
Abstract
Context
Vestibular dysfunction compromises balance and daily function, with benign paroxysmal positional vertigo (BPPV) being the most common. Vestibular rehabilitation therapy (VRT), an exercise-based intervention, enhances vestibular adaptation and symptom recovery. Tailored VRT combined with home exercises can improve adherence when aligned with recommended exercise dosing and clinician guidance.
Aims
To determine the facilitators and barriers to patient adherence to vestibular rehabilitation therapy.
Settings and Design
Cross-sectional Methods and Materials: A cross-sectional study was conducted among 60 patients aged 30–65 years receiving VRT at specialized centers. Ethical approval was obtained before study initiation. Participants completed a validated self-administered questionnaire on demographics, adherence, facilitators, and barriers to VRT participation. Data were analyzed descriptively to determine factors affecting adherence levels.
Statistical analysis used
Per-question analysis using Microsoft Excel.
Results
Of the 60 participants (61.7% females), BPPV accounted for 81.7% of diagnoses, followed by vestibular neuritis and Ménière’s disease and vestibular migraine. Over half of ongoing VRT patients had treatment duration >12 weeks, while most former patients received VRT <4 weeks. Adherence was moderate—60% maintained consistent home exercise practice. Key facilitators included therapist feedback and clear exercise instructions; main barriers were time constraints, symptom exacerbation, and motivation lapses. Overall, 73.3% rated VRT as “very effective.”
Conclusions
Adherence to VRT can be enhanced through personalized communication, structured education, and collaborative goal-setting. Addressing time limitations, symptom flares, and psychosocial challenges is essential for sustained compliance. Adaptive exercise programs supported by motivational frameworks such as self-determination theory warrant further investigation in longitudinal trials.
Introduction
Vestibular dysfunction leads to symptoms like vertigo, nausea, and instability. 1 Benign paroxysmal positional vertigo (BPPV) is the most common vestibular disorder (VD), and nearly 30% of people with dizziness experience vestibular migraine. 2 These disorders mainly impact adults and women, making daily tasks difficult and raising the risk of falls. 1
Vestibular rehabilitation therapy (VRT) is an exercise program that helps promote vestibular compensation through adaptation, substitution, and habituation. 3 VRT includes gaze stabilization exercises, habituation practices, canalith repositioning maneuvers for BPPV, and balance training to reduce symptoms and improve function.4,5 The goal is to reduce symptoms and improve function. Some exercises may initially worsen symptoms, but habituation can reduce the severity over time. 6 VRT enables patients to regain independence in their daily and social activities.
VRT is effective for various VDs, including BPPV, unilateral vestibular hypofunction (UVH) and bilateral vestibular hypofunction (BVH), Ménière’s disease, vestibular neuritis, vestibular migraine, and labyrinthitis. Customized VRT, along with personalized home exercise programs, can result in better symptom management and functional recovery. 7
Successful VRT relies on patients consistently practicing their exercises, as this encourages neuroplastic changes vital for recovery. 7 Greater adherence to the program is associated with improvements in symptoms and better functional outcomes. 7
Even with these benefits, adherence to VRT is often moderate due to factors such as lack of motivation, initial symptom worsening, time limitations, insufficient education, and limited support. 7 It is crucial to create personalized and supportive interventions that include patient education and follow-up. By addressing the barriers to adherence and identifying aids, clinicians can develop strategies that increase patient engagement with VRT.
Subject and methods
A cross-sectional observational study was conducted and data was collected from vestibular rehabilitation setups. A sample size of 59 was calculated by using the formula
Patients aged 30–65 years diagnosed with VDs receiving or having received VRT were included and those with cognitive impairments or significant comorbidities affecting participation were excluded. Age, sex, and clinical characteristics of participants were recorded.
Institutional Ethical Committee clearance was obtained prior to study commencement. Informed consent was obtained from all participants.
A self-developed questionnaire, validated by three subject experts for content validity, was administered via google form The questionnaire assessed demographics, adherence to VRT, facilitators (e.g., motivation, therapist feedback, goal-setting), barriers (e.g., discomfort, lack of time), and perceived VRT effectiveness.
Data was analyzed via per-question analysis.
