
Abstract
Objective:
In patients with Duchenne muscular dystrophy (DMD) the effect of continued corticosteroid (CS) use into adulthood on respiratory function remains unclear. We studied if prolongation of CS into adulthood is beneficial for forced vital capacity (FVC), age at start of non-invasive ventilation (NIV), and age at start of continuous (24/24 h) ventilation.
Methods:
In this retrospective study, adult (≥18 years) DMD patients were stratified into 20 ‘CS-naïve’ patients (never used CS or only as a child during <1 year) and 37 ‘continued CS’ patients (continued CS until age of 18 years or older).
Results:
‘Continued CS’ patients showed at 18 years a higher FVC%pred (50.3, SD:16.4) compared to ‘CS-naïve’ patients (36.9, SD:13.8) (p = 0.007). Patients continuing CS beyond the age of 18 demonstrated a slower annual decline in FVC%pred of 2.9% (SE:0.5) in comparison to 3.8% (SE:0.4) in the ‘CS-naïve’ group, and the difference in relative annual decline in FVC%pred was significant (p = 0.012). The annual decline in FVC in absolute value in patients continuing CS was 102 ml (SE:28) slower in comparison to ‘CS-naïve’ patients (p < 0.001). Moreover, there was a delay in age at initiation of NIV: mean age at start of NIV was 28.3 (95%CI: 25.4–31.2) in ‘continued CS’ in comparison to 20.3 (95%CI: 19.0–21.6) in ‘CS-naïve’ patients (p < 0.001), and at start of continuous NIV 33.3 (95%CI: 31.5–35.2) in comparison to 26.0 (95%CI: 24.7–27.2) years (p < 0.001).
Conclusion:
Our data suggest benefit of continuing CS until age 18 years and beyond on respiratory function including delayed need to start (continuous) NIV.
Introduction
Duchenne muscular dystrophy (DMD) is a muscle-wasting disease caused by a genetic defect in the dystrophin gene located on the X-chromosome. 1 The first symptoms are lower limb proximal weakness and calf hypertrophy. Most patients become wheelchair dependent around the ages of 10–12 years. Wheelchair dependency and axial muscle weakness often lead to development of scoliosis. Over time patients experience loss of motor function in upper limbs and progressive weakness of respiratory muscles. They also develop cardiomyopathy, which can lead to symptomatic heart failure and a risk of cardiac arrhythmias and sudden death.1,2
While in the 1960–1970s, average life expectancy was limited to 14.4 years, survival has increased following advances in standards of care including, in particular, improved respiratory management.3,4 According to a recent meta-analysis, median life expectancy with ventilatory support, introduced in most settings in the 1990s, ranged between 21.0 and 39.6 years. 4
Currently, there is no curative treatment for DMD, but disease modifying treatments including exon-skipping therapies are under investigation or already available in high income countries, and gene therapy development is ongoing. But, at present, CS remain the mainstay treatment, especially in low and middle income countries. Although, the exact mechanism is not fully understood, it is believed to involve a combination of anti-inflammatory properties and interaction with genes involved in muscle regeneration (anabolic effects). 5 Corticosteroids started during early childhood have been shown to delay loss of ambulation, reduce the risk of progressive scoliosis, slow cardiopulmonary dysfunction, and improve survival in young patients.1,6–9 However, long-term use raises concerns about side effects, including behavioural and mood changes, weight gain, growth and puberty inhibition, impaired fat and glucose metabolism, fluid retention, arterial hypertension, osteoporosis with increased risk of vertebral fractures, and cataract development. 1
Where the effects of CS in young DMD patients have clearly been shown, the impact of continued CS use into adulthood remains unclear, particularly regarding respiratory function.
Therefore, our aim is to study whether extending CS treatment into adulthood is beneficial focusing on forced vital capacity (FVC) decline and the need for ventilation.
Methods
Study population
In this retrospective study performed at the University Hospitals of Leuven we collected data from all adults (≥18 years) with DMD who visited the sleep laboratory between the 1st of January 2006 and the 30th of April 2024. These patients are referred on a yearly basis to this sleep laboratory by the pediatric and adult neurology departments to investigate the presence of (nocturnal) hypoventilation to start or adapt non-invasive ventilation (NIV) upon indication.
Institutional ethics committee provided ethical approval for the study to be conducted (S70035).
Clinical data
The following respiratory data were extracted from the medical files. FVC expressed in milliliters (ml) (FVCabs) and %predicted (FVC%pred) calculated according to reference data.10,11 In adults unable to stand we used arm span to estimate height (the surrogate ulnar length might have been more valid in severe scoliotic patients but this parameter was not systematically recorded in the medical files). Only one FVC value was assigned to each age. If ≥2 valid values were available, the value closest to the age was used (e.g., if FVC was 44%pred at 17.8 years and 42%pred at 18.4 years, the 44%pred value was assigned to the age of 18). Start of NIV: refers to the age at which a patient started nocturnal NIV at home. Patients using continuous positive airway pressure for obstructive sleep apnea without night-time hypercapnia were not classified as NIV-users. Start of 24/24 h NIV: denotes the age at which a patient became completely ventilator dependent and started continuous use of NIV, including mouth-piece ventilation. Age at loss of ambulation (defined as the age at which the patient became fully wheelchair-dependent for mobility). Age at need for scoliosis surgery: recorded as the date the surgery was performed or, if no surgical procedure was possible, the date of the first report of spinal curvature >30° Cobb's angle.
