
Abstract
Background and objectives:
Disease-modifying treatments (DMT) have dramatically changed phenotypes in patients with spinal muscular atrophy (SMA). Because publications regarding standards of care were published before DMTs emerged, detailed recommendations and guidelines for physiotherapeutic management are still lacking. The objective of this study was to map the physiotherapeutic management of patients with SMA within the SMArtCARE network, a disease-specific registry for patients with 5q-SMA with 83 participating centers in Germany, Switzerland, and Austria.
Methods:
An online survey using a modified Delphi approach was conducted among physiotherapists with two questionnaire rounds between June 2022 and June 2023. Seven physiotherapeutic experts developed and revised the questionnaires focusing on the main topics of stretching, positioning, mobility and exercise, and chest physiotherapy. The second questionnaire was based on eight different case studies.
Results:
The second questionnaire was sent to 148 participants with a response rate of 28%. Most of the physiotherapists were well experienced in treating SMA patients. There was a strong consensus that home-based stretching should be used in pediatric patients with contractures regardless of their motor function. Muscle strengthening training was considered to be essential for all sitters and for walkers with moderate motor function restriction by a strong consensus. For all patients with respiratory involvement there was a consensus for prophylactic respiratory therapy.
Conclusion:
Our results describe the current physiotherapeutic management and recommendations within the SMArtCARE network. These findings highlight the need for an individualized approach, and the necessity of developing and adjusting existing guidelines.
Introduction
Spinal muscular atrophy (SMA) is a genetic disease caused by mutations in the SMN1 gene resulting in the degeneration of alpha motor neurons in the spinal cord. Patients present progressive muscle weakness and atrophy. However, the clinical spectrum is quite heterogeneous: On one end, there are infants with early onset of symptoms, who – without disease-modifying treatment (DMT) – never achieve the ability to sit independently. These patients often suffer from respiratory insufficiency and dysphagia with consecutive failure to thrive. On the other end of the spectrum, there are patients with onset of symptoms as late as the second decade of life. They achieve independent walking, although – without DMT – this ability is often lost during the course of the disease.1,2 Patients can be classified into three groups based on their best motor function: non-sitter, sitter and walker.
In the past years, three DMTs have been approved by FDA and EMA and dramatically changed the clinical course of SMA patients: the first DMT, nusinersen (an antisense oligonucleotide), was approved in 2016 in the USA and one year later in Europe. Onasemnogene abeparvovec (a gene therapy) and risdiplam (a small molecule) followed in 2019 and 2020, respectively. With theses DMTs new phenotypes and new challenges have emerged, which would not have been conceivable in the natural course of the disease.3456789–10
Physiotherapy for SMA patients includes physiotherapeutic (PT) assessments, counseling and treatment. PT assessments focus on the evaluation of motor function of patients, such as the Children Hospital of Philadelphia – Infant Test of Neuromuscular Disorders (CHOP-INTEND) for non-sitters, or the Hammersmith Functional Motor Scales Expanded (HFMSE) for sitters and walkers.11,12 PT counseling and treatment comprise the main areas of stretching, positioning, mobility and exercise, and chest physiotherapy. Within the SMArtCARE network, PT assessments and counseling are usually performed in combination with medical follow-up visits in specialized neuromuscular centers, while treatment is provided in physiotherapeutic practices. Physiotherapists from the SMArtCARE network work in specialized neuromuscular centers caring for a great number of SMA patients and are regularly trained in PT assessments and the management and treatment of SMA patients leading to a profound expertise. These physiotherapists usually do not treat SMA patients on a regular basis in physiotherapeutic practices.
In 2007, a committee of experts published the SMA standard of care (SOC) consensus statements. 13 The SOC guidelines have been distributed worldwide and are used by clinicians caring for SMA patients as well as by researchers in clinical trials. Although the SOC have been updated in 2017 to include physiotherapy and rehabilitation, 14 this revision was published just as DMTs for SMA began to hit the market. With the advent of new phenotypes resulting from DMTs, there is a continuous need to adjust care concepts, particularly in the field of physiotherapy. The goal of this study was to map the current state of PT management for SMA patients within the SMArtCARE network.