Results
The study sample’s average age was 47.75 years (SD = 16.92). It included 61.7% females and 38.3% males. Figure 1 displays the prevalence of VDs among participants. Prevalence of peripheral VDs.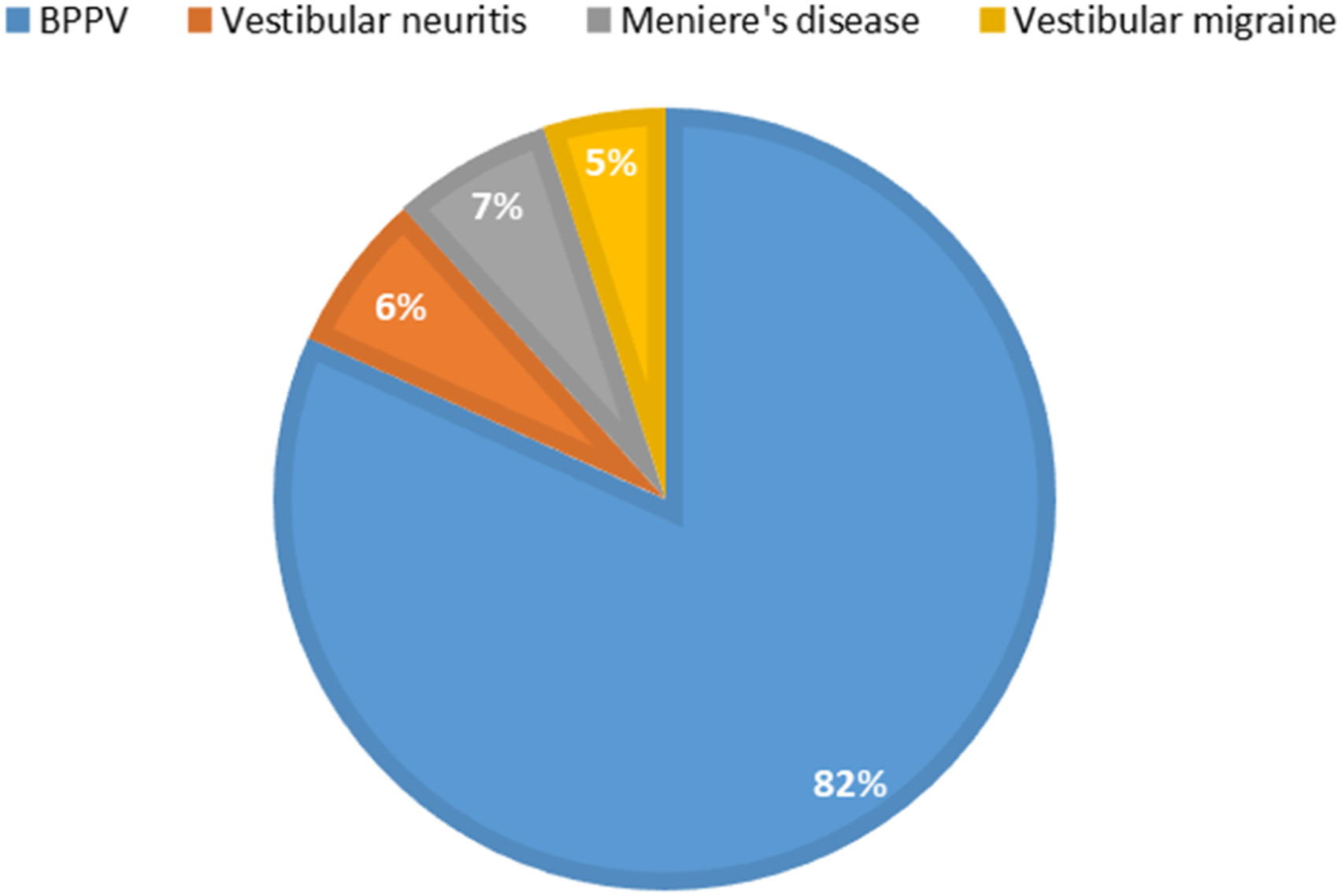
According to the data collected, 62% individuals were currently receiving VRT while 38% had received it in past.
Amongst those receiving VRT currently, 21.74% have been in treatment for less than 4 weeks, indicating they are in the early stages. Those who have been receiving VRT for 4–8 weeks represent 17.39%, while 8.70% fall within the 8–12 weeks range.
Among the participants who have received VRT in the past, a majority (55.56%) underwent therapy for less than 4 weeks, suggesting either early discontinuation or short treatment duration.
