
Abstract
Purpose:
Bullying is a widespread problem in Canada and throughout the world. Children and youth with chronic illnesses or physical disabilities are more likely to be targets of bullying of all kinds. However, there is a paucity of research about bullying involving youth with neuromuscular disorders. The study aimed to assess the prevalence of bullying in youth with neuromuscular disorders and how bullying rates impact their quality of life and well-being.
Methods:
An online survey was administered at a single timepoint to youth with a neuromuscular disorder. The survey captured data about demographics, bullying frequency, quality of life, and emotional well-being. Descriptive statistics summarized demographic and bullying data. Spearman rank correlations measured the relationships between bullying prevalence and quality of life/well-being.
Results:
Twenty-nine participants completed the survey (22 male; mean age = 13 years, 10.8 months (SD = 2 years, 10.8 months). Twenty-four of 29 participants (82.8%) had been bullied at some point in their life. Participants reported being bullied most frequently for their appearance and their disability. Bullying did not correlate with quality of life and well-being.
Conclusions:
Participants with neuromuscular disorders reported high rates of bullying without impacts on quality of life and well-being. We posit participants exhibit resilience.
Introduction
Bullying is a pervasive problem that transcends borders, impacting children and adolescents globally. 1 Bullying is defined as an unwanted aggressive behavior that involves an actual or perceived power imbalance, is repeated or likely to repeated, and may cause harm or distress to the individual being bullied. 2 Bullying manifests in numerous forms, such as physical (e.g., hitting, pinching, destroying or stealing belongings), verbal (e.g., name-calling, teasing, spreading rumors), social (e.g., excluding someone, scapegoating, humiliating others), as well as cyber (e.g., using the internet or text messaging to intimidate, put-down, spread rumors). 3 Persons who experience bullying, perpetrators, and witnesses all play roles within bullying dynamics and individuals may take on multiple roles. 4 Research has shown that at least one in three youth report having experienced bullying at some point in their life. 5 In Canada, over 50% of school-aged youth have reported being bullied at some point in their life with these rates dropping to 40% during the covid-19 pandemic. 6 Yet children and youth with chronic disorders experience even higher rates of bullying (Odds ratio [OR] = 1.65) than children without disabilities. 7 Specifically, children with a chronic physical illness and/or physical disability (including obesity, asthma, chronic skin diseases, visual impairments, spina bifida/cerebral palsy) were more likely to be targets of all types of bullying including physical (OR = 1.47), social (OR = 1.47), verbal (OR = 1.67), cyberbullying (OR = 1.29), and illness-specific teasing (OR = 5.29), specifically if the illness was visible. 7
Despite increasing awareness and anti-bullying strategies, bullying remains a significant issue with far-reaching consequences. 1 Repercussions from bullying in children and youth are profound and mutli-faceted. Short- and long-term impacts of bullying include declines in physical and psychological well-being, social relations, and academic performance.7–9 Children and youth who have experienced bullying report increased risk of anxiety, depression, self-harm, and suicidal thoughts, with these risks extending into adulthood.10–12 A decline in physical and psychological well-being, social relations between peers and parents, and school environment have negatively impacted quality of life (QoL) of school-aged children and adolescents. 13
Despite extensive research on bullying among children with visible and non-visible disabilities,14–16 there is a noticeable gap in research studies focusing on youth with progressive muscle weakness conditions or neuromuscular disorders, such as myopathies and spinal muscular atrophy (SMA). These neuromuscular disorders lead to significant physical challenges, requiring reliance on caregiver and assistive technologies. Particularly, youth with neuromuscular disorders may be impacted by bullying in other ways. For example, the psychological impacts may manifest as withdrawal or decreased communication not only with peers, but caregivers such as healthcare providers, leading to negative impacts on engagement in their medical care.17–19 Given these medical factors such as muscle weakness, difficulty ambulating and increased fatigue, as well as the risk of impact on engagement in care, it is imperative to understand the bullying experiences of youth with neuromuscular disorders.
This study aims to fill the gap by identifying the prevalence of bullying among youth with neuromuscular disorders and examining the impact of bullying on their quality of life and well-being. By addressing this critical issue, the study seeks to provide additional knowledge pertaining to the impact of bullying on vulnerable populations while informing strategies to foster resilience and support for affected youth.