Methods
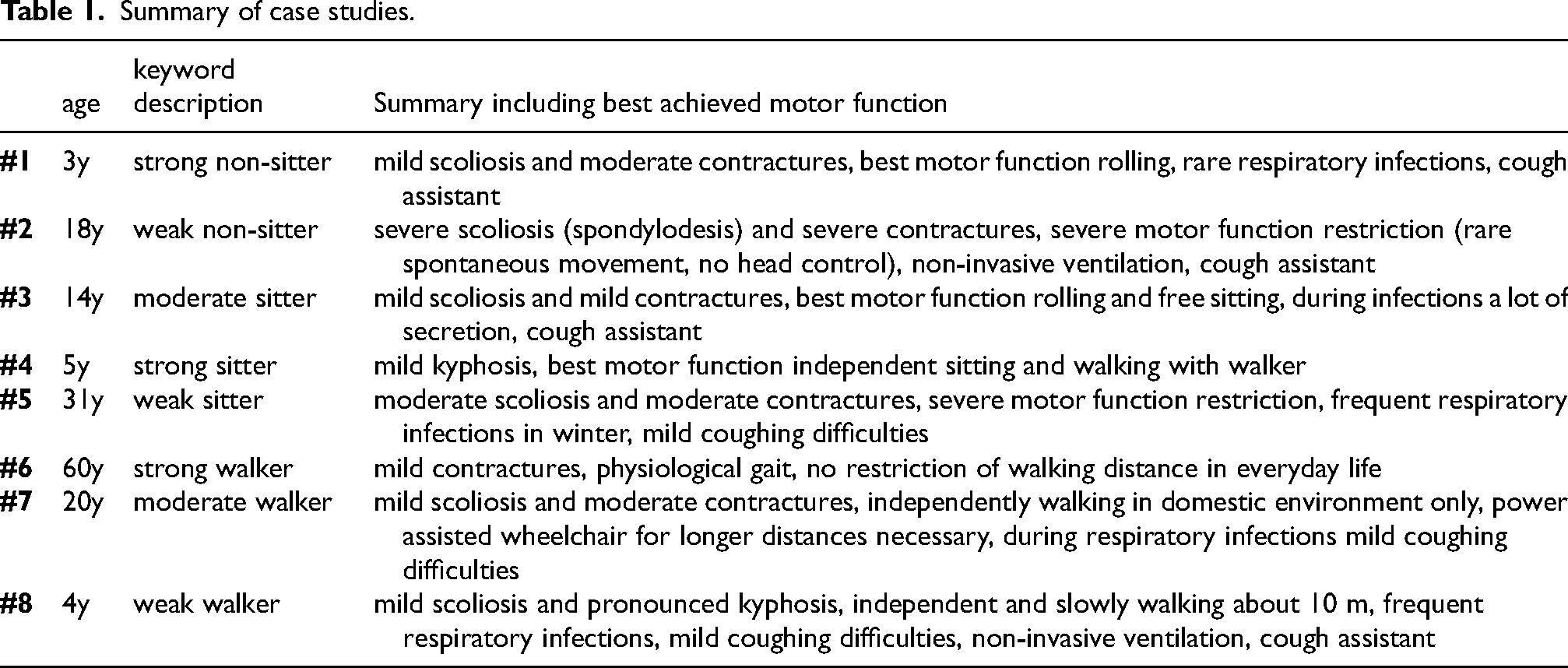
To design the questionnaire, we used a two-step approach with an initial questionnaire to identify topics of interest and a second questionnaire based on eight different case studies. Both questionnaires included four main parts on PT management: stretching, positioning, mobility and exercise and chest physiotherapy. Regarding positioning four subtopics were addressed: seat supply, supported standing training, trunk orthosis and bracing. The first questionnaire was based on the three main categories non-sitter, sitter and walker analogue to the SOC. A translation of the first questionnaire is provided as supplemental material. The second questionnaire was then adapted with 8 different case studies after receiving feedback from most of the participants requesting further clinical information to assess the necessity for the different PT interventions. Case studies were developed by an expert round based on real patients. For the case studies, patients were characterized by age, motor function (best achieved motor milestone, wheelchair use and results of PT assessments), orthopedic complications such as contractures and scoliosis, respiratory involvement and details on DMTs. To define sufficient head and trunk control, we used HINE definition (Hammersmith Infant Neurological Examination), which specifies the ability to maintain head upright consistently beyond the fifth month of life. Information on PT assessments included CHOP-INTEND, Revised Upper Limb Module (RULM), HFMSE and 6 Minute Walk Test (6MWT). Orthopedic complications, were categorized in mild (= no functional restrictions), moderate (= some functional restrictions) and severe (= functional restrictions). A summary of the case studies is displayed in Table 1, for complete case studies see supplemental material. In addition, a translation of the second questionnaire is provided as part of the overall results of the second questionnaire in the supplemental material.
Summary of case studies.
Questionnaires were sent to all physiotherapists registered in the SMArtCARE network – all working in specialized neuromuscular centers—via an online survey. As this survey was directed at both physiotherapists working with adult patients and physiotherapists working with pediatric patients, an introductory question was asked after presenting each case study, asking the participant if they considered themselves able to complete the case study based on their expertise.
Questionnaires were based on and analyzed according to the modified Delphi method. Responses were rated on a 7-point scale with 1 corresponding to “No, I don’t think it's necessary at all” and 7 to “Yes, I think it's absolutely necessary”. For data analysis, responses of 1 or 2 were considered as “disagree”, 3, 4 or 5 as “neither agree nor disagree“, and 6 or 7 as “agree”. A vote of > 95% of participants was defined as strong consensus, 75–95% as consensus, 50–75% as majority approval, and a vote < 50% was defined as no consensus.
Data were analyzed descriptively, with results presented as absolute frequencies and percentage values. After descriptive statistical analysis, flow charts were created for distinct recommendations.