Those with a therapy duration of 4–8 weeks madeup 41.67%, reflecting a notable intermediate treatment phase. Only a small percentage received therapy for 8–12 weeks or beyond 12 weeks (both 5.56%), indicating fewer individuals completed or engaged in long-term rehabilitation. This distribution may highlight challenges in maintaining therapy adherence over time or may reflect clinical decisions tailored to patient progress.
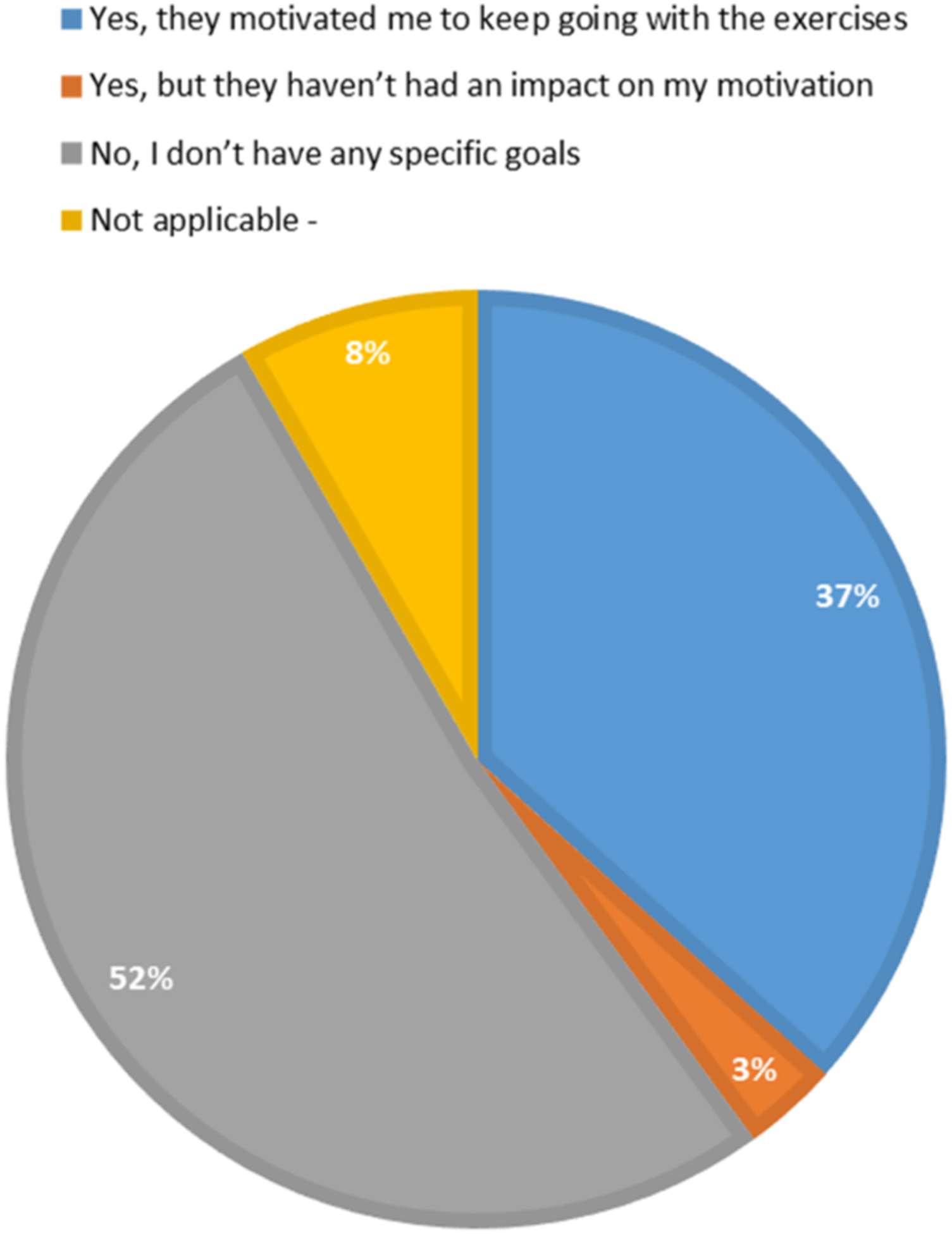
About 60% of participants reported consistent adherence. They said they “always” or “often” did their exercises, while 38.3% participated only occasionally or rarely. Figures 2 and 3 show how physiotherapist feedback influences patient motivation and how setting goals helps with exercise adherence. Influence of physiotherapist’s