Methods
Design & procedure
This study was approved by the research ethics boards at Holland Bloorview Kids Rehabilitation Hospital and the Children's Hospital of Eastern Ontario. This study was part of a larger cross-sectional, multi-center, mixed methods study. Data was collected in two phases: (1) a survey was administered at a single timepoint to youth and optionally to caregivers; (2) the dyad was invited to complete a semi-structured interview (see Chatur et al., 2024). 20 The current article focuses on findings from the youth survey. The survey asked questions about four topics: demographics, bullying experiences, QoL, and their well-being. All participants provided informed consent prior to participation.
Participants
A convenience sample of youth from a Holland Bloorview Kids Rehabilitation Hospital in Toronto, Canada and the Children's Hospital of Eastern Ontario in Ottawa, Canada were recruited from neuromuscular clinics.
The inclusion criteria included: (1) confirmed diagnosis of a muscular dystrophy, congenital-onset neuromuscular disease (i.e., congenital myopathy, congenital muscular dystrophy, congenital myasthenic syndrome) or SMA; (2) aged 10–19 years old; and, (3) the ability of the participant to read and communicate in English or French.
Outcome measures
Demographics
A purposefully developed form captured participant characteristics, including age, gender, family demographics (e.g., highest level of parent/guardian education), schooling, neuromuscular diagnosis, comorbidities, physical function, and technology use. The form contained 19 items and six possible branching items.
Bullying experiences
The Bullying and Cyberbullying: Perpetrators, Victims and Witnesses Survey (B&C:PVWS) by Mishna et al. (2012) was adapted with permission to identify bullying and cyberbullying experiences. 21 Questions examined the frequency of experiences in the participant's life, types of bullying experienced, and reasons for bullying in the past 30 days on four-point Likert scales (never, once or twice, 3 or 4 times, every day). For the bullying frequency and reasons for being bullied items, experiences in one's life were added to account for possible impacts of the covid-19 pandemic.
Qol
The KIDSCREEN-10 Index was used to measure health related QoL through a 10-item questionnaire. 22 Items asked participants their thoughts on their health over the past week on a five-point Likert scale (excellent, very good, good, fair, poor). Rasch analysis of raw scores provided a global unidimensional latent HRQoL score. Higher scores indicate better HRQoL.
Well-being
The EPOCH Measure of Adolescent Well-being assessed five positive psychological characteristics (i.e., engagement, perseverance, optimism, connectedness and happiness) that may facilitate the well-being, physical health, and other positive outcomes into adulthood. 23 Participants were instructed to indicate how much a statement described them on a five-point Likert scale (almost never, sometimes, often, very often, almost always). There were four items for each of the five domains.
Data analysis
Descriptive statistics (i.e., mean, frequencies) summarized demographic and bullying frequency data. Spearman rank correlations measured the relationship between bullying rates, and QoL and well-being. Analysis was conducted using SPSS (Version 25, IBM Corp, Armonk, NY).
Results
Twenty-nine youth completed the survey. Demographic data are available in Table 1.
Sample demographics.