Results
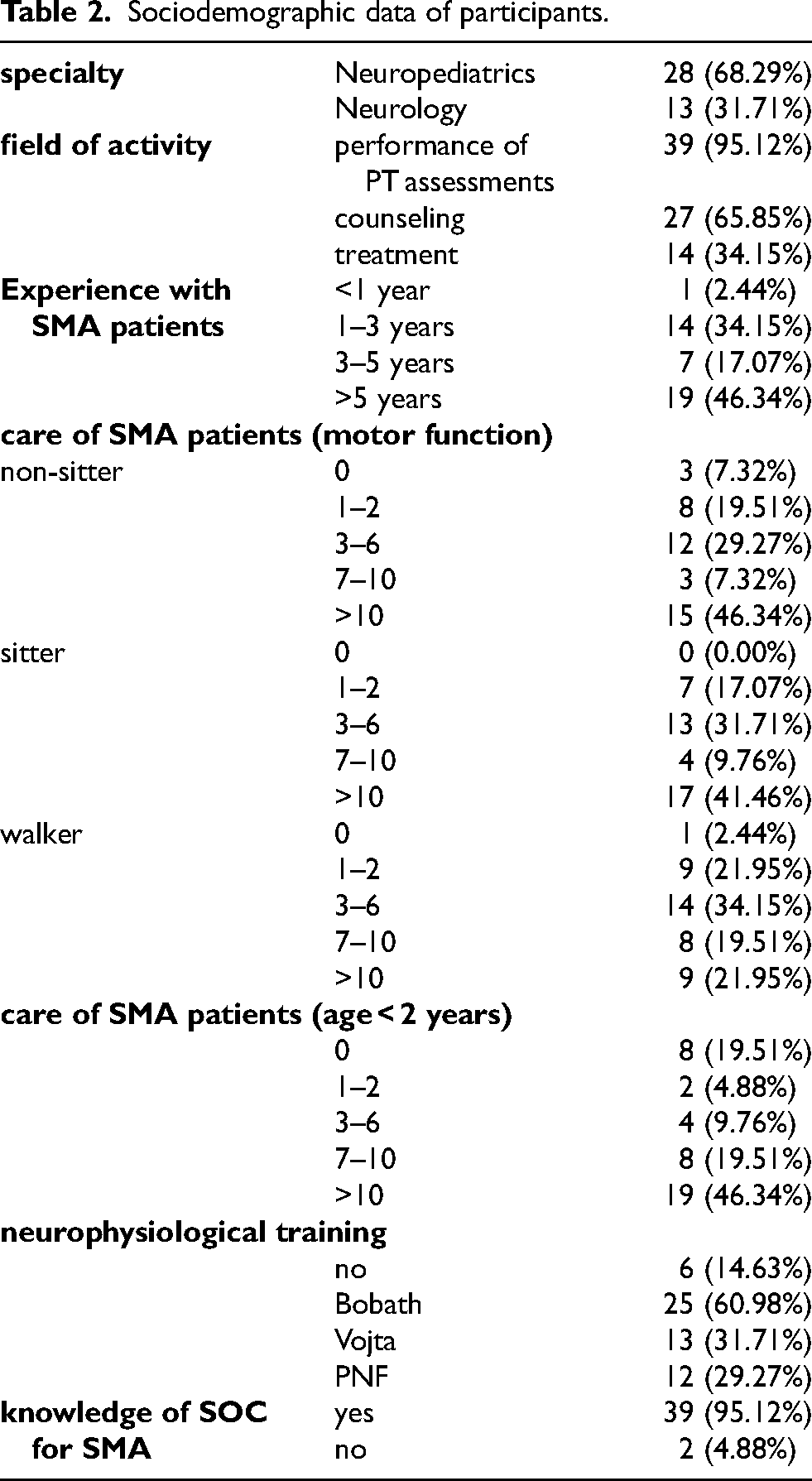
The second questionnaire was sent to 148 participants with a survey response rate of 28%. As participants only replied to case studies specific to their expertise (adult or pediatric patients), the response rate per individual case study was actually lower and ranged from 10–17%. Table 2 lists the sociodemographic data of participants. The majority of physiotherapists worked in neuropediatric departments and performed PT assessments. In addition, most participants reported several years of experience with SMA patients and being familiar with the SMA SOC. The complete results of round two with a translation of the second questionnaire are included as supplemental material.
Sociodemographic data of participants.
Stretching
There was a strong consensus to routinely perform home-based stretching in pediatric patients with contractures and a consensus for adult patients with contractures. It was recommended with a consensus to regularly instruct and review the stretches performed in everyday life by physiotherapists in pediatric patients. There were inconsistent results regarding frequency and duration of home-based stretching exercises, but there was a majority approval that stretching longer than 60 min was not considered necessary. Manual-passive stretching techniques were supported by consensus for weak non-sitters while active stretching techniques were supported for strong walkers by consensus. Positioning as stretching technique (e.g., standing device, orthosis) was recommended by consensus in strong non-sitters while it was denied by consensus for strong walkers (see Figure 1).