Furthermore, data on other key disease milestones were reviewed.
Classification of DMD patients by CS use
Patients without CS prescription or who used CS only as a child for a period <1 year, were categorised as ‘CS-naïve’ patients. Patients who continued CS use from childhood until age 18 or older were designated as ‘continued CS’ patients. In case they stopped CS treatment beyond the age of 18, we only included data when collected before discontinuation.
Statistical analysis
Analyses were performed in SSPS (version 29.0). Data distribution was evaluated using the Kolmogorov-Smirnov test and was found to be gaussian. Differences in outcome were evaluated using the two-sided student-t-test and Fischer's exact test. Additionally, we performed Kaplan-Meier analyses with Log-Rank (Mantel-Cox) test.
To assess the impact of age and CS on FVC%pred and FVCabs from age 18 yearson, a linear mixed-effects model for repeated measurements was used, with FVC%pred or FVCabs as dependent variables, the patients and slopes as random and age, steroid-impact as fixed variables. We also measured the slope of a relative annual decline in FVC%pred, calculated as ((FVC%pred at age X minus FVC%pred at age of 18)/FVC%pred at age of 18) * 100. The linear mixed effects model for repeated measurements was performed using R version 4.4.1.
Results
Study population
Seventy-four DMD patients were referred to the sleep laboratory. Five patients were excluded due to absence of longitudinal data: 1 was relocated to another center, 2 declined (monitoring for) NIV and 2 were palliative patients (one was suffering from end-stage cardiac failure, and the other from end-stage pulmonary insufficiency not responding to a NIV trial), both died shortly after evaluation. In addition, 12 patients were excluded because they received CS for >1 year during childhood and/or early adolescence; by per definition, they could not be considered ‘CS-naïve’. This left a total of 57 patients: 20 in the ‘CS-naïve’ and 37 in the ‘continued CS’ group. Of the 37 patients receiving corticosteroids, 33 were prescribed daily treatment, while 4 were on an intermittent (alternating) regimen.
We could retrieve the age at steroid initiation for 36 of 37 patients, with a mean ± SD of 7.5 ± 2.1 (range 4.7–12.7) years.
Among the ‘continued CS’ patients, all but 4 continued CS use after turning 18. In three of them CS were stopped at the patient's explicit request, in one because of weight gain.
Patient demographics, drug use and key disease milestone data are shown in Table 1. The age range at latest visit or at the time of death was 19.3 to 43.7 years in the ‘CS-naïve” and 18.8 to 35.5 years in the ‘continued CS’ group.
Patient demographics, drug use and key disease milestone data.

Abbreviations: CS = corticosteroids: 0 = ‘CS-naïve’ and 1 = ‘continued CS’ patients; / = not used; ‘defect’ pointed to need for more sophisticated gene sequencing analysis; ♯ = in frame deletion, which is rarely observed in Duchenne but based on both the clinical history and the muscle biopsy data the patient was considered as Duchenne; (*) exon skip therapy temporarily stopped for ±1 year; ? = date unknown; NN = not necessary.
Genetic data were available for 51 patients. All but one had out-of-frame mutations confirming the diagnosis of DMD. The exception had an in-frame deletion of exon 5 of the dystrophin gene, but muscle biopsy showed a complete loss of dystrophin consistent with DMD. Only 1 of the 6 patients without genetic data had a muscle biopsy report (which was compatible with DMD), though all exhibited typical clinical features of DMD confirmed by a neurologist. Seven patients received clinical trial drugs nowadays approved by the FDA as potentially effective: 6 received exon-skipping drugs, but only 2 continued treatment beyond 18 years of age; one 21 year old patient is currently on givinostat.
Cross-sectional analyses at 18 years
FVC%pred
We could retrieve FVC%pred values at the age of 18 in 17/20 ‘CS-naïve’ and in 31/37 ‘continued CS’ patients (Table 2(a)). There were different reasons for missing data: some patients did not attend for evaluation, or were suffering from a respiratory infection not able to perform a reliable pulmonary function test. In the ‘CS-naïve’ FVC%pred (mean ± SD) was 36.9 ± 13.8%pred, in the ‘continued CS’ patients 50.3 ± 16.4; p = 0.007. The mean (95%CI) FVC%pred difference was 13.3 (22.4 to 3.9).
Impact of corticosteroids on clinical manifestations.