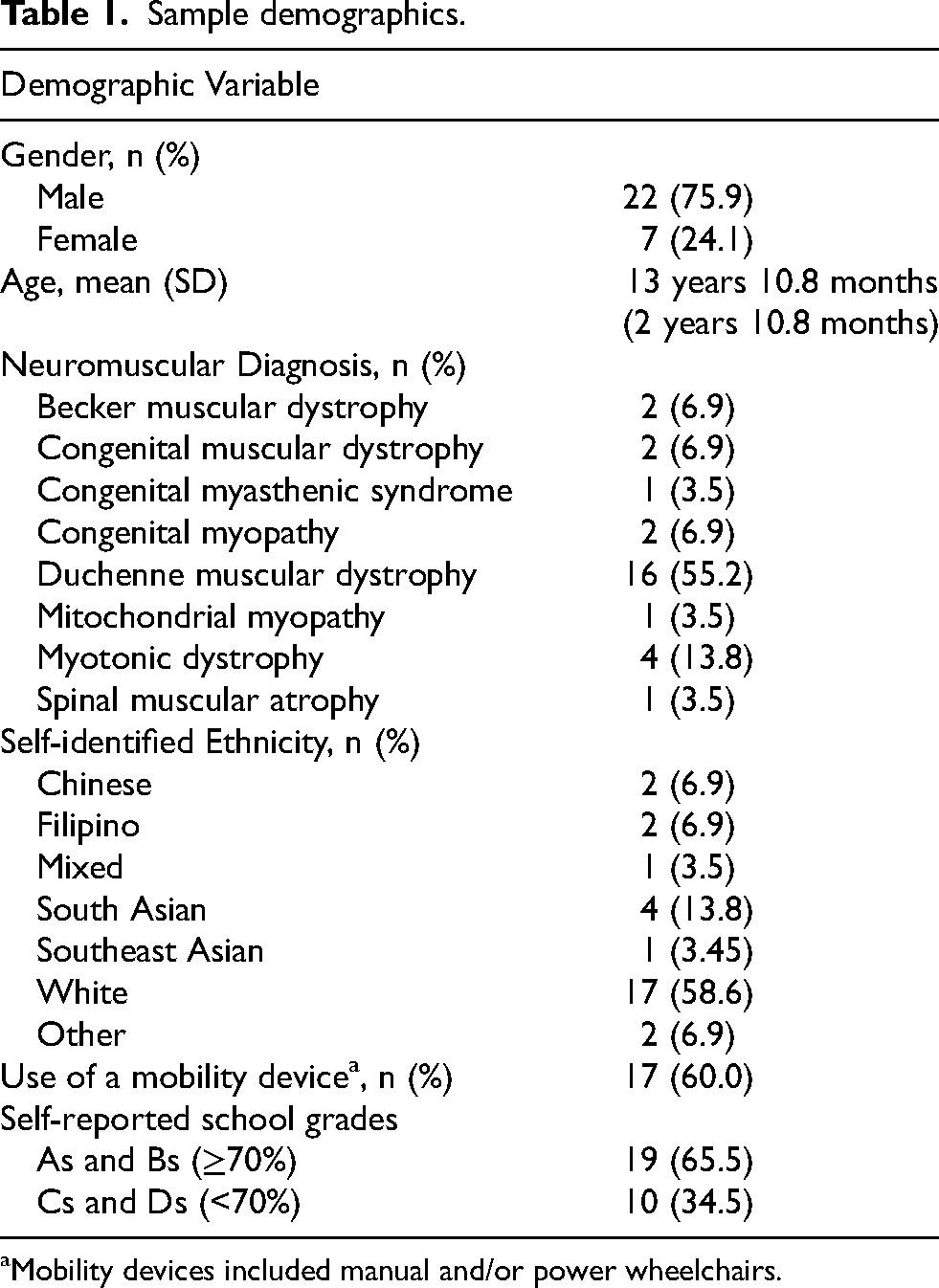
Mobility devices included manual and/or power wheelchairs.
Twenty-four of 29 participants (82.8%) reported that they had been bullied at some point in their life (Table 2). Over participants’ lifetime, social bullying was the most prevalent type of bullying experienced. Three participants indicated they had been bullied every day, however when participants were subsequently asked about specific types of bullying, a greater number of participants said they were verbally bullied every day (n = 4).
Frequency of bullying types experienced.

N = 24 as only those who indicated they had been bullied in their life answered the question on types of bullying.
Of the 24 individuals who reported being bullied in their life, the most common reasons for being bullied were their appearance (n = 13, 54.2%) and their disability (n = 15, 62.5%). An association matrix is represented in Table 3. A negative correlation would indicate higher rates of bullying are associated with worse QoL/well-being. In most cases, no statistically significant relationships were measured. Notable negative associations included bullying because of one's school marks with both QoL (ρ = −0.56, p < 0.001) and the connectedness well-being domain (ρ = −0.46, p = 0.02).
Frequency of type of bullying and reasons for bullying versus QoL and well-being domains.