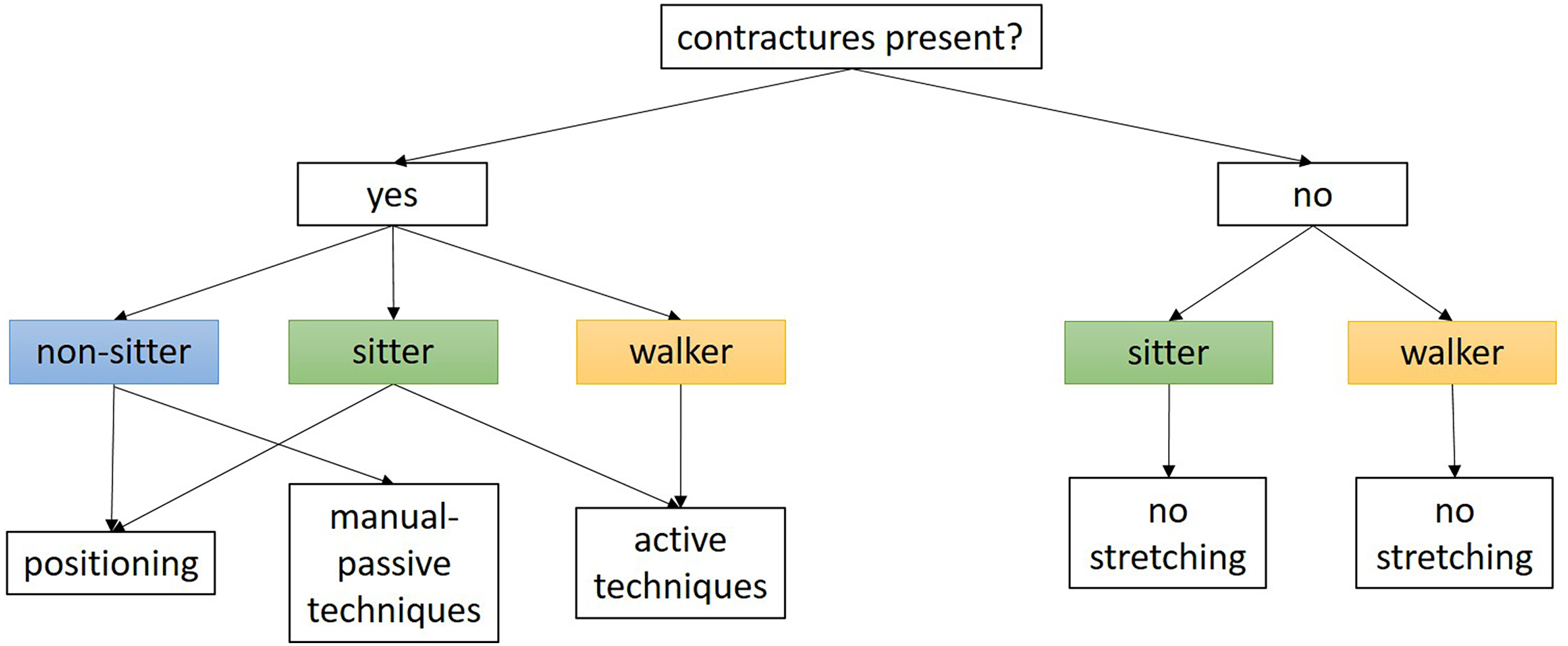
Stretching.
Positioning
A customized seat supply was proposed with a consensus for all non-sitters and for sitters with visible scoliosis.
The need for a supported standing device in non-sitters was only consented for patients with sufficient head and trunk control. For sitters, there was a consensus for supported standing training in patients with contractures but without independent locomotion (e.g., crawling, walking with walker). Again, there were inconsistent results regarding the frequency and duration of supported standing training. To regularly instruct and review the need, fit and functional adequacy of the seat and standing supply as part of the PT assessment was deemed meaningful by a strong consensus for pediatric non-sitters and by consensus for all other patients.
There was a strong consensus to recommend a trunk orthosis for non-sitters with scoliosis and kyphosis. On the other hand, there was a consensus not to use a trunk orthosis for non-sitters after spondylodesis and walkers without scoliosis. For walkers with scoliosis, a trunk orthosis was considered necessary by a consensus for pediatric patients and was denied by a consensus for adult patients (see also Figure 2).
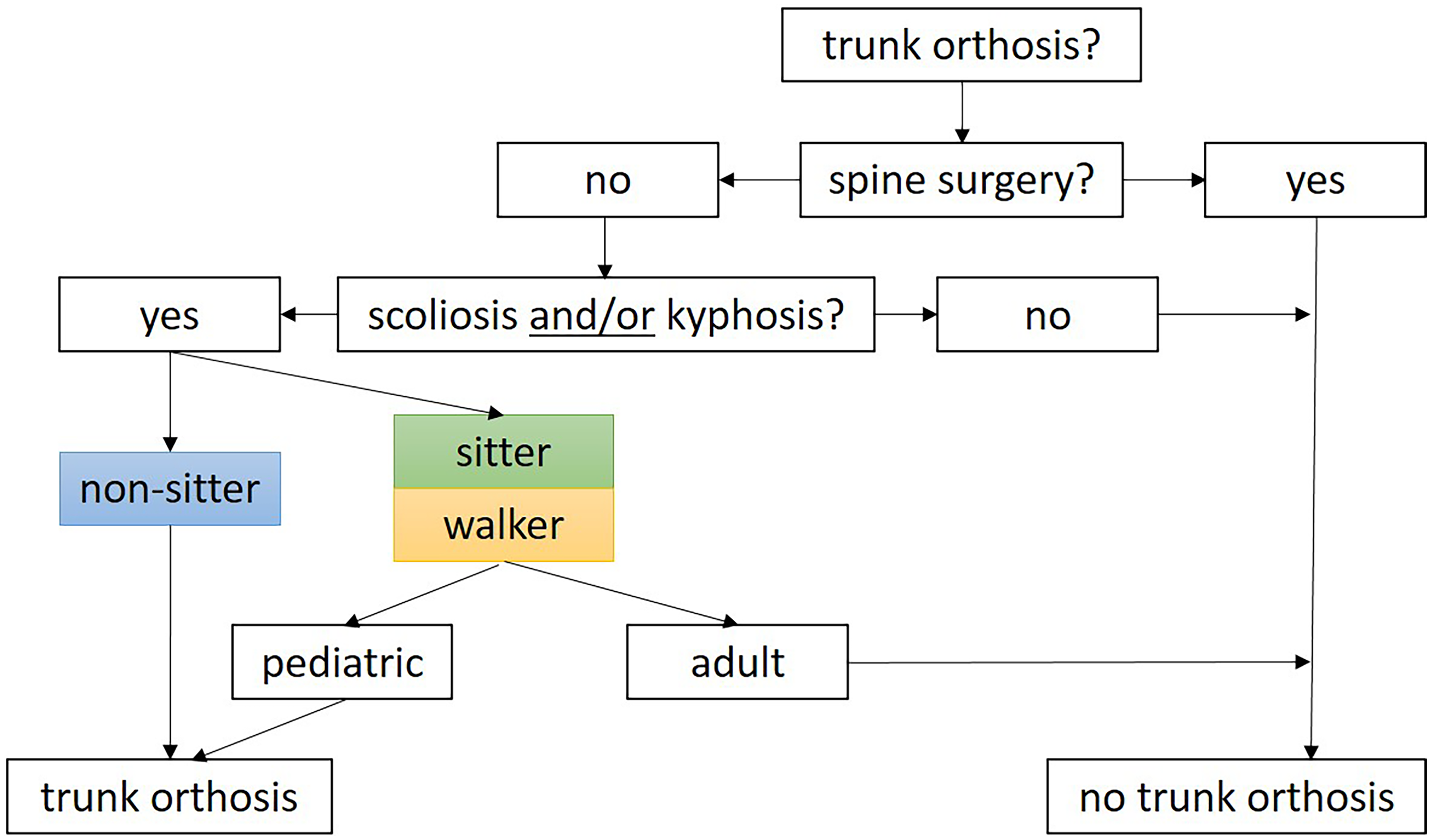
Trunk orthosis.