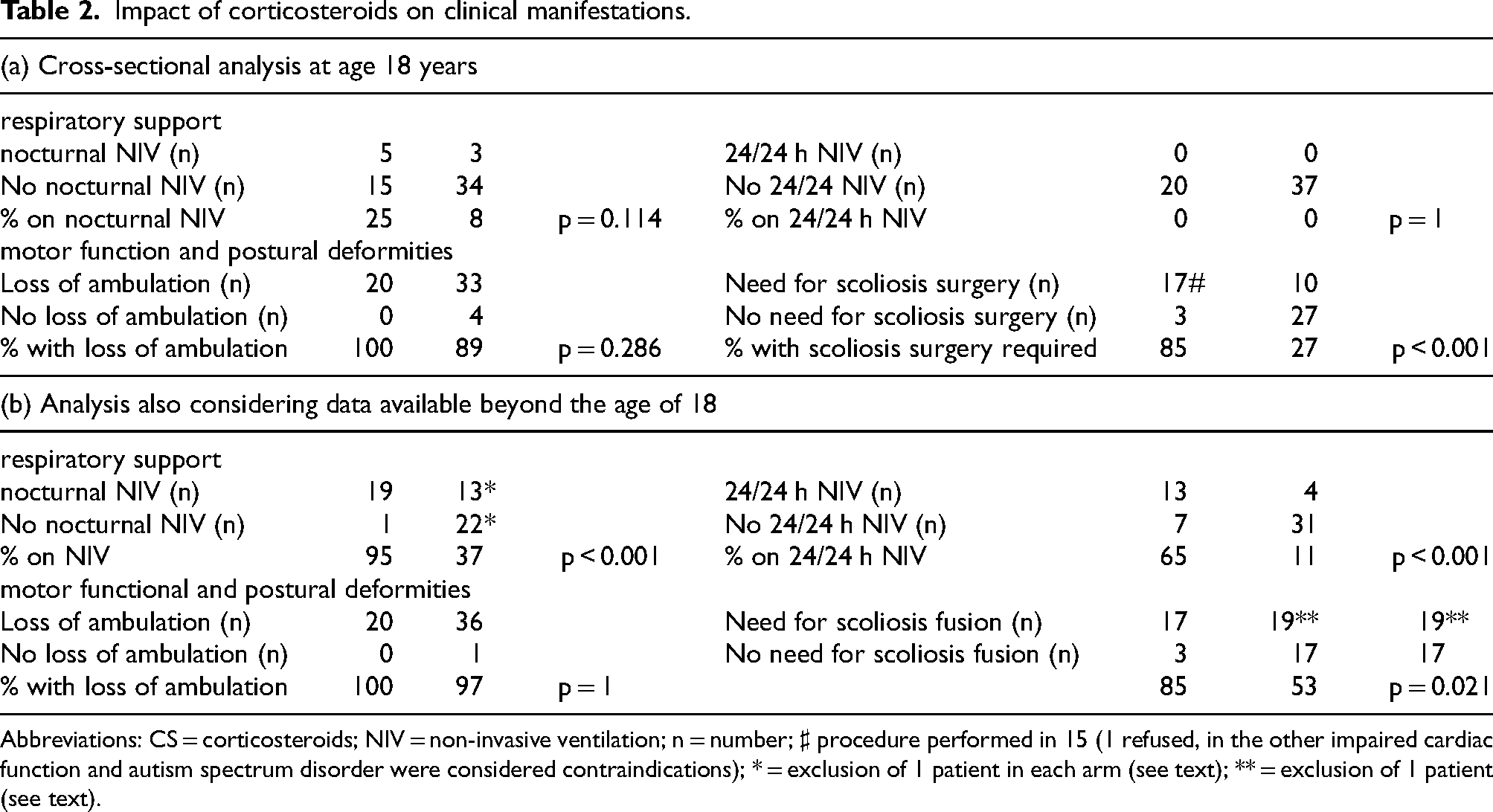
Abbreviations: CS = corticosteroids; NIV = non-invasive ventilation; n = number; ♯ procedure performed in 15 (1 refused, in the other impaired cardiac function and autism spectrum disorder were considered contraindications); * = exclusion of 1 patient in each arm (see text); ** = exclusion of 1 patient (see text).
Initiation of nocturnal and continuous NIV
In both ‘CS-naïve’ and ‘continued CS’ patients, a minority were on NIV (25% and 8%, respectively; p = NS), and none required 24-h ventilatory assistance. None of the patients required tracheal ventilation.
Loss of ambulation and need for scoliosis surgery
All patients who were not on CS lost ambulation before the age of 18, in contrast, 4 patients (11%) in the ‘continued CS’ group remained ambulant at that age; p = NS.
In the ‘CS-naïve’ group, scoliosis surgery was deemed necessary for 17/20 (85%) patients, while in the ‘continued CS’ patients in only 10/37 (27%) patients; p < 0.001.
Longitudinal follow-up data at the age of 18 years and beyond
Evolution of FVC%pred and FVCabs over the range 18–24 years (the number of FVC values after 24 years was very low)
In Figure 1 we present individual FVC%pred and FVCabs values. Notably, 5/37 ‘continued CS’ patients exhibited an increase in FVCabs of at least 150 ml.