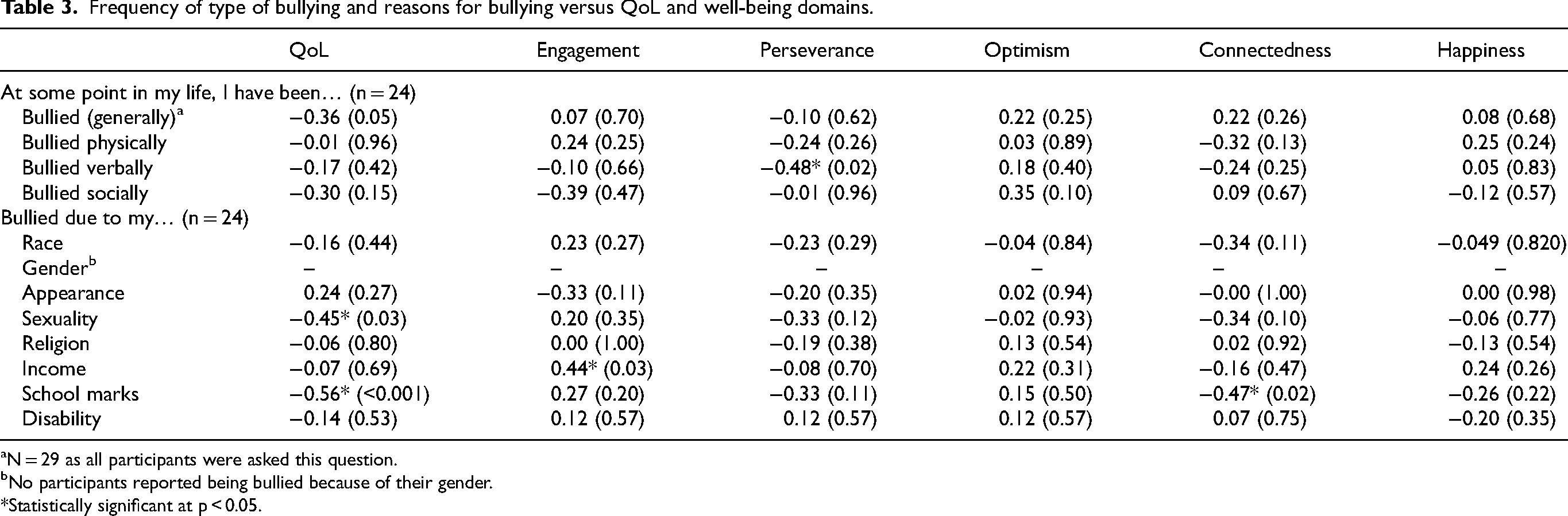
N = 29 as all participants were asked this question.
No participants reported being bullied because of their gender.
*Statistically significant at p < 0.05.
Since being bullied because of one's school marks was associated with both worse QoL and connectedness, participants’ experiences at school were investigated further through the specific QoL question, “In the last week, have you got on well at school?” Of those reported having been bullied due to their school marks (n = 7), only 2 (6% of bullied) participants got on very well or extremely well compared to those who were bullied for other reasons (n = 13, 54% of bullied) or not bullied at all (n = 4, 80% of not bullied).
Most correlation tests detected no relationship between the frequency of bullying (type and reason) and QoL/well-being. For example, all items within the optimism and happiness well-being domains, such as having fun with friends, being optimistic about one's future, and loving life did not have significant relationships with bullying frequency. Furthermore, higher rates of social bullying were positively correlated with a belief things will work out no matter how difficult they seem (ρ = 0.41, p = 0.05).