Braces were proposed with a strong consensus for non-sitters with moderate contractures and without severe motor function restriction. For non-sitters with severe motor function restriction, sitters with contractures and weak walkers without contractures, braces were recommended by consensus.
Mobility and exercise
Muscle strengthening training was considered necessary by a strong consensus for all sitters and for walkers with moderate motor function restriction. For non-sitters without severe restriction of motor function as well as for weak and strong walkers, there was a consensus for muscle strengthening training.
Regarding the concept and technique for muscle strengthening and activation, results were diverse. Bobath was recommended with a consensus for all children aged five years or younger. For other concepts, such as Vojta, proprioceptive neuromuscular facilitation (PNF), and other approaches, no clear results were obtained. However, not to follow one of these concepts was denied by a consensus or even strong consensus for all patients.
There was only a consensus for whole body vibration training in pediatric sitters without severe motor function restriction. Regarding the frequency of whole body vibration training there were inconsistent results. A duration of longer than 60 min was rejected for all patients.
Chest physiotherapy
For all patients with respiratory involvement there was a consensus or strong consensus for prophylactic respiratory therapy. For patients without respiratory involvement, prophylactic respiratory therapy was denied by a consensus. Regarding the technique, active and coughing techniques were deemed meaningful by a consensus in walkers but not for other phenotypes. Moreover, there was a consensus to regularly instruct and review the respiratory therapy technique and equipment performed at home for non-sitters, pediatric sitters and pediatric walkers (see Figure 3).
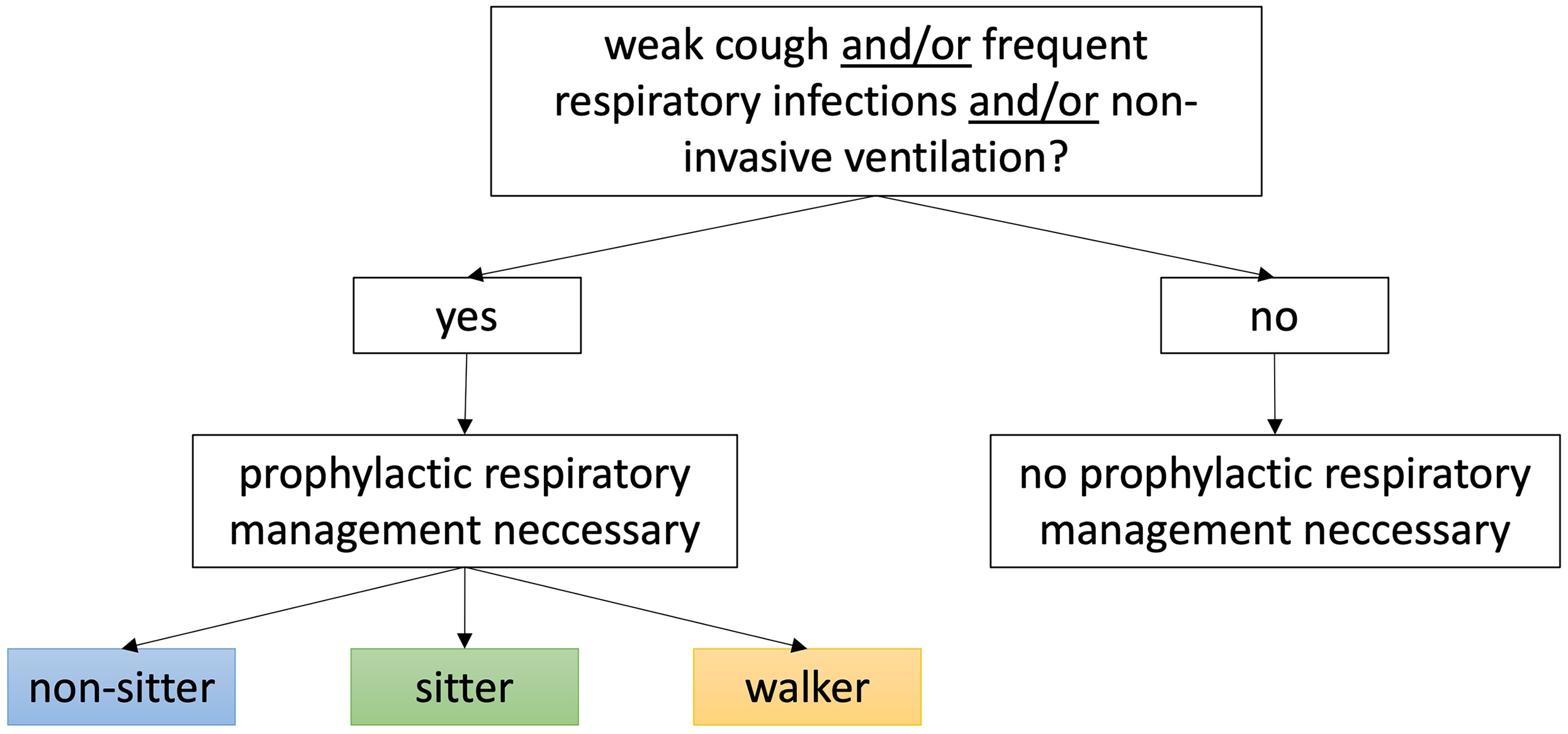
Chest physiotherapy.