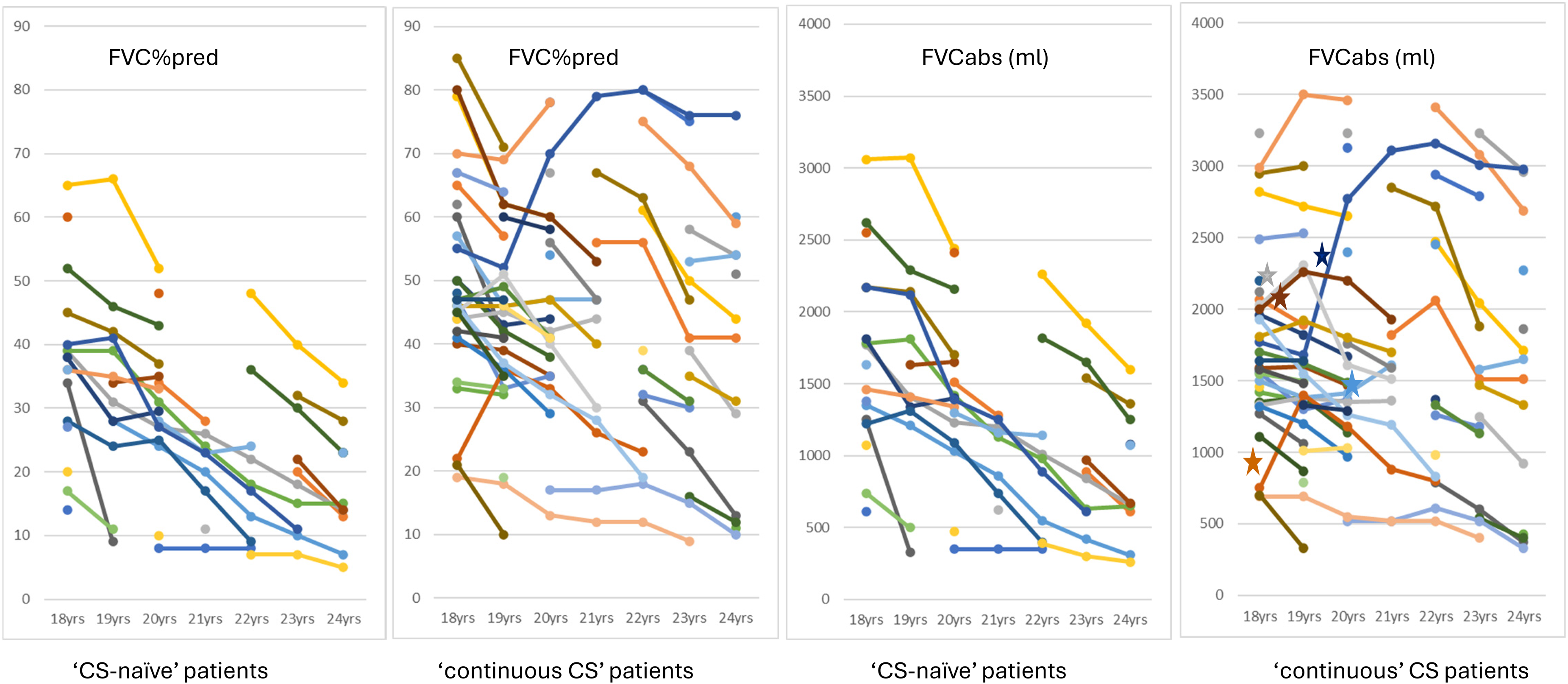
Individual FVC%pred and FVCabs values. Abbreviations: FVC = forced vital capacity; FVC%pred = FVC expressed in %predicted; FVCabs = FVC expressed in absolute value; ml = milliliter, CS = corticosteroids; * = increase of ≥150 ml in comparison to previous value.
The linear mixed effects model for repeated measurements analysis (Figure 2(a)) revealed that FVC%pred declined significantly at an estimated rate of 3.8% per year in the ‘CS-naïve’ and 2.9% in the ‘continued CS’ group, not reaching statistically significant difference between both groups. However, when evaluating the relative annual change in FVC%pred values, the difference was significant (p = 0.012). The FVCabs also declined significantly by an estimated 178 ml per year in the ‘CS-naïve’ and 81 ml in the ‘continued CS’ group. The slope of decline in FVCabs was steeper in the ‘CS-naïve’ group compared to the ‘continued CS’ group, with an estimated difference of 102 ml (p < 0.001). A calculation after excluding the 7 patients who received exon-skipping drugs or givinostat yielded similar findings (Figure 2(b)).
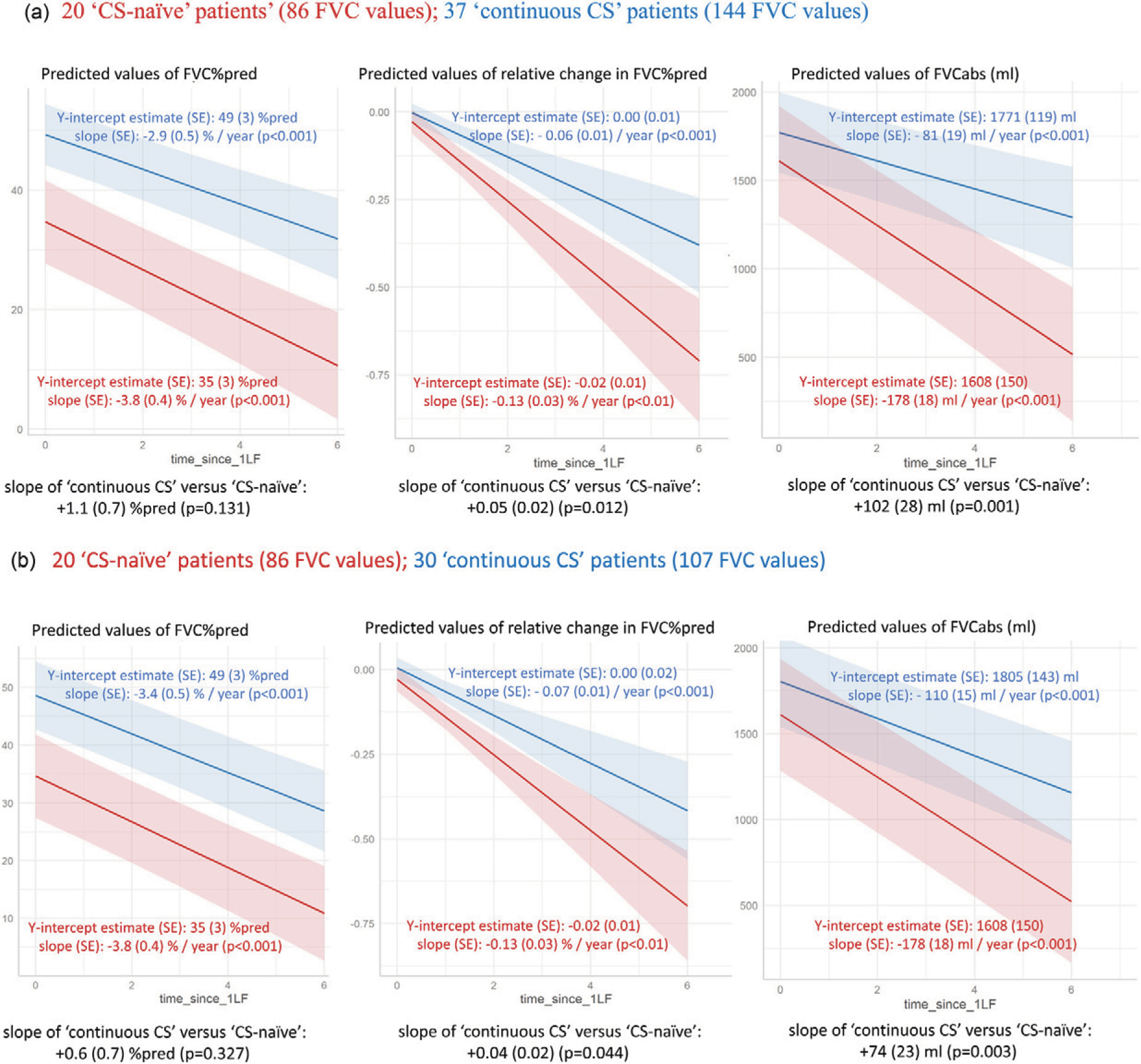
Linear mixed effects model for repeated measurement analyses over the range 18–24 years. (a) = analyses on all patients, (b) = analyses after excluding the 7 patients who used exon skip drugs or givinostat. Abbreviations: FVC = forced vital capacity; FVC%pred = FVC expressed in %predicted; FVCabs = FVC expressed in absolute value; ml = milliliter; CS = corticosteroids; SE = standard error.