feedback on patient’s motivation. Effect of goal-setting on adherence to VRT.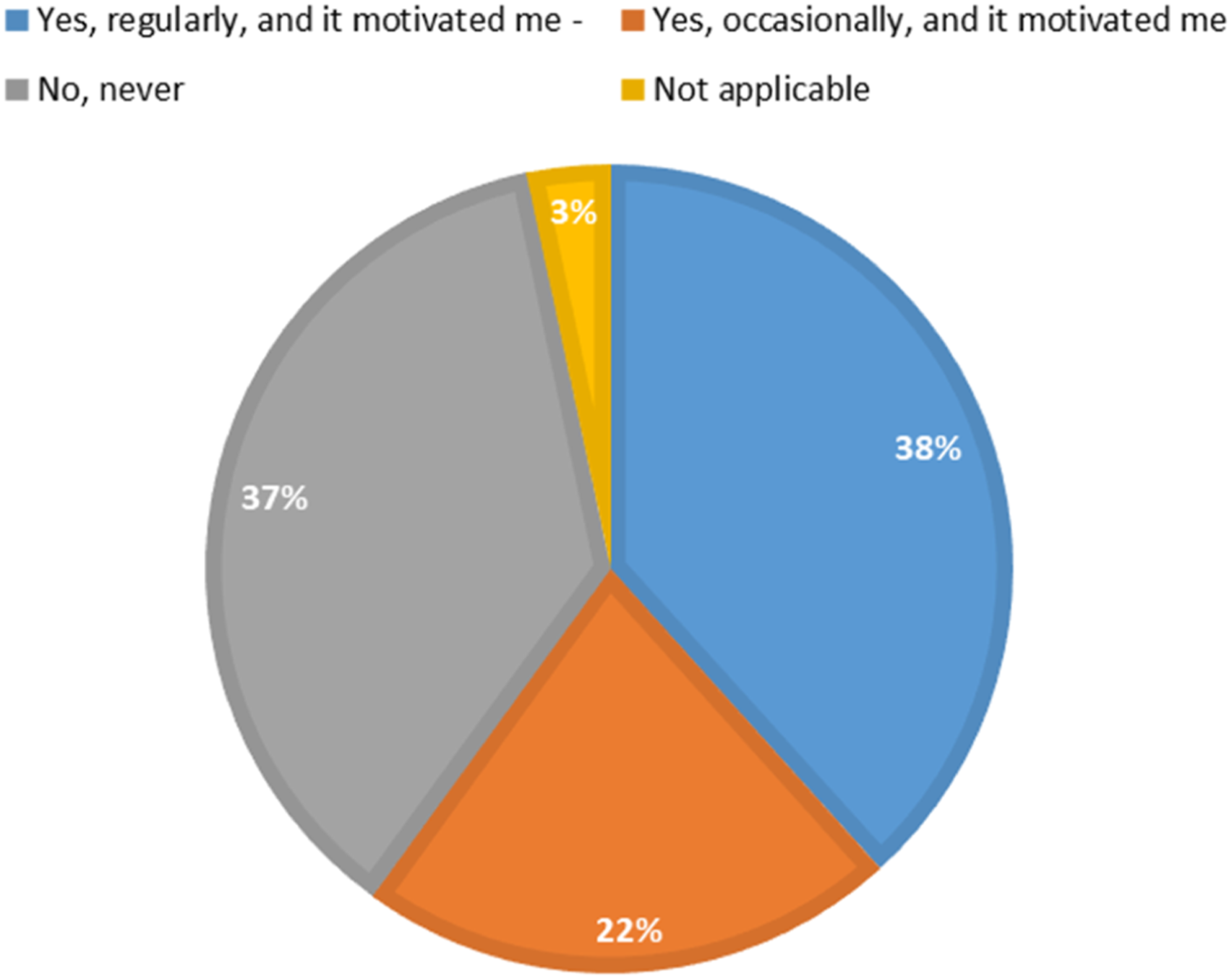
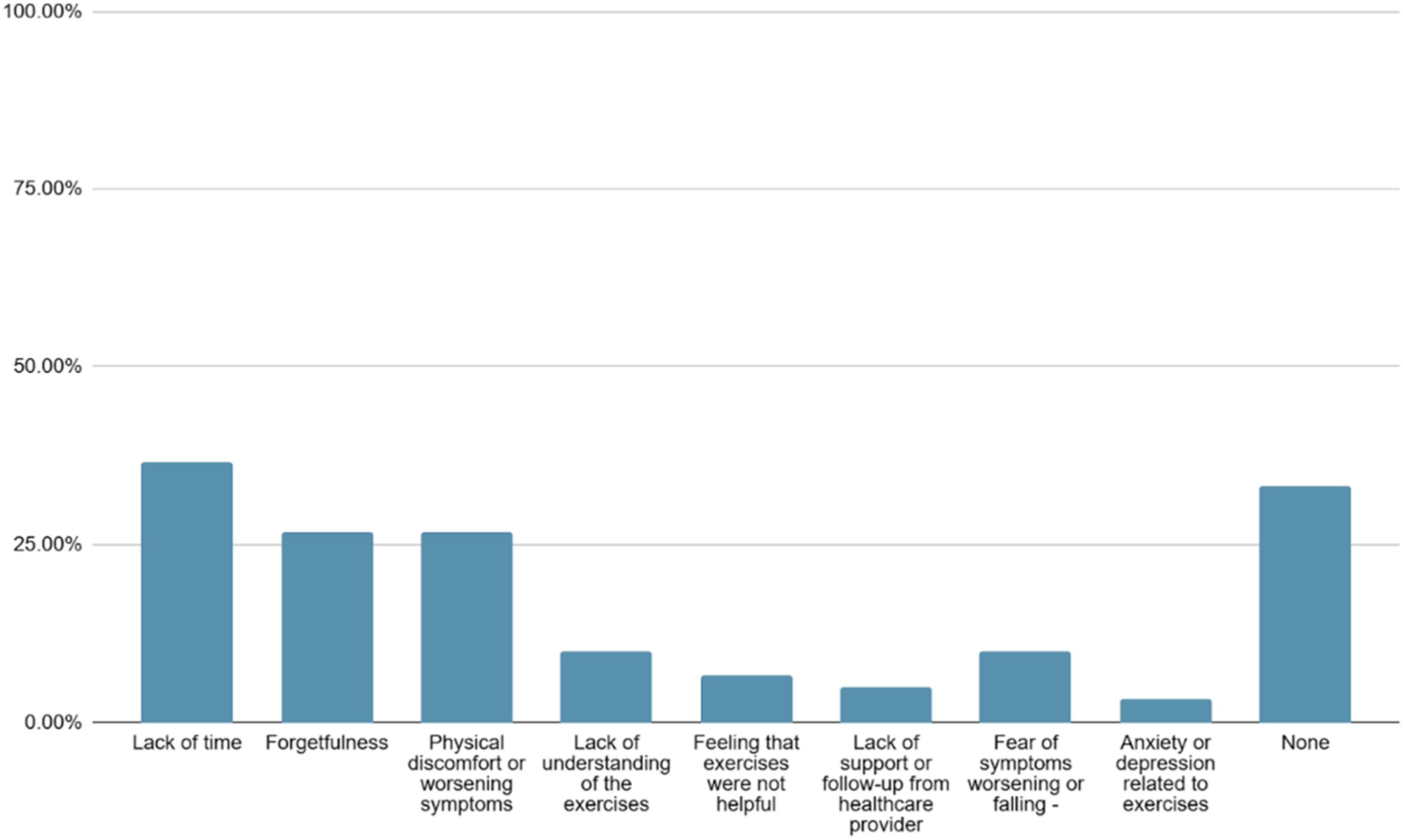
Motivation levels were high. 52% of participants reported being very motivated, and 33.3% said they were moderately motivated. Figures 4 and 5 illustrate the factors that help and hinder exercise adherence as reported by patients.