Discussion
To our knowledge, this is the first study to present the current state of PT management for SMA patients in Germany and Austria. The survey response rate of 28% reflects the high relevance of the topic and the urgent need for extended and standardized recommendations for the PT management of SMA patients.
Our study incorporated eight case studies with detailed clinical information, enabling a more differentiated evaluation of physiotherapeutic management than in the current SMA SOC presented. This approach revealed important aspects to consider beyond the traditional motor function categories of non-sitter, sitter, and walker. 14 For example, our findings recommend home-based stretching interventions for all patients with contractures. There was a majority approval to even deny home-based stretching for sitters and walkers without contractures. Thus, the presence or absence of contractures was more decisive for the recommendation of home-based stretching exercises than the categorization between non-sitter, sitter, and walker. A supported standing training, recommended for sitters and non-sitters in the SOC, was also recommended in our study for non-sitters with sufficient head and trunk control, sitters as well as for walkers with severe restrictions of motor function. This result is particularly relevant in the context of new, developing phenotypes under DMTs, such as non-sitters achieving head-control or even “former sitters” achieving the ability to walk a few steps. Regarding the topic mobility and exercise, it is striking that our results recommend muscle strengthening and activation even for non-sitters without severe motor function restrictions. By contrast, SOC merely suggest “assistive technology and adaptive equipment” and only propose aquatic therapy regarding this topic. 14 When comparing our results with those of the SOC, it should be noted that the SOC was based on evidence supporting the interventions available at the time of its development, whereas our results are based on the expert opinions of physiotherapists.
Collectively, our findings highlight the importance of prioritizing individual motor function rather than focusing solely on achieved motor milestones, especially with patients turning stronger under DMTs. Whereas the SOC recommend chest physiotherapy primarily for non-sitters and sitters and suggest manual techniques, our results suggest to extend this recommendation to include chest physiotherapy for all SMA patients with impaired respiratory function. This is particularly relevant as there is evidence that respiratory function does not improve to the same extent as motor function under DMTs. 15 We here identified another important area to provide more precise recommendations on chest physiotherapy. In conclusion, our results suggest that many PT interventions require an individualized approach that should consider motor function elements such as head control, orthopedic complications such as contractures and scoliosis, respiratory involvement, and patient age. Our findings may contribute to further studies aiming to derive evidence and recommendations for the physiotherapy management of SMA patients. Most of the existing recommendations for PT management of patients with SMA lack proper evidence. For example, it is obvious that the natural course of SMA goes along with a worsening of contractures, 16 but there is an ongoing discussion whether and how contractures can be ameliorated. And while SMA SOC recommend stretching, a systematic review did not reveal clinically relevant long-term effects of regular stretching exercises regarding joint mobility, pain, spasticity, or activity in people with neurological conditions. 17 This review included diverse patient cohorts, ranging from adults with stroke, brain injury and spinal cord injury to children with cerebral palsy, Charcot-Marie-Tooth disease and Duchenne muscular dystrophy. There was no definition of how often stretches must be performed and no subgroup analysis regarding age of patients. Another systematic review on children with cerebral palsy or Charcot-Marie-Tooth disease found low-grade evidence that casting can temporarily increase ankle range of motion. 18 Comparable data for patients with SMA is still lacking. Nevertheless, there is a clear consensus that stretching should be performed at least when contractures are present, although it remains unclear whether prophylactic intervention is effective. An interview-based study on the impact of contractures on daily functioning in adolescents with SMA found that contractures did not significantly affect their daily lives, 19 indicating that treatment plans should always be adapted to patients’ individual needs. This also applies to muscle strengthening: a small randomized clinical trial involving twelve ambulatory SMA patients reported no significant change in clinical measures of motor function or strength after six months of exercise. 20 Two smaller studies observed similar results, suggesting that muscle strengthening in SMA patients can be performed safely, but evidence of improving muscle strength and/or function is still missing.21,22 Furthermore, a Cochrane review on physiotherapy for type 3 SMA patients concluded that there is insufficient evidence to determine either harmful or beneficial effects. 23 In clinical situations where evidence-based guidelines are lacking, expert opinion may bridge the gap to support clinical decisions. This, however, does not negate the need for research in this field. Such research is crucial to provide solid evidence and develop clear treatment recommendations for the PT management of patients with SMA.