Initiation of nocturnal and continuous NIV
All but 1 of the 15 patients in the ‘CS-naïve’ group who were not on NIV at age 18 started NIV in the following years (Table 2(b)). This patient died suddenly at home. The cause of death could not be retrieved from the medical file. In the analysis of the ‘continued CS’ patients we excluded 2 patients who stopped CS treatment before NIV was started; and, 4 patients died before NIV was necessary (3 suddenly at home, 1 in hospital due to a cardiac arrest during a COVID infection).
The Kaplan-Meier analysis is presented in Figure 3(a). In the ‘CS-naïve’ cohort, the mean (95%CI) age at initiation of NIV was 20.3 (19.0–21.6), in the ‘continued CS’ group 28.3 (25.4–31.2) years; p < 0.001.
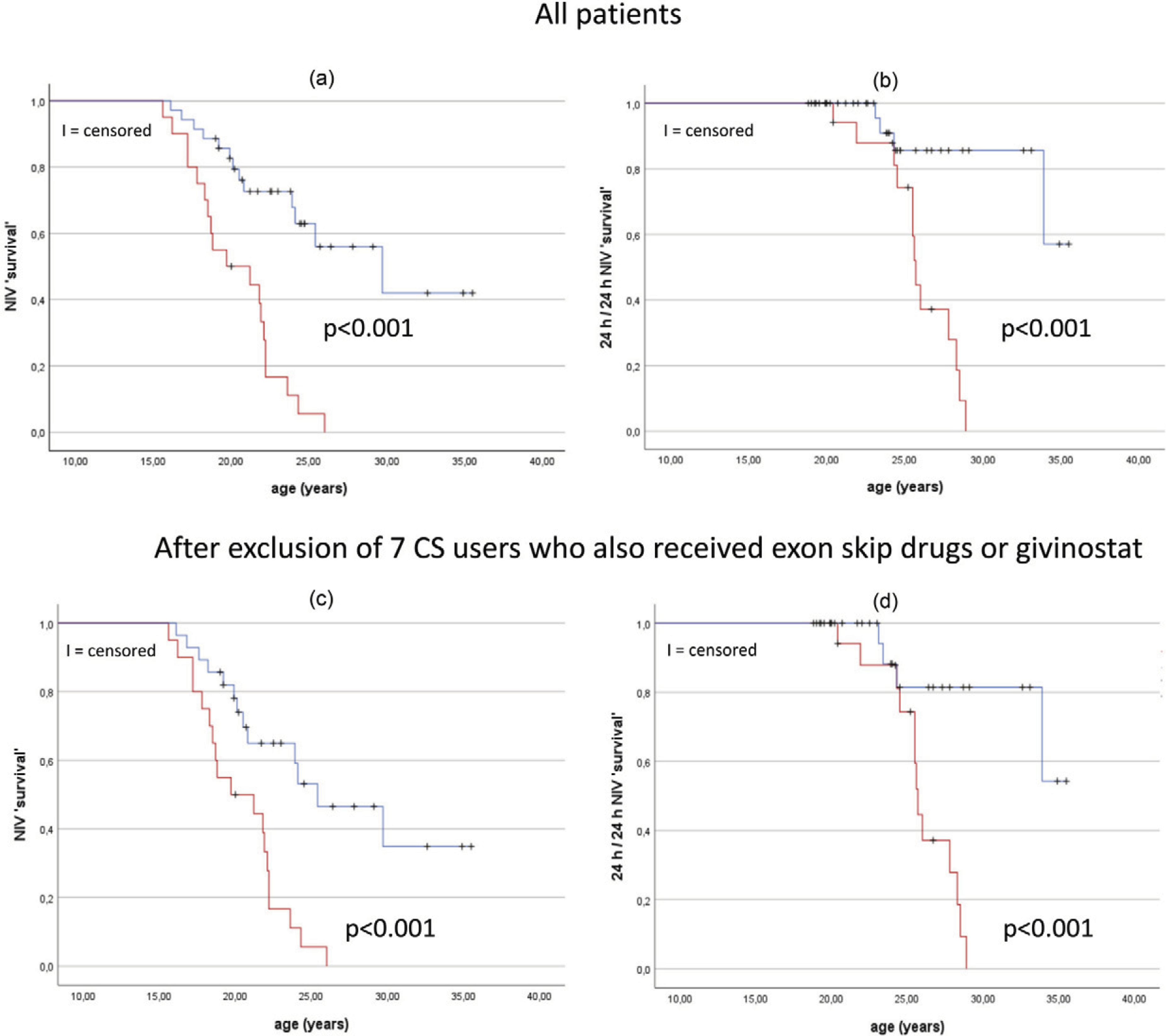
Kaplan-Meier analyses regarding initiation of nocturnal and continuous non-invasive ventilation in all patients (a) and (b) and after exclusion of 7 patients who also received exon-skipping drugs or givinostat (c) and (d). Red curve = ‘CS-naïve’ patients and blue curve = ‘continuous CS’ patients. Abbreviations: CS = corticosteroids; NIV ‘survival’ = fraction not started with non-invasive ventilation; 24/24 h NIV ‘survival’ = fraction without need for continuous non-invasive ventilation.
FVC data within 1 year before or after starting NIV were available for 17 ‘CS-naïve’ and 14 ‘continued CS’ patients without difference between the groups: FVC%pred (mean+/-SD) respectively 26 ± 15%pred and 30 ± 14%pred (p = 0.452). For FVCabs, means+/-SD were 1062 ± 540 ml and 1185 ± 605 ml, respectively (p = 0.560).