Discussion
Bullying in youth with neuromuscular disorders has not been well described to-date. The current study presented the prevalence of traditional bullying experiences and its impact on QoL and well-being in a sample of Canadian youth with neuromuscular disorders. Some level of bullying was identified by 82.8% of participants, which is greater than the approximately 30% reported in large-scale studies with school-aged children and youth,5,6,24 yet in line with other survey-based studies reporting that 90% of youth with disabilities have been bullied in their lifetime. 25 Physical bullying was the least prevalent type of bullying reported with 24% of participants having experienced physical bullying; however, the prevalence reported in this study is greater than school-based studies that report physical bullying frequencies between 10–12%. 24 Verbal and social bullying were also observed to be much higher than in school-based population at 87.5% vs. 24–40% and 83.3% vs. 21–44%, respectively.5,24,25
Notably, most of the types of bullying experienced (i.e., physical, verbal, social) were not statistically associated in either direction with QoL or well-being (except verbal bullying vs. perseverance; ρ = −0.48, p = 0.02), which was unexpected based on previous literature. For example, an Australian study of school-aged children identified significantly lower scores in emotional well-being, including happiness, life satisfaction and emotional regulation in those who experienced bullying at some point in their life compared to those who were never bullied. 24 Additionally, a systematic review by Dubey at al. (2022), concluded that adolescents’ health-related QoL declined when they experienced bullying. 13 However, based on interviews with the same participants as the present study, Chatur et al. (2024) reported that participants described having decreased sensitivity to bullying over time by deciding they did not care, laughing off the experience, the provision of social support and facilitating prevention strategies, among other strategies. 20 Interview participants noted that these strategies helped them minimize the personal burden of being bullied. These findings from both the interview and survey-based studies suggest that these youth with neuromuscular disorders do not believe their quality of life or well-being have been impacted by bullying.
While type of bullying was not observed to impact most aspects of participants’ QoL or well-being, several of the reasons for which participants reported being bullied did impact QoL and/or well-being. From an examination of the reasons for being bullied and their relationships with participants’ well-being and QoL, issues surrounding participants’ experiences at school were observed. Particularly, participants who experienced bullying reported having a worse time at school (KIDSCREEN) and made less connections with their peers at school (EPOCH). Several reasons for these experiences are hypothesized. These observations of lower QoL and well-being may be due to higher rates of bullying alone, however lower QoL/well-being may be attributed to fewer opportunities to build relationships at school due to missing school for medical appointments, deteriorating health, or other health-related issues.26,27 Moore et al. (2017) suggested that having stronger relationships and connectedness may reduce bullying directly when children/youth receive social support (e.g., strength in numbers) or indirectly when peers provide comfort or counseling. Based on the results from this study, youth with neuromuscular disorders may need additional interventional support to achieve adequate connectedness for it to be a protective factor. 28 With that, it is recommended that clinicians address relationship development in neuromuscular clinic visits and coaching programs tailored to children with neuromuscular disorders.
Youth with DMD represented over half the sample. While we believe the study's findings are generalizable to the neuromuscular community experiencing progressive muscle weakness, we understand youth with DMD may have different experiences. For instance, youth with DMD may have specific social difficulties due to neurodevelopmental differences in social processing. Specifically, many youth with DMD experience neurobehavioural conditions (e.g., ADHD), learning differences (e.g., learning disability, intellectual disability), psychosocial disorders (e.g., anxiety, depression), and physical limitations that make it difficult to keep up with peers, 29 which may compound to decreased social connectedness and relatedness which are important factors related to bullying prevention. This supports the significant relationship between being bullied due to one's marks and lower connectedness. On the other hand, the high proportion of youth with DMD may also impact the overall findings of quality of life. The DMD literature reports that youth with DMD report similar levels of quality of life to their peers 30 whereas individuals with Facioscapulohumeral muscular dystrophy (although there were no participants in this study) report difficulties during social interactions due to fear of social rejection due to facial weakness, leading to lower quality of life. 31 There are many types of experiences within the neuromuscular community. Overall, it is suggested that similar interventions targeting social connectedness is important to build trust and positive relations between peers even if these social difficulties are not directly related to bullying experiences.
Study findings suggest that participants exhibited protective factors against commonly reported impacts of bullying (i.e., lower QoL and well-being). Participants may have strong resiliency capacities. Resiliency is the ability to adapt and thrive despite adversity, 32 defined through personal protective factors like: (1) mastery—opportunity for individuals to interact with and enjoy relationships in their environment (optimism, self-efficacy, adaptability); (2) relatedness—capacity to be in a relationship (trust, support, comfort, tolerance); and, (3) emotional reactivity—threshold of tolerance prior to the occurrence of an adverse event (sensitivity, recovery, impairment). 33 Resiliency emerges as a crucial protective factor against the adverse effects of bullying. 20 Indeed, those with a disability often experience adversity that could lead to the development of different psycho-emotional attributes. Taking Moore's factorial model of resilience, 33 important derivations can be extracted from the current study. Participants reported no deficits in the optimism well-being domain (i.e., having positive attitudes about one's life both now and in the future) even when higher rates of bullying were reported. Additionally, perseverance, part of grit and in line with self-efficacy, was shown to be stable even with higher rates of bullying. Overall, participants did not exhibit lower levels of the well-being components that contribute to the mastery factor of resiliency, even though that is a commonly reported in the literature. 13 To summarize, study participants endorsed stable mastery (i.e., optimism, self-efficacy, adaptability) and low levels of relatedness (i.e., trust, support, comfort, tolerance) at school. Emotional reactivity was not addressed. In line with Moore and Woodcock (2017), the youth with neuromuscular disorders in the current study would benefit from bullying prevention strategies encouraging relatedness between peers (e.g., social skill programs, peer support networks, etc.). 28 Stable mastery in the face of experiencing bullying may promote participants’ desire and perseverance in working towards program goals.