4
Facilitators to adherence to VRT. Barriers to adherence to VRT.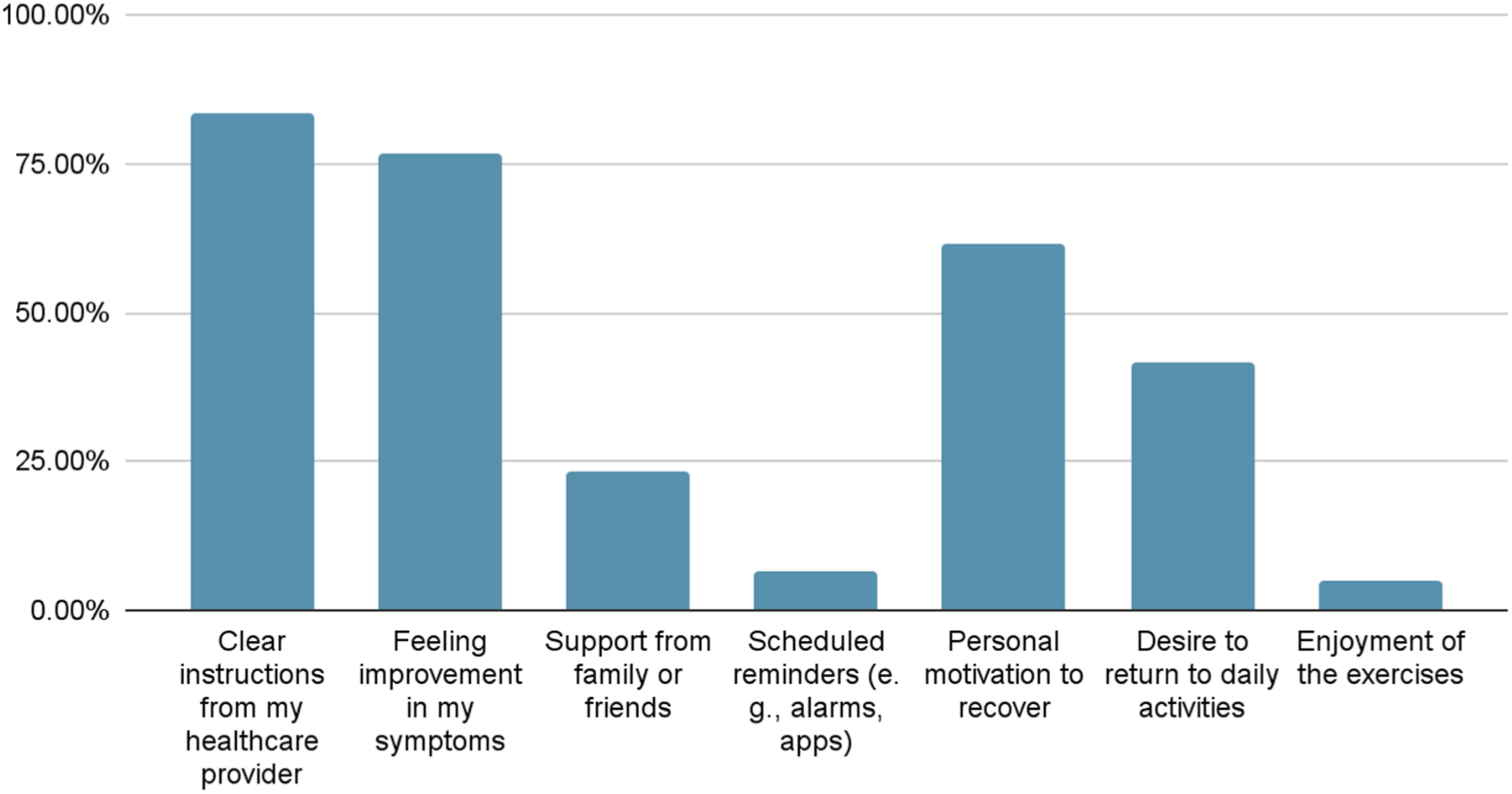
Discussion
In this study, the prevalence of VDs was predominated by BPPV which was followed by vestibular neuritis and Ménière’s disease. BPPV is the most common peripheral VD seen in the world, contributing to 20–30% of overall diagnoses of vertigo, as confirmed in the literature. The high prevalence of BPPV in this study, 81.67%, matches global data reported by Von Brevern et al. 8 It also corresponds with findings from India, where Sarkar M et al. found that BPPV caused 60.5% of peripheral VDs. 9 According to Yin et al., the higher prevalence of BPPV is mainly due to common age-related degenerative changes that cause otoconia dislodgement, increasing its frequency in the general population. 10 In contrast, vestibular neuritis and Meniere’s disease result from more specific causes like viral inflammation and other pathologies, making them less common.
These results collectively support the heterogeneity of VDs.