Among the 7 ‘CS-naïve’ patients not initiating 24/24 h NIV, 4 died (2 due to heart failure in the hospital and 2 suddenly at home without any notification in the medical file of the exact cause of death). The 31 ‘continued CS’ patients not on 24/24 h NIV included the 4 patients who died before nocturnal NIV was initiated, along with 1 patient on nocturnal NIV who suddenly died at home.
The Kaplan-Meier analysis is presented in Figure 3(b). In the ‘CS-naïve’ group, the mean (95%CI) age was 26.0 (24.7–27.2), in the ‘continued CS’ patients 33.3 (31.5–35.2) years; p < 0.001.
Additional Kaplan-Meier analyses regarding the initiation of NIV and 24/24 h NIV after excluding the 7 patients who also received exon-skipping drugs or givinostat, are presented in Figure 3(c) and (d). The differences remained significant (p < 0.001).
Loss of ambulation and need for scoliosis surgery
Three of the 4 patients in the ‘continued CS’ group who were still ambulant at age 18, eventually lost ambulation at ages 20, 23 and 30 years, respectively. (Table 2(b)) The fourth patient, currently 25.5 years old, remains ambulant.
The Kaplan-Meier analysis is presented in Figure 4(a). We excluded 1 patient from the ‘CS-naïve’ and 1 from the ‘continued CS’ group due to missing data on the exact age of ambulation loss. In the ‘CS-naïve’ mean (95%CI) age at loss of ambulation was 10.3 (9.8–10.9) and in the ‘continued CS’ group 15.1 (13.5–16.7) years; p < 0.001.
