studies.35,36 Our work adds to this body of knowledge but is specific to practical skill teaching. In particular students ability to control their physical environment led to feelings of relaxation comfort and reduced stress. While this is appreciated by both students and educators, it is also evident that a fully online approach is not welcome and can undermine social presence in particular, with both students and staff perceiving a lack of empathy from each other in certain instances. Further research on how to augment the social and teaching presence when using digital technology to teach practical skills in health sciences is warranted. It is worth noting when considering the results of this work that students who were in university during the pandemic years and had spent the least time on campus compared to other year groups, made up over 50% of the survey’s student respondents. Although digital technologies were defined at the beginning of the survey, many students may have utilised this survey to vent frustrations of the impact of the Covid-19 pandemic on learning, rather than to reflect on the methods and attributes of digitally enhanced teaching used to support their learning. Results indicate that in some cases, the pivot to online learning resulted in a lack of appropriate design and facilitation, detrimental to teaching presence, which in turn undermines the social presence of digitally supported practical teaching and learning. The importance of “setting the climate” to facilitate learning is highlighted. These results may be due to efforts from staff to concentrate on content which supports the achievement of learning outcomes, but with less regard to teaching presence and social presence. This outcome is understandable during a period of pivoting due to pandemic related restrictions and may reflect that those surveyed considered their teaching and learning during the pandemic rather than in the post Covid era. Indeed, the free-response boxes were often used by students to communicate strong and negative attitudes towards online learning. This contrasts with staff responses, which were often positive and hopeful towards digitally enhanced teaching tools to improve the future of learning. One explanation for these findings and the discrepancy between staff and student perspectives is that many students did not make a distinction between digitally enhanced teaching approaches using technological tools and remote online learning. Therefore, when answering the survey, many students did not consider digital tools as an adjunct to traditional teaching but as a replacement. This lack of distinction may be explained by the impact of the Covid-19 pandemic on education and the pivot to distance learning.
Looking forward
In the post Covid era, the importance of ensuring there is a balance between traditional and technologically assisted learning should help prevent ‘Zoom-fatigue’ (16) and potential burnout, while maximising the aspects of traditional teaching and technology enhanced teaching to ensure student success in each domain of the community of inquiry.37–39
Students reported a major barrier to learning was low acceptance of digital tools among staff, indicating a potential deficit in teaching presence. The factors influencing staff acceptability of digitally enhanced teaching is an area that warrants further research to improve practical skill teaching moving forward. It is encouraging that this study found that staff who received training in digital teaching tools reported improved self-efficacy in delivering and designing digital teaching materials. Thus, there is a need for continuous support to build educator confidence in their ability to select and use digital tools that will support students in meeting the intended learning objectives. This in turn will result in improved teaching presence and is especially important given the increase in different digital tools which have been reported to show promise in teaching practical skills to health science students such as virtual reality 40 and artificial intelligence. 41 Frequent opportunities for staff to upskill will also ensure educators stay up-to-date with rapidly evolving technologies while managing student expectations of what’s feasible of technology in the classroom. For example, students highlighted social media platforms as a potential teaching resource that should be better utilised by teaching staff. Whether this is an appropriate expectation of teaching staff, or an effective platform to leverage in order to achieve learning outcomes is contentious. Learning from the techniques employed by social media platforms to maintain attention and encourage engagement may be helpful when designing and delivering pre-recorded teaching materials, however it is important that pedagogy and learning outcomes are not compromised.
It is worth noting that of the 56% of staff who had not carried out digitally enhanced practical skill assessment, over one third were unsure what digitally enhanced assessment tools would be appropriate to assess varied learning outcomes. Students also described feeling frustrated when staff overused a single digital tool to support practical skill teaching. Thus, the standardisation of digitally enhanced teaching and assessment methods should be prioritised to map appropriate digital tools to learning outcomes and ensure assessment integrity. This will also be important for managing student expectations of their learning experiences and preparing them for success. For example, creating interdisciplinary guidelines detailing how to successfully set-up equipment to ensure students are supported in recording high quality skill demonstrations may improve student trustworthiness of remote grading. The current study was used to inform the creation of an Open Educational Resource which educators and students can refer to, to guide them when evaluating the suitability of a digitally enhanced tool for teaching a practical skill, or whether a skill is suitable to digitally enhanced teaching or assessment. 42 This digital resource provides an evidence base of recommendations on digitally enhanced teaching and assessment for both those who teach and those who learn.
There is also ample opportunity for those who teach to collaborate with industry and create or enhance digital education options for those involved in medicine and other health sciences. For many educators, digital technologies suitable for their teaching needs may not yet exist, in particular for the assessment of hard skills requiring haptic awareness and manual dexterity. 43
Limitations
The study’s findings should be considered alongside its limitations. Firstly, although definitions and examples were provided in the survey introduction, it’s possible that many students interpreted ‘digitally enhanced teaching’ as a pseudonym for ‘online learning’. Therefore, many student responses may have represented attitudes towards remote practical skills teaching, rather than blended teaching approaches. Future research exploring digitally enhanced practical teaching should emphasise this distinction to ensure validity. It is also worth noting that results of this study are only relevant to practical skills in the health sciences and may not translate to other areas with practical skills that may be supported by online and/or digital educational tools.
Conclusion
The current study identified the importance of maximising aspects of traditional teaching and technology enhanced teaching and ensuring a balance between teaching approaches for student success. Specifically with respect to practical teaching, there is a need to consider the effect of technology on teaching presence. While technology can lead to positive experiences within social and cognitive presences, a deficit in teaching presence due to the addition or omission of technology or reduced ability to use technologies effectively may undermine student success. Our work indicates that staff training may improve self-efficacy in delivering and designing digital teaching materials which in turn may improve the teaching presence.
Footnotes
Author note
Ethical considerations
This study has received ethical approval from the Trinity College Dublin School of Medicine Research Ethics Committee (ID 20210604).
Consent to participate
Informed consent was received from all participants before they completed and submitted the survey.
Authors’ Contributions
Both CF and AO’B made a significant contribution to the work reported. Both have drafted or substantially revised the article, agreed on the journal to which the article will be submitted. Both authors have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. Both authors agree to take responsibility and be accountable for the contents of the article.
Funding
This research was funded through an external grant from the Teaching and Learning Forum as part of the Strategic Alignment of Teaching and Learning Enhancement Funding in Higher Education 2020. The funders had no involvement in this paper from design to submission. This research helped to develop an Open Educational Resource which can be accessed for free through the Teaching and Learning Forum (registration required).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be provided by the corresponding author upon request.