The predominance of VDs among females is consistent with prior literature by Ciorba A et al. 11 According to a study by Palmeri R et al., this gender disparity is thought to be influenced by hormonal and anatomical factors, including postmenopausal changes, estrogen fluctuations, and their effects on otoconial demineralization and vestibular function. 12
The adherence to VRT exercises by participants differed widely. In the current study, 35% of participants reported that they “always” did the prescribed exercises.
The adherence results in the current study are consistent with the previous literature by Im YH et al., which has shown moderate adherence rates to vestibular rehabilitation. 10 The patients with chronic VDs likely had lower adherence to VRT compared to those with acute VD because ongoing symptoms and perceived lack of benefit likely occurred during the progression of the rehabilitation. 10
The pattern of adherence shows that it is challenging to keep patients actively involved in VRT.
According to this study, participants’ motivation to engage in vestibular rehabilitation exercise was high. A positive sense of motivation is encouraging, as motivation has been recognized as a key factor that influences adherence and rehabilitation outcomes in VRT.
According to Im YH et al. and Kalderon L, motivation impacts the amount of the patient’s input, their readiness to keep the exercises in case their symptoms get worse, and their general commitment to their exercise program.10,13 Personal motivation drives individuals to maintain commitment despite challenges, supported by motivational theories that emphasize on intrinsic motivation as critical for consistent engagement. 13
When the patient is aware of the purpose as well as the expected result of the exercises and gets constant feedback, they will probably be more committed to adhering to the exercises.
51.7% lacked specific exercise goals, highlighting a gap in structured goal-setting during therapy. Absence of clear goals has been recognized as a barrier to consistent exercise adherence, suggesting that more emphasis on goal-setting between patients and physiotherapists could enhance motivation and commitment. In particular, Berengüí et al. conducted a systematic review showing that goal-setting in a rehabilitation context may improve rehabilitation outcomes through better motivation, effort and adherence. 14
The findings of this study highlight several important barriers affecting patient adherence and engagement in VRT. Time constraints were the most reported barriers, hence reflecting rehabilitation research that identifies difficulty fitting therapy into daily schedules as a key factor reducing adherence.
Importantly, issues related to non-adherence, such as forgetting sessions and experiencing physical discomfort or symptom worsening during therapy, aligning with Kalderon et al. (2024), who identified symptom provocation and time management as key barriers alongside motivational and psychosocial factors in vestibular home exercise adherence. 13
Moreover, lack of perceived support during sessions and feelings of anxiety or depression about therapy, though less commonly reported, highlight the psychosocial complexities influencing engagement thus indicating that therapeutic alliance and emotional support are crucial facilitators of adherence and positive outcomes. 15 In this study, 73.3% of participants reported VRT to be very effective in improving their symptoms. These findings align with previous research demonstrating significant symptomatic improvement and high patient satisfaction following VRT across various VDs.
Conclusion
The present study highlighted key factors that influenced adherence to VRT. Facilitators to adherence to VRT were identified as clear communication from providers to patients, patient education on the positive effects of VRT, and the involvement of patients in establishing their goals and aspects of patient-centered care. Barriers to adherence to VRT were identified as time commitments, preceded symptom exacerbations while during exercises, and psychosocial factors including anxiety and not having a support system. Addressing these barriers requires flexible and individualized approaches along with supportive communication with their therapist, education on their symptoms and being active, and awareness of setbacks or emotional responses. Future research is needed to discover personalized and patient-centered responses to promote adherence and prolonged involvement in physiotherapy to be effective for vestibular rehabilitation.
Clinical implications
Given the multifaceted nature of these facilitators and barriers—encompassing structural, cognitive, emotional, and relational dimensions—a comprehensive approach towards VRT involving scheduling flexibility, patient education, reassurance, and therapeutic support is required to optimize VRT program engagement.
Limitations of study
This study is limited by sample size, retrospective design, potential selection bias, and a lack of duration for follow-up. Limitations of this study also include its reliance on self-reported data which may be influenced by recall bias, and the cross-sectional design that restricts causal inference. The unequal disorder representation, with 81% of participants diagnosed with BPPV may limit the generalizability of the findings to other VDs.
Further scope of the study
Future Researchers should study larger and more diverse patient samples and explore the role of socioeconomic, psychological, and environmental influences on compliance with VRT. Future research should aim to include a more balanced sample of patients with various VDs besides BPPV to better understand disorder-specific factors affecting rehabilitation adherence and outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.