The use of case studies is a strength of this study to approximate more detailed recommendations for the PT management of SMA patients. Yet, it was still not possible to comprehensively map the broad phenotypic spectrum of SMA. In our study, participants were well experienced with 95% being familiar with SMA SOC, in contrast to only 50% in a previous study among 172 American physiotherapists. 24 One limitation of our study is that we do not have sociodemographic data on those physiotherapists who were invited to take part in the survey but did not reply. Further, it should be noted that these participating physiotherapists do not regular treat SMA patients, but instead perform PT assessments and provide counselling in neuromuscular centers. However, as patients and families are free to choose their physiotherapist, it is challenging to find and contact physiotherapists who regularly treat SMA patients in physiotherapy practices for a research project. As a first step, we therefore opted for the approach of surveying the physiotherapists from the SMArtCARE network. Our results underline the importance of a regular interchange between those physiotherapists who treat patients on a regular basis and those who work in specialized neuromuscular centers doing PT assessments and holding greater expertise for the underlying disease. To develop treatment guidelines, further studies involving those physiotherapists who treat SMA patients in physiotherapeutic practices on a regular basis are required.
Conclusions
This study highlights the urgent need to review and expand existing standards of care for SMA. By emphasizing the importance of personalized interventions based on diverse clinical aspects, rather than motor milestones only, we provide results that may contribute to further research with the aim to develop comprehensive and evidence-based recommendations for the physiotherapeutic management addressing the complex and evolving needs of SMA patients across their lifespan.
Supplemental Material
sj-docx-1-jnd-10.1177_22143602251359801 - Supplemental material for Physiotherapeutic management of patients with SMA: A questionnaire-based online survey among physiotherapists within the SMArtCARE network
Supplemental material, sj-docx-1-jnd-10.1177_22143602251359801 for Physiotherapeutic management of patients with SMA: A questionnaire-based online survey among physiotherapists within the SMArtCARE network by Sibylle Vogt, Cornelia Voigt-Müller, Heidi Rochau-Trumpp, Eva Malm, Doris Roland-Schäfer, Gerda Roetmann, Judith van Vugt, Sabine Stein, Janbernd Kirschner and Astrid Pechmann in Journal of Neuromuscular Diseases
Footnotes
Acknowledgments
We would like to thank all physiotherapists who took part in the survey. We would like to thank Biogen for the support and organization of the initial kick-off workshop with all physiotherapeutic experts. Biogen did not have any influence on content and design of the questionnaires and data analysis within this project. Biogen, Roche and Novartis Gene Therapies provide financial support for the SMArtCARE registry but had no influence on data analysis and interpretation. SMArtCARE studygroup (non-author contributors): Günther Bernert, Maggie C.Walter, Susanne Goldbach, Tim Hagenacker, Hanns Lochmüller, Wolfgang Müller-Felber, Ulrike Schara-Schmidt, Kristina Probst-Schendzielorz, Matthias Baumann, Harald Binder, Maren Hackenberg, Clemens Schächter, Max Behrens, Michelle Pfaffenlehner, Astrid Blaschek, Katharina Vill, Iris Hannibal, Birgit Warken-Madelung, Annika Roser-Unruh, Marcus Deschauer, Paul Lingor, Isabell Cordts, Anne Buchberger, Ricarda von Heynitz, Petra Rau, Antonia Demleitner, Uta Diebold, Antje Schmidt, Tajana Brunckhorst, Antje Schmidt, Katharina Dörnbrack, Christina Saier, Christine Mauz, Adrian Tassoni, Tim Kampowski, Franziska Wenzel, Sven Seilnacht, Astrid Eisenkölbl, Manuel Pühringer, Marie-Luise Drax, Elisabeth Steiner, Sandra Bayer, Sandra Baumann, Johanna Feichtmayr, Nino Weiß, Harald Faninger, Katharina Kinsky, Franz- Philipp Brändle, Susanne Grinzinger, Christian Rauscher, Anna- Maria Gaese, Lisa Bratka, Elke Tiefenthaler, Marina Flotats Bastardas, Viola Horneff, Kerstin Böcking, Sabine Hettrich, Sybille Stephan-Lutter, Christine Sprengart, Isabelle Meyers, Tobias Geis, Wolfgang Wittmann, Martin Groß, Stefan Kappel, Katja Koch, Oliver Summ, Julian Großkreutz, Bernd Friedrich, Susana Cristina da Costa Pinto, Maj-Britt Bartels, Mohammad Kalaf, Kristin Loyal, Astri Fromm, René Günther, Hanna Sophie Lapp, Maren Freigang, Colin Murphy, Sybille Döhler, Tim Hagenacker, Benjamin Stolte, Jaqueline Lipka, Melina Schlag, Svenja Brakemeier, Valerie Scherwietes, Andreas