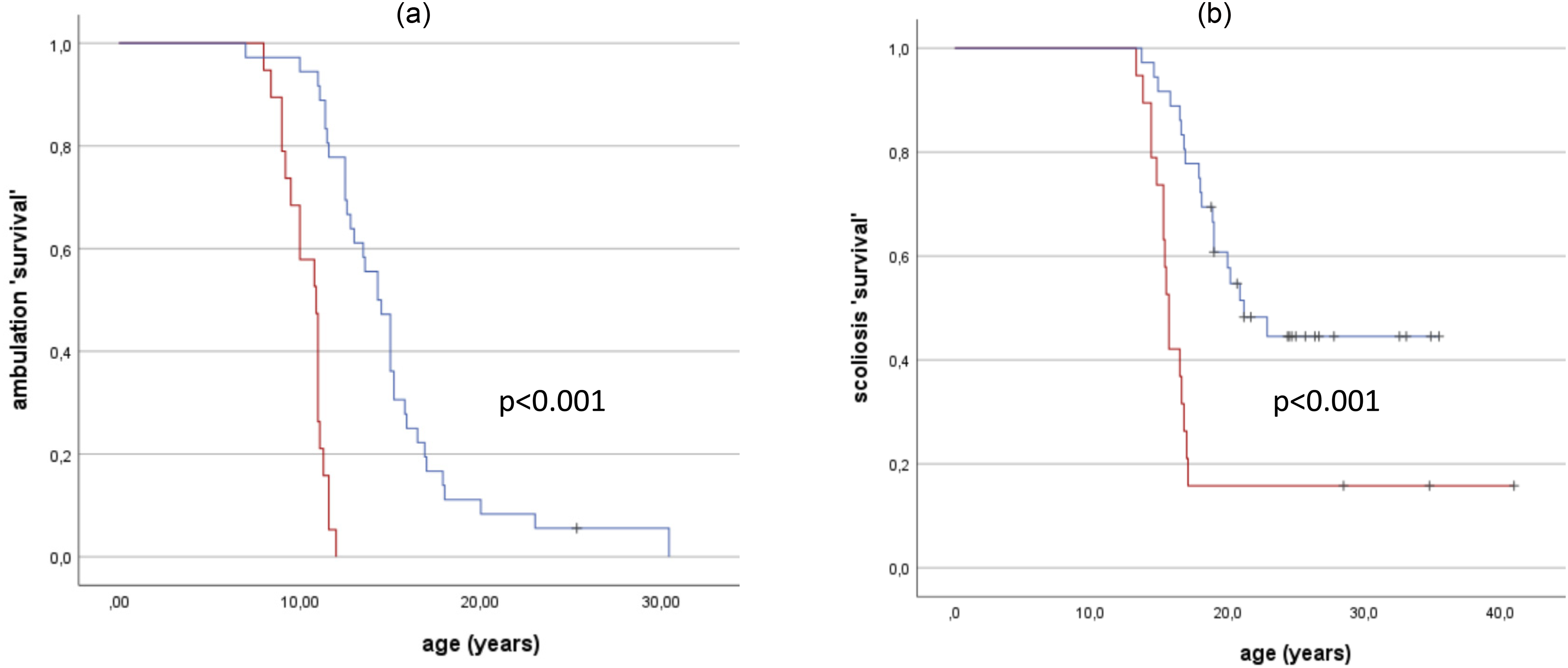
Kaplan-Meier analyses regarding time ∼ loss of ambulation (a) and time ∼scoliosis surgery. Red curve = ‘CS-naïve’ patients and blue curve = ‘continuous CS’ patients. Abbreviation: CS = corticosteroids.
In the analysis of need for scoliosis surgery, we excluded 1 patient from the ‘continued CS’ group who stopped CS immediately upon reaching age 18, while scoliosis surgery was performed more than 2 years later. Scoliosis surgery after age of 18 in the ‘continued CS’ group was necessary in 9 of the 26 patients without indication for scoliosis surgery before the age of 18 and was performed at age (mean+/-SD) of 20.0 ± 1.5 years. The percentage of patients requiring scoliosis surgery was significantly lower in ‘continued CS’ compared to ‘CS-naïve’ patients (p = 0.021).
The Kaplan-Meier analysis is presented in Figure 4(b). We excluded 1 patient from the ‘CS-naïve’ group because the age at which surgery occurred was missing. In the ‘CS-naïve’ group the mean (95%CI) age at need for scoliosis surgery was 19.5 (15.3–23.7) years, in the ‘continued CS’ group 25.9 (22.9–28.8) years; p < 0.001.
Discussion
Our findings indicate that DMD patients who continued CS from childhood into adulthood, experienced not only a significant delay in age at loss of ambulation and a lower (and later) need for scoliosis surgery, but also maintained a significantly better FVC compared to ‘CS-naïve’ patients. Moreover, adult patients who continued CS beyond age 18 demonstrated a significant slower relative annual decline in FVC%pred and FVCabs. Finally, there was a significant delay in the age at initiation nocturnal and continuous NIV.
Recently, Hnaini et al. highlighted respiratory heterogeneity in pulmonary function decline among DMD patients of similar ages and CS regimens. 12 The etiology involves patient factors such as genotype, phenotype, ambulation and scoliosis status and treatment factors including initiation of cough assist and ventilation. Our study also revealed considerable heterogeneity, evident in the significant scatter of FVC%pred and FVCabs values depicted in Figure 1. Notably, in 5 subjects on CS we observed annual increases in FVCabs of at least 150 ml after the age of 18, further contributing to the observed heterogeneity.
While substantial evidence supports positive effects of CS on FVC, most studies focus on children or adolescents, with few evaluating patients beyond age 18.13,14 We refer to the publication by McDonald, which is based on a global, 20-centre collaboration that prospectively collected clinical history and pulmonary function data from 397 DMD patients. While this data-base is substantial, it includes only a maximum of 13 patients in the ‘continued CS’ group per age category beyond 18 years, with only 4 or fewer ‘CS-naïve’ patients. 13 LoMauro performed a 7-year retrospective study on 115 DMD patients a single Italian center. In this study, a maximum of 6 ‘continued CS’ patients per age category were followed beyond 18 years and no FVC data were available after age 22. 14 Notably, compared to these studies, our study included a larger number of adult patients in both the ‘continued CS’ (n = 37) and ‘CS-naïve’ (n = 20) groups.