While resilience was suggested as a protective factor in this specific study, there is little to no research on resiliency in youth with neuromuscular disorders in which to compare the findings. Future research should focus on children and youths’ response to bullying, as well as neuromuscular disease progression and life attainment. It is recommended that a nationwide Canadian survey study with validated resiliency measures is conducted for a larger and more generalizable sample size.
Limitations
There are several limitations to this study. Firstly, the sample size was small due to recruitment barriers (i.e., covid-19, family time). Data collection was impacted by the covid-19 pandemic. To minimize this barrier, an additional question was added to the bullying frequency survey of “I have been bullied in my life…” instead of only asking about the previous 30 days. Participants completed the survey through different restriction and quarantine points of the pandemic. This recollection of bullying may underestimate the true rates as this survey was performed at a time where covid-19 regulation for isolation was in effect. Furthermore, while the KIDSCREEN-10 is a validated measure to understand youth's QoL, it provides only a simplified estimation. There may be more nuanced aspects of the participants’ QoL that was unable to be captured with the KIDSCREEN-10. With the use of convenience sampling, there was over-representation of youth with Duchenne muscular dystrophy, (n = 16, 55.2%) as this disorder has an incidence of 3500–5000 live births and only impacts males. 34
Conclusions
A sample of Canadian youth with neuromuscular disorders was surveyed about their bullying experiences (frequency, type) and their QoL and well-being. Over 80% of participants experienced bullying in their lifetime, which is greater in frequency than general school populations (30%). Trouble at school impacted QoL and connectedness, while all other types of/reasons for bullying had no relationship with QoL or well-being. It is hypothesized that the general stability of the participants’ QoL and well-being, regardless of their levels of bullying experienced, is related to resilience. Participants showed stable mastery resilience, but lower relatedness resilience. We recommend that clinicians focus on building resiliency, and specifically relatedness. A cross-Canada survey with validated resiliency measures for a larger cohort is recommended.
Footnotes
Abbreviations
Acknowledgements
We would like to thank Emilie Hill-Smith from the Children's Hospital of Eastern Ontario for her support in participant recruitment and study operations. Lastly, we would like to thank all the participants and their caregivers who participating in the study.
Ethical considerations
This study was approved by the research ethics boards at Holland Bloorview Kids Rehabilitation Hospital and the Children's Hospital of Eastern Ontario.
Consent to participate
All participants provided informed written consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Academic Health Sciences Centre Alternative Funding Plan (AHSC AFP) Innovation Fund (HBV-20-001).
Declaration of conflicting interests
HL receives support from the Canadian Institutes of Health Research (CIHR) for Foundation Grant FDN-167281 (Precision Health for Neuromuscular Diseases), Transnational Team Grant ERT-174211 (ProDGNE) and Network Grant OR2-189333 (NMD4C), from the Canada Foundation for Innovation (CFI-JELF 38412), the Canada Research Chairs program (Canada Research Chair in Neuromuscular Genomics and Health, 950-232279), the European Commission (Grant # 101080249) and the Canada Research Coordinating Committee New Frontiers in Research Fund (NFRFG-2022-00033) for SIMPATHIC, and from the Government of Canada, Canada First Research Excellence Fund (CFREF) for the Brain-Heart Interconnectome (CFREF-2022-00007). All other authors have no interests to declare.
Data availability
The datasets generated during this study are not available for secondary use.