Hahn, Andrea Hackemer, Lena Russ, Katharina Unverfehrt, Kyrikos Martakis, Eckard Hamelmann, Georg Classen, Efstratios Sougioultzis, Kristina Albers, Loreen Plugge, Dorothea Holzwarth, Alexandra Klotz, Stephanie Geitmann, Gabriel Dworschak, Daniel Fritzen, Ute Baur, Annika Henak, Franziska Busch, Veronka Horber, Hanna Küpper, Nadja Kaiser, Andrea Bevot, Eva Jansen, Esther Maihöfer, Birgit Meßmer, Ralf A. Husain, Heike de Vries, Anja Müller, Christa Bretschneider, Sindy Becker, Daniela Steuernagel, Sabine Borowski, Peter Huppke, Sabine Illsinger, Hans Hartmann, Barbara Ramadan, Jessika Johannsen, Deike Weiss, Jonas Denecke, Paula Steffens, Joenna Driemeyer, Christoph Kamm, Sophie Fischer, Nora Töpper, Kathleen Weinreben, Andreas Hermann, Birgit Kauffmann, Marieke Ziegler, Ulf Hustedt, Wibke Wagner, Inka Brandes, Kristin Kook, Meike Kahrs, Kirsten Fündeling-Tieletz, Jan Christoph Koch, Bettina Göricke, Tareq Mohamad Muhandes, Tobias Baum, Jörg Tiedemann, Ulrike Wolf, Mario Müller, Cornelia Köhler, Wolfgang N. Löscher, Anna Hotter, Anna Resch, Katrin Schüler, Pascal Martin, Alexander Mensch, Caroline Deborah Stapf, Ilka Schneider, Anna Katharina Koelsch, Thomas Kendzierski, Sebastian Plutz, Max Obenauf, Andreas Merkenschlager, Janina Gburek-Augustat, Gerd Meyer zu Hörste, Sarah Wiethoff, Steffen Heitmann, Marion Thomas, Mathias Müller, Tanja Zindler, Maria Rehfeldt, Christoph Neuwirth, Susanne Wäger, Jasmin Bischofberger, Christina Knellwolf, Isabella Bischofberger, Susanne Petri, Camilla Wohnrade, Bogdan Bjelica, Michaela Schwippert, Gabriela Veronika Pilshofer, Kathrin Mörtlbauer, Elke Pernegger, Tanja Neumair, Anna Elmecker, Verena Angermair, Christof Reihle, Markus Blankenburg, Sarah Braun, Michael Schroth, Lutz Dondit, Julia Haverkamp, Daniela Banholzer, Eva Wendel, Annekathrin Roediger, Robert Steinbach, Benjamin Ilse, Almut Fritsch, Saskia Beyer, Friederike Schulze-Hartung, Ben-Ole Holtz, Marvin Ritter, Ulrike Schara-Schmidt, Heike Kölbel, Adela Della-Marina, Andrea Gangfuß, Barbara Andres, Isabella Schreiner, Britta Holtkamp, Nina Rademacher, Mareike Schimmel, Daniela Angelova-Toshkina, Sabrina Geissler, Lisa Jung, Gudrun Schreiber, Oliver Schwartz, Hélène Guillemot, Timo Deba, Barbara Fiedler, Eva Johann to Settel, Geerthe Margriet Balk, Sindy Steglich, Heymut Omran, Anette Schwerin-Nagel, Barbara Plecko, Joachim Zobel, Heidemarie Pilch, Christian Stadler, Meike Steinbach, Maike Tomforde, Eva Stögmann, Georg Huber, Burkhard Stüve, Raffi Topakian, Petra Müller, Ina Krahwinkler, Regina Trollmann, Bettina Behring, Stephanie Schüssler, Raphael Seebröker, Matthias Türk, Arpad von Moers, Klaus Goldhahn, Manuela Theophil, Katharina Müller-Kaempffer, Daniela Zeisler, Kathrin Bühner, Sabine Hermann, Sylke Nicolai, Maggie Walter, Simone Thiele, Laura Grimm, Stephan Wenninger, Peter Reilich, Miriam Hiebeler, Laura Grimm, Markus Weiler, Wolfgang Wick, Sandra Schmich, Nicole Berberich, Marcel Mann-Richter, Marion Schnurr, Guido Stocker, Claudia Weiß, Corinna Stoltenburg, Angela M. Kaindl, Alexandra Wagner, Joanna Schneider, Annette George, Lieske van der Stam, Amira Abo Houf, Sabine Wider, Bianca Rippberger, Juliane Hug, Matthias Eckenweiler, Thorsten Langer, Nikolai Jung, Alexa Sonnefeld, Sebastian Friedrich, Gert Wiegand, Gert Wiegand, Gilbert Wunderlich, Claudia Wurster, Zeljko Uzelac, Kurt Wollinsky, Dorothee Lule, Johannes Dorst, Vicktoria Göbel, Beate Muschner, Janna Steinbreier, Daniel Zeller, Julia Bellut, Brigitte Brauner, Christine Leypold;
Author contributions
SV, CM, HRT, EM, DRS, GR, JVV, SS and AP were part of the expert round designing and revising the two questionnaires. CM, SV and AP performed the data analysis and wrote the first draft of the manuscript. All authors critically revised the manuscript und approved the final version.
Funding
The authors received no financial support for the research, authorship, and publication of this article. Biogen, Roche and Novartis Gene Therapies provide financial support for the SMArtCARE registry.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SV, HRT, EM, DRS, GR, JVV, SS and AP participated in the initial workshop sponsored by Biogen. SV received honoraria, consulting fees, travel support and grants/contracts for a SMA assessment training workshop from Biogen. EM received travel support from Edgewise Therapeutics. SS received honoraria, consulting fees, travel support and grants/contracts for a SMA Assessment training workshop from Biogen. JK received consulting fees and honoraria from Biogen, Novartis and Roche and participated on a Data Safety Monitoring Board from Biogen.
Data availability statement
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.