At age 18, we observed significantly higher FVC%pred values in the ‘continued CS’ compared to the ‘CS-naïve’ patients. This finding aligns with data published by McDonald and Lo Mauro.13,14 McDonald reported a higher peak FVC and a delayed onset of the decline in the CS group prior to age 10. Although the slope of FVC%pred decline during the second decade was similar for both groups, the early impact of CS resulted in better preservation of FVC parameters later in the disease course. LoMauro's data suggested a steeper decline in FVC%pred after age 18 for ‘continued CS’ compared to ‘CS-naïve’ patients. Our study, with a larger sample in both groups, showed that the slope of FVC decline after age 18 was less steep in ‘continued CS’ group. Although this decline in FVC%pred was not statistically significant, the relative decline, considering the starting FVC%pred at age 18, was significantly slower, indicating a real slower decline in pulmonary function. Moreover, FVCabs data demonstrated a significantly slower decline compared to ‘CS-naïve’ counterparts. These findings suggest that CS use slows down the decline in FVC, even after the age of 18 and postpones the need for respiratory support.
Comparative studies on the age of initiation of NIV between ‘continued CS’ and ‘CS-naïve’ patients are scarce. Koeks et al. performed a cross-sectional analysis of clinical and pulmonary function data from 5345 DMD patients from 31 countries. CS treated patients were less likely to need ventilatory support, though their findings were presented only graphically in the appendix of their article and analysis stopped at the age of 20. 15 In our Kaplan-Meier analysis, the mean age of NIV initiation in the ‘continued CS’ patients was 28.3 years, significantly older than the 20.3 years for ‘CS-naïve’ patients. It is important to note that the criteria for initiating NIV at our center have remained consistent over time, primarily based on gas exchange data obtained during annual polysomnography. Moreover, the FVC values at the time of NIV initiation were similar.
To our knowledge, this is the first study to report on use of 24/24 h NIV in DMD patients stratified by CS use. In our Kaplan-Meier analysis, the mean age at initiation of continuous NIV was 26.0 years in ‘CS-naïve’ patients, slightly higher than the mean age of 22.3 years reported in a large single-center (Newark, USA) chart review by Bach which focused on (presumed) non-CS treated patients. 16 More importantly, our study presents the novel finding that 24/24 h NIV dependency can be delayed until a mean age of 33.3 years in patients continuing CS treatment beyond age 18.
Although age at loss of ambulation and need for scoliosis surgery were not the primary outcome parameters, the results are noteworthy.
The delay in ambulation loss and less patients needing scoliosis surgery among ‘continued CS’ patients might have implications for pulmonary function. Cohorts with early loss of ambulation have been associated with a higher rate of pulmonary function decline.12,17–19 This decline may arise from several mechanisms including secretion retention due to reduced cough ability, development of atelectasis, and progression of scoliosis and development of restrictive pulmonary disease. The combination of progressive scoliosis and respiratory muscle weakness has been shown to negatively impact pulmonary function.14,18–20 Interestingly, if scoliosis surgery is necessary in ‘continuous CS’ patients, it is often delayed and should be kept into consideration even for patients older than 18. Chronic high-dose CS treatment inhibits growth and puberty, so changes in scoliosis curve may still occur later on. 1
The strength of this study lies in it reflection of real-world data from a relatively large cohort of adult DMD patients. However, there are limitations.
First, as noted in the methods, the reliability of using arm span instead of ulnar length as a surrogate for height to calculate FVC%pred may be subject to criticism.
Second, most ‘CS-naïve’ patients were born in an earlier era than those continuing CS. Over time, strategies related to DMD-dedicated physiotherapy (e.g., cough assist) may have evolved, introducing potential bias.
Third, a subset of 7 ‘continued CS’ patients received additional treatments such as gene modification therapies (exon-skipping) or a supplementary anti-inflammatory agent (givinostat), drugs that are now considered potentially effective for DMD, which could have influenced the reported outcomes. However, only 3 of them used these drugs until age 18 or beyond. Even after excluding these 7 patients, the positive impact of CS remained evident. Nevertheless, in our rapidly evolving medical landscape, it is essential to acknowledge the potential effects of these additional treatments.
In conclusion, continuation of CS into adulthood appears beneficial in terms of slowing the decline in FVC, delaying the initiation of NIV and postponing the need for 24/24 h NIV. However, the balance between these benefits and the risk of non-ventilatory side effects remains an open question, warranting further longitudinal research in larger cohorts of adult DMD patients.
Footnotes
Acknowledgements
The authors thank Dr Tinne Goos for her assistance in the statistical analysis.
Ethical considerations
All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee (the Ethics Committee Research UZ / KU Leuven, Leuven, Belgium) and based on the principles of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
For a retrospective type of study, official patient consent is not required. Ethics approval was received from the Ethics Committee Research UZ / KU Leuven (S70035).
Credit author statement
Bertien Buyse: Conceptualisation, Methodology, Formal analysis, Writing – original draft; Dries Testelmans: Review and editing; Alexandros Kalkanis: Review and editing; Mieke Boon: Review and editing; Liesbeth Dewaele: Review and editing; Kristl Claeys: Methodology, review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request. Data are located in controlled access data storage at UZ Leuven/KU Leuven, Leuven, Belgium.